
Abstract
Objectives: Engagement with music (i.e. listening, moving to the beat, joining in, performance) is documented to enhance cognition, mood, socialization, and a host of other wellness indicators in advancing age. A number of comprehensive scales measure this engagement, but a brief, accessible scale designed for general use with older adults is lacking. This project was undertaken to create and offer preliminary validation of the 7-item Music in Aging Wellness Scale (MAWS).
Method: Seven items reflecting aspects of music engagement (ME) were developed by expert opinion (e.g. ‘I always tap my foot or sway my body to good music’) for completion on a 1–7, strongly disagree to strongly agree, Likert scale. These were subject to exploratory factor analysis (EFA) (n = 349 cases) along with a set of six experimental items on ageism. It was hypothesized these items would cluster by content, thus showing separation into distinct factors.
Results: This was achieved and the resulting measure showed sound internal consistency (0.82), split-half reliability (0.71), and one-year test–retest (0.83). The MAWS total score was found to correlate significantly in expected directions with common gerontological measures. High scorers reported less depression, more mastery, less loneliness, and larger social networks. No association was found for worry-based anxiety and self-reported cognitive decline.
Conclusion: This preliminary reliability and validity study suggests that the MAWS may be an appropriate outcome and tracking measure for older adults involved in music-wellness interventions. Future research will further validate MAWS characteristics and associations with other established measures in this important field.
This study was approved by the University of New England Institutional Review Board via Expedited Review (0323-10).
Introduction
Enjoyment of and participation in making music is widely believed to contribute to positive, healthful aging (Hays et al., Citation2002). Benefits accrue to the brain, body, and spirit (Hallam & Creech, Citation2016). Whether through performance—playing an instrument, singing—or simply listening with focused interest, engagement with music has been shown to promote positive social interactions (Southcott, Citation2009), reduce depression (Leubner & Hinterberger, Citation2017; Zhao et al., Citation2016), and enhance quality of life in aging adults (Coffman, Citation2002; Solé et al., Citation2010).
The neuroprotective and neurorehabilitation potentials of music engagement (ME) are well documented. Music-related boosts to memory performance have been shown in both in community-dwelling older adults (Mammarella et al., Citation2007) and persons diagnosed with Alzheimer disease (Clark & Warren, Citation2015). Community choruses have formed in cities across the US to engage older adults with dementia in music performance for brain health and social wellness (Mittelman & Papayannopoulou, Citation2018; Smith et al., Citation2022).
ME is typically quantified through self-report of a target person or an informant (Greenberg & Rentfrow, Citation2017). Until the advent of digital streaming and online sharing, the only way to know of an individual’s ME was to ask them. Greenberg and Rentfrow advocate convincingly for building on this base of self-report data, in large population samples, and adding in digital tracking to quantify this engagement more fully. They call this big music data: ‘There are fantastic opportunities forthcoming with Big Data that can be a new frontier in generating knowledge and technology on the beneficial psychological powers of music’ (p. 54). Self-report is the essential starting point.
One popular self-report measure is the comprehensive Music USE Questionnaire (Chin & Rickard, Citation2012). The MUSE is a 24-item questionnaire (32 and 58 item versions also available), responded to on a 0–5 Likert (0 not at all/strongly disagree to 5 a great deal/strongly agree), inclusive of five ME styles (i.e. social connection, dance, cognitive/emotional regulation, physical exercise, and engaged production), and comprised three indices: Index of Music Training, Index of Music Instrument Playing, and Index of Music Listening. Two studies involving 210 adults (M age = 38) and 154 adults (23) were conducted. The authors reported sound internal consistency (0.78–0.87) across scale components and various preliminary validity indicators. They concluded ‘With this ME profile, researchers will be able to capture the complete music background of an individual in a brief 5-min self-response questionnaire’ (p. 441).
In contrast, the 35-item Music Engagement Questionnaire (MusEQ) was developed specifically for completion by an informant in support of dementia research (Vanstone et al., Citation2016). Self-completion is also an option. Factor analysis of items completed by 391 community respondents (171 as informants; 218 reporting about self; mean age 38) yielded six interpretable factors—Daily (5 items; e.g. ‘I listen to music while I perform chores or boring tasks’), Emotion (8; ‘relax when listening to peaceful music’), Perform (6; ‘People who know me describe me as a musical person’), Consume (6), Respond (4), Prefer (3)—with subscale internal consistency reliabilities ranging from 0.63 to 0.87. The resulting MusEQ was subsequently administered to 22 older adults (16 with a dementia diagnosis confirmed through screening) and their family caregivers. Informant ratings were found to be similar across five of six domains, and total scores were highly correlated (0.78). The only difference was in Emotion which was significantly higher in the self-report group. The authors suggest broad utility for the MusEQ in aging-related studies, especially those that would benefit from informant input.
Another self-report measure—the ME questionnaire—was developed on a large sample of over 2500 teenagers and young adults who responded to an online competition (Hollebeek et al., Citation2016). Respondents were asked to report on their music preferences at age 14. A 25-item preliminary scale was assessed through exploratory factor analysis (EFA) with half of the sample, and an 11-item version was then validated with the other half through confirmatory factor analysis. The ME addresses three interpretable factors associated with ME: social-identity (4 items; e.g. ‘Part of my role among friends is to keep them informed about new music or when bands will be touring’), transportive (4; ‘Listening to music is an escape’), and affect-inducing (3; ‘Some songs send shivers up my spine or give me goose bumps’). Chronbach alphas ranged from 0.82–0.92.
While rigorous in development and comprehensive in coverage, these scales all have limitations when applied to older adults. The MUSE and ME were developed on data from persons under age 60. Participants in MusEQ development represented a broader age range (i.e. ∼20–80s based on reported standard deviations), and additional validation focused on older adults. The case for the MusEQ as an informant measure appears strong, but its length could be burdensome to some older respondents when other constructs also require measurement (i.e. potentially making for an overly long survey).
Health, function, and wellness assessment of older adults involves striking a balance between comprehensive measurement and economy in the selection of tools (VanSwearingen & Brach, Citation2001). Fatigue can impact negatively on measurement quality (Yu et al., Citation2010). The geriatric literature is replete with short-form versions of long-form scales for this reason. While the 30-item Geriatric Depression Inventory, for example, may capture deeper nuances of mood, the 15-item and 5-item short forms are more widely used precisely because of their brevity (Aikman & Oehlert, Citation2001; Wall et al., Citation1999). Measuring the core features of a construct, such as depression, is often enough. There is general acceptance among older adults and the health professionals who serve them that music is therapeutic (Khan et al., Citation2016). Numerous clinical trials of music interventions have shown benefits across a range of outcomes (Leubner & Hinterberger, Citation2017; Zhao et al., Citation2016). Yet, longstanding personal interest in music (i.e. pre-trial ME) is often not discussed in such studies (see Coulton et al., Citation2015; Liao et al., Citation2018). The addition of a brief, self-report measure of ME in older adults could enhance such studies.
In sum, what appears missing from the literature on ME is a simple scale tailored to the subjective wellness of older adults: their participation in music, the pleasure they derive from it, and the personal mattering it may bring (e.g. pride in music knowledge). This scale could serve as a pre-intervention of measure of music interest as well as an accessible outcome measure of engagement. The goal of the present study was to develop an accessible, brief scale to measure subjective music-related wellness in community-dwelling older adults aged 55–98 years.
It was hypothesized that a series of ME items (i.e. declarative statements) presented to a large sample of community-dwelling older adults would: (1) statistically cluster together distinct from other aging-related constructs; and (2) a total score derived from these items would correlate with common health and wellness indicators in aging.
Method
Item development and context
Items for the Music in Aging Wellness Scale (MAWS) were developed by the author, with input from faculty colleagues at the University of New England (UNE), for a supplemental survey associated with an ongoing longitudinal study of healthful aging in northern New England. The UNE Center for Excellence in Aging & Health engages with community-dwelling older adults through its Legacy Scholars Program (LSP). ‘Scholars’ are adults, aged 55 years and older, who complete annual surveys on health and wellness, participate in a research registry, volunteer for IRB-approved studies, support intergenerational service-learning on aging (see Meuser et al., Citation2022), and participate in the cultural life of this ‘Age Friendly University’ (see Gugliucci & O’Neill, Citation2019). Over 650 scholars have completed the core annual survey since January 2019, and two thirds also completed an optional health supplement initiated in January 2021. Music items for the MAWS were part of this supplement to support future research on music and wellness. Time-linked data (i.e. when surveys were completed close in time) from both surveys were merged and analyzed for this study.
Music items were written for Likert scale response: 1 (Strongly Disagree) to 7 (Strongly Agree); a response frame employed in other core survey items. Items were worded strongly (i.e. with emphasis on extreme views) to encourage variability in response and reduce risk for severe skew (Comrey, Citation1988). This is to avoid everyone responding strongly agree to an item written more generally (e.g. ‘I enjoy music’). Descriptive statistics for these items are presented in .
Table 1. Music item properties.
All ME item distributions were slightly skewed as is common in psychosocial measurement (Blanca et al., Citation2013). Skewness refers to a score distribution’s ‘lean’ from center (i.e. towards left/low tail or right/high tail), and kurtosis refers to the height of the distribution. A normal distribution is visualized as an upside down ‘U’ whereby two-thirds of scores fall in the center area and rest sloping evenly to the tails. High kurtosis reflects a flattening of this U shape with more scores in the tails. Blanca and colleagues define skewness and kurtosis scores together in these ranges: 0.26–0.75 range as slightly non-normal, 0.76–1.25 as moderately so, 1.26–1.75 as highly so, 1.76–2.25 as extreme, and 2.26+ as very extreme. Distributions beyond the high range raise measurement validity concerns.
All music items were acceptable per these ranges. The distribution of one music item (listen to…) was just slightly skewed, five items were moderately skewed, and one item (sing or hum to self…) fell in the high range for kurtosis but not for skew (i.e. flattened distribution with scores spread evenly across all levels). The sum of these items—the proposed MAWS Total Score for interpretation—was just slightly skewed as shown in .
Figure 1. Frequency distribution of sum of music items.
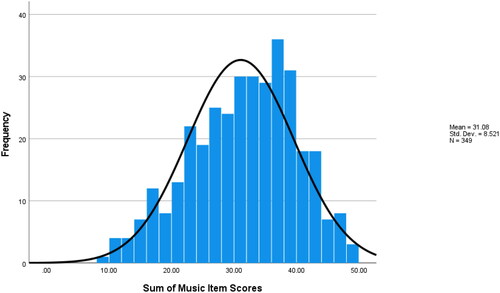
Sample Characteristics. Full ME data were available from 349 participants when the dataset was extracted in January 2023, thus forming the sample for this project. Participants were primarily female (73%), white (98%), moderately old with a mean age of 73.4 years (SD 6.5), and well-educated with mean years of 17.8 (SD 2.91). Most (71%) were retired, and many (65%) reported being married or partnered.
Wellness measures
Legacy Scholars complete various measures of wellness in their annual core and supplemental surveys. Measures of self-reported emotional, cognitive, and interpersonal wellness were considered as validity correlates based on established associations with music in the literature (see Introduction). Selected emotion measures were the 15-item Geriatric Depression Scale (GDS15; Sheikh & Yesavage, Citation1986; Yesavage et al., Citation1982) and the 8-item Penn State Worry Questionnaire (PSWQ8; Hopko et al., Citation2003; Meyer et al., Citation1990). The Ascertain Dementia 8 (AD8; Galvin et al., Citation2006, Citation2007) and the Pearlin Mastery Scale (PMS; Pearlin & Schooler, Citation1978) addressed cognitive wellness. Interpersonal wellness was measured through the Lubben Social Network Scale (LSNS; Lubben et al., Citation2006) and the 8-item UCLA Loneliness Scale (UCLA-LS8; Hays & Dimatteo, Citation1987). For all measures save one—the LSNS—higher scores were more suggestive of a problem (i.e. higher GDS15 scores are more suggestive of clinical depression). Lower scores on LSNS indicate a smaller social network and so suggest a risk for isolation. Descriptive statistics for these are presented in .
Table 2. Properties of the MAWS and validity measures.
Sample frame
All 349 participants completed the music items at Time 1; 128 (37%) completed the music items at Time 2 which restricted the sample for determination of test–retest reliability. Completion of the core and supplemental annual surveys are typically completed within a 2-month window. Missing values are minimal across both surveys. Three measures (PMS, LSNS, and UCLA-LS8) were drawn from the supplement and so co-occurred precisely in time with the music items. The remaining measures were drawn from the annual core survey and evidence somewhat smaller effective sample sizes (see ).
Analysis
The 7 music items posited for the MAWS are listed in . These show sound face validity in their wording: all refer explicitly to engagement in music. It was presumed that these items would cluster together as ‘music-related’ in an EFA. Additional items of another type were available to challenge this assumption. To further test this clustering hypothesis, the 7 music items were analyzed along with 6 experimental items designed to measure harm from personal experiences of ageism. On their face, engagement with music and harm from ageism would seem unlikely to correlate, and so it was hypothesized they would separate into distinct factors in EFA. Principal Axis Factoring was conducted to test this in accordance with EFA guidelines for psychological measures (see Flora & Flake, Citation2017; Osborne, Citation2015).
Additional analyses targeted measures of non-normality discussed above, scale reliability (internal consistency, split-half, test–retest), correlation with other wellness measures (i.e. for validity determination), and mean difference testing (One Way ANOVA).
Results
Factor analysis
A Principal Axis Factoring with direct oblimin rotation was run on the 7 music and 6 ageism items. Minimum factor loading was set to 0.30 to exclude weak relationships. Communalities were all above the 0.30 threshold. All item inter-correlations were below 0.80, suggesting acceptable collinearity for EFA, and the determinant was found acceptable at 0.014. Bartlet’s Test of Sphericity was significant (p < .001) in further support of this EFA approach.
Quality of model fit was assessed via the Kaiser-Meyer-Olin measure of sampling adequacy which yielded a solid 0.76. The model contained four factors with Eigenvalues > 1, ranging from 3.53 to 1.01, and together these explained 52% of model total variance. The factor pattern matrix is presented in .
Table 3. Factor pattern matrix for music for aging in wellness scaleFootnote1.
As hypothesized, the experimental ageism items all clustered under one factor (2). Music items loaded cleanly on the remaining three factors. A review of item content suggests the following titles for these component factors: (1) Joining in Voice & Rhythm; (3) Prioritization for Wellness; and (4) Musical Aptitude. While meaningful in content terms, subscales like these with few items risk unreliability when scored and interpreted separately (Maciej Serda et al., Citation2003). In accordance with the goal of a simple measure of music wellness, just the total sum of the 7 item scores is proposed to constitute the MAWS score for interpretation.
Descriptives and scale reliability
shows descriptive statistics and reliability indicators for the MAWS total score and other wellness measures. The MAWS showed sound internal consistency reliability (Cronbach Alpha; 0.82), acceptable split-half reliability (Gutman; 0.71), and sound test–retest reliability (Intraclass Correlation, 0.83). Similar levels were found for the other wellness measures, except for the self-report AD8 which evidenced weaker reliability as found in other studies (Chio et al., Citation2018).
Validity associations
MAWS correlations with other wellness measures are shown in . The MAWS total score was associated with both social network size (0.23; p < .001) and loneliness (−0.16; p = .004). Persons reporting greater music wellness also report larger social networks and less subjective loneliness. Of the cognitive measures, just mastery was associated with music wellness (0.15; p = .007); perception of cognitive decline on the AD8 was not. This latter finding may be related to the weaker psychometric properties of this scale when relying on self-report. Mood was correlated with music wellness (−0.16; p = .013), but not worry-based anxiety. Higher reported music wellness was associated with lower reported depression on the GDS15.
Table 4. Correlations of MAWS with validity measures.
MAWS scores did not differ by sex (Male M = 30.3, SD = 8.8; vs. Female M = 31.3, SD = 8.5), and nonsignificant correlations were found for age and years of education.
Impact of musical performance history
In addition to the MAWS items presented so far, the LSP supplemental survey also asks if a respondent was ever a participant in a formal singing group and if they have a history of playing one or more instruments. Persons with expertise in music performance may be expected to score higher on a music wellness scale than others without these backgrounds. If so, this may be considered another indicator of validity. To test this, a four-level variable was created to show such differences (see labels in ).
Figure 2. MAWS score distributions by level of performance experience.
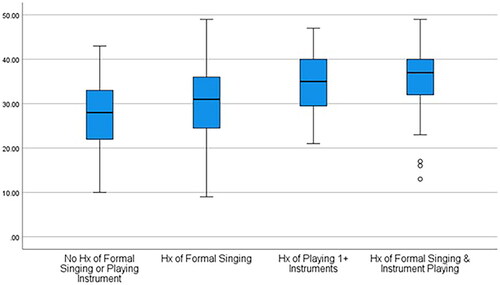
A one-way between subjects ANOVA was conducted to compare levels of expertise in music performance with MAWS total scores. There was a significant effect of music performance on MAWS total score at the p < .0001 level for the four conditions [F(3, 345) = 20.11, p = 0.000)]. Post hoc comparisons via the Tukey HSD test indicated that the mean MAWS score for no performance history (M = 27.71, SD = 7.88) was significantly lower than the other positive performance history categories. History of formal singing (M = 29.59, SD = 8.67) also differed significantly from the other three categories as visualized in . Both history of playing an instrument and the combination (singing + instrument) differed significantly from the other two categories but did not differ from each other (M = 34.16 vs. 35.79, SD = 7.24 vs. 7.36). Participants who reported playing a musical instrument evidenced higher MAWS total scores than those who sang formally or informally.
One MAWS item (‘I am expert at reading music’) may relate to music performance, a facet of ME not directly represented in this scale. A one-way between subjects ANOVA compared levels of expertise in music performance with this single item. There was a significant effect of music performance on music reading at the p < .0001 level for the four conditions [F(3, 345) = 88.7, p = 0.000)]. Post hoc comparisons via the Tukey HSD test showed no difference between persons with no formal history of singing or instrument playing and those with a formal history of singing only (M = 1.58 vs. 2.09, SD = 0.83 vs. 1.51). A significant difference (p < .0001) emerged only for those reporting a history of playing an instrument and the combination (M = 4.11 vs. 4.49, SD = 1.91 vs. 1.55).
Discussion
This study established the reliability and preliminary validity of the MAWS comprised 7 items which together reflect three facets (factors) of ME: (1) Joining in Voice & Rhythm; (2) Prioritization for Wellness; and (3) Musical Aptitude. Responses on a 1–7 Likert scale are summed to obtain the MAWS total score which evidenced sound internal consistency reliability (0.82), acceptable split-half reliability (0.71), and sound 1-year test–retest reliability 0(.83). MAWS scores were normally distributed, and no differences were found based on gender, age, or education level. The MAWS correlated significantly, and in the expected direction, with established gerontological measures associated with cognition (mastery), mood (depression), and interpersonal wellness (loneliness, isolation). As shown in , the MAWS also captures a wide range of musical engagement scores in persons with casual interest to those involved in formal performance (i.e. singing in a group, playing an instrument). These findings suggest that the MAWS has value as a brief, evidence-based, baseline and/or outcome measure for research and clinical/wellness projects involving older adults.
The MAWS’ high test–retest reliability suggests that it may also tap into long-held beliefs and practices with respect to ME. This may be useful for projects seeking to re-activate longstanding musical interests in persons residing in long-term care, diagnosed with dementia, experiencing loneliness, or reporting mood disturbance. A recent intervention study suggests such a utility. A randomized controlled trial of a 12-session music therapy intervention in long-term care targeted cognition, mood, pain, subjective wellness, and other outcomes (Castillejos & Godoy-Izquierdo, Citation2021). Said the authors of their post-intervention findings: ‘As expected, the participants who received the music intervention, despite its short duration, demonstrated notable improvements including enhanced functional status and autonomy, increased hand grip, enhanced cognitive functioning improved overall mood, reduced pain, and increased happiness’ (p. 97). Half of these benefits held up at 2 wk post invention. A measure that was conspicuously missing, however, was one of ME. Might participants with high longstanding music wellness have responded differently than those with low such wellness? Were gains two weeks later driven by responses of those with high music wellness? These questions would seem relevant but cannot be answered without a scale like the MAWS.
A potential criticism of the MAWS is its brevity and the aspects of music wellness it does not address. As reviewed earlier, other scales—notably the MUSE and MusEQ—involve many more questions and so cover additional components of engagement. The three factors of the MAWS are clearly represented in these longer scales. What these scales add are elements of music production and performance that the MAWS only touches on. The only MAWS item that comes close is ‘I am expert at reading music.’ Post hoc testing following a significant one-way ANOVA showed that participants who reported playing an instrument agreed more with this item than others, including formal singers. The MAWS appears to capture an element of music performance in this sense. Is this enough to justify its use as an outcome measure?
More research is needed to address this question. The degree to which the MAWS may correlate with scores derived from the MUSE or MusEQ is certainly relevant for establishing validity. The apparent overlap in content suggests that these scales will intercorrelate. Another issue is the relevance of performative measures of ME involved older adult wellness-focused projects. Does measuring music performance matter? If the goal is to engage participants in singing, moving to the rhythm, and enjoying this experience, the MAWS would appear capable of measuring such impacts in a brief, accessible manner.
The MAWS may also contribute Greenberg and Rentfrow’s ‘Big Music Data’ approach to further demonstrate the value of music to wellness in advancing age. Self-reports of music interest are the foundation on which digitally derived music access and behavior patterns are added. A brief scale that captures the ‘gist’ of this interest for older adults may be applicable to studies involving many constructs requiring measurement.
As suggested above, another potential application is in intervention research, including clinical trials. Prior affinity for music would seem relevant even when the primary outcome is mood, memory, socialization, or something else. A recent review of 187 studies pointed to numerous definitional, methodological, and reporting inconsistences in music intervention research (Robb et al., Citation2018). Robb and colleagues stated: ‘There needs to be a clear scientific premise for why an investigator expects the specified use of music to influence the outcome of interest. Yet, less than half of the reviewed studies included a theoretical framework or offered a scientific rationale. Identifying and measuring not only outcomes, but also the proposed mechanisms of action allow investigators to move beyond basic questions about efficacy, and begin answering questions about how, why, and for whom an intervention works’ (p. 32).
Use of a ME scale—the MAWS (i.e. when brevity is important) and others reviewed earlier—could provide helpful context for such investigations and, perhaps, support targeting of interventions. Might people with high music interest/engagement prior to an intervention respond differently (better?) than those with low engagement? The answers to this and similar questions are relevant for targeting music interventions.
Limitations
The MAWS was developed based on expert opinion alone. The seven items were written, scrutinized by colleagues of the author, and then administered directly to community-dwelling older adults over a 2-year period. The scale is neither theory-driven nor based on a more extensive exploratory study from which items were extracted based on factor analysis. EFA was applied after to confirm an a priori hypothesis that the 7-item MAWS would cluster to form a coherent whole. This was demonstrated with the inclusion of six additional test items of another construct (i.e. ageism) in the EFA. Perfect separation was achieved, supporting validity in a post hoc sense. Additional prospective research is needed to confirm the factor structure of the MAWS with new participants and inclusive of other measures of ME. This work is in process.
Conclusion
The joys and wellness benefits of ME for older adults are well established (Sorrell & Sorrell, Citation2008). There appears to be a need in music-related research and intervention for a brief, accessible scale to measure music-related wellness in this population. The MAWS may be a solid choice for measurement in projects now and in the future.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
Notes
1 Ageism item loadings in box.
References
- Aikman, G. G., & Oehlert, M. E. (2001). Geriatric depression scale. Clinical Gerontologist, 22(3–4), 63–70. https://doi.org/10.1300/J018v22n03_07
- Blanca, M. J., Arnau, J., López-Montiel, D., Bono, R., & Bendayan, R. (2013). Skewness and Kurtosis in real data samples skewness and kurtosis in real data samples. Methodology, 9(2), 78–84. https://doi.org/10.1027/1614-2241/a000057
- Castillejos, C., & Godoy-Izquierdo, D. (2021). “Music makes my old heart beat”: A randomised controlled study on the benefits of the use of music in comprehensive care for institutionalised older adults. Applied Psychology Health and Well-Being, 13(1), 84–108. https://doi.org/10.1111/APHW.12217
- Chin, T. C., & Rickard, N. S. (2012). The music USE (MUSE) questionnaire: An instrument to measure engagement in music. Music Perception, 29(4), 429–446. https://doi.org/10.1525/mp.2012.29.4.429
- Chio, O. I., Yip, P. K., Liu, Y. C., Chen, L. H., Wang, P. C., Tsai, T. H., & Tang, S. H. (2018). Detection of cognitive impairment using self-rated AD8 and informant-reported AD8. Journal of the Formosan Medical Association = Taiwan yi Zhi, 117(1), 42–47. https://doi.org/10.1016/j.jfma.2017.02.015
- Clark, C. N., & Warren, J. D. (2015). Music, memory and mechanisms in Alzheimer’s disease. Brain: A Journal of Neurology, 138(Pt 8), 2122–2125. https://doi.org/10.1093/BRAIN/AWV148
- Coffman, D. D. (2002). Music and quality of life in older adults. Psychomusicology: A Journal of Research in Music Cognition, 18(1–2), 76–88. https://doi.org/10.1037/h0094050
- Comrey, A. L. (1988). Factor-analytic methods of scale development in personality and clinical psychology. Journal of Consulting and Clinical Psychology, 56(5), 754–761. https://doi.org/10.1037/0022-006X.56.5.754
- Coulton, S., Clift, S., Skingley, A., & Rodriguez, J. (2015). Effectiveness and cost-effectiveness of community singing on mental health-related quality of life of older people: Randomised controlled trial. The British Journal of Psychiatry: The Journal of Mental Science, 207(3), 250–255. https://doi.org/10.1192/BJP.BP.113.129908
- Flora, D. B., & Flake, J. K. (2017). The purpose and practice of exploratory and confirmatory factor analysis in psychological research: Decisions for scale development and validation. Canadian Journal of Behavioural Science / Revue Canadienne Des Sciences du Comportement, 49(2), 78–88. https://doi.org/10.1037/cbs0000069
- Galvin, J. E., Roe, C. M., Coats, M. A., & Morris, J. C. (2007). Patient’s rating of cognitive ability: Using the AD8, a brief informant interview, as a self-rating tool to detect dementia. Archives of Neurology, 64(5), 725–730. https://doi.org/10.1001/archneur.64.5.725
- Galvin, J. E., Roe, C. M., Xiong, C., & Morris, J. C. (2006). Validity and reliability of the AD8 informant interview in dementia. Neurology, 67(11), 1942–1948. https://doi.org/10.1212/01.wnl.0000247042.15547.eb
- Greenberg, D. M., & Rentfrow, P. J. (2017). Music and big data: A new frontier. Current Opinion in Behavioral Sciences, 18, 50–56. https://doi.org/10.1016/j.cobeha.2017.07.007
- Gugliucci, M. R., & O’Neill, D. (2019). Health professions education: Advancing geriatrics and gerontology competencies through Age-Friendly University (AFU) principles. Gerontology & Geriatrics Education, 40(2), 194–202. https://doi.org/10.1080/02701960.2019.1576658
- Hallam, S., & Creech, A. (2016). Can active music making promote health and well-being in older citizens? Findings of the music for life project. London Journal of Primary Care, 8(2), 21–25. https://doi.org/10.1080/17571472.2016.1152099
- Hays, R. D., & Dimatteo, M. R. (1987). A short-form measure of loneliness. Journal of Personality Assessment, 51(1), 69–81. https://doi.org/10.1207/S15327752JPA5101_6
- Hays, T., Bright, R., & Minichiello, V. (2002). The contribution of music to positive aging: A review. Journal of Aging and Identity, 7(3), 165–175. https://doi.org/10.1023/A:1019712522302
- Hollebeek, L. D., Malthouse, E. C., & Block, M. P. (2016). Sounds of music: Exploring consumers’ musical engagement. Journal of Consumer Marketing, 33(6), 417–427. https://doi.org/10.1108/JCM-02-2016-1730/FULL/XML
- Hopko, D. R., Stanley, M. A., Reas, D. L., Wetherell, J. L., Beck, J. G., Novy, D. M., & Averill, P. M. (2003). Assessing worry in older adults: Confirmatory factor analysis of the Penn State Worry Questionnaire and psychometric properties of an abbreviated model. Psychological Assessment, 15(2), 173–183. https://doi.org/10.1037/1040-3590.15.2.173
- Khan, W. U., Mohamad Onn Yap, I. A., O’Neill, D., & Moss, H. (2016). Perceptions of music therapy for older people among healthcare professionals. Medical Humanities, 42(1), 52–56. https://doi.org/10.1136/MEDHUM-2015-010778
- Leubner, D., & Hinterberger, T. (2017). Reviewing the effectiveness of music interventions in treating depression. Frontiers in Psychology, 8, 1109. https://doi.org/10.3389/FPSYG.2017.01109/BIBTEX
- Liao, S. J., Tan, M. P., Chong, M. C., & Chua, Y. P. (2018). The impact of combined music and Tai Chi on depressive symptoms among community-dwelling older persons: A cluster randomized controlled trial. Issues in Mental Health Nursing, 39(5), 398–402. https://doi.org/10.1080/01612840.2017.1417519
- Lubben, J., Blozik, E., Gillmann, G., Iliffe, S., Von Kruse, W. R., Beck, J. C., & Stuck, A. E. (2006). Performance of an abbreviated version of the lubben social network scale among three European community-dwelling older adult populations. The Gerontologist, 46(4), 503–513. https://doi.org/10.1093/GERONT/46.4.503
- Maciej Serda, F. G., Becker, M., Cleary, R. M., Team, H., Holtermann, D., The, N., Agenda, P., Science, S. K., Sk, R., Hinnebusch, A. R., Hinnebusch, I., Rabinovich, Y., Olmert, D. Q. G. L. Q., Uld, W. K. H. U., Ri, V., Lq, W. K. H., Frxqwu, E., Zklfk, L. V., … فاطمی Edvhg, ح. (2003). Calculating, interpreting, and reporting cronbach’s alpha reliability coefficient for likert-type scales. Uniwersytet Śląski, 7(1), 343–354. https://doi.org/10.2/JQUERY.MIN.JS
- Mammarella, N., Fairfield, B., & Cornoldi, C. (2007). Does music enhance cognitive performance in healthy older adults? The Vivaldi effect. Aging Clinical and Experimental Research, 19(5), 394–399. https://doi.org/10.1007/BF03324720/METRICS
- Meuser, T., Cohen Konrad, S., Robnett, R., & Brooks, F. (2022). Telecollaboration in gerontology service learning: Addressing isolation & loneliness in a pandemic. Gerontology & Geriatrics Education, 43(1), 18–33. https://doi.org/10.1080/02701960.2021.1956489
- Meyer, T. J., Miller, M. L., Metzger, R. L., & Borkovec, T. D. (1990). Development and validation of the Penn state worry questionnaire. Behaviour Research and Therapy, 28(6), 487–495. https://doi.org/10.1016/0005-7967(90)90135-6
- Mittelman, M. S., & Papayannopoulou, P. M. (2018). The Unforgettables: A chorus for people with dementia with their family members and friends. International Psychogeriatrics, 30(6), 779–789. https://doi.org/10.1017/S1041610217001867
- Osborne, J. W. (2015). What is rotating in exploratory factor analysis? Practical Assessment, Research, and Evaluation, 20(1), 2. https://doi.org/10.7275/hb2g-m060
- Pearlin, L. I., & Schooler, C. (1978). The structure of coping. Journal of Health and Social Behavior, 19(1), 2–21. https://doi.org/10.2307/2136319
- Robb, S. L., Hanson-Abromeit, D., May, L., Hernandez-Ruiz, E., Allison, M., Beloat, A., Daugherty, S., Kurtz, R., Ott, A., Oyedele, O. O., Polasik, S., Rager, A., Rifkin, J., & Wolf, E. (2018). Reporting quality of music intervention research in healthcare: A systematic review. Complementary Therapies in Medicine, 38, 24–41. https://doi.org/10.1016/J.CTIM.2018.02.008
- Sheikh, J. I., & Yesavage, J. A. (1986). 9/geriatric depression scale (GDS) recent evidence and development of a shorter version. Clinical Gerontologist, 5(1–2), 165–173. https://doi.org/10.1300/J018v05n01_09
- Smith, A. P., Kampen, R., Erb, T., MacDonald, S. W. S., & Sheets, D. J. (2022). Choral singing and dementia: Exploring musicality as embodied and relational accomplishment. Journal of Aging Studies, 63, 101077. https://doi.org/10.1016/J.JAGING.2022.101077
- Solé, C., Mercadal-Brotons, M., Gallego, S., & Riera, M. (2010). Contributions of music to aging adults’ quality of life. Journal of Music Therapy, 47(3), 264–281. https://doi.org/10.1093/JMT/47.3.264
- Sorrell, J. A., & Sorrell, J. M. (2008). Music as a healing art for older adults. Journal of Psychosocial Nursing and Mental Health Services, 46(3), 21–24. https://doi.org/10.3928/02793695-20080301-09
- Southcott, J. E. (2009). And as I go, I love to sing: The Happy Wanderers, music and positive aging. International Journal of Community Music, 2(2), 143–156. https://doi.org/10.1386/ijcm.2.2-3.143_1
- Vanstone, A. D., Wolf, M., Poon, T., & Cuddy, L. L. (2016). Measuring engagement with music: Development of an informant-report questionnaire. Aging & Mental Health, 20(5), 474–484. https://doi.org/10.1080/13607863.2015.1021750/SUPPL_FILE/CAMH_A_1021750_SM2698.ZIP
- VanSwearingen, J. M., & Brach, J. S. (2001). Making geriatric assessment work: Selecting useful measures. Physical Therapy, 81(6), 1233–1252. https://doi.org/10.1093/ptj/81.6.1233
- Wall, J. R., Lichtenberg, P. A., MacNeill, S. E., Walsh, P., & Deshpande, S. A. (1999). Depression detection in geriatric rehabilitation. Clinical Gerontologist, 20(3), 13–21. https://doi.org/10.1300/J018v20n03_03
- Yesavage, J. A., Brink, T. L., Rose, T. L., Lum, O., Huang, V., Adey, M., & Leirer, V. O. (1982). Development and validation of a geriatric depression screening scale: A preliminary report. Journal of Psychiatric Research, 17(1), 37–49. https://doi.org/10.1016/0022-3956(82)90033-4
- Yu, D. S. F., Lee, D. T. F., & Man, N. W. (2010). Fatigue among older people: A review of the research literature. International Journal of Nursing Studies, 47(2), 216–228. https://doi.org/10.1016/J.IJNURSTU.2009.05.009
- Zhao, K., Bai, Z. G., Bo, A., & Chi, I. (2016). A systematic review and meta-analysis of music therapy for the older adults with depression. International Journal of Geriatric Psychiatry, 31(11), 1188–1198. https://doi.org/10.1002/GPS.4494