
Abstract
Objective: The Parliamentary Assembly invited the member states of the Council of Europe to ‘guarantee women's effective exercise of their right of access to a safe and legal abortion’. While abortion legislation and statistics give an impression of the legislative, cultural, and religious views of the societies and the socio-economic health of the female population, only one study conducted in 2011 looked into the current legislation and trends in terminations of pregnancy in the European Union.
Materials and Methods: From January 2017 to December 2018, a group of experts, the authors of the present article, liaised with colleagues practising in 32 European countries to collect data on abortion legislation and statistics using three different questionnaires.
Results: The article presents the results of this initiative and compares the status quo and recent trends in abortion legislation and statistics across Europe.
Conclusions: The European legislations are still very heterogenous and abortion rates vary widely between countries, confirming that laws do not correlate with abortion rates. This compilation of data, also available on a website (www.abort-report.eu), may help to change laws to better meet the needs of women who decided to have an abortion as a solution to the underlying problem of an unwanted pregnancy.
摘要
目的:欧洲议会要求委员会成员国“保证妇女能够切实获得安全合法堕胎的权利”。虽然堕胎法和统计数据体现了法律、文化和宗教的社会观点, 以及女性保健的社会经济状况, 但只有2011年的一项研究调查了欧洲联盟目前终止妊娠的法律和趋势。
材料和方法:从2017年1月至2018年12月, 本文专家联合32个欧洲执业的同事, 通过三个不同的问卷收集有关堕胎立法和统计的数据。
结果:本文介绍了这项研究的结果, 并比较了全欧洲堕胎法和统计数据的现状和近期趋势。
结论:欧洲的法律仍有很大的异质性, 各国堕胎率的差别也很大, 这证实法律并不受堕胎率的影响。这些汇编的数据也可在网站(www.abort-report.eu)上获得, 这可能有助于改进法律, 以满足那些决定通过堕胎来解决意外怀孕问题的潜在妇女群体的需求。
Keywords:
Introduction
Statistics on abortion reflect the consequence of legislative, cultural, and religious views of the societies, and the socio-economic health of the female population. For example, statistics on abortion can reflect the accessibility or delays of abortion services, the health care provider attitudes to abortion and their training, or the cost of the procedure [Citation1]. Moreover, the widespread hormone scepticism that has been observed for several years has resulted in a true pill scare and further contributed to a decrease in the use of effective contraception and consequently an increase in unplanned pregnancies and abortions [Citation2]. Finally, it has been shown that the recent economic shocks have also contributed to an increasing abortion trend as couples confronted with unwanted pregnancies decide to terminate them due to lack of economic security to maintain a family [Citation3].
The main goal of starting the European Union (EU) in 1951 was to promote peace, its values, and the well-being of its citizens. In this context the Council of Europe in 2008 stated one common goal in a resolution of the Parliamentary Assembly as ‘guarantee women’s effective exercise of their right of access to a safe and legal abortion’ and to ‘lift restrictions which hinder, de jure or de facto, access to safe abortion’ [Citation4].
Three years later, in 2011, Gissler et al. [Citation5] found large variations in abortion legislation and rates between the 27 EU member states. No similar study was published since, although laws, practices and attitudes have changed in several European countries. Moreover, the abortion pill mifepristone, first approved in 1988 in France and listed as essential medicine by the WHO in 2005, is used increasingly in most European countries and has recently been approved in the few remaining countries (e.g., Bulgaria, Czech Republic, Ireland, and Slovenia) [Citation6,Citation7].
A group of European experts, all obstetricians/gynaecologists (OB/GYN) and members of the International Federation of Professional Abortion and Contraception Associates (FIAPAC), the authors of the present article, therefore decided to collect legislation and abortion data in Europe to compare the status quo and recent trends in legislation and abortion data between countries. This article presents the results of this initiative.
Materials and methods
The study period was a 2-year process (January 2017 to December 2018) (). As a first step, the experts selected health indicators that could be analysed based on their experience, national abortion statistics available in their countries, and sexual and reproductive health. They then invited colleagues (i.e., OB/GYNs mostly members of FIAPAC) practising in 32 European countries (the 28 European Union members plus Iceland, Norway, Switzerland and Serbia) to participate in the project. Invited OB/GYNs volunteered to participate in the data collection process. OB/GYNs (authors included) who provided requested information and data became correspondents if they agreed to contribute for future updates. The affiliation of correspondents varied, some were working in a hospital or family planning organisation and some had their private practice.
Figure 1. Study design and data availability.
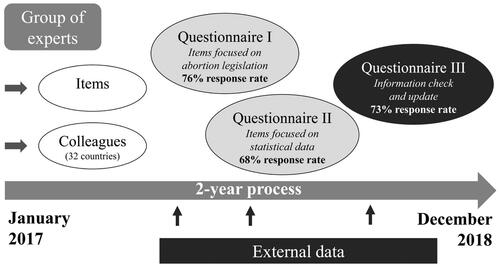
Two questionnaires were constructed using items selected by the experts. Questionnaire I (85 items) focussed on abortion legislation, and Questionnaire II (116 items) on practical (detailed reproductive health information) and statistical data on abortion, fertility, and contraception. The questions were close-ended to facilitate analysis. When possible, the questionnaires were prefilled with official data from each country found on the Internet before being consecutively sent by e-mail to all correspondents. Instructions to validate the data, indicate data sources, and fill out and submit the questionnaires were provided. Approximately one year later, a third questionnaire (Questionnaire III) grouping the most frequently completed items from Questionnaires I and II was sent to all correspondents to check, update, and source information.
For the purpose of this article, the following data were analysed using Excel (Microsoft): overall number of abortions (i.e., number of reported legal abortions); abortion rate (i.e., number of reported legal abortions per 1000 women between 15 and 44 or 49 years of age according to the country); abortion ratio (i.e., number of abortions per 1000 live births per year); and percentage of medical abortions amongst all abortions.
Results
Data available
There was at least one correspondent for 29 of the 32 European countries (there were no correspondents for Malta, Romania, and Slovakia). Questionnaires I, II, and III were consecutively sent to at least one correspondent in 29, 22, and 26 countries, and completed for 22 (76%), 15 (68%), and 19 (73%) countries, respectively (). Information collected from websites of non-governmental organisations working in the field or government agencies (i.e., International Planned Parenthood Federation (IPPF) European Network [Citation8], Central Intelligence Agency (CIA) [Citation9]; United Nations (UN) [Citation10]) and national statistics (external data) was collected during the whole study period, leading to between 12 and 31 items filled out per country (see Supplementary Table 1 in the Appendix) for 31 countries (no data for Malta). The list of national sources provided by the correspondents or found on the Internet is presented in the Appendix (Supplementary Table 2).
Legislation
In December 2018, in most European countries, the law allowed abortion on request or on such broad grounds that it could be interpreted as allowing abortion on request (). Nevertheless, some restrictions in access to abortion are still in place in most countries.
Figure 2. Legal grounds for abortion in Europe. Source: www.abort-report.eu.
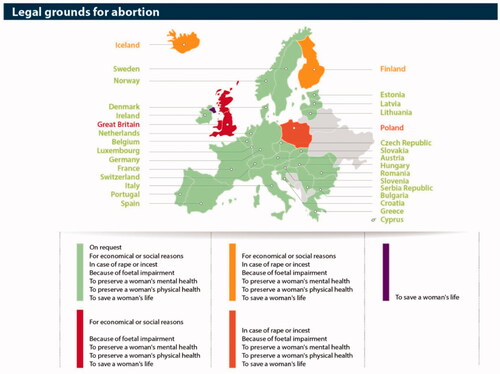
The first country to legalise abortion was the former Soviet-Union in 1920 and then the former communist countries in the 1950s. The first country in Western-Europe to legalise abortion was the UK (1967 abortion act) with other countries following and a great number enacting their laws in the 1970s. The most recent addition to this group was the Republic of Ireland. In May of 2018 this country voted to repeal the abortion ban in a referendum (the 8th amendment) and the bill was signed into law in September of 2018. Abortion services are in place since January 2019. It is noteworthy that abortion was made illegal again only in 3 countries in the last 100 years: Soviet Union during the 2nd World War, Romania under the dictatorship of Nicolae Ceaușescu, and Poland at the request of the Polish Pope John Paul II (Karol Józef Wojtyła).
Few countries in Europe give women truly unrestricted access to abortion. Most require some conditions to be fulfilled. Specific written consent is to be obtained before abortion in all countries allowing it on request except Austria, and Sweden. A waiting period between the pre-abortion and abortion visits is mandatory in some European countries lasting between 2 and 7 days according to the country (). In France, this waiting period was removed in 2015, but a 2-day waiting period is still mandatory for minors and when women visit a social worker before requesting the abortion. In the UK and Finland, abortion is still only legal if two doctors consent.
Table 1. Obligatory waiting periods (‘cooling off’).
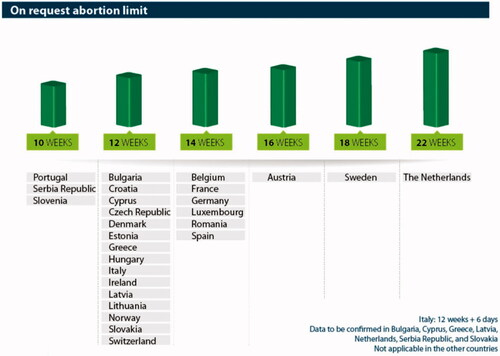
Moreover, although abortion has been allowed, there is an upper gestational age limit in all countries. This varies widely, with the time limit ranging from 10 weeks (Portugal, Serbia Republic, and Slovenia) to 22 weeks (The Netherlands) and 24 weeks (UK) ().
Figure 3. Legal time limits* for performing on request abortion by European country. *In weeks of amenorrhoea. Source: www.abort-report.eu.
Medical abortion is easily and legally accessible on request in most European countries. However, most countries also apply a legal upper gestational age limit ranging from 7 weeks (Belgium, Luxembourg out of hospital, Switzerland, France if done outside of a hospital setting) to 9 or 10 weeks (all other countries) for home use of medical abortion. Medical abortion is the method of choice in second trimester abortion in most countries, and is also widely practiced in the late first trimester.
Abortion rate
The way in which the number of abortions is reported varies widely in Europe. Some countries make a huge effort to get complete numbers by analysing underreporting and adding the estimated underreporting like France, where a special commission is charged with this task [Citation11]. Other countries take the legally required notification of the treating doctors at face value without any evaluation of possible underreporting like Germany and Switzerland. This makes a comparison between countries difficult as real differences in abortion numbers are confounded by differences in completeness of the national reporting system.
The overall number of abortions ranged from 921 (Iceland) to 216,685 (France) The abortion rates per 1000 women between 15 and 49 years of age (44 years in some countries) and abortion ratio per 1000 births, also vary widely across Europe ().
Table 2. Main descriptive statistics for abortion in Europe.
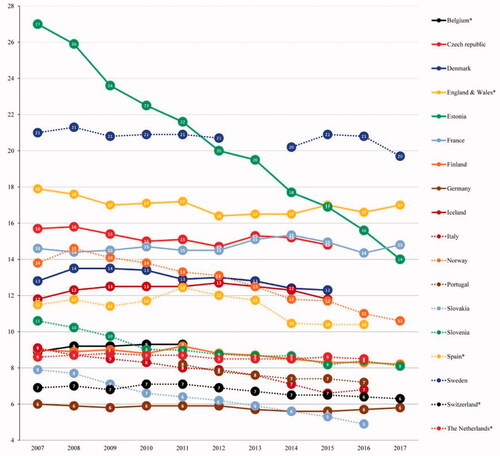
From 2007 to 2017 (), abortion rate remained stable or decreased in most countries, regardless of the initial abortion rate. The decrease was particularly marked in Estonia, Norway, Slovenia, and Slovakia. A marked reduction has also been seen in many countries in teenage abortions with a shift in the age groups with the highest abortion rates (from 20–24 to 25–30 years) in some countries.
Figure 4. Abortion rate in women of childbearing age (15–49 years) by European country. x-axis: years; y-axis: abortion rate per 1000 women of childbearing age (15–49 years). *According to national statistics childbearing age is comprised between 15 and 44 years.
Medical abortion
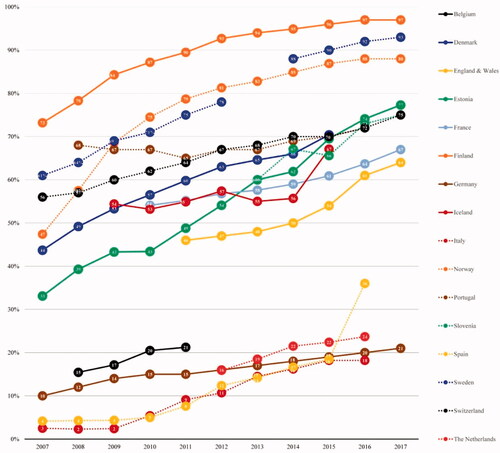
The percentage of medical abortions varies widely across Europe, ranging from 18% (Italy, 2016) to 97% (Finland, 2017) (). Medical abortion rates have steadily increased from 2007 to 2017, in all countries (). In 2015, 2016, and 2017, medical abortion was the most commonly used method in most countries averaging 63%.
Figure 5. Percentage of medical abortions by European country. x-axis: years; y-axis: percentage.
Discussion
Findings and interpretation
Our data show that the national differences in legislation continue to decrease in the European Union and neighbouring countries. As described by Gissler et al. in 2011 [Citation5], there are still large differences in legislation but the laws and regulations have nonetheless become gradually more homogenous during the last years. In Belgium and Italy, a mandatory waiting period of 6 and 7 days is still required between the first contact during counselling and the abortion procedure. Counselling is provided by the abortion centre in Belgium and by a doctor in Italy. In Portugal, Serbia, and Slovenia, abortion on request is only permitted up to a gestational age limit of 10 weeks from the last menstrual period while in 12 other countries the same applies up to 12 or 14 weeks. Ireland is the most recent addition to the list of countries that allow abortion after a referendum in 2018. The situation is more complex in the United Kingdom, where abortion was legalised in the Isle of Man only in 2019, 52 years after the Abortion Act of 1967 made abortion legal in England, Wales, and Scotland [Citation12]. Northern Ireland was the last member of the UK to revise its law dating back to 1861 and legalise abortions in March 2020. [Citation13] However the provision of abortion services remains unstable due to heavy political and legal debates. [Citation14]
Other European countries where abortion is still not permitted are Malta and Poland. Abortions are not allowed either in Andorra, Liechtenstein, Monaco, San Marino, and Vatican City [Citation15], but these countries were not included in our study as they were small, not members of the EU and did not plan to join the EU [Citation16]. Another anomaly is the Faroe Islands of Denmark, where abortion is not available although they are part of Denmark.
There have not been significant changes in abortion rates in most European countries within the last decade except in some of them, especially in Estonia where abortion rates changed the most having gone from a very high 27 per 1000 women in 2007 to an average 14 per 1000 women in 2017. This significant decline has also been observed in former Soviet Union countries when effective contraception became more available.
No statistical data are available from Austria as abortion costs are not covered by social security and no other reporting system is in place. The official data from Poland represent only a fraction of the abortion performed in reality due to the illegal status of abortion on request. In Hungary, mifepristone is not available despite being approved.
Strengths and weaknesses
Our study has some limitations. Regarding missing data, not all of the countries and not all of the information was included in this follow-up due to lack of data and/or correspondents. Data on illegal or other unreported terminations of pregnancy are missing: immigrants or women crossing borders to have pregnancies terminated are not included as in most countries there is no requirement to report them. There can be disparities with unofficial figures especially in countries with restricted access to abortion due to reporting only being required from public institutions but not private ones. Regarding the correspondents, there could be bias in their selection and because of their voluntary nature.
In addition, it is clear that more coherent and consistent reporting of abortion numbers is needed, as well as uniform definitions of abortion terms and types, age criteria, and statistical measures. For instance, induced abortion, the ‘intentional loss of an intrauterine pregnancy due to medical or surgical means’ is the term used in the 11th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10), the list of medical classifications by the WHO [Citation17]. However, it is sometimes used interchangeably with ‘termination of pregnancy’ depending on the country in which the term is used. Furthermore, the Corona crisis has had an impact on abortion provision, making it more difficult in some cases but also facilitating access for some women as with the approval of telemedicine. However, we could not include data on this aspect because it has occurred recently and most national abortion statistics have a longer delay before they are published. Future studies should analyse this aspect.
Our study also has strengths. To the best of our knowledge no other study compares legislation information and statistical data between European countries, except the study by Gissler et al. [Citation5]. Information on abortion legislation and statistics can be collected from a myriad of websites addressing abortion legislation and statistics on the Internet. However, abortion is a conspicuous and controversial topic on the Internet. In addition, information is most often directed at women and is prepared by anti-abortion groups which makes the reliability of the information problematic [Citation10,Citation18–21]. Focussing on official websites helps narrow down the search and improve the quality of collected information. From a legislative standpoint, there is the Global Abortion Policies Database from WHO’s Department of Reproductive Health and Research which allows for comparisons [Citation22]. Additionally, the World Abortion Laws Map from the Centre for Reproductive Rights allows for visual comparisons of the legal status of abortion across the globe [Citation23]. Other websites such as the UN, the IPPF EN, and the Guttmacher Institute provide useful reports, newsletters, and fact sheets [Citation8,Citation24,Citation25]. From a statistical standpoint, the search is even more difficult. http://data.un.org/ [Citation24] provides abortion rates from countries around the globe for the period between 1996 and 2005. The WHO website provides a fact sheet from 2012 with numbers by continent [Citation26]. Otherwise, it is necessary to look for individual countries websites to retrieve the type of information provided in this article. Community-based or geographically remote health care professionals may not be able to take advantage from the academic model of online information searches to retrieve evidence-based information [Citation27]. Moreover, websites on abortion generally gather data on only one aspect: legislation, methodology, abortive medicines’ commercialisation, global or regional or national statistics. They do not address all the aspects of access to abortion, national guidelines, off label use, and do not allow for easy nor rapid comparisons between countries. Furthermore, all of the national websites are written in the national language with a huge variation concerning the amount of information provided in English. This article which makes available legislation and statistics in the same place bridges these gaps. In addition, most of the data used for this analysis have been validated by national correspondents.
Open questions and future research
The data collected for this study are also displayed on a website: www.abort-report.eu. This website is easily accessible and facilitates information and comparisons between participating countries from all over Europe (EU plus Iceland, Norway, Serbia, and Switzerland) at a glance and allows going back to 10 years earlier, the website being updated in a yearly basis with the help of correspondents in each country. Finding correspondents and maintaining their participation to update the present data is the new challenge.
Today, the European legislation is still heterogenous in the studied countries, which is an indication that it is neither based on evidence nor on the needs of women concerned; also, abortion rates widely vary between countries, confirming that laws do not influence abortion rates [Citation28]. This compilation may help to change laws and orient them on the real needs of women with unwanted pregnancies. A project to standardise data collection in Europe would be a step forward to improve the comparison of abortion statistics between countries. Moreover, linking these statistics with other underlying factors possibly correlated to abortion rates, such as income level or birth rate, would make them more intelligible.
Supplemental Material
Download MS Word (63.9 KB)Acknowledgements
The authors are extremely grateful to the correspondents who have freely completed questionnaires on legislation and abortion statistics, in particular: Drs Nausikaä MARTENS (Belgium), Vesna STEPANIC (Croatia), Øjvind LIDEGAARD (Denmark), Helle KARRO (Estonia), Oskari HEIKINHEIMO (Finland), Ines THONKE (Germany), Gyula CSERMELY (Hungary), Catherine CHERY (Luxembourg), Mette LØKELAND (Norway), Krystyna KACPURA (Poland), Sharon CAMERON (Scotland), Bojana PINTER (Slovenia), Helene HULDI (Switzerland). They want to thank Fabienne PÉRETZ and Carolina ROJIDO (Abelia Science) for their assistance in preparing the manuscript. Medical writing assistance was funded by Exelgyn.
Disclosure statement
The authors were all members of the external scientific advisory board of Exelgyn at the time of the manuscript preparation and writing. CF has served on an ad hoc basis as an invited lecturer for Exelgyn; AA is a board member at Nordic Pharma and MSD, and an investigator for some Nordic Pharma studies; TB is a member of advisory boards for Merck and HRA, has an occasional consultancy relationship with Exelgyn and Nordic, and is a speaker in conferences/symposiums organised by Bayer, Merck, HRA, Gedeon and Exelgyn; RL has a financial relationship (member of advisory boards, lecturer, and/or consultant) with Exelgyn, Nordic Pharma, Exeltis, Bayer Pharma, and Teva; ML has an occasional consultancy relationship with Exelgyn and Nordic; MP has an occasional consultancy relationship with Exelgyn and Nordic; KGD: reimbursement and fees for advisory boards or speakers from Exelgyn, HRA Pharma, LinePharma, Mithra, Bayer AG MSD/Merck, Exeltis, Gedeon Richter, Natural Cycles, MedinCell, Actavis, Ferring, and Myovant.
References
- Doran F, Nancarrow S. Barriers and facilitators of access to first-trimester abortion services for women in the developed world: a systematic review. J Fam Plann Reprod Health Care. 2015;41(3):170–180.
- Bajos N, Rouzaud-Cornabas M, Panjo H, et al. The French pill scare: towards a new contraceptive model? Popul Soc. 2014;5:4. Available from: https://www.ined.fr/fichier/s_rubrique/19893/population_societies_2014_511_pill_scare.en.pdf
- Lima JM, Reeves A, Billari F, et al. Austerity and abortion in the European Union. Eur J Public Health. 2016;26(3):518–519.
- Parliamentary Assembly of the Council of Europe. Resolution 1607, Access to safe and legal abortion in Europe; 2008 Apr 16. Available from: http://assembly.coe.int/nw/xml/XRef/Xref-XML2HTML-en.asp?fileid=17638.
- Gissler M, Fronteira I, Jahn A, et al. Terminations of pregnancy in the European Union [published correction appears in BJOG. 2012 Mar;119(4):516]. BJOG. 2012;119(3):324–332.
- Gibson L. WHO puts abortifacients on its essential drug list. BMJ. 2005;331(7508):68.
- Gynuity Health Projects. List of mifepristone approvals; 2017 June 1. Available from: https://gynuity.org/resources/list-of-mifepristone-approvals.
- International Planned Parenthood Federation European Network. Available from: https://www.ippfen.org.
- Central Intelligence Agency. The world factbook. Available from: https://www.cia.gov/the-world-factbook/.
- Altshuler AL, Gerns Storey HL, Prager SW. Exploring abortion attitudes of US adolescents and young adults using social media. Contraception. 2015;91(3):226–233.
- Ministère des Solidarités et de la Santé. Publication du rapport de la Commission sur les données et la connaissance de l’interruption volontaire de grossesse (IVG); 2016 July 27. Available from: https://drees.solidarites-sante.gouv.fr/etudes-et-statistiques/publications/communiques-de-presse/article/publication-du-rapport-de-la-commission-sur-les-donnees-et-la-connaissance-de-l.
- BBC News. Date set for Isle of Man abortion reform to come into force. BBC News. 2019 Feb 21. Available from: https://www.bbc.com/news/world-europe-isle-of-man-47311669.
- BBC News. Eighth Amendment repealed as Irish president signs bill into law. BBC News. 2018 Sept 18. Available from: https://www.bbc.com/news/world-europe-45568094.
- THE IRISH TIMES, NI secretary can direct establishment of abortion services, judge rules. THE IRISH TIMES. 2022 Feb 8. Available from: https://www.irishtimes.com/news/crime-and-law/ni-secretary-can-direct-establishment-of-abortion-services-judge-rules-1.4796919.
- US News. Abortion not allowed in these European countries. US News. 2018 May 24. Available from: https://www.usnews.com/news/best-countries/articles/2018-05-24/these-countries-in-europe-have-the-strictest-abortion-laws
- European Union. About the EU. Countries. Available from: https://europa.eu/european-union/about-eu/countries_en.
- ICD-11 for Mortality and Morbidity Statistics. Pregnancy, childbirth or the puerperium. 2020 Sept. Available from: https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/1517114528.
- Swartzendruber A, Newton-Levinson A, Feuchs AE, et al. Sexual and reproductive health services and related health information on pregnancy resource center websites: a statewide content analysis. Womens Health Issues. 2018;28(1):14–20.
- Conti JA, Cahill E. Abortion in the media. Curr Opin Obstet Gynecol. 2017;29(6):427–430.
- Bryant AG, Narasimhan S, Bryant-Comstock K, et al. Crisis pregnancy center websites: Information, misinformation and disinformation. Contraception. 2014;90(6):601–605.
- Kavanaugh ML, Bessett D, Littman LL, et al. Connecting knowledge about abortion and sexual and reproductive health to belief about abortion restrictions: findings from an online survey [published correction appears in Womens Health Issues. 2013 Sep–Oct;23(5):e327]. Womens Health Issues. 2013;23(4):e239–e247.
- World Health Organization (WHO). Global abortion policies database. Available from: https://abortion-policies.srhr.org/.
- Center for Reproductive Rights. Available from: https://reproductiverights.org/worldabortionlaws.
- United Nations Statistics Division. UNdata. A world of information. Available from: https://data.un.org/.
- Guttmacher Institute. International abortion. Legality and safety. Available from: https://www.guttmacher.org/international/abortion/legality-and-safety.
- World Health Organization (WHO). Sexual and reproductive health. Publications. Facts on induced abortion worldwide; 2012 Jan. Available from: https://www.who.int/reproductivehealth/publications/unsafe_abortion/abortion_facts/en/.
- Younger P. Internet-based information-seeking behaviour amongst doctors and nurses: a short review of the literature. Health Info Libr J. 2010;27(1):2–10.
- Rowlands S. Abortion: a disunited Europe. J Fam Plann Reprod Health Care. 2015;41(3):164–167.