Abstract
Objective. The aim of this study is to investigate changes in sexual activity and the prevalence of erectile dysfunction (ED) in Thai males. In addition, the treatment-seeking behaviour of Thai patients suffering from ED is also investigated.
Materials and methods. In a cross sectional study using a standardized questionnaire with a multi-stage stratified random sampling, 2,269 men aged 40–70 were interviewed. The questionnaire was designed to investigate the effects of socioeconomic factors, medical conditions and unhealthy lifestyles on the development of ED. Furthermore, the questionnaire was designed to characterize the treatment-seeking behaviour of Thai patients suffering from ED.
Results. Compared to the first report dated the year 2000, the prevalence of ED has increased from 37.5% to 42.18%. In terms of socioeconomic factors, the highest prevalence of ED was observed among unemployed men (78.51%). Prostatism and/or prostatitis (Odd ratios (OR) = 2.02) and long histories of smoking (more than 30 years, OR = 2.36) were identified as statistically significant risk factors for ED, with p-values of <0.001. It is important to notice that 38.78% of the ED patients wanted to discuss their problem with spouses or partners. Three quarters of the ED patients (74.54%) preferred oral medication as therapy.
Conclusions. The epidemiology of ED in Thailand is changing. An increased prevalence of ED does require further epidemiological studies on a regular basis in order to better understand the etiology of ED and look for measures (such as education) to counter the disease.
Introduction
Erectile dysfunction (ED) has become a global health concern because it affects nearly 50% of men older than 40 years of age Citation[1-3]. Thus, a large number of epidemiological studies investigating men's sexual activity, the prevalence of ED and ED patients' treatment-seeking behaviour has been conducted in past years. Results of these studies as well as study designs have been a controversial topic for discussion within the global academic community Citation[1]. In the meantime, the Massachusetts Males Aging Study (MMAS) Citation[4] was the first longitudinal, community-based, randomized, wide-scale epidemiological study in ED and its study design is one of the standard designs used in epidemiological studies on ED.
Despite the large scale of epidemiological studies throughout the world, data on sexual activity and ED in Thai males derive from only two epidemiological studies. The first one is a Thailand-specific study published in 2000 Citation[5], and the second is an Asian study that recruited 250 men from Thailand Citation[6].
A similar prevalence of ED was reported in both studies. However, regional differences within Thailand were observed. The current study was conducted in a larger number of Thai males in order to better capture regional differences regarding ED in Thailand. The same design as the first Thailand specific study was used to reflect changes in the epidemiology over time.
Materials and methods
This study was conducted in 2,269 Thai males, aged 40–70, who reside in urban and municipal areas. The study was a cross-sectional survey and based on a multi-stage stratified random sampling Citation[5]. It covered the Bangkok metropolitan area and four other regions; the central, the north, the northeast and the south of Thailand. The study was carried out in personal face-to-face interviews. lists demographics and social and economic characteristics of the current study population compared to the population in the previous study conducted seven years ago.
Table I. Demographic, social and economic characteristics of the study population
The effects of socioeconomic factors, medical conditions and unhealthy behaviour on the development of ED as well as counselling behaviours of ED patients were analysed by using an adjusted version of the questionnaire used in the “Cross-National Epidemiological Study of the Risk Factors, Prevalence and Health Behaviours Associated with MED”. The interviewers were trained before going into the field, and the supervisors were also on site to assist in clarifying questions.
Degrees of ED were defined in accordance with the MMAS group using a scale from one to four of experiences during the past six months. The patients were then categorized as normal, mild ED, moderate ED or severe ED into groups A, B, C and D respectively. Body mass index (BMI) was rated as follows: underweight (<18.5 kg/m2), normal (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obese (≥30 kg/m2). Data were analysed using the Statistical Package of Social Science software program. Patients' characteristics according to ED severity were compared using χ2 test and odd ratios (OR). Statistically significant differences were considered when the p-value was <0.05.
Results
Medical history
The majority of the study population (63.29%) has a history of smoking. At the time of conducting the study, 35.08%, 28.21% and 36.71% of the study population were current smokers, ex-smokers and non-smokers respectively. The mean duration of smoking was 25 years with an average of 14 cigarettes a day.
Of the 2,269 patients, 54 (2.38%) were underweight; 1,301 (57.34%) normal weight; 813 (35.83%) overweight; 101 (4.45%) were obese. In 25.17% of the interviewed men at least one comorbidity was present. The incidence of observed comorbidities including diabetes, hypertension, heart disease, prostatism/prostatitis and peptic ulcer, was 9.43%, 19.39%, 6.08%, 21.07% and 25.17%, respectively.
Sexual activity
The most common frequency of sexual activity among all males aged 40–70 years was one to three times per month (34.7%). Males aged 50–59 and 60–70 rated 37.68% and 60.4%, respectively. By contrast, the most common frequency of sexual intercourse among males aged 40–49 was four to six times per month (34.63%).
The most frequent rate of sexual activity for those whose highest academic achievement was primary or secondary school level was one to three times per month (46.54% and 36.69% respectively). This compares with a majority rate of four to six times per month among those at vocational and university level (35.88% and 37.11%, respectively).
Prevalence of ED
The estimation of the overall prevalence of ED is 42.18%. The proportions consist of 17.5%, 13.13% and 11.55% of males with mild, moderate and severe dysfunction, respectively. presents degrees of ED among Thai males aged 40–70 years by age and socioeconomic factors. The prevalence rates of ED are 23.39% in those 40–49 years of age, 47.79% in those 50–59 years of age, and 76.95% in those 60–70 years of age. This finding indicates that the problem of ED among Thai males increases rapidly with age.
Table II. Degree of ED among Thai males aged 40–70 years by age and socioeconomic factor
The effects of socioeconomic factors on ED
Unmarried men (57.38%) have a higher prevalence of ED than those who are married (38.72%), especially in severe ED cases (25.47% versus 8.38%, respectively). The degree of ED varies with education, occupation and income (). The percentages of prevalence of ED in those achieving academic levels of primary, secondary, vocational and university level are 60.29%, 42.93%, 38.91% and 30.37%, respectively. Unemployed men have the highest prevalence of ED (78.51%); followed by agricultural workers/fisherman (58.62%), managerial workers (45.14%), clerical workers (39.18%), sales workers/merchants (39.18%), service workers (37.77%), policemen/soldiers (35.26%), transportation/communication workers (34.62%), manufacturing/construction workers (33.91%) and professional or technical workers (31.14%). Those with low levels of personal income have the highest prevalence of ED (51.77%) in all the degrees of ED. Considering the association with aging and socioeconomic factors on ED, the highest rate of ED occurs among non-employed men.
Medical conditions and their effects on ED
Our study demonstrates that underweight and obese men (53.70%, and 42.56%, respectively) had a higher prevalence rate of ED than those rated normal weight (42.28%) and overweight (41.20%). However, body mass indices were not identified as statistically significant risk factors for ED (p‐value = 0.024). Interestingly, the underweight and obese groups have the highest prevalence of ED in Grade D (severe) and Grade B (mild), respectively. The distribution of ED severity according to smoking status, BMI, and alcohol consumption is summarized in . Furthermore, major chronic diseases such as diabetes (the prevalence of ED = 70.09%, OR = 3.6), hypertension (the prevalence of ED = 57.56%, OR = 2.18), heart disease (the prevalence of ED = 71.74%, OR = 3.79) and prostatism/prostatitis (the prevalence of ED = 55.86%, OR = 2.02) are significantly associated with an increased prevalence of ED (p-value < 0.001, ). However, there was no significant difference in the prevalence of ED between those who have peptic ulcers (46.58%) and those who do not (40.69%), (OR = 1.26, p > 0.2). In addition, males who have experienced trauma and injuries in the spinal cord and pelvic region got ED than those who do not.
Figure 1. Distribution of erectile dysfunction severity in 2,269 Thai males by smoking status, body mass index, and alcohol consumption.
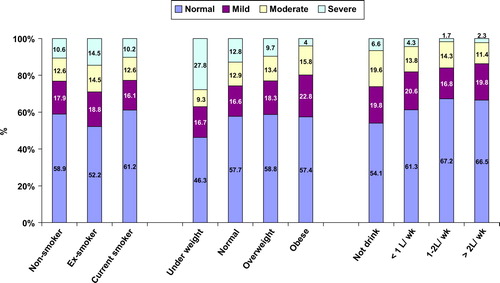
Table III. Degree of ED among Thai males age 40–70 years by major chronic illness
Unhealthy behaviours and their impacts on ED
Regarding the impact of smoking on ED, we found that there is a statistically significant relationship between the duration of smoking and ED among current and former smokers (p-value < 0.001), especially those who have smoked cigarettes for more than 30 years (57.76%, OR = 2.36, ). Severe ED occurs in 7.33% of participants who have smoked for 1–5 years and the percentage increases to 20.69 in participants with more than 30 years of smoking. Alcohol and caffeine consumption have an impact on ED. Male participants who exercise regularly have a lower prevalence of ED (41.83%) than those who do not (43.18%), especially in severe ED (10.58% versus 14.33%). However, exercise has no statistically significant impact on ED (OR = 0.94, p = 0.087).
Table IV. Degree of ED among males aged 40–70 years by smoking status, number of cigarettes/days and duration of smoking
Sexual activity in association with erectile dysfunction
The most common pattern of sexual activity of the group without ED is four to six times a month (37.33%). The ED group has substantially decreased sexual activity. The largest percentage of sexual activity in the mild, moderate and severe ED groups is one to three times per month (54.67%, 85.29% and 92.31%, respectively). Unsurprisingly, the percentage of sexual abstinence within the last six years among males aged 40–49, 50–59 and 60–70 years is 13.46%, 23.74%, and 34.07%, respectively. However, the reasons for sexual abstinence in the metropolitan area during the past six months are: lack of desire for sexual activity (40.97%), lack of partner desire (16.6%), no partner (13.1%), bad health (7.3%), erectile dysfunction (4.96%), and fear of failure (3.38%).
Counseling and seeking care for ED
The various responses given regarding the problem of ED among participants are 1) discuss with partners or spouses (38.78%), 2) keep it to themselves (32.00%), 3) discuss with friends (21.15%), 4) consult urologist (17.06%), 5) consult general practitioners (13.53%). Nevertheless, most of the respondents felt ‘neither comfortable nor uncomfortable’ (36.18%), or ‘comfortable’ (25.56%) to discuss the problem of ED with physicians. In addition, the percentages of respondents feeling ‘somewhat uncomfortable’, ‘very uncomfortable’, and ‘somewhat comfortable’ were 14.81%, 13.75% and 9.7%, respectively.
As a therapeutic option 76.55% of the ED patients use exercise as their first choice of treating ED, 17.8% take medication and 9.56% take tonics or other stimulating substances. Oral medication is the preferred choice of treatment in 74.54% of ED patients.
Discussion
The percentage of ED found in Thai men, assessed using the same questionnaire, increased from 37.5% in the first Thai report in 2000 Citation[5] to 42.18% in this study. Therefore, the estimated projection of our current data suggests that approximately 3.58 million people (0.4128 × 8.5 million men) are affected by ED. A European observational study on ED showed that 52.9% of patients experienced ED symptoms ranging from one to five years and 42.5% had severe ED based on IIEF-EF scores Citation[7]. However, ED is a major health problem for 40% of men over 40, and one that will likely worsen with time. Citation[8-10] Although a limitation of this research is the problem of studying different cohorts at different times, a comparison of data between the first study in 2000 and this study showed different results in many categories Citation[5] (). As the response rate cannot be provided the sample representative of Thai male population remains an issue. In the previous study most people took no action, while the participants in this study preferred to discuss their ED problem with partners or spouses. The method of ‘discussing the problem with partners’ is shared by Nicolosi et al.'s study as the most sought-after way of dealing with ED problems in southeast Asian countries Citation[6].
Moreover, a statistically significant correlation between ED and prostatism/prostatitis found in this study is substantiated by results from the Cologne Male Survey Citation[11].
Data from surprisingly gives a connotation that alcohol consumption could render a positive effect on ED. The possible explanations are that first, the current data provide only status of drinking while risk factors were not taken into account. Second, the amount of drink doesn't reflect the actual amount consumed, and third, excessive alcohol consumers were not included in the study.
Healthcare for ED shifted Citation[9] to pharmacotherapy with oral medication chosen as a preferred formulation in this study. Therefore, studies further observing the development of ED prevalence are deemed necessary Citation[2]. In addition, health economic data should be obtained in order to estimate costs associated with the therapy of ED.
Conclusion
This study demonstrates an increasing prevalence of ED among Thai men. This prevalence varies among men with different socioeconomic status, medical conditions and unhealthy behaviours. Our data shows that the most afflicted groups are the unemployed and smokers with more than 30 years of smoking. With scant data on ED available, more epidemiological studies on ED in the Thai population are necessary.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Nehra A, Kulaksizoglu H. Global perspectives and controversies in the epidemiology of male erectile dysfunction. Current Opin Urol 2002; 12(6)493–496
- Chew K K, Earle C M, Stuckey B G, Jamrozik K, Keogh E J. Erectile dysfunction in general medicine practice: prevalence and clinical correlates. Int J Impotence Res 2000; 12(1)41–45
- El-sakka A I. Characteristics of erectile dysfunction in Saudi patients. Int J Impotence Res 2004; 16(1)13–20
- Feldman H A, Goldstein I, Hatzichristou D G, Krane R J, McKinlay J B. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urology 1994; 151(1)54–61
- Kongkanand A. Prevalence of erectile dysfunction in Thailand. Thai Erectile Dysfunction Epidemiological Study Group. Int J Andrology 2000; 23(Suppl.2)77–80
- Nicolosi A, Glasser D B, Kim S C, Marumo K, Laumann E O. Sexual behaviour and dysfunction and help-seeking patterns in adults aged 40–80 years in the urban population of Asian countries. BJU Int 2005; 95(4)609–614
- Haro J M, Beardsworth A, Casariego J, Gavart S, Hatzichristou D, Martin-Morales A, et al. Treatment-seeking behavior of erectile dysfunction patients in Europe: results of the Erectile Dysfunction Observational Study. J Sexual Medicine 2006; 3(3)530–540
- Prins J, Blanker M H, Bohnen A M, Thomas S, Bosch J L. Prevalence of erectile dysfunction: a systematic review of population-based studies. Int J Impotence Research 2002; 14(6)422–432
- Wessells H, Joyce G F, Wise M, Wilt T J. Erectile dysfunction. J Urology 2007; 177(5)1675–1681
- de Boer B J, Bots M L, Lycklama a Nijeholt A A, Moors J P, Pieters H M, Verheij T J. Erectile dysfunction in primary care: prevalence and patient characteristics. The ENIGMA study. Int J Impotence Res 2004; 16(4)358–364
- Braun M, Wassmer G, Klotz T, Reifenrath B, Mathers M, Engelmann U. Epidemiology of erectile dysfunction: results of the ‘Cologne Male Survey’. Int J Impotence Res 2000; 12(6)305–311