
Abstract
Objective: Stress describes the physiological reaction to threat or pressure, which manifests as physical symptoms of exhaustion or energy loss and psychological symptoms, including irritability or tension. If untreated, chronic stress or burnout may develop, both are areas of unmet medical need. Evidence-based treatment and prevention measures are needed.
Methods: Prevention strategies and existing treatment options for stress-related symptoms were evaluated to establish criteria for an adequate pharmacological approach to stress. The authors reviewed the literature to reach a clinically meaningful strategy for prevention and treatment of persistent stress symptoms and their consequences, including burnout and secondary diseases.
Results: Current medication reveals a treatment gap. Most drugs target only psychological or physical stress symptoms. Furthermore, psychotropic medications sometimes prescribed for stress often have unacceptable side effects and bear a risk of overtreatment. Ideally pharmacological therapy should afford comprehensive treatment of all stress symptoms with a favourable safety profile.
Conclusions: Rhodiola rosea extract (RRE) fulfils important requirements. It is the main adaptogen approved by the HMPC/EMA for the indication ‘stress’ and influences the release of stress hormones while boosting energy metabolism as revealed in animal literature. RRE offers comprehensive treatment of stress symptoms and can prevent chronic stress and stress-related complications.
Keywords:
Introduction
Stress describes the physiological reaction to environmental threats or pressures, which can be self-driven e.g., striving for perfection, high ambition or external such as social pressures, excessive demands or workloads. Although the body may initially adapt to perform under stress, it soon becomes dysfunctional if stress persists and has a too high intensity. Stress manifests itself in a wide variety of both physical and psychological symptoms, has a negative impact on performance and leads to absence from work. Work-related stress occurs across all groups of society and affects 22% of the European workforce. It is a crucial factor in 50–60% of all lost working days (Milczarek, Schneider, & González, Citation2009) with a rising trend. In 2016, a survey of a large German health insurance company revealed that over 60% of survey participants are now more stressed than in 2013 (Techniker Krankenkasse, Citation2016). The World Health Organization (WHO) has called stress ‘the health epidemic of the 21st century’.
If stress persists and is left untreated, it can result in serious health problems including burnout and secondary conditions, e.g., depression, anxiety, cardiovascular, gastrointestinal, neurological or musculoskeletal disease or diabetes – consequently with higher costs to the community and a higher impact on individuals’ lives. The main implications for individuals related to health impairment are lower income and reduced quality of life. However, stress has not only individual, but also social and economic consequences. Organisations are affected by rising costs related to sick leave, reduced productivity and higher staff turnover (European Agency for Safety and Health at Work [EU-OSHA], Citation2014).
Methods
The authors reviewed the current literature to identify and assess prevention strategies and treatment options for stress-related symptoms and thus established criteria for an adequate and holistic pharmacological approach to stress. The aim of this process was to propose a consensus for prevention and treatment of symptoms of persistent stress as well as for prevention of health consequences of stress such as burnout and secondary diseases. In this review article we have outlined current understanding of the pathophysiology of stress and identified the areas of greatest clinical need for intervention, which occurs at two stages: as a preventive treatment for a patient with stress to avoid the development of chronic stress and for those already suffering from persistent stress, an appropriate therapy to avoid burnout and secondary diseases. Assessment of prevention and treatment strategies identified some non-pharmacological approaches and some pharmacological approaches which have shown limited efficacy targeting the symptoms of stress and these are outlined below. The literature review process identified a significant amount of data on the clinical effects of Rhodiola rosea extract (RRE) on stress and stress-related disorders and mechanistic studies allude to the ability of RRE to normalise stress and boost energy levels. Thus, in the latter part of this review article we have focused our attention on RRE as a specific pharmacological approach to stress management.
Stress, allostatic state and allostatic (over)load
In 1936 Hans Selye postulated the so-called general adaptation syndrome which describes the stereotyped response of an organism in reaction to a stressor. This syndrome consists of three stages. The first stage is the alarm reaction (‘fight or flight’ response) in which resources are mobilised to maintain homeostasis. This has subsequently been termed as allostasis, which describes the biological response to stressors to promote stability through change (McEwen, Citation2000). Primary mediators of allostasis include, but are not confined to, hormones of the hypothalamic-pituitary-adrenal (HPA) axis, catecholamines and cytokines.
Restoration of allostasis leads to the second stage of resistance, in which defence and adaptation are sustained and optimal. However, many current stressors are persistent and can lead an organism into stage three where the body’s capacity to withstand them is surpassed by the consequences of exhaustion and depleted reserves. Extreme psychological stress impacts on the complex regulation of emotion by the brain and on human psychological resilience and vulnerability to psychopathology (Charney, Citation2004).
The concepts of allostasis and allostatic load link the protective and survival values of the acute response to stress to the adverse consequences that result if the acute response persists and becomes chronic (McEwen & Wingfield, Citation2003). An allostatic state may result from an imbalance of the primary mediators, reflecting excessive production of some and inadequate production of others (McEwen, Citation2005). In some cases, the stress mediators themselves can turn on the body and cause problems. If recovery from the acute event is not accompanied by an adequate homeostatic response to terminate the acute adaptive response of stress mediators, the deleterious effects on psychological and physiological function termed allostatic load occur. The allostatic load is the burden borne by a brain and body adapting to challenges, both physiological and psychological. A sustained allostatic state may ensue, termed allostatic overload. The tipping point for allostatic overload will vary among individuals. It manifests as disease e.g., chronic hypertension and the generation of atherosclerotic plaques, elevated glucocorticoids leading to insulin resistance and increased risk for cardiovascular disease, immunosuppression or elevation of inflammatory cytokines (see below).
Pathomechanism, symptoms and health consequences of chronic stress
The symptoms of stress can be multiple and affect many organ systems. The physiological stress response involves stimulation of the autonomic nervous system (ANS) and the hormonal system, with potentially negative impact on the cardiovascular system, the musculoskeletal system, the immunological system and others ().
Figure 1. Multi-faceted symptoms of stress.
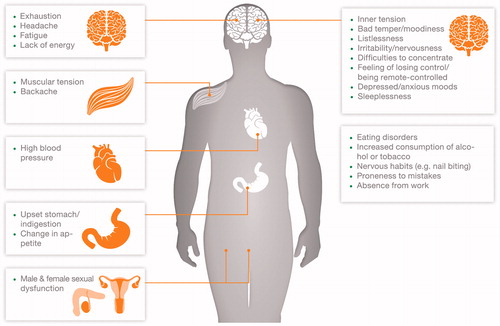
Fatigue and exhaustion manifest as key physical stress symptoms. Others can be gastrointestinal symptoms, headache, backache or sexual dysfunction. Psychological and emotional symptoms of stress include e.g., tension, irritability, anxious or depressive mood, bad temper and the feeling of losing control. Concomitantly, changes in cognition, including forgetfulness and inability to concentrate may occur. Behavioural symptoms of stress include social withdrawal, alcohol and cigarette abuse, eating disorders, proneness to mistakes and work absence (Edwards, Heufelder, & Zimmermann, Citation2012; Milczarek et al., Citation2009).
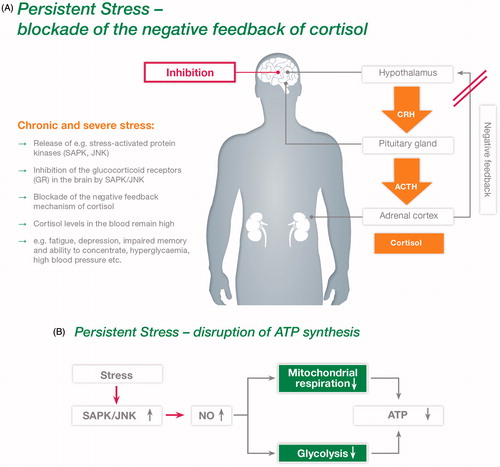
These symptoms result from several postulated pathomechanisms. The HPA axis is one of the main stress response pathways. Stress induces the release of corticotropin releasing hormone (CRH) in the hypothalamus. This activates the pituitary gland to release adrenocorticotropic hormone (ACTH). The latter stimulates the release of adrenaline, noradrenaline and cortisol in the adrenal gland. The actions of this hormone system are tightly regulated normally to ensure that the organism can respond quickly and adequately to stress, via negative feedback mechanisms, levels of hormones e.g., cortisol return to normal values.
Chronic stress, however, results in persistently elevated levels e.g., of cortisol, as demonstrated in animal and cell models. Studies of rabbits under immobilisation stress revealed an activation of e.g., stress-activated protein kinase/Jun N-terminal protein kinase (SAPK/JNK) (Panossian, Hambardzumyan, Hovhanissyan, & Wikman, Citation2007). Previous studies, e.g., with mouse hippocampal (HT22) cells, indicate that JNK leads to an inhibition of glucocorticoid receptor function. This again results in a blockade of the negative feedback mechanism of cortisol release (see ; Panossian, Citation2013; Panossian et al., Citation2007; Wang et al., Citation2005). Consequently, cortisol levels in the blood remain high which may lead to fatigue, depression, impaired cognitive performance, hyperglycaemia, high blood pressure and other health problems as a long-term consequence.
Figure 2 (A) Postulated pathomechanisms of stress: persistent stress leads to a blockade of the negative feedback of cortisol. (Adapted from Panossian, Citation2013; Panossian et al., Citation2007). (B) Postulated pathomechanisms of stress: persistent stress leads to a disruption of ATP synthesis. (Adapted from Panossian & Wikman, Citation2009).
At the intracellular level, high cortisol levels impact on the balance between trophic and atrophic factors within neurones, thus affecting neurogenesis and brain plasticity in the hippocampus and frontal cortex, which results in neurodegenerative changes involved in mood regulation (Gould & Tanapat, Citation1999).
Investigations with rat cells showed that the release of SAPK leads to an increase in nitric oxide (NO) release (Guan, Buckman, Springer, & Morrison, Citation1999). The latter impairs both glycolysis and mitochondrial function which results in a decrease in adenosine triphosphate (ATP) synthesis (see ; Brown, Citation2001; Giulivi, Citation1998). Low ATP levels are associated with symptoms such as loss of energy, fatigue and exhaustion (Panossian, Citation2013; Panossian & Wikman, Citation2009).
A role of inflammatory mechanisms involving cytokines has also been hypothesised in chronic stress-related mental diseases, such as depression, anxiety or dementia (Bagyinszky et al., Citation2017; Kim et al., Citation2017).
An association between type 2 diabetes and depression has recently been explained, to some extent, by unspecific pathophysiological mechanisms involved in the stress response (Berge & Riise, Citation2015). Chronic stress is also associated with an increased risk of cardiovascular disease (CVD) (Bot & Kuiper, Citation2017; Nabi et al., Citation2013). Long-term work stress accounts for an estimated 16% of male and 22% of female CVD in the EU (Houtman, Citation2005). Recent studies report that the activity of the amygdala, a key component of the brain involved in emotion and stress, is of predictive value for the incidence of acute cardiovascular events during a median follow up period of 3.7 years among nearly 300 individuals with no prior history of CVD (Tawakol et al., Citation2017).
Burnout
Burnout is a stress disorder of unspecific risk stage which is characterised by symptoms of mental exhaustion and physical fatigue, cynicism or depersonalisation and reduced personal accomplishment (Hochstrasser et al., Citation2016). It represents a risk factor not only for psychiatric diseases such as depression and anxiety, but also for cardiovascular, metabolic and other somatic diseases. Work-related burnout has been associated with an increased 10-year mortality risk (Ahola, Väänänen, Koskinen, Kouvonen, & Shirom, Citation2010). Thus, the prevention of burnout deserves special attention.
The usual non-pharmacological treatment is cognitive behavioural therapy or psychotherapy and there is currently no specific pharmacological treatment for burnout. Several biomarkers have been tested for association with burnout, but the results are contradictory and there are currently no established biochemical markers which can be considered as reliable indicators for burnout (Danhof-Pont, van Veen, & Zitman, Citation2011).
Stress-vulnerability and resilience, respectively, play an important role in the predisposition for, or resistance against, burnout and are an area of focus in stress research. The stress-vulnerability model was first hypothesised by Zubin and Spring (Citation1977) to identify and treat relapses of mental illness. It suggests that people inherit a genetic predisposition to mental illness. This vulnerability in itself is not sufficient to manifest the disorder and requires interaction with bio-pyscho-social stressors (Goh & Agius, Citation2010). Increased vulnerability is potentially influenced by genetic factors and/or individual stress experience and may lead to decreased resilience to stress. Conversely, stress overload and burnout may be prevented by enhancing resilience. Hence, the prevention of burnout and exhaustion by enhancement of resilience on the one hand and by the adequate treatment of stress symptoms on the other is very important and appears to be an area of a considerable unmet medical need.
Stress management strategies
Popular coping strategies, such as distraction, physical activities, relaxation, socialising and healthy food, may be employed in order to get out of the stressful situation with the aim of regaining inner calm and strength. The usual form of care for work-related chronic stress is coaching, using a cognitive-behavioural approach whose primary aim is to reduce symptoms and improve functioning (Schoutens, Frings-Dresen, & Sluiter, Citation2016). As an alternative non-pharmacological approach, mindfulness-based stress reduction is a clinically standardized meditation technique that has demonstrated an effect on stress reduction in healthy people, with benefit similar to that of standard relaxation training (Chiesa & Serretti, Citation2009).
However, many modern stressors are persistent and the body’s capacity to withstand them is surpassed by the consequences of exhaustion and depleted reserves, leading to burnout (German Association for Psychiatry, Psychotherapy and Psychosomatics [DGPPN], Citation2012). Thus, as mentioned above, the areas of unmet clinical need for intervention may be identified in two stages: as a preventive treatment in a patient with stress or a lack of vitality to avoid the development of chronic stress or exhaustion, and secondly, as a first-line treatment when persistent stress and exhaustion are present, to avoid burnout and secondary diseases. It should not be the goal of a treatment strategy to make one keep going while neglecting the signs and symptoms of exhaustion, but rather to assist in coping with temporary unusual demands, allowing for rapid readaption to normal states once the stressful situation has subsided.
Pharmacological interventions
If stress symptoms persist, together with continuously demanding life circumstances that cannot easily be avoided, pharmacological intervention may become necessary to prevent serious mental and social sequelae. However, current pharmacotherapy reveals a treatment gap. Many herbals, vitamin combinations or prescription medicines tend to focus only on single symptoms, rather than comprehensively on all aspects of stress or burnout. Besides, psychiatric prescription drugs like antidepressants, anxiolytics or β-blockers are mostly indicated for more severe diseases, such as depression or anxiety and there is a risk of overtreatment including severe side effects and/or risk of dependency.
Herbal treatment options or other drugs available over-the-counter (OTC) tend to focus either on increasing/preserving energy reserves (treatment of physical symptoms) or on promoting relaxation (treatment of psychological symptoms). For example: those acting as energisers, including vitamins/minerals and tonics; and those acting on mood, relaxation and sleep, such as St. John’s wort, valerian, passion flower, lavender and antihistamines. An ideal pharmacological therapy should offer a comprehensive treatment of all relevant stress symptoms combined with a favourable safety profile.
Adaptogens
The term ‘adaptogen’ is used to describe medicinal plants that have the capacity to normalise body functions and strengthen systems compromised by stress and are able to enhance the ‘state of non-specific resistance’ of an organism to stress described above as allostasis. The Committee on Herbal Medicinal Products (HMPC) which is the European Medicines Agency’s (EMA) committee responsible for compiling and assessing scientific data on herbal substances, preparations and combinations developed the reflection paper on the adaptogenic concept (EMA, Citation2008).
In this paper, adaptogens are defined as virtually non-toxic to the recipient. They are non-specific in pharmacological properties and act by increasing the resistance of an organism to a broad spectrum of adverse biological, chemical and physical factors. Adaptogens act as regulators with a normalising effect on the various organ systems and their effect is the more pronounced the deeper the pathologic changes in the organism are.
As such, adaptogens should be differentiated from traditional herbal medicinal products of related action, such as tonics and stimulants. The EMA has established HMPC monographs on many herbals including some adaptogens, i.e., preparations deriving from Eleutherococcus senticosus, Panax ginseng and Rhodiola rosea. These monographs cover their therapeutic use and safety as registered drugs.
Rhodiola rosea extract (RRE)
Extract from the roots and rhizomes of Rhodiola rosea (RRE) is an adaptogen that acts to increase the body’s resistance to stress, exhaustion and fatigue. It is the main adaptogen given the indication ‘stress’ by the HMPC (European Medicines Agency’s [EMA], Citation2011, Citation2012). A wide variety of preclinical in vivo and ex vivo studies conducted in cell lines and animal models have elucidated the presence of several biochemical and pharmacological stress-reducing actions of RRE. It possesses a unique mechanism of action: it normalises the release of stress hormones while simultaneously boosting energy metabolism via activation of ATP synthesis in mitochondria (; Abidov, Crendal, Grachev, Seifulla, & Ziegenfuss, Citation2003; Olsson, von Schéele, & Panossian, Citation2009; Panossian et al., Citation2007). Blood levels of several stress mediators (e.g., p-SAPK/p-JNK, NO, cortisol) were assessed in rabbits under immobilisation stress; in the animals under stress that received placebo the levels of the above-mentioned markers were significantly elevated while in animals which received RRE (1 mg/kg for seven days) the stress mediators remained virtually unchanged (Panossian et al., Citation2007). In other studies, rats treated with RRE (50 mg/kg) exhibited a significantly prolonged duration of exhaustive swimming in comparison with untreated rats. Furthermore, RRE induced the (re)synthesis of ATP in rat mitochondria from skeletal muscles and stimulated recovery after exercise (Abidov et al., Citation2003).
Figure 3. Proposed model for the mode of action of Rhodiola rosea extract (RRE): normalisation of stress hormone release and activation of ATP synthesis.
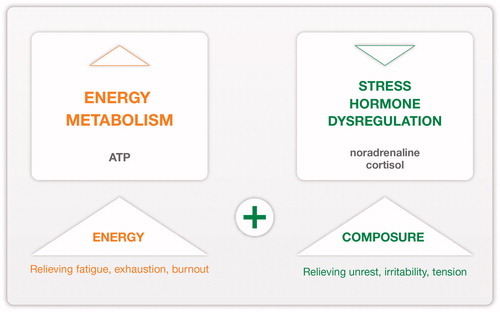
RRE acts to normalise cortisol synthesis potentially through inhibition of the SAPK pathway involved in the pathogenesis of glucocorticoid resistance, which is also found in certain chronic immune/inflammatory diseases and in some patients with depression (Panossian, Citation2013; Panossian et al., Citation2007). At the same time, through inhibition of the SAPK/JNK pathway, RRE potentially prevents the formation of NO and the associated decline in ATP synthesis (Guan et al., Citation1999; Panossian & Wikman Citation2009).
Stress leads to a damage of the mitochondrial function and the excessive production of reactive oxidative species (ROS) in mitochondria, which may cause damage e.g., to proteins, nucleic acids, and membranes, which in turn can lead to activation of cell death processes such as apoptosis (Zhang, Wu, Lu, Guo, & Ma, Citation2006). RRE may also offer potential protection against heart and brain diseases (e.g., heart attack, stroke, depression and Alzheimer’s disease) through anti-oxidative/anti-inflammatory mechanisms (Lee et al., Citation2013; Olpe & Seifritz, Citation2014; Zhang et al., Citation2016).
RRE products with medicinal drug status must fulfil high pharmaceutical requirements with regard to their quality and safety, e.g., products containing RRE WS® 1375 (Rosalin®). It should also be noted that there are many dietary supplements available which contain Rhodiola rosea drug or extracts that do not comply with the high standards set by the HMPC and pharmaceutical quality requirements for registered medicinal drugs.
Clinical studies with RRE
In several clinical studies of stress, burnout and chronic fatigue, RRE was found to be effective, safe and well tolerated.
Stress symptoms
In clinical studies, mental work capacity, attention, task performance and overall mood improved during the course of treatment with RRE and stress and self-reported mild anxiety were reduced (; e.g., Cropley, Banks, & Boyle, Citation2015; Darbinyan et al., Citation2000; Edwards et al., Citation2012; Heldmann, Roth, Dienel, & Münte, Citation2016).
Table 1. Clinical studies with Rhodiola rosea extract (RRE) in subjects with stress symptoms.
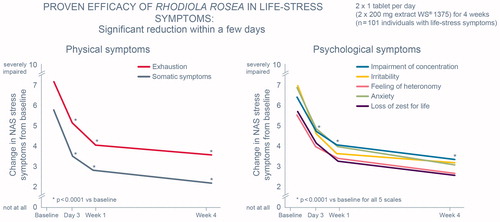
Among people suffering from life-stress symptoms, clinically relevant improvement in stress symptoms, stress-related disabilities in work, social and family life, functional impairment and overall therapeutic effect were observed with RRE treatment over four weeks (; Edwards et al., Citation2012). In this single-arm study, adult subjects with life-stress symptoms (n = 101) treated in general practice received open-label RRE (200 mg, twice-daily). Seven widely recognised questionnaires to cover various aspects of stress symptoms and psychological well-being were employed to assess the outcome of treatment. Invariably, all outcome variables showed significant, consistent and steady improvement in stress symptoms, fatigue, quality of life, mood, concentration, disability, functional impairment and overall therapeutic effect. The improvements were observed as early as after three days of treatment and continued throughout the whole study duration of 28 days.
Figure 4. Efficacy of Rhodiola rosea extract (RRE) in management of life stress symptoms. NAS: Numerical Analogue Scales-rating of symptoms from 0 (not at all) to 10 (severely impaired). (Adapted from Edwards et al., Citation2012).
RRE has also demonstrated positive effects in the treatment of symptoms of mild anxiety associated with stress. Among students with self-reported anxiety and stress (n = 81) who were randomised to receive either RRE or a control (no treatment), the RRE group reported a significant reduction in self-reported anxiety, anger, confusion, stress and vigour at 14 days and a significant improvement in total mood as compared with the no treatment group (Cropley et al., Citation2015).
The effect of RRE on neuropsychological and neurophysiological measures of attention and mental resource allocation has recently been studied (Heldmann et al., Citation2016). The results of this trial of 50 healthy volunteers (aged 30–50 years) at risk for stress symptomatology showed increased performance under multi-tasking conditions over the course of RRE administration for 12 weeks. Overall, RRE had a positive influence on attention and mental resource allocation and thus on speed and quality of performance under conditions of high cognitive demand.
In an earlier study, the effect of RRE on healthy physicians on night duty (n = 56) was evaluated using a combination of tests that measured overall level of mental fatigue, involving complex perceptive and cognitive cerebral functions, such as associative thinking, short-term memory, calculation and ability of concentration and speed of audio-visual perception. A significant improvement in these test results was observed in the RRE group during the two-week treatment period, suggesting that RRE can reduce general fatigue under certain stressful conditions (Darbinyan et al., Citation2000).
Chronic fatigue symptoms and exhaustion
Unexplained chronic fatigue is a widespread healthcare problem that significantly affects the working population (Jackson & Macleod, Citation2017) and which is often associated with stress. First-line treatments are cognitive behavioural or graded exercise therapy (Daniels & Loades, Citation2017). However, these treatments yield only moderate effect sizes. RRE is shown to improve mental performance in people with stress-related fatigue and further to improve all dimensions of chronic fatigue symptoms (; Lekomtseva, Zhukova, & Tartakovsky, Citation2013; Olsson et al., Citation2009).
Table 2. Clinical studies with Rhodiola rosea extract (RRE) in subjects with chronic fatigue.
In a double-blind study, participants (n = 60) selected according to diagnostic criteria for fatigue syndrome were randomised to receive RRE (576 mg extract/day) or placebo for four weeks. Significant effects of RRE in comparison with placebo were observed for symptoms of fatigue (Pines burnout scale) and in tests of attention (Connors computerised continuous performance test II [CCPT II]). Pre- versus post-treatment cortisol responses to awakening were significantly different in the treatment group compared with the control group. Thus, RRE is found to exert an anti-fatigue effect that increases mental performance, particularly the ability to concentrate and decreases cortisol response to awakening stress in burnout patients with fatigue syndrome (Olsson et al., Citation2009).
Significant improvements in specific chronic fatigue outcomes (e.g., multi-dimensional fatigue inventory 20 [MFI-20], recent perceived stress questionnaire [PSQ-R], Sheehan disability scale [SDS]) have been demonstrated with RRE treatment among 101 patients with chronic fatigue treated in an open-label, single-arm study for up to eight weeks (p < .001). Furthermore, the results of the trial supported the therapeutic effect on concomitant conditions related to chronic fatigue such as mood, concentration, quality of life and general well-being which was demonstrated with RRE treatment (200 mg, twice-daily; Lekomtseva et al., Citation2013).
Burnout symptoms
The aim of the treatment of stress and burnout with an adaptogen is to increase stress resistance, thus addressing the source rather than the symptoms of the syndrome and preventing subsequent diseases associated with a history of burnout. The core indicators of burnout are subjective perceptions of chronic demand-related stress with subsequent emotional exhaustion and decreased performance in work-related or self-set tasks. Reported symptoms of burnout comprise not only psychiatric or mood disorders such as fatigue, cynicism, impaired sexual life, lack of concentration or a generally negative attitude toward work, but also somatic symptoms such as headaches, hypertension or irritable stomach. Treatment with RRE for eight and 12 weeks, respectively, was accompanied by a clear improvement in burnout symptoms (; Goyvaerts & Bruhn, Citation2012; Kasper & Dienel, Citation2017).
Table 3. Clinical studies with Rhodiola rosea extract (RRE) in subjects with burnout symptoms.
Investigating the effects of RRE on burnout-related symptoms, a German non-interventional study was conducted in 128 primary care practices and included 330 patients with two or more burnout indicator symptoms (exhaustion, depression, insomnia, fatigue or drop in performance). A considerable alleviation of these symptoms after the administration of RRE for eight weeks was reported based on the results of the self-rating questionnaires used in this trial (Goyvaerts & Bruhn, Citation2012).
An exploratory single-arm, multi-centre study investigated the clinical outcomes in burnout patients (n = 118) treated with RRE (200 mg, twice-daily) over 12 weeks. The aim of the treatment with RRE was to increase stress resistance and thus to aim at the source rather than at the symptoms of the syndrome and to further prevent subsequent diseases associated with a history of burnout. A broad spectrum of rating scales was employed to evaluate the therapeutic effect of RRE in the treatment of burnout symptoms, such as fatigue, cynicism, difficulties to concentrate, impaired sexual life and also somatic symptoms. A wide range of the evaluated outcome measures improved considerably over the course of treatment. Some of these changes were already significant after the first week of RRE administration (Kasper & Dienel, Citation2017).
The trials to date, although limited in participant numbers and often exploratory in design, nonetheless provide promising results and an encouraging basis for future randomised controlled trials further investigating the clinical outcomes of RRE in patients with high symptom load of chronic stress, chronic fatigue and burnout. Clinical experience of sexual problems in individuals that were predominately due to stress have been helped by RRE and recent studies involving male and female stressed rats have confirmed this finding (Edwards, Eltbogen, & Nöldner, Citation2017; Edwards, Kumar, & Nöldner, Citation2016). RRE has also shown encouraging data in exploratory studies of diseases that can occur as a consequence of stress, including depression (Darbinyan et al., Citation2007) and anxiety (Bystritsky, Kerwin, & Feusner, Citation2008).
Safety and tolerability of RRE
RRE presents a very favourable safety profile. In clinical studies, no serious side effects that could be attributed to RRE were reported (e.g., Cropley et al., Citation2015; Edwards et al., Citation2012; Kasper & Dienel, Citation2017; Lekomtseva, Zhukova, & Wacker, Citation2017).
The HMPC monograph on Rhodiola rosea roots and rhizomes states that there are no known side effects (EMA, Citation2012). In addition, to date no drug-drug interactions have been reported for RRE (EMA, Citation2012).
Treatment recommendation
RRE has the potential to close the treatment gap for clinically relevant stress symptoms, which is due to its dual mode of action providing both physical and psychological symptom relief, normalising stress hormone levels and increasing energy and its excellent safety profile. RRE potentially addresses multiple aspects in the management of stress and burnout:
Prevention of stress symptoms from becoming chronic.
Treatment of stress symptoms.
Prevention of stress-related complications (burnout) and secondary diseases.
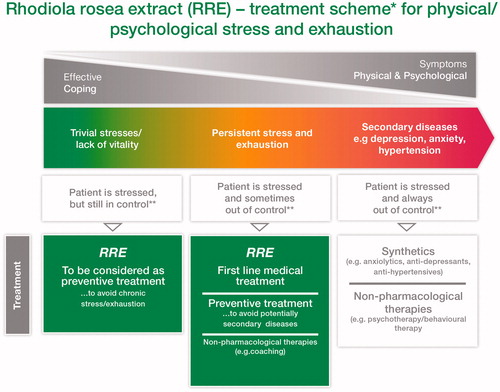
summarises the authors’ treatment recommendations for the use of RRE in various stages of stress.
Figure 5. Intervention stages for treatment of physical/psychological stress and exhaustion. Patients with medical conditions that may result in symptoms of stress and exhaustion such as anaemia, migraine, IBS (irritable bowel syndrome), cancer and hormonal disturbances, may also receive RRE after assessment and management of the medical condition. **‘Control’ in this context means: normal functioning in daily life.
Limitations
There is still much to learn about the pathophysiology of stress, resilience and stress vulnerability, including cellular and cerebral network mechanisms which are the focus of current research interests. In parallel to increasing knowledge of these phenomena, additional investigations are needed to further elucidate the impact of RRE on mechanisms that play a significant role in stress in the human body. Clinical evidence for the effect of RRE on stress and stress-related symptoms to date may be limited to studies of exploratory design; appropriate study populations are sometimes difficult to define. However, the studies so far provide promising results, especially in frequently difficult to treat populations. Further randomised controlled trials are needed to confirm the promising results of the existing studies with RRE in patients with symptoms of chronic stress, chronic fatigue and burnout.
Acknowledgements
Editorial assistance was provided by H + O communications Ltd.
Disclosure statement
Ion-George Anghelescu has received consulting fees and/or honoraria from Schwabe, Boehringer Ingelheim, Otsuka, Janssen, Lundbeck, Lilly, Medice, Servier and Trommsdorf (I.G. A.).
David Edwards reports honoraria and support within the last three years from Bayer, Besins, Pfizer and Schwabe.
Erich Seifritz has received consulting fees and/or honoraria from Schwabe, Otsuka, Janssen, Lundbeck, Eli Lilly, Servier, Hoffmann La Roche, Vifor, Takeda, Sunovion, Pfizer, Astra Zeneca and Angelini.
Siegfried Kasper has received grants/research support, consulting fees and/or honoraria within the last three years from Angelini, AOP Orphan Pharmaceuticals AG, AstraZeneca, Eli Lilly, Janssen, KRKA-Pharma, Lundbeck, Neuraxpharm, Pfizer, Pierre Fabre, Schwabe and Servier.
Additional information
Funding
References
- Abidov, M., Crendal, F., Grachev, S., Seifulla, R., & Ziegenfuss, T. (2003). Effect of extracts from Rhodiola rosea and Rhodiola crenulata (Crassulaceae) roots on ATP content in mitochondria of skeletal muscles. Bulletin of Experimental Biology and Medicine, 136, 585–587. doi:10.1023/B:BEBM.0000020211.24779.15
- Ahola, K., Väänänen, A., Koskinen, A., Kouvonen, A., & Shirom, A. (2010). Burnout as a predictor of all-cause mortality among industrial employees: A 10-year prospective register-linkage study. Journal of Psychosomatic Research, 69, 51–57. doi:10.1016/j.jpsychores.2010.01.002
- Bagyinszky, E., Giau, V. V., Shim, K., Suk, K., An, S. S. A., & Kim, S. (2017). Role of inflammatory molecules in the Alzheimer’s disease progression and diagnosis. Journal of the Neurological Sciences, 376, 242–254. doi:10.1016/j.jns.2017.03.031
- Berge, L. I., & Riise, T. (2015). Comorbidity between type 2 diabetes and depression in the adult population: Directions of the association and its possible pathophysiological mechanisms. International Journal of Endocrinology, 2015, 164760. doi:10.1155/2015/164760
- Bot, I., & Kuiper, J. (2017). Stressed brain, stressed heart? Lancet (London, England), 389, 770–771. doi:10.1016/S0140-6736(17)30044-2
- Brown, G. C. (2001). Regulation of mitochondrial respiration by nitric oxide inhibition of cytochrome c oxidase. Acta Biochimica et Biophysica Sinica, 1504, 46–57. doi:10.1016/S0005-2728(00)00238-3
- Bystritsky, A., Kerwin, L., & Feusner, J. D. (2008). A pilot study of Rhodiola rosea (Rhodax) for generalized anxiety disorder (GAD). Journal of Alternative and Complementary Medicine, 14, 175–180. doi:10.1089/acm.2007.7117
- Charney, D. S. (2004). Psychobiological mechanisms of resilience and vulnerability: implications for successful adaptation to extreme stress. The American Journal of Psychiatry, 161, 195–216. doi:10.1176/appi.ajp.161.2.195
- Chiesa, A., & Serretti, A. (2009). Mindfulness-based stress reduction for stress management in healthy people: A review and meta-analysis. Journal of Alternative and Complementary Medicine (New York, N.Y.), 15, 593–600. doi:10.1089/acm.2008.0495
- Cropley, M., Banks, A. P., & Boyle, J. (2015). The effects of Rhodiola rosea L. extract on anxiety, stress, cognition and other mood symptoms. Phytotherapy Research, 29, 1934–1939. doi:10.1002/ptr.5486
- Danhof-Pont, M. B., van Veen, T., & Zitman, F. G. (2011). Biomarkers in burnout: A systematic review. Journal of Psychosomatic Research, 70, 505–524. doi:10.1016/j.jpsychores.2010.10.012
- Daniels, J., & Loades, M. E. (2017). A novel approach to treating CFS and co-morbid health anxiety: A case study. Clinical Psychology &; Psychotherapy, 24, 727–736. doi:10.1002/cpp.2042
- Darbinyan, V., Aslanyan, G., Amroyan, E., Gabrielyan, E., Malmström, C., & Panossian, A. (2007). Clinical trial of Rhodiola rosea L. extract SHR-5 in the treatment of mild to moderate depression. Nordic Journal of Psychiatry, 61, 343–348. doi:10.1080/08039480701643290
- Darbinyan, V., Kteyan, A., Panossian, A., Gabrielian, E., Wikman, G., & Wagner, H. (2000). Rhodiola rosea in stress induced fatigue-a double blind cross-over study of a standardized extract SHR-5 with a repeated low-dose regimen on the mental performance of healthy physicians during night duty. Phytomedicine: International Journal of Phytotherapy and Phytopharmacology, 7, 365–371. doi:10.1016/S0944-7113(00)80055-0
- German Association for Psychiatry, Psychotherapy and Psychosomatics. (2012). Position paper burnout. [cited 19 May 2017]. Available from: http://www2.psychotherapeutenkammer-berlin.de/uploads/stellungnahme_dgppn_2012.pdf
- Edwards, D., Eltbogen, R., & Nöldner, M. (2017). Stress-induced female sexual dysfunction: Beneficial effect of the Rhodiola rosea extract Rosalin® (WS® 1375). The Journal of Sexual Medicine 14, e196 (P-04-004). doi:10.1016/j.jsxm.2017.03.240
- Edwards, D., Heufelder, A., & Zimmermann, A. (2012). Therapeutic effects and safety of Rhodiola rosea extract WS® 1375 in subjects with life-stress symptoms-results of an open-label study. Phytotherapy Research, 26, 1220–1225. doi:10.1002/ptr.3712
- Edwards, D., Kumar, V., & Nöldner, M. (2016). Stress-induced sexual dysfunction in rodents and humans: The Rhodiola rosea extract WS® 1375 shows clinical promise. The Journal of Sexual Medicine 13, S158 (P-01-051). doi:10.1016/j.jsxm.2016.03.201
- European Medicines Agency. (2008). Reflection paper on the adaptogenic concept. Document reference. EMEA/HMPC/102655/2007. [cited 19 May 2017]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2009/09/WC500003646.pdf
- European Medicines Agency. (2011). Community herbal monograph on Rhodiola rosea L., rhizoma et radix. Document reference. EMA/HMPC/232091/2011. [cited 19 May 2017]. Available from: www.ema.europa.eu/docs/en_GB/document_library/Herbal_-_Community_herbal_monograph/2011/09/WC500112677. pdf
- European Medicines Agency. (2012). Committee on herbal medicinal products (HMPC). Assessment report on Rhodiola rosea L., rhizoma et radix. Document reference. EMA/HMPC/232100/2011. [cited 19 May 2017]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Herbal_-_HMPC_assessment_report/2012/05/WC500127861.pdf
- European Agency for Safety and Health at Work. (2014). Calculating the cost of work-related stress and psychosocial risks. European Risk Observatory Literature Review. [cited 19 May 2017]. doi:10.2802/20493
- Giulivi, C. (1998). Functional implications of nitric oxide produced by mitochondria in mitochondrial metabolism. Biochemical Journal, 332, 673–679. doi:10.1042/bj3320673
- Goh, C., & Agius, M. (2010). The stress-vulnerability model how does stress impact on mental illness at the level of the brain and what are the consequences? Psychiatria Danubina, 22, 198–202.
- Gould, E., & Tanapat, P. (1999). Stress and hippocampal neurogenesis. Biological Psychiatry, 46, 1472–1479. doi:10.1016/S0006-3223(99)00247-4
- Goyvaerts, B., & Bruhn, S. (2012). Rhodiola rosea special extract SHR-5 in burnout and fatigue syndrome. Erfahrungsheilkunde, 61, 79–83. doi:10.1055/s-0031-1298676
- Guan, Z., Buckman, S. Y., Springer, L. D., & Morrison, A. R. (1999). Both p38αMAPK and JNK/SAPK pathways are important for induction of nitric-oxide synthase by interleukin-1β in rat glomerular mesangial cells. Journal of Biological Chemistry, 274, 36200. doi:10.1074/jbc.274.51.36200
- Heldmann, M., Roth, G., Dienel, A., & Münte, T. F. (2016). Impact of Rhodiola Rosea extract WS 1375 on electrophysiological correlates of attention allocation in a dual task paradigm. Clinical Neurophysiology, 127, e290. doi:10.1016/j.clinph.2016.05.159
- Hochstrasser, B., Brühlmann, T., Cattapan, K., Hättenschwiler, J., Holsboer-Trachsler, E., Kawohl, W., et al. (2016). Therapieempfehlungen des Schweizer Expertennetzwerks Burnout (SEB). Burnout-Behandlung Teil 1: Grundlagen[Therapy recommendations of the Swiss Expert Network Burnout (SEB). Burnout treatment part 1: Basics]. Swiss Medical Forum, 16, 538–541.
- Houtman, I. L. D. 2005. European foundation for the improvement of living and working conditions. Work-related stress. [cited 19 May 2017]. Available from: http://eurofound.europa.eu/sites/default/files/ef_files/pubdocs/2005/127/en/1/ef05127en.pdf
- Jackson, H., & MacLeod, A. K. (2017). Well-being in chronic fatigue syndrome: Relationship to symptoms and psychological distress. Clinical Psychology & Psychotherapy, 24, 859–869. doi:10.1002/cpp.2051
- Kasper, S., & Dienel, A. (2017). Multicenter, open-label, exploratory clinical trial with Rhodiola rosea extract in patients suffering from burnout symptoms. Neuropsychiatric Disease and Treatment, 13, 889–898. doi:10.2147/NDT.S120113
- Kim, T. K., Kim, J. E., Choi, J., Park, J. Y., Lee, J. E., Lee, E. H.,…Han P.L. (2017). Local interleukin-18 system in the basolateral amygdala regulates susceptibility to chronic stress. Molecular Neurobiology, 54, 5347–5358. doi:10.1007/s12035-016-0052-7
- Lee, Y., Jung, J. C., Jang, S., Kim, J., Ali, Z., Khan, I. A., & Oh, S. (2013). Anti-inflammatory and neuroprotective effects of constituents isolated from Rhodiola rosea. Evidence-Based Complementary and Alternative Medicine, 2013, 514049. doi:10.1155/2013/514049
- Lekomtseva, Y., Zhukova, I., & Tartakovsky, I. (2013). Therapy effects and safety of Rhodiola Rosea extract WS® 1375 in subjects with symptoms of chronic fatigue. The Siberian Scientific Medical Journal, 12, 73–75. doi:10.20538/1682-0363-2013-5-73-75
- Lekomtseva, Y., Zhukova, I., & Wacker, A. (2017). Rhodiola rosea in subjects with prolonged or chronic fatigue symptoms: Results of an open-label clinical trial. Complementary Medicine Research, 24, 46–52. doi:10.1159/000457918
- McEwen, B. S. (2000). Allostasis and allostatic load: Implications for neuropsychopharmacology. Neuropsychopharmacology: Official Publication of the American College of Neuropsychopharmacology, 22, 108–124. doi:10.1016/S0893-133X(99)00129-3
- McEwen, B. S. (2005). Stressed or stressed out: What is the difference? Journal of Psychiatry & Neuroscience, 30, 315–318.
- McEwen, B. S., & Wingfield, J. C. (2003). The concept of allostasis in biology and biomedicine. Hormones and Behavior, 43, 2–15. doi:10.1016/S0018-506X(02)00024-7
- Milczarek, M., Schneider, E., & González, E. R. (2009). European Risk observatory report. OSH in figures: stress at work – facts and figures. [cited 19 May 2017]. Available from: https://osha.europa.eu/en/publications/reports/TE-81-08-478-EN-C_OSH_in_figures_stress_at_work
- Nabi, H., Kivimäki, M., Batty, G. D., Shipley, M. J., Britton, A., Brunner, E. J.,… Singh-Manoux A. (2013). Increased risk of coronary heart disease among individuals reporting adverse impact of stress on their health: The Whitehall II prospective cohort study. European Heart Journal, 34, 2697–2705. doi:10.1093/eurheartj/eht216
- Olpe, H. R., & Seifritz, E. 2014. Bis er uns umbringt? Wie Stress die Gesundheit attackiert – und wie wir uns schützen können[Until he kills us? How stress attacks the health - and how we can protect ourselves]. Bern, Switzerland: Verlag Hans Huber.
- Olsson, E. M., von Schéele, B., & Panossian, A. G. (2009). A randomised, double-blind, placebo-controlled, parallel-group study of the standardised extract SHR-5 of the roots of Rhodiola rosea in the treatment of subjects with stress-related fatigue. Planta Medica, 75, 105–112. doi:10.1055/s-0028-1088346
- Panossian, A. G. (2013). Adaptogens in mental and behavioral disorders. The Psychiatric Clinics of North America, 36, 49–64. doi:10.1016/j.psc.2012.12.005
- Panossian, A., Hambardzumyan, M., Hovhanissyan, A., & Wikman, G. (2007). The adaptogens Rhodiola and Schizandra modify the response to immobilization stress in rabbits by suppressing the increase of phosphorylated stress-activated protein kinase, nitric oxide and cortisol. Drug Target Insights, 2, 39–54.
- Panossian, A., & Wikman, G. (2009). Evidence-based efficacy of adaptogens in fatigue, and molecular mechanisms related to their stress-protective activity. Current Clinical Pharmacology, 4, 198–219. doi:10.2174/157488409789375311
- Schoutens, A. M., Frings-Dresen, M. H., & Sluiter, J. K. (2016). Design of a randomized controlled trial on the effect on return to work with coaching plus light therapy and pulsed electromagnetic field therapy for workers with work-related chronic stress. BMC Public Health, 16, 597. doi:10.1186/s12889-016-3276-6
- Tawakol, A., Ishai, A., Takx, R. A., Figueroa, A. L., Ali, A., Kaiser, Y., … Pitman R. K. (2017). Relation between resting amygdalar activity and cardiovascular events: A longitudinal and cohort study. Lancet, 389, 834–845. doi:10.1016/S0140-6736(16)31714-7
- Techniker Krankenkasse. (2016). Entspann dich, Deutschland - TK-Stressstudie 2016 [Relax, Germany - TK Stress Study 2016]. [cited 19 May 2017]. Available from: https://www.tk.de/centaurus/servlet/contentblob/921466/Datei/177594/TK-Stressstudie%202016% 20Pdf%20barrierefrei.pdf
- Wang, X., Wu, H., Lakdawala, V. S., Hu, F., Hanson, N. D., & Miller, A. H. (2005). Inhibition of Jun N-terminal kinase (JNK) enhances glucocorticoid receptor-mediated function in mouse hippocampal HT22 cells. Neuropsychopharmacology, 30, 242–249. doi:10.1038/sj.npp.1300606
- Zhang, X., Du, Q., Liu, C., Yang, Y., Wang, J., Duan, S., & Duan, J. (2016). Rhodioloside ameliorates depressive behavior via up-regulation of monoaminergic system activity and anti-inflammatory effect in olfactory bulbectomized rats. International Immunopharmacology, 36, 300–304. doi:10.1016/j.intimp.2016.05.008
- Zhang, X., Wu, X. Q., Lu, S., Guo, Y. L., & Ma, X. (2006). Deficit of mitochondria-derived ATP during oxidative stress impairs mouse MII oocyte spindles. Cell Research, 16, 841–850. doi:10.1038/sj.cr.7310095
- Zubin, J., & Spring, B. (1977). Vulnerability-a new view of schizophrenia. Journal of Abnormal Psychology, 86, 103–126. doi:10.1037/0021-843X.86.2.103