
Abstract
Objective
This rapid review aims to identify the types of technologies used by people with dementia and their supporters during the COVID-19 pandemic, and the issues which influenced technology adoption within their usual care routines.
Methods
PubMed, PsychInfo, Scopus, and Cochrane COVID reviews were searched to identify peer-review studies published since 2020. A total of 18 studies were included and synthesised thematically.
Results
Of these, most were conducted in the community (n = 15) with people with dementia only (n = 11) and involved qualitative methods (n = 11). The majority (n = 12) focused on digital off-the-shelf and low-cost solutions, such as free video conferencing platforms, to access care, socialise or take part in interventions. Whilst often well-accepted and associated with positive outcomes (such as improved social connectedness), lack of digital literacy or support to use technologies, limited access to appropriate technology, individuals’ physical, cognitive, or sensory difficulties, were highlighted and likely to threaten the adoption of these solutions. The quality of the evidence was mixed, neither very robust nor easily generalisable which may be attributed to the challenges of conducting research during the pandemic or the need to rapidly adapt to a new reality.
Conclusion
While COVID-19 has fast-tracked the adoption of technology, its use is likely to continue beyond the pandemic. We need to ensure this technology can leverage dementia support and care and that people with dementia are enabled and empowered to use it.
Introduction
In the last two years, there has been increased evidence of the impact of COVID-19 and related restrictions on people with dementia and their supporters (the latter term is used throughout this review to refer to informal caregivers, such as families and/or friends. This term was preferred by people with dementia consulted for this work). The control and safety measures instituted in most countries to mitigate the viral spread, such as physical distancing, stay-at-home and curfew orders, and travel restrictions have negatively impacted people’s lives. They have disrupted people’s well-established daily routines, reduced social interactions and usual support networks, and limited access to vital support services. The impact of these measures has been felt harder by people with dementia, who are particularly vulnerable to isolation and stimulus deprivation (Giebel et al., Citation2021a; Hanna et al., Citation2022; Suárez-González et al., Citation2020; Tuijt et al., Citation2021a). People with dementia faced an increased risk of social isolation and negative health outcomes such as worsening symptoms and severe behavioural disturbances, and increased cognitive and functional decline (Manca et al., Citation2020; Numbers & Brodaty, Citation2021). Along with these, challenges faced by family supporters have also increased, raising concerns about their mental well-being (Wei et al., Citation2022).
The mainstay of COVID-19 management has relied on containment and mitigation strategies, implying that various types of activities (e.g. shopping, working, and leisure) were interrupted with many shifting from in person to online (Talbot & Briggs, Citation2022). This has resulted in an accelerated spread and use of assistive and everyday technology.
Assistive technology refers to ‘any item, piece of equipment, product or system whether acquired commercially, off-the-shelf, modified or customised, that is used to help persons with disability’ (ISO, Citation2011). Assistive and everyday technology can play an important role in promoting independent living, safety, and autonomy of people with dementia, and supporting the quality of life of this population and their supporters (Gibson et al., Citation2015; van der Roest et al., Citation2017). Technologies for assisting people with dementia and/or their supporters can be categorised into: memory support, treatment and interventions, safety and security, training, care delivery, social interaction and networking (Carretero, Citation2015; Lorenz et al., Citation2019).
Assistive technology has been claimed to be of great value to help manage and respond to current and future dementia care issues, such as care staff shortages. Studies have shown that the pandemic has heightened the need for and boosted the uptake of assistive and everyday technology in various social and health domains for people with special needs (Layton et al., Citation2021). It is not clear, however, whether uptake of technology in dementia care has increased and what its impact is.
The aim of this rapid review was therefore to explore how people with dementia and their supporters have been using assistive and everyday technology during the COVID-19 pandemic. We wish to identify the types of technologies used by people with dementia and their supporters at any stage of the disease trajectory, and the factors that influenced technology adoption within their usual care routines. Specifically, this rapid review sought to answer the following questions:
What technologies used by people with dementia and their supporters have been subjected to research during the COVID-19 pandemic?
What is the impact of technologies used during the COVID- 19 pandemic on people with dementia and their supporters?
How has the uptake of technologies by people with dementia and their supporters changed during the COVID-19 pandemic?
What is the current knowledge about the acceptability, facilitators and barriers that affect the effective use of technologies by people with dementia and their supporters during the COVID- 19 pandemic?
The pandemic reminded us all how rapidly things can change. Evidence gathered during COVID-19 must be synthesised without undue delays to avoid the risk of getting outdated. In such circumstances, rapid reviews are recommended by the World Health Organisation (WHO) (Tricco et al., Citation2017). Through this rapid review we expect to gather actionable evidence to fuel the discussion on care practice innovation, contribute to expanding knowledge on the topic, and increase public awareness of technologies and its role in dementia care during unprecedented times.
Materials and methods
The protocol of this review was registered in PROSPERO (CRD42022298935) and conducted as part of a larger project led by the INTERDEM taskforce on assistive technology. Two experts by experience (i.e. people with dementia) were consulted at different points during the development of this review. We used recommended general guidance for rapid reviews to support the conduct of this work (Garritty et al., Citation2021). The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) checklist (Page et al., Citation2021) was used as a basis for the reporting.
Eligibility criteria
Studies were selected according to the inclusion and exclusion criteria outlined below.
Participants
Participants included people with dementia (all types) and their supporters (i.e. family and/or friends that provide informal care). While not all individuals with mild cognitive impairment (MCI) will progress to dementia, MCI may still be considered a prodromal or ‘pre-dementia’ stage and was therefore included in this review.
Intervention
Products included technological devices, such as computers, tablets, and reminders. Devices that were piloted and had not yet been commercialised were considered. Non-technological devices, such as basic aids (for example, walking sticks and grab rails), were excluded from the searches.
Context
Studies published since 2020, when the COVID-19 started, at all levels of social and healthcare settings (i.e. primary, secondary, and tertiary healthcare) or in the community were considered. Studies exclusively based on or reporting data obtained before the COVID-19 pandemic were excluded from this review.
Outcomes
Studies reporting on all outcomes pertaining to patients and their supporters’ health, quality of life and related constructs, and that were associated with the use of technologies were considered. These outcomes come directly from participants and may be measured using a variety of tools and instruments.
Study design
Reviews (all types), randomised controlled trials, cohort studies, case studies, and cross-sectional studies published in peer-review journals were included. Conference abstracts were not deemed appropriate to be included in this rapid review as most of these are not peer-reviewed. In addition, identifying relevant conferences, and locating their abstracts can be time and resource-intensive which contradicts the purpose of a rapid review.
Information sources
A rapid electronic search strategy was used to identify English, Spanish, Portuguese, Dutch, and German published studies and indexed in the following databases: PubMed, PsychInfo, Scopus, and Cochrane COVID reviews. We searched for studies published since 2020, when the COVID-19 pandemic started. Reference lists of the identified papers were checked to ensure that relevant eligible studies were not excluded.
Search strategy
The following terms were developed with the support of a professional librarian and piloted and optimised before being used in the current review:
(dementia or alzheimers or cognitive impairment or memory loss) AND (technology or technological or technologies) AND (COVID-19 or coronavirus or 2019-ncov or sars-cov-2 or cov-19). The detailed search strategy for the three first databases is fully reported in Appendix A.
Selection process
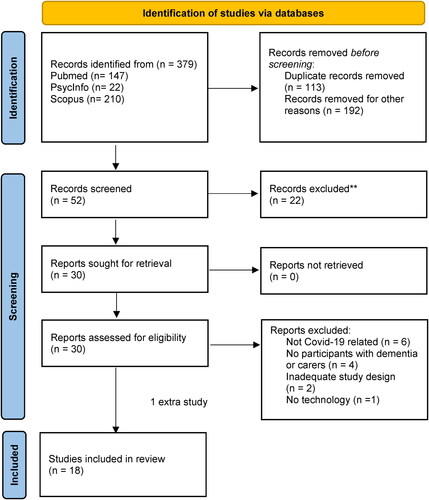
References identified were exported and managed with the EndNote software. Searches were conducted by one review author (AB) who also screened the titles and abstracts of all identified references. Duplicates and titles and abstracts that did not meet the inclusion criteria were excluded. For records where eligibility was unclear, the full texts were obtained and scrutinised. The full text of all reports marked as include or unsure were retrieved by one reviewer (AB) and assessed for eligibility independently by two other researchers (MC and CS). Any disagreement between them was resolved through discussion with the whole team. Reasons for exclusion were recorded as part of the screening process ().
Figure 1. PRISMA flow diagram (Page et al., 2021).
Data charting process
A standard, pre-piloted form was used to extract data from the included studies for evidence synthesis. Extracted information included: study setting, country, design, type of patient and public involvement, and details of the technologies, including function, stage of development, target beneficiaries, outcomes and ethical issues, and limits regarding the uptake of technologies. Two review authors independently extracted data (ARF and FMH). Discrepancies were solved by consensus, referral to a third review author (LF) or to the wider team. The authors of the primary studies were contacted if further information was deemed necessary. An author was contacted but no answer was received.
Risk of bias assessment
One reviewer (AB) assessed the methodological quality of eligible studies using the latest Mixed Methods Appraisal Tool (Hong et al., Citation2018) and results were discussed with all authors. The MMAT is a generic critical appraisal tool that covers qualitative, quantitative, and mixed methods research studies. The tool is considered appropriate for this review given the anticipated heterogeneity of study designs to be included.
An overall score was calculated for each study. The scores are presented in using stars (*): 5***** or 100% quality criteria met; 4 **** or 80% quality criteria met; 3 *** or 60% quality criteria met; 2 ** or 40% quality criteria met; 1 * or 20% quality criteria met. No studies were excluded based on this assessment. The decision whether each item was fulfilled or not was based on the information provided in the paper. The MMAT can be seen in Appendix B.
Table 1. Studies included in the rapid review.
Synthesis methods
Given the broad scope of the review, a wide range of study designs were included. A formal statistical meta-analysis was not deemed appropriate. Instead, results were summarised in tabular and narrative form. All quantitative and qualitative data were analysed using thematic synthesis and organised according to the questions posed by the review. The thematic synthesis comprised three stages: 1) two reviewers (CS and MC) first analysed the abstracts of each included article and developed a list of codes and key findings. This list was updated and adjusted by two other reviewers (AF and FMH) during data extraction and revised by all authors; 2) similarities between codes were identified. Codes were grouped into ‘themes’ that captured and described patterns in the data across studies; 3) in a group discussion, all authors finally interpreted the meaning of each theme in relation to the research questions and a narrative description for each one of them was provided.
Results
A total of 379 records were initially identified through database search. Duplicates were removed (n = 113) and the titles of the remaining records reviewed. Of these, 52 records were considered appropriate for further screening. The abstracts of these 52 records were reviewed and studies that did not meet the inclusion criteria were excluded. This left 30 full-text articles to be assessed for eligibility. At this stage, reports were excluded based on varying reasons: not COVID-19 related; population that did not suit the inclusion criteria; study design that did not meet the inclusion criteria; no technology assessed. This led to a total of 17 records for final inclusion. The search was repeated three months later, prior to the start of analysis, and one further study was identified and included in this review (Talbot & Briggs, Citation2022; ).
Characteristics of the included studies
The geographical scope of the included studies was varied, with five studies from each of United States of America (USA) and United Kingdom (UK) and one study from each of eight other countries: Brasil, Canada, Chile, Italy, Japan, Norway, South Korea, and Spain. All were published in English. Most studies used descriptive cross-sectional designs (n = 16). Of these, eight were qualitative, five quantitative and three used mixed methods. Two interventional studies were included - a randomised controlled trial (Park et al., Citation2021) and a pre-post quasi experimental study (Yahara et al., Citation2021). The effect sizes were omitted in most quantitative studies. Most studies were conducted in the community (n = 15); two reported data from care homes (Park et al., Citation2021; Yahara et al., Citation2021) and one from both institutional and community contexts (Giebel et al., Citation2021b). Ten studies involved people with dementia only, six included both people with dementia and their family supporters, and two were concerned with family supporters only. Four studies targeted people with mild cognitive impairment (Farhang et al., Citation2022; Goodman-Casanova et al., Citation2020; Park et al., Citation2021; Yahara et al., Citation2021). Talbot and Briggs (Citation2022) involved people living with mild-to-moderate dementia; the severity of dementia was not clearly reported in the remaining studies.
The level of public involvement (PPI) was limited. In four studies, the PPI can be mainly described as advisory/consultative, as per the National Institute for Health Research (NIHR) categorisation. People with dementia contributed to the designing of interview topics (Giebel et al., Citation2021b) and session themes (Mattos et al., Citation2021), piloting and refining a survey (Tam et al., Citation2021), and in providing feedback on draft interview guides (Tuijt et al., Citation2021b). The remaining studies did not report on PPI.
Reference to ethical issues was scarce and limited to: dilemmas between promoting autonomy and avoiding risk, or maintaining privacy (Mattos et al., Citation2021; Tam et al., Citation2021) and increasing safety measures (Farhang et al., Citation2022) difficulties in obtaining informed consent when people with dementia do not understand or are unaware of the presence of the technology (Masoud et al., Citation2021); and safety-netting concerns around collecting data online (Quail et al., Citation2021), as this may not clearly detect causes for distress and restlessness. The quality of the evidence was mixed, and neither robust nor easily generalisable.
Type and impact of technologies
Three studies focused on the use of non-specific digital technologies during the pandemic (Gedde et al., Citation2021; Giebel et al., Citation2021b; Talbot & Briggs, Citation2022). The remaining studies involved: i) Video conferencing or telephone for social connection, remote consultations, and intervention delivery (Arighi et al., Citation2021; Collins et al., Citation2021; Farhang et al., Citation2022; Iyer et al., Citation2021; Kalicki et al., Citation2021; Masoud et al., Citation2021; Mattos et al., Citation2021; Quail et al., Citation2021; Tam et al., Citation2021; Tuijt et al., Citation2021a; Weems et al., Citation2021; Yahara et al., Citation2021) ii) Robots - Humanoid (Park et al., Citation2021) and Pet robots (van Orden et al., Citation2022); and iii) Telemedicine (Goodman-Casanova et al., Citation2020).
The framework by Carretero (Citation2015) and Lorenz et al. (Citation2019) was used to organise the technologies by typology. The largest number of technologies identified in the literature were within the categories ‘treatment and interventions’ (Mattos et al., Citation2021; Park et al., Citation2021; Quail et al., Citation2021; van Orden et al., Citation2022; Weems et al., Citation2021; Yahara et al., Citation2021) and ‘care delivery’ (Arighi et al., Citation2021; Collins et al., Citation2021; Goodman-Casanova et al., Citation2020; Iyer et al., Citation2021; Kalicki et al., Citation2021; Tuijt et al., Citation2021b), followed by ‘social interaction and networking’ (Farhang et al., Citation2022; Masoud et al., Citation2021; Tam et al., Citation2021).
Treatment and interventions (n = 6). This category covers technologies that are intended to provide psychosocial support and improve participants’ wellbeing.
One study focused on pet robots to promote socialisation (van Orden et al., Citation2022). The study shows that robotic pets can help reduce loneliness and anxiety and increase socialisation by promoting positive group interactions and experiences (van Orden et al., Citation2022). Park et al. (Citation2021) evaluated the impact of a robot-assisted cognitive training programme. Compared to traditional cognitive training, this programme, conducted over 6 weeks with people living with MCI, showed a greater effect on depression and global cognitive function in the short-term. Positive effects were also reported for language production, memory, and attention (Park et al., Citation2021).
Yahara et al. (Citation2021) evaluated the use of remote reminiscence and Quail et al. (Citation2021) a remote therapeutic intervention which included amongst others, cognitive stimulation activities, reminiscence, and music therapy, to improve general cognition. Short-term benefits on people with dementia included reduced apathy, better mood, cognition, and engagement (Quail et al., Citation2021). No significant differences were found between remote reminiscence and face-to-face reminiscence, with the former also showing a reduction in supporters’ anxiety and burden (Yahara et al., Citation2021).
The two studies targeting supporters were focused on distance support groups aiming to provide emotional support and to minimise the impact of COVID-19 pandemic on their mental health (Mattos et al., Citation2021; Weems et al., Citation2021). These studies showed that remote support groups can be an important tool to access information and guidance concerning dementia and improve families’ self-care. They were well received by supporters and a positive impact on emotional state and well-being was reported, together with a reduction of social isolation and loneliness (Mattos et al., Citation2021).
Care delivery (n = 6). The category ‘care delivery’ covers telecare and telehealth interventions. Technologies classified under this category aimed to facilitate direct contact and exchange of relevant information between professionals, people with dementia and their supporters. Five studies used remote consultations with care professionals via telephone (Tuijt et al., Citation2021b), video (Arighi et al., Citation2021; Kalicki et al., Citation2021) or both (Collins et al., Citation2021; Iyer et al., Citation2021). Collins et al. (Citation2021) refer that most participants in their study opted for video conference consultations as an alternative to telephone consultations. Reasons included increased ability to visualise the context and to enable the entire care team to meet the patient at the same time (Iyer et al., Citation2021). Collins et al. (Citation2021) suggest that people using video conferences tend to be younger than those using telephone. According to the study conducted by Kalicki et al. (Citation2021) in the USA, FaceTime was the most used platform for video conferences.
A further study (Goodman-Casanova et al., Citation2020) investigated a television-based platform service designed to provide telecare services at home using the TV. Whilst no differences were seen in health and wellbeing, the potential of the product to enhance recreation levels was highlighted.
Social interaction and networking (n = 3). This category includes technologies that used distance communication, via mobile phone or Internet applications, or online platforms to exchange experiences (Lorenz et al., Citation2019). They can play an important role for people with dementia and their supporters by supporting the maintenance of social interactions despite the COVID-19 related stay-at-home orders and travel restrictions.
Masoud et al. (Citation2021) report on the experiences of those who have attended virtual Memory Cafes. Farhang et al. (Citation2022) and Tam et al. (Citation2021) explored the experiences of living with dementia during the pandemic, reflecting on the use of phone and video calls to maintain social connectedness. Participants in these studies considered technology essential to promote social connectedness (Giebel et al., Citation2021b; Masoud et al., Citation2021; Talbot & Briggs, Citation2022). Overall, people with dementia and their supporters reported feeling comfortable using technology to connect with others, however, both groups reported that virtual connections did not feel the same as in-person (Tam et al., Citation2021). Some people with dementia reported a struggle to manage online conversations (Talbot & Briggs, Citation2022). While people with dementia have demonstrated ability to learn technological skills, they also expressed a need for training on how to use digital technologies. In Talbot and Briggs (Citation2022), dementia-friendly leaflets containing information on how to use technologies, such as Zoom, was mentioned as a specific helpful resource (Talbot & Briggs, Citation2022).
Uptake of technologies during COVID-19
Only two of the identified studies focused on the changes in the use of technologies by people living with dementia and their supporters during the COVID-19 pandemic (Gedde et al., Citation2021; Kalicki et al., Citation2021). Gedde et al. (Citation2021) provide a snapshot of access to assistive technology by people living with dementia and their family supporters before and during the pandemic. The study, involving 126 dyads (people with dementia and family supporters), showed that 14% of the family supporters reported more digital contact with people living with dementia, and approximately 20% showed increased interest in technologies. In a study conducted in USA, Kalicki et al. (Citation2021) reported that 35% of 310 people living with dementia in the community engaged in video-based telehealth encounters for the first time during the pandemic.
Facilitators and barriers
Thirteen studies identified several factors that affected the use of technologies during the pandemic. These were categorised into barriers and facilitators related to the technology itself, the individuals using the technology and their supporters.
Technology-related factors
Participants expressed a high degree of satisfaction over convenience (Collins et al., Citation2021; Weems et al., Citation2021), time efficiency, adaptability (i.e. ability to minimise time away from families and friends) (Weems et al., Citation2021) and cost savings of technologies (Iyer et al., Citation2021). However, studies also identified several technology-related barriers. Most barriers were related to poor internet connection and lack of access to technology (Farhang et al., Citation2022; Iyer et al., Citation2021; Masoud et al., Citation2021; Mattos et al., Citation2021; Quail et al., Citation2021; Tam et al., Citation2021; Weems et al., Citation2021), followed by studies reporting that technology uptake did not exempt the help or presence of a caregiver or assistant (Giebel et al., Citation2021b; Kalicki et al., Citation2021; Park et al., Citation2021; Quail et al., Citation2021; Tuijt et al., Citation2021b). Four studies reported the lack of capable devices (including old computers or devices without cameras) (Iyer et al., Citation2021; Kalicki et al., Citation2021; Masoud et al., Citation2021; Mattos et al., Citation2021), and one mentioned lack of guidance on digitally delivered assessment and care (Quail et al., Citation2021). Four studies raised questions related to experiences of impersonal care delivery and interaction (Masoud et al., Citation2021; Mattos et al., Citation2021; Quail et al., Citation2021; Weems et al., Citation2021), and one study (van Orden et al., Citation2022) mentioned emotional implications that should be safeguarded when using robot companion pets, including the degree to which adults believe the robotic pets to be real.
Kalicki et al. (Citation2021) found that care professionals were often unaware of these non-medical barriers to telehealth access. In addition, Giebel et al. (Citation2021b) noted that few community and institutionalised dementia care services in the UK were able to provide support via technology. Of those that did, many were delayed in getting set up, leaving people with dementia in need of support for some time.
Individual-related factors
The most frequently reported individual-level barriers comprised difficulties with technology use, either due to unfamiliarity, lack of experience and knowledge about technology use, or digital illiteracy (Farhang et al., Citation2022; Gedde et al., Citation2021; Giebel et al., Citation2021b; Iyer et al., Citation2021; Mattos et al., Citation2021; Park et al., Citation2021; Quail et al., Citation2021; Talbot & Briggs, Citation2022; Tam et al., Citation2021; Tuijt et al., Citation2021b; Weems et al., Citation2021). Compared to people with dementia, supporters reported less issues when using technology, including less problems logging in or in understanding how the technology works (Tam et al., Citation2021).
Difficulties related to the dementia and dementia stage, including cognitive impairment and behavioural disturbances (Iyer et al., Citation2021; Kalicki et al., Citation2021; Masoud et al., Citation2021; Quail et al., Citation2021; Tuijt et al., Citation2021b) together with visual and hearing limitations (Giebel et al., 2021b; Iyer et al., Citation2021; Kalicki et al., Citation2021) were also common. Lack of interest by the person with dementia in using technology was reported by one study (Masoud et al., Citation2021), whereas another (Gedde et al., Citation2021) reported that only a minority of supporters (17%) showed an increased interest in technology under COVID-19 pandemic restrictions.
To overcome these barriers, people with dementia relied on their relatives to support them to use the technology (Tuijt et al., Citation2021b). Consequently, barriers related to time-consuming demands and the overburden of caregiving responsibilities were also mentioned by supporters (Mattos et al., Citation2021; Weems et al., Citation2021).
Discussion
Against a backdrop of unprecedented challenges in access, availability and utilisation of medical assistance, social support and care services, this rapid review aimed to explore how people with dementia and their supporters have been using technology during the COVID-19 pandemic.
Recent recommendations stress the importance of identifying the needs of those with dementia and their supporters in order to establish technological strategies for their assistance and support (Cuffaro et al., Citation2020). The studies included in this review focused on a variety of assistive and everyday technologies. The most common ones fell into the categories ‘treatment and interventions’ (technologies aiming to provide psychosocial support and improve participants’ wellbeing) and ‘care delivery’ (technologies aiming to facilitate direct contact and exchange of relevant information between professionals, people with dementia and their family supporters) and focusing on the remote delivery of care or psychosocial interventions. Available evidence on technology for supporters is focused on technology-based interventions i.e. remote programmes aiming to improve the provision of care. Supporters use these services to obtain information about their needs, to share experiences, and to get emotional support.
The above evidence shows that technology is often well-accepted by people with dementia and their supporters. It is associated with positive outcomes, including social connectedness, and improved mood, and can help to buffer the negative impacts of caregiving. Albeit the benefits that have been reported, several barriers are also highlighted and are likely to threaten the engagement and adoption of these solutions. These include lack of digital literacy or limited access to a supporter to assist with the technologies, limited access to appropriate technology, the overreliance on supporters’ abilities, and individuals’ cognitive or sensory impairments. Whilst the potential of technologies in alleviating caregiving burden, burden itself is reported by supporters to be a barrier to the use of technologies.
Overall, these barriers overlap with the ones identified in previous studies (Egan & Pot, Citation2016; Guisado-Fernández et al., Citation2019; Meiland et al., Citation2017), and suggest that there are common factors that undermine a more extensive adoption of assistive and everyday technologies. In this respect, one may expect that by targeting efforts to address these modifiable barriers the adoption of these solutions will likely be promoted and increased. Whilst these challenges also existed in a pre-pandemic era, they have become more apparent during COVID-19, due to an increased need for digital contact to overcome the reduced availability of community and in-person support services (Gedde et al., Citation2021; Kalicki et al., Citation2021). Although a huge effort was made to keep services running, in the UK, for example, Giebel et al. (Citation2021b) noted that many dementia care services were unable or were significantly delayed in setting up technology to support people during the pandemic. It became evident in the identified studies that only a minority of people with dementia were able to use the technologies independently; most participants needed assistance from an engaged supporter. Addressing technological issues (such as lack of internet access) and providing individual support when introducing a technology are encouraged, but difficult to meet during a pandemic. It is therefore recommended to fully use the time after the pandemic to design and implement technologies tailored to the needs of people with dementia, particularly to those that live alone or do not have supporters Over the next few years, clinicians, service providers and policymakers, should seize these opportunities to support the technological transformation in dementia care.
A minority of studies reported on new technologies; most have focused on existing, easily accessible, and low-cost everyday technologies that have been repurposed as an assistive technology during the COVID-19 to counteract the negative impact of the pandemic on people’s lives.
Studies conducted during the pandemic have been mostly targeted at people living at home in the community rather than in institutional care settings. People with dementia living in care settings were among the most severely affected by the pandemic. The vulnerability of this population means that they often rely on personal assistance when using technology. Restrictions imposed by the pandemic, such as physical distancing, may have deprived people of the support needed to use some technologies, whilst increasing the use of others. Adding to this, the visiting restrictions, together with the problems posed by the pandemic itself, made it difficult for care settings to take part in research. This same reason, together with differences between countries when it comes to involvement of experts by experience in research, may have accounted for the limited scope of PPI found in the studies. Prior research has already highlighted the pitfalls of deploying technological solutions without proper validation by their target population, pointing to the need for user-centred design and user testing of solutions, particularly if these are aimed at people with dementia and their caregivers (Behera et al., Citation2021; Evans et al., Citation2015; Øksnebjerg et al., Citation2020; Rai et al., Citation2020). Despite the pandemic-related challenges, we believe the active involvement of people with dementia and their supporters in different stages of the research was still viable. Experts by experience, particularly those living in the community, could have been sourced through national organisations that provide involvement opportunities for patients and the public.
A rapid review was deemed to be the most appropriate method to gather timely evidence related to COVID-19. A systematic review investigating the effectiveness of technologies to support people with dementia and their supporters would provide a full overview over the field, but it could be outdated by the time it would be made available.
In addition, this review provides a retrospective snapshot of what has been researched rather than reflecting the current picture and what the future might hold. Several technologies may have been developed and implemented but not reported due to COVID-19 constraints. Furthermore, this synthesis may be limited by the broad scope of the theme, that led to the inclusion of studies with diverse designs, methods, and outcomes. In particular, the use of various outcome measures made it hard to compare results across studies. This suggests the need for a more judicious application of standardised measures that will support clinicians and researchers to understand how technology can be used to overcome the immediate and long-term needs of people with dementia and their supporters. Also, the effect sizes were omitted in most quantitative studies, meaning that the magnitude of differences is often unaddressed. Most studies were conducted in the USA and UK which also hinders generalisation, as some of the technologies available or in common use may differ between countries (for example, FaceTime is prevalent in USA).
Finally, identifying the stages of dementia for which the reported technologies were intended was problematic as this was not clearly or consistently reported in the studies. As people with dementia represent a heterogeneous group, it would have been valuable to map technologies against types of dementia, as they present different needs. For example, compared to Alzheimer’s Disease and other common types of dementia, people with Posterior Cortical Atrophy (PCA) usually have quite well-preserved memory but are more likely to experience difficulties with vision. This can potentially pose different and additional challenges on using technology (e.g. finding it difficult to engage or to recognise people in an online meeting).
Despite these limitations, frameworks were used to frame and synthetise evidence regarding typology of technologies and PPI, which are believed to strengthen the intelligibility and replicability of our methodology. In addition, the review team consisted of dementia researchers from a range of disciplines from different health and social backgrounds. Screening, full-text review, and data extraction were performed independently by at least two reviewers, minimising the potential for single-reviewer bias, while we have also reduced the potential for selection bias by using a broad comprehensive search strategy. With this we expect the rapid review can contribute to expanding knowledge on the topic and increase public awareness of technologies and its role in dementia care.
Conclusion
Evidence generated during the COVID-19 pandemic suggests that off-the-shelf and low-cost solutions, including online platforms, have been used by people with dementia and their supporters to respond to the negative impacts of physical and social restrictions imposed by the pandemic. While the pandemic has fast-tracked the adoption of this technology, its use is likely to continue beyond the pandemic. Future studies should be targeted at the age-related digital divide, as well as at health-related conditions such as sensory impairments that are likely to be experienced by the end users of such technologies. It became evident that only a minority of people with dementia were able to use the technologies independently. Future studies need to ensure that technologies can leverage dementia support and care and that people with dementia are enabled and empowered to use it.
Acknowledgements
We would like to thank Helen Rochford-Brennan (HRB) and Nigel Hullah (NH) – experts by experience – for sharing their experience with us throughout this review. We are also very grateful for the input provided by Dianne Gove (DG) and Ana Diaz (AD). MPC is supported by the NIHR MindTech, MedTech Co-operative and NIHR Nottingham Biomedical Research Centre.
Disclosure statement
No potential conflict of interest was reported by the authors.
Correction Statement
This article has been corrected with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
References
- Arighi, A., Fumagalli, G. G., Carandini, T., Pietroboni, A. M., Riz, M., de, A., Galimberti, D., & Scarpini, E. (2021). Facing the digital divide into a dementia clinic during COVID-19 pandemic: Caregiver age matters. Neurological Sciences: Official Journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology, 42(4), 1247–1251.https://doi.org/10.1007/s10072-020-05009-w
- Behera, C. K., Condell, J., Dora, S., Gibson, D. S., & Leavey, G. (2021). State-of-the-art sensors for remote care of people with dementia during a pandemic: A systematic review. Sensors, 21(14), 4688. https://doi.org/10.3390/s21144688
- Carretero, S. (2015). Mapping of effective technology-based services for independent living for older people at home: Deliverable 1. Luxembourg, Publications Office, Shaping Europe’s digital future (europa.eu)
- Collins, J. T., Mohamed, B., & Bayer, A. (2021). Feasibility of remote Memory Clinics using the plan, do, study, act (PDSA) cycle. Age and Ageing, 50(6), 2259–2263. https://doi.org/10.1093/ageing/afab173
- Cuffaro, L., Di Lorenzo, F., Bonavita, S., Tedeschi, G., Leocani, L., & Lavorgna, L. (2020). Dementia care and COVID-19 pandemic: A necessary digital revolution. Neurological Sciences: Official Journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology, 41(8), 1977–1979.https://doi.org/10.1007/s10072-020-04512-4
- Egan, K. J., & Pot, A. M. (2016). Encouraging innovation for assistive health technologies in dementia: Barriers, enablers, and next steps to be taken. Journal of the American Medical Directors Association, 17(4), 357–363.https://doi.org/10.1016/j.jamda.2016.01.010
- Evans, J., Brown, M., Coughlan, T., Lawson, G., & Craven, M. P. (2015). A systematic review of dementia focused assistive technology. In M. Kurosu (Ed.), Human-Computer Interaction: Interaction Technologies; 17th International Conference, HCI International 2015, Los Angeles, CA, USA, August 2 - 7, 2001; Proceedings, Part II. Springer, pp. 406–417.
- Farhang, M., Miranda-Castillo, C., Behrens, M. I., Castillo, E., Mosquera Amar, S., & Rojas, G. (2022). Impact of social isolation and coping strategies in older adults with mild cognitive impairment during the Covid-19 pandemic: A qualitative study. Aging & Mental Health, 26(7), 1395–1416. https://doi.org/10.1080/13607863.2021.1958145
- Garritty, C., Gartlehner, G., Nussbaumer-Streit, B., King, V. J., Hamel, C., Kamel, C., Affengruber, L., & Stevens, A. (2021). Cochrane Rapid Reviews Methods Group offers evidence-informed guidance to conduct rapid reviews. Journal of Clinical Epidemiology, 130, 13–22.https://doi.org/10.1016/j.jclinepi.2020.10.007
- Gedde, M. H., Husebo, B. S., Erdal, A., Puaschitz, N. G., Vislapuu, M., Angeles, R. C., & Berge, L. I. (2021). Access to and interest in assistive technology for home-dwelling people with dementia during the COVID-19 pandemic (PAN.DEM). International Review of Psychiatry (Abingdon, England), 33(4), 404–411.https://doi.org/10.1080/09540261.2020.1845620
- Gibson, G., Dickinson, C., Brittain, K., & Robinson, L. (2015). The everyday use of assistive technology by people with dementia and their family carers: A qualitative study. BMC Geriatrics, 15(89), 89.https://doi.org/10.1186/s12877-015-0091-3
- Giebel, C., Cannon, J., Hanna, K., Butchard, S., Eley, R., Gaughan, A., Komuravelli, A., Shenton, J., Callaghan, S., Tetlow, H., Limbert, S., Whittington, R., Rogers, C., Rajagopal, M., Ward, K., Shaw, L., Corcoran, R., Bennett, K., & Gabbay, M. (2021a). Impact of COVID-19 related social support service closures on people with dementia and unpaid carers: A qualitative study. Aging & Mental Health, 25(7), 1281–1288.https://doi.org/10.1080/13607863.2020.1822292
- Giebel, C., Hanna, K., Callaghan, S., Cannon, J., Butchard, S., Shenton, J., Komuravelli, A., Limbert, S., Tetlow, H., Rogers, C., Eley, R., Rajagopal, M., Ward, K., & Gabbay, M. (2021b). Navigating the new normal: Accessing community and institutionalised care for dementia during COVID-19. Aging & Mental Health, 26(5), 905–910. https://doi.org/10.1080/13607863.2021.1914545
- Goodman-Casanova, J. M., Dura-Perez, E., Guzman-Parra, J., Cuesta-Vargas, A., & Mayoral-Cleries, F. (2020). Telehealth home support during covid-19 confinement for community-dwelling older adults with mild cognitive impairment or mild dementia: Survey study. Journal of Medical Internet Research, 22(5), e19434.https://doi.org/10.2196/19434
- Guisado-Fernández, E., Giunti, G., Mackey, L. M., Blake, C., & Caulfield, B. M. (2019). Factors influencing the adoption of smart health technologies for people with dementia and their informal caregivers: Scoping review and design framework. JMIR Aging, 2(1), e12192.https://doi.org/10.2196/12192
- Hanna, K., Giebel, C., Tetlow, H., Ward, K., Shenton, J., Cannon, J., Komuravelli, A., Gaughan, A., Eley, R., Rogers, C., Rajagopal, M., Limbert, S., Callaghan, S., Whittington, R., Butchard, S., Shaw, L., & Gabbay, M. (2022). Emotional and mental wellbeing following covid-19 public health measures on people living with dementia and carers. Journal of Geriatric Psychiatry and Neurology, 35(3), 344–352. https://doi.org/10.1177/0891988721996816
- Hong, Q. N., Pluye, P., Fàbregues, S., Bartlett, G., Boardman, F., Cargo, M., Dagenais, P., Gagnon, M.-P., Griffiths, F., Nicolau, B., O’Cathain, A., Rousseau, M.-C., & Vedel, I. (2018). Mixed Methods Appraisal Tool (MMAT), version 2018. Registration of Copyright (#1148552). Canadian Intellectual Property Office.
- International Organization for Standardization (ISO). (2011). 9999:2011: Assistive products for persons with disability - Classification and terminology [Online]. http://www.iso.org/iso/catalogue_detail.htm?csnumber=50982.
- Iyer, S., Mehta, P., Weith, J., Hoang-Gia, D., Moore, J., Carlson, C., Choe, P., Sakai, E., & Gould, C. (2021). Converting a geriatrics clinic to virtual visits during covid-19: A case study. Journal of Primary Care & Community Health, 12, 21501327211000235. https://doi.org/10.1177/21501327211000235
- Kalicki, A. V., Moody, K. A., Franzosa, E., Gliatto, P. M., & Ornstein, K. A. (2021). Barriers to telehealth access among homebound older adults. Journal of the American Geriatrics Society, 69(9), 2404–2411.https://doi.org/10.1111/jgs.17163
- Layton, N., Mont, D., Puli, L., Calvo, I., Shae, K., Tebbutt, E., Hill, K. D., Callaway, L., Hiscock, D., Manlapaz, A., Groenewegen, I., & Sidiqi, M. (2021). Access to assistive technology during the Covid-19 global pandemic: Voices of users and families. International Journal of Environmental Research and Public Health, 18(21), 11273.https://doi.org/10.3390/ijerph182111273
- Lorenz, K., Freddolino, P. P., Comas-Herrera, A., Knapp, M., & Damant, J. (2019). Technology-based tools and services for people with dementia and carers: Mapping technology onto the dementia care pathway. Dementia (London, England), 18(2), 725–741.https://doi.org/10.1177/1471301217691617
- Manca, R., Marco, M., & Venneri, A. (2020). The impact of covid-19 infection and enforced prolonged social isolation on neuropsychiatric symptoms in older adults with and without dementia: A review. Frontiers in Psychiatry, 11, 585540.https://doi.org/10.3389/fpsyt.2020.585540
- Masoud, S. S., Meyer, K. N., Martin Sweet, L., Prado, P. J., & White, C. L. (2021). “We don’t feel so alone”: A qualitative study of virtual memory cafés to support social connectedness among individuals living with dementia and care partners during Covid-19. Frontiers in Public Health, 9, 660144. https://doi.org/10.3389/fpubh.2021.660144
- Mattos, E. B. T., Da Francisco, I. C., Pereira, G. C., & Novelli, M. M. P. C. (2021). Grupo virtual de apoio aos cuidadores familiares de idosos com demência no contexto da COVID-19. Cadernos Brasileiros de Terapia Ocupacional, 29, e2882. https://doi.org/10.1590/2526-8910.ctore2201
- Meiland, F., Innes, A., Mountain, G., Robinson, L., van der Roest, H., García-Casal, J., A., Gove, D., Thyrian, J., R., Evans, S., Dröes, R. M., Kelly, F., Kurz, A., Casey, D., Szcześniak, D., Dening, T., Craven, M. P., Span, M., Felzmann, H., Tsolaki, M., & Franco-Martin, M. (2017). Technologies to support community-dwelling persons with dementia: A position paper on issues regarding development, usability, effectiveness and cost-effectiveness, deployment, and ethics. JMIR Rehabilitation and Assistive Technologies, 4(1), e6376. https://doi.org/10.2196/rehab.6376
- Numbers, K., & Brodaty, H. (2021). The effects of the COVID-19 pandemic on people with dementia. Nature Reviews. Neurology, 17(2), 69–70. https://doi.org/10.1038/s41582-020-00450-z
- Øksnebjerg, L., Janbek, J., Woods, B., & Waldemar, G. (2020). Assistive technology designed to support self-management of people with dementia: User involvement, dissemination, and adoption: A scoping review. International Psychogeriatrics, 32(8), 937–953.https://doi.org/10.1017/S1041610219001704
- Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J., M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J., M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, … V. A., Whiting, Moher, D. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ (Clinical Research ed.), 372(71), n71. https://doi.org/10.1136/bmj.n71
- Park, E.-A., Jung, A.-R., & Lee, K.-A. (2021). The humanoid robot sil-bot in a cognitive training program for community-dwelling elderly people with mild cognitive impairment during the covid-19 pandemic: A randomized controlled trial. International Journal of Environmental Research and Public Health, 18(15), 8198.https://doi.org/10.3390/ijerph18158198
- Quail, Z., Bolton, L., & Massey, K. (2021). Digital delivery of non-pharmacological intervention programmes for people living with dementia during the COVID-19 pandemic. BMJ Case Reports, 14(6), e242550. https://doi.org/10.1136/bcr-2021-242550
- Rai, H., Cavalcanti, A., Yates, L., Schneider, J., & Orrell, M. (2020). Involvement of people with dementia in the development of technology-based interventions: Narrative synthesis review and best practice guidelines. Journal of Medical Internet Research, 22(12), e17531. https://doi.org/10.2196/17531
- Suárez-González, A., Comas-Herrera, A., & Livingston, G. (2020). Impact of COVID-19 on people living with dementia: Emerging international evidence. BMJ, 369, m2463. https://doi.org/10.1136/bmj.m2463
- Talbot, C. V., & Briggs, P. (2022). The use of digital technologies by people with mild-to-moderate dementia during the COVID-19 pandemic: A positive technology perspective. Dementia (London, England), 21(4), 1363–1380.https://doi.org/10.1177/14713012221079477
- Tam, M. T., Dosso, J. A., & Robillard, J. M. (2021). The impact of a global pandemic on people living with dementia and their care partners: Analysis of 417 lived experience reports. Journal of Alzheimer’s Disease: JAD, 80(2), 865–875.https://doi.org/10.3233/JAD-201114
- Tricco, A. C., Langlois, E. V., & Straus, S. E. (2017). Rapid reviews to strengthen health policy and systems: A practical guide. World Health Organization. https://apps.who.int/iris/bitstream/handle/10665/258698/9789241512763-eng.pdf
- Tuijt, R., Frost, R., Wilcock, J., Robinson, L., Manthorpe, J., Rait, G., & Walters, K. (2021a). Life under lockdown and social restrictions - the experiences of people living with dementia and their carers during the COVID-19 pandemic in England. BMC Geriatrics, 21(1), 301. https://doi.org/10.1186/s12877-021-02257-z
- Tuijt, R., Rait, G., Frost, R., Wilcock, J., Manthorpe, J., & Walters, K. (2021b). Remote primary care consultations for people living with dementia during the COVID-19 pandemic: Experiences of people living with dementia and their carers. The British Journal of General Practice: The Journal of the Royal College of General Practitioners, 71(709), e574–e582. https://doi.org/10.3399/BJGP.2020.1094
- van der Roest, H. G., Wenborn, J., Pastink, C., Dröes, R.-M., & Orrell, M. (2017). Assistive technology for memory support in dementia. The Cochrane Database of Systematic Reviews, 6(6), CD009627.https://doi.org/10.1002/14651858.CD009627.pub2
- van Orden, K. A., Bower, E., Beckler, T., Rowe, J., & Gillespie, S. (2022). The use of robotic pets with older adults during the Covid-19 pandemic. Clinical Gerontologist, 45(1), 189–194.https://doi.org/10.1080/07317115.2021.1954122
- Weems, J. A., Rhodes, S., & Powers, J. S. (2021). Dementia caregiver virtual support: An implementation evaluation of two pragmatic models during COVID-19. Geriatrics, 6(3), 80.https://doi.org/10.3390/geriatrics6030080
- Wei, G., Diehl-Schmid, J., Matias-Guiu, J. A., Pijnenburg, Y., Landin-Romero, R., Bogaardt, H., Piguet, O., & Kumfor, F. (2022). The effects of the COVID-19 pandemic on neuropsychiatric symptoms in dementia and carer mental health: An international multicentre study. Scientific Rreports, 12(1), 2418. https://doi.org/10.1038/s41598-022-05687-w
- Yahara, M., Niki, K., Ueno, K., Okamoto, M., Okuda, T., Tanaka, H., Naito, Y., Ishii, R., Ueda, M., & Ito, T. (2021). Remote reminiscence using immersive virtual reality may be efficacious for reducing anxiety in patients with mild cognitive impairment even in Covid-19 pandemic: A case report. Biological and Pharmaceutical Bulletin, 44(7), 1019–1023. https://doi.org/10.1248/bpb.b21-00052
Appendix A.
Scopus search strategy
(TITLE-ABS-KEY (dementia OR dement* OR alzheimer* OR ‘lewy body’ OR creutzfeldt OR binswanger OR korsakoff OR frontotemporal OR ‘vascular dementia’ OR ‘pick disease’ OR ‘cognitive impairment’ OR ‘cognitive decline’ OR ‘memory loss’) AND TITLE-ABS-KEY (covid OR ‘covid-19’ OR corona* OR ‘sars cov 2’) AND TITLE-ABS-KEY (technolog* OR ‘assistive technolog*’ OR ‘assistive device*’ OR device* OR electronic*)) AND (LIMIT-TO (PUBSTAGE, ‘final’) OR LIMIT-TO (PUBSTAGE, ‘aip’)) AND (LIMIT-TO (PUBYEAR, 2022) OR LIMIT-TO (PUBYEAR, 2021) OR LIMIT-TO (PUBYEAR, 2020)) AND (LIMIT-TO (DOCTYPE, ‘ar’) OR LIMIT-TO (DOCTYPE, ‘re’)) AND (LIMIT-TO (LANGUAGE, ‘English’) OR LIMIT-TO (LANGUAGE, ‘Portuguese’) OR LIMIT-TO (LANGUAGE, ‘Dutch’) OR LIMIT-TO (LANGUAGE, ‘German’) OR LIMIT-TO (LANGUAGE, ‘Spanish’))