
Abstract
Objectives
Due to increasing care needs and decreasing care potentials, research around informal caregiving gains attention. Relatively new – but of utmost importance – is the role of socioeconomic inequalities in care and wellbeing. Although caregiving can be rewarding, a growing body of research shows that informal caregiving often has negative consequences for individuals’ wellbeing. Theoretically, we expect these negative outcomes to be more pronounced among caregivers with lower socioeconomic resources. The current study examines socioeconomic inequalities in the consequences of caregiving inside the household for life satisfaction.
Methods
We draw on longitudinal data from the Survey of Health, Ageing, and Retirement in Europe (SHARE waves 2, 4, 5, and 6). We estimated pooled ordinary least squares and fixed-effects regression models to examine the consequences of informal care provision within the household for individuals’ life satisfaction, and whether household wealth moderates this relationship, controlling for individuals’ sociodemographic and health characteristics.
Results
Care provision inside the household was negatively associated with older adults’ life satisfaction. The longitudinal analyses accordingly show that the uptake of care led to declines in life satisfaction. Differentiating by socioeconomic background, we find that caregivers with higher socioeconomic resources in terms of wealth generally experienced higher life satisfaction. Our longitudinal analyses on wellbeing declines reveal, however, that these mechanisms did not significantly differ by socioeconomic status of the caregiver.
Discussion
Our findings suggest the need for increased investments in support services for informal caregivers to mitigate caregiving burdens, irrespective of socioeconomic status, and enhance later life wellbeing.
Introduction
One of the major challenges of population aging is that an increase in the number of older adults is expected to lead to increasing care demands. Across Europe, projections for the future number and share of care dependent older adults support this assumption, and also show that the number of potential caregivers decreases while the supply of formal care has been reducing (Albertini & Pavolini, Citation2017; Colombo, Llena-Nozal, Marcier, & Tjadens, Citation2012), which in turn puts pressure on caregivers.
Consequently, a growing body of research investigates the effect of caregiving on the wellbeing of informal caregivers. Cross-sectional studies show that caregivers often experience lower happiness (Verbakel, Citation2014), and declines in their life satisfaction (Hajek & König, Citation2016) and quality of life (Rafnsson, Shankar, & Steptoe, Citation2017) in longitudinal assessments. However, these links vary by context. Caregiving within the household context is especially detrimental for one’s mental health (Kaschowitz & Brandt, Citation2017; Litwin, Stoeckel, & Roll, Citation2014). Moreover, care seems to be generally less detrimental to wellbeing in Northern welfare states (Brenna & Novi, Citation2016) and with a more developed national and regional care infrastructure (Verbakel, Citation2014; Wagner & Brandt, Citation2018).
Thus far, there is limited research on how the wellbeing consequences of caregiving might vary by socioeconomic status (SES) as by now research on SES and care has focused mainly on care recipients. This question is important as lower SES groups are typically more involved in informal care and provide care at higher intensities (Broese van Groenou & De Boer, Citation2016; Saito, Kondo, Shiba, Murata, & Kondo, Citation2018) which, according to the caregiver “stress process model” (Pearlin, Mullan, Semple, & Skaff, Citation1990), contributes to higher burden. Moreover, individuals with lower SES cannot easily access formal assistance due to lower financial means and typically have less information about the “care system” in general (Albertini & Pavolini, Citation2017; Ilinca et al., Citation2017). It is also well known that (older) individuals with lower SES are in worse health and report lower wellbeing compared to individuals with higher SES (Jivraj & Nazroo, Citation2014; Schöllgen, Huxhold, & Tesch-Römer, Citation2010), which could make them vulnerable to caregiving related changes in wellbeing. Findings from Switzerland (Tough, Brinkhof, Siegrist, & Fekete, Citation2020) and Japan (Saito et al., Citation2018; Tokunaga & Hashimoto, Citation2017) indeed suggest that individuals in lower SES groups – measured by income and education – are more likely to provide intense care, and to report caregiving burden compared to those in higher SES groups. As these are cross-sectional studies, however, they cannot examine changes in informal caregiving and wellbeing, and their variation by socioeconomic status.
Based on the longitudinal Survey of Health, Ageing and Retirement in Europe (SHARE), we aim to fill this gap by investigating the wellbeing consequences of informal within household care across different SES groups. We not only assess whether caregivers in lower SES groups experience lower levels of wellbeing compared to those in higher SES groups but address wellbeing changes due to caregiving for different SES groups. SES is measured by household wealth, which represents individuals’ life course accumulation and current ownership of financial resources that provide the means to lead more self-determined lives in later life (Demakakos et al., Citation2016; Jivraj & Nazroo, Citation2014). To the best of our knowledge, this is the first study to address wealth disparities in the wellbeing consequences of informal caregiving in Europe. The remainder of this paper is structured as follows. First, we discuss theoretical approaches and empirical evidence on SES, care and wellbeing. Next, we describe the data and methods used in this study. Following, we present our empirical findings, a discussion of the results and implications.
Theoretical links and empirical findings on SES, caregiving and wellbeing
Following the behavioral “informal care model” (Broese van Groenou & De Boer, Citation2016) the decision to give care is driven by an individual’s willingness to provide care and their social and political environment. This “willingness” is formed by attitudes and beliefs that are shaped by a range of socio-cultural norms at the individual (e.g. family, gender, religion) and country (solidarity, reciprocity) levels, affection towards the care dependent person, and perceived barriers. The perceived support of family members or the social network and the provision of formal support via the community can positively influence individuals’ care uptake. However, the geographical distance between caregiver and care dependent person and employment can hinder hands-on caregiving.
Following these arguments, socioeconomic disparities in the uptake of informal caregiving can be expected. Specifically, individuals in lower SES groups are more likely to provide care and at higher intensities than those in higher SES groups due to a combination of demographic and socioeconomic factors. These include smaller and more kin-based social networks (Broese van Groenou & Van Tilburg, Citation2003), and closer geographic proximity to kin (Fors & Lennartsson, Citation2008) among lower SES groups. Additionally, lower SES individuals have higher risks of poor health for a larger share of their lives (Pongiglione, De Stavola, & Ploubidis, Citation2015), lower employment rates, with and without health-related limitations (Schram, Schuring, Oude Hengel, & Burdorf, Citation2019), and fewer resources to access privately-paid carers (Broese van Groenou, Glaser, Tomassini, & Jacobs, Citation2006). Yet, the informal care model does not explicitly state how caregiving itself is linked to caregivers’ wellbeing and the socioeconomic disparities therein.
Here we draw upon the well-known “stress process” framework (Pearlin et al., Citation1990), which posits that caregiving, though rewarding, can diminish wellbeing due to the interplay of caregivers’ characteristics and the caregiving context (e.g. socioeconomic resources, gender, health history, living arrangements) as well as caregiving related stressors. Caregiving stressors include health problems of the care dependent, a changing relationship between the caregiver and care recipient, and stress induced by time constraints when caregivers juggle caregiving (and other family responsibilities) and employment demands. However, support from social network members and the use of formal care may diminish caregiving burden (Pearlin et al., Citation1990; Verbakel, Metzelthin, & Kempen, Citation2018).
Combining the two outlined theoretical models leads to two assumptions. First, lower SES individuals are more likely to provide care, overall, and with higher intensities. Second, lower SES individuals experience higher levels of caregiving stress as they are often less reliant on formal care due to their lower financial means and need to rely solely on their smaller network (Aartsen, Veenstra, & Hansen, Citation2017).
Furthermore, subjective wellbeing varies by one’s socioeconomic status, due to material, behavioral, and psychosocial mechanisms. Given structural inequalities in resource allocation, socioeconomically advantaged groups can access better material living conditions (e.g. housing or leisure activities), adopt healthier lifestyles (e.g. positive health behaviors), and develop internal psychosocial resources to mitigate external stressors (e.g. perceived control, social integration), thereby enhancing their subjective wellbeing in later life (George, Citation2010; Pinquart & Sörensen, Citation2000).
There remains some debate regarding the best way to measure older adults’ socioeconomic status, as well as which indicator is most critical to their subjective wellbeing. Some commonly used indicators include education, income, occupational class, and wealth. Depending on the life course, these indicators are more or less suitable to capture wellbeing differences between individuals (see George, Citation2010; Grundy & Holt, Citation2001; Pinquart & Sörensen, Citation2000; Read, Grundy, & Foverskov, Citation2016 for detailed reviews). Wealth is, arguably, the most critical to older adults’ wellbeing as, unlike income, it is less sensitive to labor force participation or occupation type. Moreover, unlike education and occupational class that reflect past circumstances, wealth reflects one’s current socioeconomic position and is associated with individuals’ health and social participation (Demakakos et al., Citation2016; Niedzwiedz et al., Citation2016). When considering caregiving, if individuals are unable to provide care independently, wealth provides greater capacity to access alternative caregiving resources such as formal care. Taken together, these approaches suggest that the wellbeing of individuals in lower SES groups will be more negatively affected by caregiving compared to individuals of higher SES groups.
Empirical overview
Socioeconomic status and care
As stated above, research on SES inequalities in care has focused mainly on care recipients. In an early study, Broese van Groenou et al. (Citation2006) found that individuals in low or middle SES groups received informal and formal care more often compared to higher SES groups. Ilinca et al. (Citation2017) partly confirm this, showing that in most European countries less affluent people use informal care more often and this may reflect their poorer health. Albertini and Pavolini (Citation2017) also showed that in countries relying on strong cash-for-care policies, the likelihood of receiving formal care positively depends on individuals’ income. Additionally, Swinkels et al. (Citation2016) suggest, that a cutback in state provided formal care increases the meaning of private income to buy formal care. Recently, Floridi, Carrino, and Glaser (Citation2021) examined the role of regional-level differences in formal care supply, across Europe, to explain SES differences in the use of home and formal care. They found that individuals with lower income and wealth were more likely than the wealthier to combine informal and formal home-care use in regions with more LTC beds.
SES differences in caregiving are less well studied. Some studies show that individuals in lower SES groups are indeed more likely to provide care to their relatives overall, and at higher intensities – at least in some contexts (e.g. for Japan Saito et al., Citation2018; Tokunaga & Hashimoto, Citation2017). One cross-sectional study of Japanese caregiving women showed that single women with lower education were at higher risk of providing care for heavily care dependent, which goes along with a higher intensity (Tokunaga & Hashimoto, Citation2017).
Socioeconomic status and wellbeing
Socioeconomic inequalities in wellbeing are well established and have been assessed in a plethora of studies. Rueda, Artazcoz, and Navarro (Citation2008) found a positive association between lower education and poor psychological health. Several other studies show that health inequalities persist among the (very) old (e.g. Enroth, Raitanen, Hervonen, & Jylhä, Citation2013; Grundy & Sloggett, Citation2003). However, context matters in a comparison of England and the U.S., Jivraj and Nazroo (Citation2014) found that having chronic conditions and living in a household with low wealth are associated with lower life satisfaction and quality of life. These relationships are more marked in the U.S. That is, having no qualification (or a degree) is more negative (more positive) for life satisfaction and quality of life than in England.
As indicated earlier, the wellbeing of informal caregivers can also be conditioned by their SES. Yet, to date, little is known about the moderating role of caregiver SES for the relationship between caregiving and wellbeing. A cross-sectional Japanese study based on data of the Japan Gerontological Evaluation Study (JAGES) suggests that older caregivers (65+) in lower income groups tend to give care, also at higher intensities, and have a higher risk of reporting depressive symptoms than those in higher income groups. However, in all income groups, caregivers were more likely to report higher depressive symptoms than non-caregivers (Saito et al., Citation2018). Research in Switzerland (Tough et al., Citation2020), assessed the subjective and objective burden of caregivers who gave heavy care to physically disabled partners taking the caregivers’ and the partners SES status into account by using information on household income, education, subjective social position, financial strain and home ownership. Their results suggest that caregiver burden, measured with the Zarit Burden Interview and by caregiving hours, was higher in lower SES groups. The authors suggest that the poor health status of the care recipient, which goes along with a higher care load, and fewer psychological resources of the caregiver to cope with burden as well as the caregivers’ unmet care needs, increase burden. Taken together, these two studies provide evidence for SES inequalities in caregivers’ psychological health and wellbeing. However, they focus on rather specific caregivers (65+) or caregiving relationships (heavily physically disabled) based on cross-sectional designs, that neither measure SES using wealth nor address changes in wellbeing.
Building on the state of research, we hypothesize that caregivers in lower SES groups experience lower levels of wellbeing compared to those in higher SES groups. Moreover, the wellbeing decline due to an uptake in caregiving is likely steeper for people with lower SES because they are more likely to face more demanding caregiving situations and have fewer resources with which to alleviate pressures caused by informal caregiving.
Methods
Data and sample
Data were drawn from SHARE version 7.0.01, which covers various aspects of older adults’ lives including their socioeconomic conditions, health and wellbeing, social support, and household contexts. Eligible participants, ages 50 years and older in private households, and their spouses/partners of any age, were interviewed biannually across participating countries (Börsch-Supan et al., Citation2013; Börsch-Supan, Kneip, Litwin, Myck, & Weber, Citation2015). Our analyses utilize data from waves 2, 4, 5, and 6 (2006–2015). We use wave 2 as our baseline because life satisfaction, our outcome of interest, was asked and measured differently in wave 1. We also excluded wave 3 due to its retrospective design, and wave 7 because questions on social support – our main independent variable of interest – were not included in the core interview. Finally, given our interest to examine the longitudinal dimension of the relationship between care provision and older adults’ wellbeing within the European context, we included European countries with data for at least two waves. Thus, four countries are excluded – Israel, Ireland, Hungary, and Croatia.
Our sample covers older adults in 17 countries including Northern (Denmark, Sweden), Western (Austria, Belgium, Netherlands, France, Germany, Switzerland, Luxembourg), Southern (Portugal, Spain, Italy, Greece), and Eastern (Czech Republic, Poland, Slovenia, Estonia) Europe. This provided us with 238,396 observations from 107,198 individuals. We further excluded older adults living alone (51,162 observations), and missing data on variables included in our analysis (32,928 observations), leaving us with an analytic sample of 154,306 person-year observations from 79,014 individuals.
Measures
Life satisfaction, our wellbeing outcome, was measured by individuals’ response to a single question: “On a scale from 0 to 10 where 0 means completely dissatisfied and 10 means completely satisfied, how satisfied are you with your life?” Thus, higher values indicate higher life satisfaction. This global measure of life satisfaction allows respondents the flexibility to weight the value of specific life domains (e.g. employment, health) by their own standards to assess their life satisfaction (Pavot & Diener, Citation1993a), and has been shown to have adequate reliability and validity (George, Citation2010; Pavot & Diener, Citation1993b). Importantly, life satisfaction is a stable indicator of wellbeing (not sensitive to changes in moods) whilst being responsive to changes in life circumstances (Pavot & Diener, Citation1993a).
Informal care provision was measured by care provision inside the household. Respondents were asked, “Is there someone living in this household whom you have helped regularly during the last twelve months with personal care, such as washing, getting out of bed, or dressing? By regularly we mean daily or almost daily during at least three months. We do not want to capture help during short-term sickness of family members.” We created a dichotomous measure based on affirmative responses to this question. We focus on care provision inside the household as previous research (Kaschowitz & Brandt, Citation2017) has shown within household caregiving is detrimental to caregivers’ mental health.
In our pooled ordinary least squares regression multivariate analyses we further excluded older adults who received care from anyone within the household. This was necessary to minimize biased estimates based on older adults who receive care having reduced capacity to provide care and potentially experiencing lower life satisfaction.
Household wealth is our main indicator of SES as it captures the life course accumulation of assets. Wealth (total net worth) represented the sum of the household’s net financial (e.g. sum of bank accounts, stock of mutual funds and bonds and savings, minus liabilities) and real assets (sum of the value of primary residence net of mortgage, other real assets, owned business, and vehicles). Furthermore, the SHARE team converted all wealth data to Euros in all countries and imputed missing data (Stuck et al., Citation2019). For our study’s purposes, we categorized household wealth by country-specific quintiles in each wave so we could assess the role of wealth inequality for wellbeing based on the household’s relative wealth position, over time, in their respective social context. Additional controls were based on the state of research, and include age (continuous), gender (men = 0, women = 1), household size (continuous), area of residence (urban = 0, rural = 1), limitations with instrumental activities of daily living (0 = none, 1 = 1+ limitations), survey wave, and country.
Analysis
Descriptive analyses, presented first, examine the relationship between caregiving and life satisfaction according to wealth quintile for the overall sample. Our multivariate analyses utilize both pooled ordinary least squares regression (POLS) with clustered standard errors at the individual level, and fixed-effects models (FEM) to examine the effect of caregiving inside the household on life satisfaction.
To examine whether wealth moderates the relationship between caregiving and life satisfaction, we included an interaction of caregiving and wealth. In the POLS models, we assume that the error terms are uncorrelated with the interaction of caregiving and wealth quintile, thereby treating unobserved differences between individuals as random. Given this is a strong assumption; we also use FEM models. In FEM models, the error terms are separated into 1) an individual specific error that remains constant over time, and 2) an idiosyncratic error term that varies over time and individuals. FEM models treats every individual as their own control, thereby controlling for all constant (un)observable characteristics (e.g. personality or preferences) between individuals that may bias the estimated pooled OLS coefficients. Therefore, FEM models focus on within-person variation to estimate the coefficients. FEM models account for selection and endogeneity biases more effectively than POLS models, however, the coefficients can still be biased. Potential endogeneity sources include unmeasured time varying predictors (e.g. previous caregiving history), measurement errors, and reverse causality. It is also important to note that estimates of the FEM represent an average treatment effect of the treated, i.e. caregiving over time for the caregivers (Brüderl & Ludwig, Citation2015).
Results
Descriptive results
Approximately 8% of the sample reported ever providing care to someone inside the household. Additionally, 35% of older adults who provided care in one wave also indicated so in a following wave, and 6% of older adults who did not give care in one wave began providing care in a subsequent wave. These caregiving transitions yield sufficient variation to support panel analysis. indicates cross-national differences in caregiving. Sothern and Eastern European countries show the highest share of within household caregivers: Spain (11.2%), Italy (10%), Czechia (10%) and Estonia (10%). Northern and Western countries had a lower prevalence of caregiving inside the household, approximately 3–5%, with the exception of Belgium (9%). Caregivers and non-caregivers in our sample also show statistically significant differences in their socio-demographic and health characteristics (). Caregivers were more likely to be older, in slightly larger households, female, less wealthy (quintile I and II), and limited in (instrumental) activities of daily living.
Table 1. Distribution of the total sample of older adults and caregivers inside the household, showing the person-year observations and individuals, by country of residence.
Table 2. Sample sociodemographic and health characteristics by caregiving status.
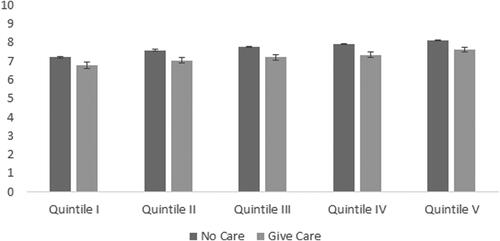
According to our descriptive results older adults’ life satisfaction varied by their caregiving status and position in the wealth distribution. , displaying the mean life satisfaction by caregiving status and wealth quintile, indicates that across all wealth quintiles, caregivers within the household report lower life satisfaction than non-caregivers. Furthermore, the least wealthy caregivers (quintile I) reported significantly lower life satisfaction than the wealthiest caregivers (quintile V). Our descriptive results provide a preliminary indication that caregiving can have negative consequences for older adults’ subjective wellbeing, which may also be conditioned by their socioeconomic resources.
Figure 1. Mean life satisfaction by caregiving status and wealth quintile showing 95% confidence intervals. Source: SHARE waves 2,4,5,6. Authors’ calculations.
Multivariate results
Our multivariate POLS regression models () show that net of controls, caregiving inside the household had a statistically significant negative association (Model 1, b= −0.35), while household wealth had a statistically significant positive association (Model 1, ranging from b = 0.29 to b = 0.73) with life satisfaction. We further examined whether household wealth moderates the relationship between caregiving inside the household and life satisfaction. The results, however, do not show a statistically significant moderating effect of wealth (Model 2).
Table 3. Pooled ordinary least square regression and fixed effects regression coefficients showing main and interaction effects of care provision and wealth on life satisfaction.
Although our POLS models indicate that care provision within the household was linked to lower life satisfaction, the estimated coefficients cannot verify that this is a deterioration driven by the uptake of caregiving. To adjust for this potential selection bias, we took advantage of the longitudinal structure of our data and estimated fixed-effects regression models, which examine changes within individuals (Models 3 and 4). Importantly, the results of our FEM show a substantial reduction in the magnitude of the coefficients but the direction of the relationships is unaltered. Specifically, care provision within the household did indeed have a negative effect on life satisfaction (Model 3, b= −0.18). Likewise, wealthier older adults reported increased life satisfaction compared to their less wealthy counterparts (Model 3, ranging from b = 0.07 to b = 0.19). As observed in the POLS models, wealth still did not significantly moderate the relationship between caregiving and life satisfaction (Model 4). Taking a closer look at wealth disparities in the relationship between informal caregiving and life satisfaction, we estimated separate POLS and FEM by wealth quintiles. Results presented in show that in each wealth quintile care providers experienced lower satisfaction, and declines in life satisfaction over time, relative to non-caregivers.
Table 4. Pooled ordinary least square regression and fixed effects regression coefficients showing the relationship between care provision and life satisfaction by wealth quintile.
Discussion
Hand in hand with several demographic and socioeconomic trends, informal caregiving among older Europeans is expected to increase in the coming years. Older adults are likely to need care, but face a reduced supply of informal caregivers (Colombo et al., Citation2012). Much research to date shows that the active provision of care is associated with negative wellbeing outcomes (Litwin et al., Citation2014; Verbakel, Citation2014; Wagner & Brandt, Citation2018). Informal caregiving and wellbeing are, however, unevenly distributed across SES groups. Yet, research to date has largely overlooked the intersection of caregiving and socioeconomic background for older adults’ wellbeing. The present study extends previous research on the wellbeing consequences of informal caregiving by examining wealth disparities in the life satisfaction of informal caregivers within the European context.
Consistent with prior research on the unfavorable mental health and wellbeing consequences of informal caregiving (Hajek & König, Citation2016; Kaschowitz & Brandt, Citation2017; Rafnsson et al., Citation2017), our findings reveal that providing care inside the household is detrimental for older adults’ self-reported wellbeing. Care provision inside the household is not only negatively associated with lower life satisfaction in cross-sectional models (pooled OLS) but also with declining life satisfaction in a longitudinal (FEM) perspective, after accounting for important characteristics of respondents. Furthermore, the weaker relationship between caregiving inside the household and life satisfaction in the longitudinal panel models suggests that caregiving inside the household is a selective process: those with initially lower levels of life satisfaction are more likely start providing care within the household. This may arise from on average poorer health of all household members and thus more care needs, lower employment and thus more time to provide care, and less access to external support by informal or formal care providers. Additionally, the results of the POLS models may be more biased due to unobserved characteristics, than the FEM, and potentially overestimate the relationship between informal caregiving and life satisfaction. Given the FEM models examine changes within persons over time, this result makes an even stronger case for the negative wellbeing consequences of the provision of care within the household.
Aligned with prior research (Jivraj & Nazroo, Citation2014; Niedwiedz et al., Citation2016), wealth is protective for older adults’ subjective wellbeing. Our cross-sectional and longitudinal findings show that wealthier older adults experience higher life satisfaction compared to the less wealthy. Contrary to our expectations, however, wealth does not moderate the relationship between caregiving inside the household and life satisfaction. Whilst our cross-sectional findings suggest that less wealthy caregivers do experience lower levels of wellbeing, this cannot solely be attributed to caregiving as can be seen in longitudinal models. These show that less wealthy caregivers do not experience steeper wellbeing declines when opting into caregiving. Instead, we find that in (almost) every wealth quintile caregiving decreases life satisfaction. This finding aligns with prior research on socioeconomic differences in the mental health of older informal caregivers in Japan (Saito et al., Citation2018), which also found similar levels of depression for caregivers across income groups.
As other studies on wellbeing in older age (e.g. Berg, Hoffman, Hassing, McClearn, & Johansson, Citation2009), our findings imply there is high stability in the level of life satisfaction for those who take up caregiving regardless of their position in the wealth distribution. For instance, the least wealthy start caregiving at a lower baseline level of life satisfaction, while the wealthiest start at a higher level, but this general pattern is unchanged over time. Still, there may be different underlying mechanisms, including coping mechanisms, which may also be related to life course cumulative (dis)advantages for each wealth group that in turn shape the evaluation of caregivers’ life satisfaction. Future research should incorporate indicators of coping mechanisms and caregiving experiences earlier in the life course, as potential mediators, to better understand socioeconomic differences in wellbeing consequences of older adults’ caregiving.
Our study is not without limitations. First, we were unable to examine the hours of caregiving within the household (only available in SHARE wave 1) which is likely to be higher amongst older adults in lower socioeconomic strata (Saito et al., Citation2018). Second, we were unable to account for the care recipients’ histories of disability or length of time in impairment, which can affect the caregivers’ preparations (psychological, financial, and others) to provide care. The initial stages of impairment are often the most demanding and caregivers may experience more initial caregiving burdens but eventually adjust to their caregiving roles. Third, we did not examine wellbeing differences by caregiving recipients (e.g. caregiving to partners or children). Although prior research shows that the relationship to care recipients differentiates caregivers’ wellbeing (Litwin et al., Citation2014; Rafnsson et al., Citation2017), our primary interest for this study was to examine the socioeconomic disparities in the life satisfaction of older informal caregivers within the household, generally. Finally, we acknowledge that socioeconomic differences in the relationship between caregiving and subjective wellbeing are likely to differ across contexts. Further analyses (available upon request) revealed a prevailing absence of wealth inequalities in the wellbeing of informal caregivers. In the few countries where we do find wealth disparities (4 out of 17 countries), the patterns are not uni-directional. Less wealthy caregivers experience declines in their life satisfaction in some contexts (Netherlands and Italy), whereas the wealthiest caregivers experience life satisfaction declines in one country (Slovenia) or improvements in another country (Poland). These contextual differences may be due to a range of factors including availability and access to formal caregiving resources, legislation regarding formal and informal caregiving, caregiving norms and preferences. Direct examination of the mechanisms that shape wealth disparities in the life satisfaction of informal caregivers across these contexts requires incorporating specific macro indicators that are beyond the scope of the current study and will addressed in future research.
Thus far, few (national) studies have examined socioeconomic disparities in the wellbeing of informal caregivers (Saito et al., Citation2018; Tough et al., Citation2020). Our study makes an important contribution to this area by demonstrating that caregiving inside the household is selective, and informal caregivers experience declines in their subjective wellbeing, regardless of their socioeconomic positioning as indexed by wealth in this study all over Europe. This study adds more weight to research that advocates for social policies to invest in programs to assess the wellbeing of caregivers and provide resources to alleviate the burdens for all informal caregivers regardless of their socioeconomic status.
Notes
1. This paper uses data from SHARE Waves 2, 4, 5, and 6 (DOIs: 10.6103/SHARE.w1.710, 10.6103/SHARE.w2.710, 10.6103/SHARE.w4.710, 10.6103/SHARE.w5.710, 10.6103/SHARE.w6.710), see Börsch-Supan et al. (Citation2013) for methodological details. The SHARE data collection has been funded by the European Commission through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812), FP7 (SHARE-PREP: GA N°211909, SHARE-LEAP: GA N°227822, SHARE M4: GA N°261982) and Horizon 2020 (SHARE-DEV3: GA N°676536, SERISS: GA N°654221) and by DG Employment, Social Affairs and Inclusion. Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, HHSN271201300071C) and from various national funding sources is gratefully acknowledged (see www.share-project.org).
Ethical approval
No ethical approval was required for our study.
Disclosure statement
We have no conflict of interest to declare.
Funding
This study is funded by the German Research Foundation (DFG) within the Open Research Area for the Social Sciences (ORA) (Grant BR 3868/4-1), to M. Brandt for the project “IN-CARE: How are varying care systems associated with inequalities in care and wellbeing in later life?”
Additional information
Funding
References
- Aartsen, M., Veenstra, M., & Hansen, T. (2017). Social pathways to health: On the mediating role of the social network in the relation between socio-economic position and health. SSM – Population Health, 3, 419–426. doi:https://doi.org/10.1016/j.ssmph.2017.05.006
- Albertini, M., & Pavolini, E. (2017). Unequal inequalities: The stratification of the use of formal care among older Europeans. The Journals of Gerontology. Series B, Psychological Sciences & Social Sciences, 72(3), 510–521. doi:https://doi.org/10.1093/geronb/gbv038
- Berg, A. I., Hoffman, L., Hassing, L. B., McClearn, G. E., & Johansson, B. (2009). What matters, and what matters most, for change in life satisfaction in the oldest-old? A study over 6 years among individuals 80+. Aging & Mental Health, 13(2), 191–201. doi:https://doi.org/10.1080/13607860802342227
- Börsch-Supan, A., Brandt, M., Hunkler, C., Kneip, T., Korbmacher, J., Malter, F., … Zuber, S. (2013). Data resource profile: The Survey of Health, Ageing and Retirement in Europe (SHARE). International Journal of Epidemiology, 42(4), 992–1001. doi:https://doi.org/10.1093/ije/dyt088
- Börsch-Supan, A., Kneip, T., Litwin, H., Myck, M., & Weber, G. (2015) (Eds.), Ageing in Europe – Supporting policies for an inclusive society. Berlin: De Gruyter. doi:https://doi.org/10.1515/9783110444414
- Brenna, E., & Novi, C. (2016). Is caring for older parents detrimental to women’s mental health? The role of the European north–south gradient. Review of Economics of the Household, 14(4), 745–778. doi:https://doi.org/10.1007/s11150-015-9296-7
- Broese van Groenou, M. I., & De Boer, A. (2016). Providing informal care in a changing society. European Journal of Ageing, 13(3), 271–279. doi:https://doi.org/10.1007/s10433-016-0370-7
- Broese van Groenou, M. I., & Van Tilburg, T. (2003). Network size and support in old age: Differentials by socio-economic status in childhood and adulthood. Ageing & Society, 23(5), 625–645. doi:https://doi.org/10.1017/S0144686X0300134X
- Broese van Groenou, M., Glaser, K., Tomassini, C., & Jacobs, T. (2006). Socio-economic status differences in older people’s use of informal and formal help: A comparison of four European countries. Ageing & Society, 26(5), 745–766. doi:https://doi.org/10.1017/S0144686X06005241
- Brüderl, J., & Ludwig, V. (2015). Fixed-effects panel regression. In H. Best & C. Wolf (Eds.), The Sage handbook of regression analysis and causal inference (pp. 327–357). London, UK: Sage Publications Ltd.
- Colombo, F., Llena-Nozal, A., Marcier, F., & Tjadens, F. (2012). Help wanted? Providing and paying for long-term care – OECD. https://www.oecd.org/health/health-systems/help-wanted-9789264097759-en.htm.
- Demakakos, P., Biddulph, J. P., Bobak, M., & Marmot, M. G. (2016). Wealth and mortality at older ages: A prospective cohort study. Journal of Epidemiology & Community Health, 70(4), 346–353. doi:https://doi.org/10.1136/jech-2015-206173
- Enroth, L., Raitanen, J., Hervonen, A., & Jylhä, M. (2013). Do socioeconomic health differences persist in nonagenarians?The Journals of Gerontology. Series B, Psychological Sciences & Social Sciences, 68(5), 837–847. doi:https://doi.org/10.1093/geronb/gbt067
- Floridi, G., Carrino, L., & Glaser, K. (2021). Socioeconomic inequalities in home-care use across regional long-term care systems in Europe. The Journals of Gerontology: Series B, 76(1), 121–112. doi:https://doi.org/10.1093/geronb/gbaa139
- Fors, S., & Lennartsson, C. (2008). Social mobility, geographical proximity and intergenerational family contact in Sweden. Ageing & Society, 28(2), 253–270. doi:https://doi.org/10.1017/S0144686X07006617
- George, L. K. (2010). Still happy after all these years: Research frontiers on subjective well-being in later life. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 65B(3), 331–339. doi:https://doi.org/10.1093/geronb/gbq006
- Grundy, E., & Holt, G. (2001). The socioeconomic status of older adults: How should we measure it in studies of health inequalities? Journal of Epidemiology & Community Health, 55(12), 895–904. doi:https://doi.org/10.1136/jech.55.12.895
- Grundy, E., & Sloggett, A. (2003). Health inequalities in the older population: The role of personal capital, social resources and socio-economic circumstances. Social Science & Medicine, 56(5), 935–947. doi:https://doi.org/10.1016/S0277-9536(02)00093-X
- Hajek, A., & König, H.-H. (2016). Informal caregiving and subjective well-being: Evidence of a population-based longitudinal study of older adults in Germany. Journal of the American Medical Directors Association, 17(4), 300–305. doi:https://doi.org/10.1016/j.jamda.2015.10.015
- Ilinca, S., Rodrigues, R., & Schmidt, A. E. (2017). Fairness and eligibility to long-term care: An analysis of the factors driving inequality and inequity in the use of home care for older Europeans. International Journal of Environmental Research& Public Health, 14(10), 1224. doi:https://doi.org/10.3390/ijerph14101224
- Jivraj, S., & Nazroo, J. (2014). Determinants of socioeconomic inequalities in subjective well-being in later life: A cross-country comparison in England and the USA. Quality of Life Research, 23(9), 2545–2558. doi:https://doi.org/10.1007/s11136-014-0694-8
- Kaschowitz, J., & Brandt, M. (2017). Health effects of informal caregiving across Europe: A longitudinal approach. Social Science & Medicine, 173, 72–80. doi:https://doi.org/10.1016/j.socscimed.2016.11.036
- Litwin, H., Stoeckel, K. J., & Roll, A. (2014). Relationship status and depressive symptoms among older co-resident caregivers. Aging & Mental Health, 18(2), 225–231. doi:https://doi.org/10.1080/13607863.2013.837148
- Niedzwiedz, C. L., Richardson, E. A., Tunstall, H., Shortt, N. K., Mitchell, R. J., & Pearce, J. R. (2016). The relationship between wealth and loneliness among older people across Europe: Is social participation protective?Preventive Medicine, 91, 24–31. doi:https://doi.org/10.1016/j.ypmed.2016.07.016
- Pavot, W., & Diener, E. (1993a). Review of the satisfaction with life scale. Psychological Assessment, 5(2), 164–172. doi:https://doi.org/10.1037/1040-3590.5.2.164
- Pavot, W., & Diener, E. (1993b). The affective and cognitive context of self-reported measures of subjective well-being. Social Indicators Research, 28(1), 1–20. doi:https://doi.org/10.1007/BF01086714
- Pearlin, L. I., Mullan, J. T., Semple, S. J., & Skaff, M. M. (1990). Caregiving and the stress process: An overview of concepts and their measures. The Gerontologist, 30(5), 583–594. doi:https://doi.org/10.1093/geront/30.5.583
- Pinquart, M., & Sörensen, S. (2000). Influences of socioeconomic status, social network, and competence on subjective well-being in later life: A meta-analysis. Psychology & Aging, 15(2), 187. doi:https://doi.org/10.1037//0882-7974.15.2.187
- Pongiglione, B., De Stavola, B. L., & Ploubidis, G. B. (2015). A systematic literature review of studies analyzing inequalities in health expectancy among the older population. PloS One, 10(6), e0130747. doi:https://doi.org/10.1371/journal.pone.0130747
- Rafnsson, S. B., Shankar, A., & Steptoe, A. (2017). Informal caregiving transitions, subjective well-being and depressed mood: Findings from the English Longitudinal Study of Ageing. Aging & Mental Health, 21(1), 104–112. doi:https://doi.org/10.1080/13607863.2015.1088510
- Read, S., Grundy, E., & Foverskov, E. (2016). Socio-economic position and subjective health and well-being among older people in Europe: A systematic narrative review. Aging & Mental Health, 20(5), 529–542. doi:https://doi.org/10.1080/13607863.2015.1023766
- Rueda, S., Artazcoz, L., & Navarro, V. (2008). Health inequalities among the elderly in Western Europe. Journal of Epidemiology & Community Health, 62(6), 492–498. doi:https://doi.org/10.1136/jech.2006.059279
- Saito, T., Kondo, N., Shiba, K., Murata, C., & Kondo, K. (2018). Income-based inequalities in caregiving time and depressive symptoms among older family caregivers under the Japanese long-term care insurance system: A cross-sectional analysis. PLoS One, 13(3), e0194919. doi:https://doi.org/10.1371/journal.pone.0194919
- Schöllgen, I., Huxhold, O., & Tesch-Römer, C. (2010). Socioeconomic status and health in the second half of life: Findings from the German Ageing Survey. European Journal of Ageing, 7(1), 17–28. doi:https://doi.org/10.1007/s10433-010-0140-x
- Schram, J., Schuring, M., Oude Hengel, K. M., & Burdorf, A. (2019). Health-related educational inequalities in paid employment across 26 European countries in 2005–2014: Repeated cross-sectional study. BMJ Open, 9(5), e024823. doi:https://doi.org/10.1136/bmjopen-2018-024823
- Stuck, S., Zuber, S., Franzese, F., Gruber, S., Birkenbach, T., Pflüger, S.-M., & Atzendorf, J. (2019). SHARE release guide 7.0.0. Munich Center for the Economics of Aging (MEA) at the Max Planck Institute for Social Law and Social Policy.
- Swinkels, J. C., Suanet, B., Deeg, D. J. H., & Broese van Groenou, M. (2016). Trends in the informal and formal home-care use of older adults in the Netherlands between 1992 and 2012. Ageing & Society, 36(9), 1870–1890. doi:https://doi.org/10.1017/S0144686X1500077X
- Tokunaga, M., & Hashimoto, H. (2017). The socioeconomic within-gender gap in informal caregiving among middle-aged women: Evidence from a Japanese nationwide survey. Social Science & Medicine, 173, 48–53. doi:https://doi.org/10.1016/j.socscimed.2016.11.037
- Tough, H., Brinkhof, M. W. G., Siegrist, J., & Fekete, C. (2020). Social inequalities in the burden of care: A dyadic analysis in the caregiving partners of persons with a physical disability. International Journal for Equity in Health, 19(1), 3. doi:https://doi.org/10.1186/s12939-019-1112-1
- Verbakel, E. (2014). Informal caregiving and well-being in Europe: What can ease the negative consequences for caregivers?Journal of European Social Policy, 24(5), 424–441. doi:https://doi.org/10.1177/0958928714543902
- Verbakel, E., Metzelthin, S. F., & Kempen, G. I. J. M. (2018). Caregiving to older adults: Determinants of informal caregivers’ subjective well-being and formal and informal support as alleviating conditions. The Journals of Gerontology. Series B, Psychological Sciences & Social Sciences, 73(6), 1099–1111. doi:https://doi.org/10.1093/geronb/gbw04
- Wagner, M., & Brandt, M. (2018). Long-term care provision and the well-being of spousal caregivers: An analysis of 138 European regions. The Journals of Gerontology Series B: Psychological Sciences & Social Sciences, 73(4), e24–e34. doi:https://doi.org/10.1093/geronb/gbx133