
In contrast to the recent and much needed attention to the social position and health status of women, health concerns for men have been relatively neglected. The gender perspective on the health of men, including ageing men, builds on experience from the women’s health movement.
This suggests that many of the important causes of ill-health in older men are bound up in complex ways with genetic, social, economic, cultural and psychological processes.
This perspective recognizes that the health of men cannot be separated from the socially constructed roles that men fulfil. In turn, these roles are strongly influenced by culturally dominant views on masculinity. Building on the foundations of the Vienna International Plan of Action on Ageing (IPAA 1982) and the UN Principles for Older Persons, and recognizing the projections for population ageing prepared by the World Health Organization’s Ageing and Health Programme, the International Society for the Study of the Ageing Male was formed in June 1997. The objective of this Society is to promote research, study and education in all matters relating to the health of men from adulthood to senescence.
The Objectives of the Society are to encourage physicians and other health-care professionals to understand male illness in the context of the Ageing process as a whole, and to adopt a multi-disciplinary approach to caring for male patients. More specifically, the Society sets out to promote the concept of healthy Ageing and to become a global forum which mobilizes talent, energy and resources in order to address critical issues that will allow men to age in health and dignity.
ISSAM aims to promote the acquisition, systematization, critical evaluation and dissemination of relevant information, publishing its own journal, organizing international, regional and national congresses/meetings, preparing teaching material, and preparing recommendations/guidelines for the diagnosis and/or management of various conditions frequently encountered in the Ageing male.
The Society has therefore, sought to redress this matter by taking a number of initiatives in the field:
To support improvement of “Quality of Life”, “life style” and “healthcare” for men, through education, creation of awareness and dissemination of information, the society has its own Journal “The Ageing Male”, published by Informa.
To support advancements in quality of social services, preventive measures and universal patient access as well as in advancement of scientific and medical knowledge.
To attempt to find ways and mean to prevent or postpone disability, immobility and dependence.
To engage in and support and encourage socio-economic research to ensure human dignity and maintain social function of the elderly.
To become a global forum which mobilizes talent, energy and resources in order to address critical issues that allow men to age in health and dignity.
Dear delegates and guests of ISSAM-2016 International Congress!
Armen MuradyanOn behalf of the Ministry of Health of the Republic of Armenia let me welcome participants and guests of ISSAM-2016, Tenth International Congress of the International Society for Study of the Aging Male.
The issue of increasing effectiveness of medical and social services today is among top priorities of the Ministry of Health of the Republic of Armenia.
We are facing the challenge of decreasing the incidence of, and preventing diseases related to aging, and improve the overall quality of life. These tasks require coordination of efforts of physicians in different fields – endocrinologists, sexual health specialists, urologists, andrologists, gynecologists, diet therapists, neurologists, cardiologists, psychologists and others. As longevity grows, problems of age-related diseases become especially pressing, in Armenia and all over the world. The goal of “getting older without getting ill” and prevention of disability among senior citizens have become very significant in the national healthcare system of our country.
This is why we are especially proud that Armenia is hosting today the 10th anniversary international congress of ISSAM.
Let me wish all participants of the Congress successful and productive work!
This event is being dedicated to the 25th anniversary of independence of the Republic of Armenia.
Dear friends and colleagues!
Artur GrabskyOn behalf of the urologist community of Armenia, I am glad to welcome you to Yerevan, the city with almost 3000 years of history, the host city of 10th Anniversary International Congress of the International Society for Study of the Aging Male (ISSAM-2016).
The Armenian Urology Association is as old as ISSAM. Every year our Association hosts and supports professional forums that allow physicians from this country to hear and talk to world-renowned doctors, study cutting-edge achievements in the sphere of prevention and treatment of urological, including male anti-aging diseases; discuss the most recent trends in development of medicine in general and urology in particular.
I am happy to say that our goals in this issue match; moreover, relevant fields of both disciplines intersect on both sides, which makes studying the problem more comprehensive and full.
Early diagnostics, prevention and treatment of aging diseases are in the focus of the professional community today like never before. This is why I am very happy to welcome interdisciplinary cooperation in the sphere of male health, and we are looking forward to meeting with our colleagues – physicians, scholars and researchers.
I invite you to take an active part in ISSAM’s 10th Anniversary International Congress. I am very hopeful that the Congress will render beneficial influence on development of urology and related fields, in this country and the rest of the world.
Welcome to Yerevan!
Intestinal microbiota and human health. The role of the intestinal dysbiosis in the pathogenesis of the metabolic syndrome, obesity and diabetes associated with it
H. AbovyanE-mail: [email protected]Abstract
Nowadays, the old hypothesis about the important influence of the human intestinal microbiota (IM) on the mental and somatic health, expressed in the second half of the 19th century, received its scientific confirmation. Back then, Mechnikov predicted the discovery of the infectious agents responsible for carcinogenesis and for the development of the “sugar disease”. The results of the recent years’ long-term researches alter the traditional picture of the pathogenesis of many diseases and initiate more profound and deep investigation of the human IM. These achievements were facilitated by the development of the novel technologies of the molecular genetics, which make possible the identification of various bacterial species previously not available for cultivation and for traditional microbiological research methods. As a result, at the moment researchers have no doubt about the contribution of the microbiota into the development of many pathologies: metabolic, autoimmune, allergic, functional, oncological, cardio-vascular, etc. Essential contribution to the studies of the IM made the “Human Microbiom” project (HMP). One of the main goals of the project was the decoding of the genomes of more than 1000 bacteria from all biotopes of the human body contacting with the environment. The intestinal microbiome contains 100 times more genes than human genome. Each person has his own unique microflora [Citation1].
IM is not only a large metabolic organ, but also a largest organ of the human body. Its mass can be up to 2.5–3 kg. However, Ley and coauthors proved that factors of the diet could lead to the changes in the IM content. Moreover, the levels of bifidobacterium and faecalibacterium have correlations with the anti-age effects.
Due to widely spread metabolic syndrome and connected pathologies, like obesity and type 2 diabetes in the last decades, the role of the IM in the development of all pathogenic stages of the “20–21 century epidemic” is in the focus of the attention of the researchers. Essential difference in the IM content of the persons with under-weight and overweight allows one to suppose the importance of the role of IM in the development of obesity. Particularly, Cani and coauthors have shown that the decrease in the diversity of the gram-positive butyrate-producing anaerobic bacteria is associated with the endotoximia, chronic inflammation and development of the insulin resistance in mice. Ley and coauthors have found the changes in the ratio of the concentrations of Bacteroidetes and Firmicutes (decrease of the former and increase of the latter) in mice with obesity. The increase of the body mass in mice with obesity is connected with the additional extraction of energy by the colon microbiota from the meal polysaccharides.
Thus, there is substantial progress in the research of the IM and in the understanding of its influence on the human health, particularly in its role in the pathogenesis of obesity and diabetes type 2. Although, many questions are still open and are the subjects for further research, but applying the methods of the IM correction such as special diet, probiotics and prebiotics, aiming at normalization of the IM facilitates the reduction of insulin resistance, normalization of the glycemic background and body mass, improvement of the other indexes of the metabolic syndrome.
References
- Costello EK, Lauber CL, Hamady M, et al. Bacterial community variation in human body habitats across space and time. Science 2009;326:1694–7
Elimination of the hypertriglyceridemia and homocysteinemia in the patients with type 2 diabetes mellitus and male hypogonadism (users of the testosterone-replacement therapy and metformin slow release)
A. AmetovO. RozhdestvenskaiaL KamyninaE-mail: [email protected]Abstract
Objectives: To investigate the dynamics of the hypertriglyceridemia and the homocysteinemia in the patients with the Type 2 Diabetes Mellitus (T2DM), users of metformin slow release GlucophagLong® (MERCK SANTE s.a.s., Lyon, France), and the male hypogonadism (corrected with testosterone-replacement therapy (TRT)).
Materials and methods: In the randomized clinical study, 74 men with T2DM, visceral obesity and male hypogonadism were included. Median of Т2DM duration was 4 years, body mass index (BMI) = 31.8 kg/m2, waist circumference (W) = 102 sm. The male hypogonadism was corrected with the adequate TRT – testosterone undecanoate i.m., the mixture of testosterone esters i.m. or testosterone gel cutaneous. The interventional groups included the patients receiving TRT and Glucophage Long® (group GL(+), n = 36). The control group consists of patients receiving TRT and metformin rapid release but not Glucophage Long® (group GL(−), n = 38). The majority of the clinical and the pharmacological characteristics at the start of investigation were comparable in the interventional and the control groups. During 12 months of TRT, we studied the dynamics of the levels of glycosylated hemoglobin HbA1c, total testosterone (Tst), homocysteine (HCys), lipids (total cholesterol (CHOL), triglyceride (TG), lipoproteins high (LPHD) and low (LPLD) density) and the anthropometric characteristics. The statistical program Statistica 6.0 (StatSoft, Tulsa, OK) was used for the data processing and the statistical significance for the differences was p < 0.05.
Results: The efficiency and the safety of TRT for the patients with T2DM, metformin users, were demonstrated. Both the groups had comparably positive dynamics (GL(+) and GL(−) accordantly): −0.32 and –0.34% for HbA1c, –0.83 and –0.74 mmol/L for CHOL, –0.27 and –0.19 mmol/L for LPLD, +0.37 and +0.28 mmol/L for LPHD (p < 0.05 versus start level, p > 0.05 interventional group versus control group). There was statistical significance in the decreases of TG in GL users: –0.4 mmol/L in comparison with –0.1 mmol/L in control group, p < 0.05.
Meanwhile HCys descended from 16.4 to 9.2 and from 15.8 to 9.6 in the interventional and the control groups, respectively (p < 0.05 versus start levels). The level of TG descended from 3.29 to 2.66 and from 3.18 to 2.80 for the interventional and control groups respectively (p < 0.05 versus start level; p < 0.05 GL(+) versus (GL(−)). The Tst-status correction was accordingly associated with TRT. But the maximal improvement of the metabolic parameters in the correction Tst-status had been associated with using GL in the interventional group (the differences between the interventional and the control groups were –1.1 nmol/L in favor of metformin slow release, p = 0.07).
The BMI in GL(+) group changed from 32.0 to 31.2 kg/m2, W – from 106 to 102 sm (p < 0.05). PSA and volume of prostate gland were constant in all groups (p < 0.05). The pharmacological compliance was better in the interventional group because the single reception and gastrointestinal events were rare (0.8% in comparison with 6.4% at the control group).
Conclusion: The inclusion of the metformin slow release in the glucose-rescue scheme was an advantage for the more positive metabolic and HCys-lowering (antiatherogenic) effects (associated with antioxidant effect) in the patients with the T2DM in combination with the visceral obesity and the male hypogonadism if TRT takes place.
Antiaging medicine over the years in different continents
W. AuerAbstract
The term of antiaging is a difficult one, since science around this phenomenon is aiming extension and Quality Improvement of life. Since human beings exist there are myths and stories about how to get a longer life and a good quality of life.
In today’s life, we are confronted with multiple chemicals, bad habits like alcohol and cigarettes, processed food and a much higher salt and sugar intake than needed by our bodies. We tend to move less and less in our daily life.
Not only because of the mentioned, but also combining our genetic factors there is a high increase in metabolic diseases – obesity and diabetes; acne, osteopenia, rheumatological diseases, nausea, headaches, heartburn, indigestion and many other effects of acidosis.
Different countries, different cultures, different genetics, different food, need different treatments and supplements.
Central Europe, USA, China, India, Middle East, Japan, Easter Europe, Russia and Mediterranean Countries: There is a lot of differences in the genetics and in the common lifestyle.
As we know in modern science, there are genetic differences based on our heritage. The number of people with diabetes has risen from 108 million in 1980 to 622 million in 2014. In Arabian countries, there is even a higher prevalence of diabetes, Asian countries seem to have an advantage in genetic when it comes to metabolic disorders. In the United States and Europe, we tend to have higher cholesterol and glucose levels.
Basically there are three issues of modern antiaging medicine:
Anti-oxidative effects;
Hyperglycemia and weight control;
Acidosis.
Antioxydans
Supplements promoting antioxidant effects were very common over the last decades. Vitamin supplements especially containing Vit A, C, D were growing and countless studies proving the positive effects were taken. From food chemicals, alcohol, cigarettes and other toxic factors, we are surrounded with, we can see an increase of stress caused diseases. Science, research and latest medical achievements made it possible to extract single enzymes or promoters for specific treatment like superoxide dismutase, a “super-antioxidant” for the skin.
There were different substances used in different countries at different times with different success:
Omega 3 and Omega 6 – fish oil capsules;
All kinds of vitamin and mineral mixtures;
Resveratrol;
Oxygen drops;
Antarctical krill oil;
Different amino acids;
NADH (nicotinamide adenine dinucleotide);
Cholecalciferol was the sunshine star in several countries;
Melatonin.
Newest trend: to take influence on the bacterial flora in the bowel with pre-, pro- and synbiotics.
The main issue about oxidative stress is to avoid it and to protect our cells.
Weight control, diabetes and obesity
Weight control is also a very big issue. Its recommendable to maintain the do’s: Sports, fresh and high quality food, water and enough sleep and avoid the don’ts: Alcohol, processed foods, stress, high fat – especially saturated and trans fat acids as in fast foods. The worst enemy is sugar in any form.
The high caloric food, fast food and candy consumed not only in the western world supports the genetic factors and so metabolic disorders, diabetes and obesity increase all around the world. In numbers: overweight (BMI 25–29.9) and obese (BMI > 30).
Any way the main cause is hyperglycemia, a high blood glucose level. So the main goal for lowering weight is to lower our postprandial sugar levels. The best and healthiest way to regulate our body is a natural one. As in many studies detected – the plant Salacia reticulata, used since thousands of years in Ayurvedic medicine, regulates our blood levels by inhibiting alpha-glucosidase, lowering our glucose levels, hunger and weight demonstrably. Combined with Vitamin D (studies show a lack of Vitamin D in about 75% of people, especially in countries with rare sun exposure), a natural remedy was developed and perfectly adapted on today’s needs. To fight obesity and to avoid diabetes is the main goal to stay healthy even in higher ages.
Notes. The country codes refer to the ISO 3166-1 Alpha-3 country codes. Data ranking for obesity is intentionally the same as for the overweight data. BMI: body mass index. Source. WHO Global Health Observatory Data Repository. (1).
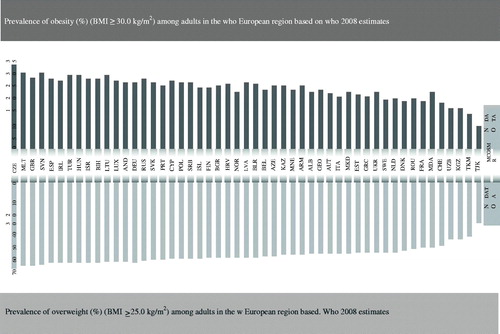
Table 1. Prostate cancer detected during medical examination in the Kemerovo region for 2011–2014.
Chronical acidosis
The acid danger – bone, skeletal and muscular problems not only osteoporosis are often treated with Vitamin D and Calcium. This is not enough. The main cause for many diseases and symptoms occurring today is chronical Acidosis – our body being flooded with acidic matters. Weak kidneys is the main cause of Acidosis in a higher age.
gastrointestinal system: too much gastric acid leads to gastritis, digestion problems, feeling, gall bladder problems;
muscle and joints: gout (uric acid!), being sore (lactic acid!), osteoporosis (a typical Acidosis Symptom) Osteoarthritis, rheumatological problems (arachidonic acid from pork);
skin, hair and teeth: alopecia, brittle nails, neurodermatitis, acne (youth and adults), cellulitis;
metabolic system: overweight, craving for high caloric/sweet food, ravenous appetite, diabetes, weight gain, elevated lactic acid;
vascular system: hypertension, strokes, early coronary calcification, nausea, headache, heart attacks;
entire organism: immunodeficiency, performance loss, anxiety, stress symptomatic, overtraining of athletes, early fatigue.
Nowadays acidosis is accepted as a cofactor in the cause of many diseases and as a result of many diseases. pH level in different body compartments is very important.
Bazenpulver is supporting our bodies to regulate the acid–alkaline-system in a natural way without side effects. For many years, we have conducted various successful studies and many doctors around the world are aware about acidosis.
The future scientists are working on permanent controlling systems for any individual person via chip and electronic recommendation.
Thank you for your attention.
Debated issues of endometriosis
A. BlbulyanAbstract
Endometriosis is one of the few pathologies that affects the fundamentals of biology. The prevailing role is played by elimination mechanisms that are represented at all levels of organization of living matter – from the molecular to the systematic. In human body, on a daily basis the so-called ectopic pathology and in hierarchy of a living organism, any ectopia is doomed to elimination, otherwise the degree of randomness of the system shall increase tragically. Ideally the elimination is to be complete. Sadly, more often it is partial, and sometimes perverse. Endometriosis, as a pathological persistent ectopia, along with the biological consequences, dramatically degrades the quality of a woman’s life. Several false “reciprocal” relationships of endometriosis (e.g. infertility) need to be revised. A therapy that is far from ideal so far should be maximally pathogenetic.
Clinical examination of the male population in the primary detection of prostate cancer for example a regional health
G. BoyadzhanA. KostinAbstract
Introduction: In recent years, prostate cancer (PC) has acquired the status of not only medical but also, to a large extent, socially relevant and depending on age problems. Primarily this is due to the increase in the incidence of PC in most age groups almost all over the world, and also by the lack of early and specific clinical symptoms. PC is characterized by a fairly long asymptomatic, calculated a few years, while the share of localized forms of PC accounted for about 31.5% of all newly diagnosed cases. In contrast, locally advanced and/or generalized forms of PC diagnosed in 68.5% of patients. The results of the autopsies established that approximately 1/3 of men older than 50 years and about 2/3 of men older than 70 years had asymptomatic PC. This allows us to predict a doubling of the number of newly registered cases of PC already by 2030.
Technique: In the present work, the objective was to evaluate the results of the clinical examination of patients in the Kemerovo region (KR). In accordance, the program includes actively identified patients as a result of the clinical examination for PC, on the basis of statistical data common information space of health for 2011–2014 according to the PSA-test results and examination of the doctor – urologist.
Results: Conducting KR clinical examination for the detection of PC can be divided into three phases: before the execution of the program of clinical examination (2011–2012), the beginning of execution (2013) and summing up the first results of the implementation (2014) of the Order of Ministry of health of the Russian Federation on carrying out of prophylactic medical examination of certain groups of adult population. In the structure of malignant neoplasms of PC with a frequency of 18.1 per 100 thousand population (5.2%), the prevalence in KR is in 7th place. Already in the early stages of execution (2013) and in summing up the preliminary results of implementation (2014) of the program of prophylactic medical examination of certain groups of the adult population, KR significantly increased active case finding of PC (Table 1).
In comparison with the rate of detection of PC in 2011 adopted during the initial, active detection of PC in 2014 increased almost 2.5 times from 51 to 124 cases. During the period 2011–2012, the diagnosis of PC was established more frequently, but diagnosis was conducted, mainly on the uptake. Thus, provided the examination was conducted in men over 50 years (test for prostatic specific antigen (PSA) and inspection urologist) allows to make a preliminary conclusion about enough high effectiveness of active detection of PC.
Along with such undeniable benefits of conducting clinical examination to identify patients with PC it is a need to consider to predict possible problems and side effects. It is obvious that clinical examination has led to the increasing load on doctors – urologists, doctors of ultrasonic diagnostics and laboratory service by increasing the number of performed blood PSA-tests available at the regional level, the acute shortage of medical staff.
Conclusion: Thus, at the additional stage of prophylactic medical examination of certain groups of adult population at the regional level in accordance with the Order of Ministry of health of the Russian Federation of 3 December 2012 №1006н, differentiated approach is necessary for the reasonable purpose of certain types of laboratory and imaging tests. Along with this, you need a clear idea of what it undoubtedly will be accompanied by additional demands on laboratory services and requires additional staffing, financial and resource support.
Testosterone resistance: a game changer in the diagnosis and treatment of testosterone deficiency and related disorders
M. CarruthersE-mail: [email protected]Abstract
Insulin resistance in type 2 diabetes is a long-established fact and a target for therapeutic intervention. We present the case for there being similar resistance to testosterone causing a relative deficiency in the majority of cases of clinical onset of symptoms of deficiency of this hormone in the adult or comorbid conditions, especially metabolic syndrome.
There are many parallels between resistance to the two hormones. This is seen in etiology, age of onset, genetics, ethnicity, heredity, familial influences, association with obesity, links with viral diseases, and autoimmune conditions. Like diabetes, androgen deficiency can arise before birth, in early life, resulting in early on-set, or later on leading to adult onset, with resistance playing a greater role. Similarly treatments such as weight loss and exercise have the effect of reducing resistance to both hormones.
Since so many of the actions of testosterone ameliorate many facets of the metabolic syndrome, it is suggested that peripheral vascular disease in diabetic men is a primary target for intervention. A double-blind placebo controlled trial of testosterone undecanoate injections in men with incipient gangrene is proposed and should rapidly translate this theory into practice.
Influence of level of estrogens at women (scent of a woman) on sexual function at men
A. FominE-mail: [email protected]Abstract
The role of sex hormones (Testosterone, Estrogens, Progesterone) in both men and women in the regulation of reproductive function, and maintaining homeostasis cannot be overestimated.
Cyclic changes of secretion of sex hormones in women are well studied and practical application in obstetrics, gynecology and in other medical specialties (cardiology, neurology, dietology, cosmetology, etc.) are found.
Today value of sex hormones, first of all Testosterone, for the man’s organism is also studied. Testosterone influences on sexual function (libido, erection, spermatogenesis), metabolism of carbohydrates, cardiovascular system, psychoemotional sphere, etc.
However today the attention is practically not paid to mutual influence of physiology of men and women. What occurs with age? The influence of cyclic fluctuations and decrease of sex hormones in women on sexual function in men is better known from popular literature, than from medical one.
We do not know whether decrease of sexual desire in men is always linked to psychoemotional disturbances, androgenic deficiency and somatic pathology. Is it possible to affect sexual activity of a man while improving hormonal disturbances in a woman?
We surveyed 50 married couples which, the leading complaint had a depression of a sex inclination at the men. In 50% of couples, testosterone deficiency neither clinically (bioimpedance), nor in laboratory was taped in men (LG, Testosterone, Sex Hormone Binding Globulin). In these couples, deficiency of estrogens was diagnosed for women as clinically (dryness mucous, a condition of a skin, psychoemotional disturbances), and also on disturbance of pH in a vagina (the test for definition of vulval acidity, is normal in a vagina, pH 4.0–4.4).
Depending on degree of expression of deficiency of estrogens, therapy was carried out by drugs: Trioginal, Ovestin®, Oestrogel, Femoston®). At compensation of deficiency of estrogens, normalization pH in vagina became perceptible (pH 4.0–4.4). We noted appreciable intensifying of a sex inclination at partners (on the basis of a poll). Besides, the augmentation of sexual desire in most of the women is noted.
Well-timed diagnostics of deficiency of estrogens at women and adequate therapy allow to carry out not only prophylaxis of such complications as an atherosclerosis and an osteoporosis, but also to keep sex harmony in married couple.
Psychosomatic feature of androgen deficiency in men
A. HakobyanE-mail: [email protected]Abstract
Background: Testosterone deficiency in males could be due to impairment in testis as well as in hypothalamus pituitary gland system, it is not uncommon to meet this problem in a long-term stressful situation where strong negative psycho-emotional influences permanently exist. Thus, we put our attention into the diabetes mellitus as a disease where both physical and psychological discomforts persist.
Aim: The current research is to make correlations between T-deficiency in primary cases of hypogonadism and T-deficiency in hypogonadal male with chronic illness such as diabetes mellitus and consequences of these both conditions on sexual wellbeing.
Method: We investigated 86 people aged from 17 to 54 with erectile dysfunction and premature ejaculation. Among these patients 12 had primary hypogonadism, the rest of them – 73 people had diabetes mellitus. The levels of LH, FSH, Prolactin and T were measured by radioimmunologic methodology. At the same time, the sperm evaluation was conducted. Sexual function was assessed by clinical observation and detailed interview.
Results: In both groups, we have observed sexual dysfunctions particularly ED, Ejaculatory problems. In cases of primary hypogonadism, sexual dysfunctions are strongly associated with hormonal deficiency (p < 0.005). In cases of diabetes mellitus, this association is not significant (p > 0.005), therefore hormonal disturbances here play only contributory role.
Conclusion: In group of primary hypogonadism with sexual dysfunctions, the role of T therapy is strongly recommended, in cases of diabetes with sexual dysfunctions, the T therapy should be as additional modality of treatment along with basic therapeutic requirements.
References
- Wu FC, Tajar A, Beynon JM, et al. Identification of late-onset hypogonadism in middle-aged and elderly men. N Engl J Med 2010;363:123–35
- Kelly DM, Jones TH. Testosterone. A metabolic hormone in health and disease. J Endocrinol 2013;217:r25–45
- Shabsigh R, Perelman MA, Lockhart DC, et al. Health issues of men: prevalence and correlates of erectile dysfunction. J Urol 2005;174:662–7
- Kupelian V, Shabsigh R, Araujo AB, et al. Erectile dysfunction as a predictor of the metabolic syndrome in aging men: results from the Massachusetts male aging study. J Urol 2006;176:222–6
Reproductive medicine and human evolution
E. HambartsoumianE-mail: [email protected]Abstract
In our presentation, we will explore the implications of sexual revolution, medical science and assisted reproduction from the perspective of human evolution. How do the selection criteria of our society combined with the progress of reproductive medicine and biotechnologies differ from the natural selection process, and to what extent will assisted reproduction affect (and already affecting) the human evolution?
Saving lives: prescription of testosterone and PDE5 inhibitors
A. HealdE-mail: [email protected]Abstract
Objective: Experimental evidence has shown potential cardioprotective actions of phosphodiesterase type-5 inhibitors (PDE5is). We investigated whether phosphodiesterase type-5 inhibitor (PDE5i) use in patients with type 2 diabetes, with high attendant cardiovascular risk, was associated with altered mortality in a retrospective cohort study.
Research design and methods: Between January 2007 and May 2015, 5956 men aged 40–89 years diagnosed with type 2 diabetes before 2007 were identified from anonymized electronic health records of 42 GP practices in Cheshire, UK and followed for 6–9 years. Hazard ratios (HR) from multivariable survival (accelerated failure time, Weibull) models were used to describe the association between on-demand PDE5i use and all-cause mortality.
Results: Compared to non-users, men prescribed a PDE5i (n = 1359) experienced lower percentage of deaths during follow-up (19.1% versus 23.8%), and lower risk of all-cause mortality [unadjusted hazard ratio (HR) = 0.69 (95% confidence interval: 0.64, 0.79); p < 0.001)]. The reduction in risk of mortality (HR = 0.54 (0.36–0.80); p = 0.002) remained after adjusting for age, eGFR, smoking status, prior CVA, hypertension, prior MI, systolic blood pressure, use of statin, metformin, aspirin and beta-blocker medication. PDE5i users had lower rates of incident MI (incidence rate ratio (0.62 (0.49–0.80), p < 0.0001) with lower mortality (25.7% versus 40.1% deaths; age-adjusted HR = 0.60 (0.54–0.69); p = 0.001) compared to non-users within this sub-group.
Conclusion: In a population of men with type 2 diabetes, use of PDE5is was associated with lower risk of overall mortality and mortality in those with a history of AMI.
Progesterone deficiency in men and women: need to change perceptions
S. Yu KalinchenkoI. A TyuzikovE. A. GrekovM. I ZhilenkoE-mail: [email protected]; [email protected]; [email protected]Abstract
Today the modern medicine is in deep crisis, characterized by a complete inability not only to stop the pandemic of obesity and type 2 diabetes, depression, hypertension, erectile dysfunction, whose treatment drugs symptomatic treatment is accompanied by increased metabolic acidosis, but also the steady growth of iatrogenic complications of pharmacotherapy.
Albert Einstein said: the significant problems we face cannot be solved at the same level of thinking we were at when we created them. Regarding obesity and type 2 diabetes: we cannot achieve success by continuing to treat type 2 diabetes as a “sugar problem” and continuing to try to find a solution with the help of “glucose-lowering” drugs, and obesity – overeating problem by continuing to develop an inefficient dietetics.
The problem of obesity, type 2 diabetes, osteoporosis, sarcopenia, osteoarthritis, depression and other age-related diseases must be addressed comprehensively from the viewpoint of hormone replacement therapy and insulin resistance and oxidative stress, underlying these diseases.
After 45 y.o. (mean age WHO), secretion of major of fat burning hormones, such as vitamin D (D-hormone) and sex hormone (testosterone, estrogens and progesterone) have decreased for all healthy people, which leads to the appearance of insulin resistance and oxidative stress and steady progression.
Diagnosis of insulin resistance is quite simple – the measurement of waist circumference and neck circumference, as well as of bioimpedance.
Insulin resistance and oxidative stress are always secondary and occur in response to age-related decline of hormones.
In recent years, understanding of testosterone and estrogen has changed, which is no longer divided into male and female sex hormones, and is considered as a universal sex hormones in the body of both sexes. As for progesterone, that it is still defined as the pregnancy hormone.
Progesterone is an important hormone that is present in women and men. Progesterone in men and women is synthesized in the adrenal cortex and gonads, participating in a wide range of physiological and biochemical reactions. High or low progesterone adversely affects the functioning of many physiological and biological processes.
Progesterone is a precursor of a number of the most important hormones of the body, including the sexual. As the progesterone produced by the most important steroids, testosterone and cortisol, directly affect the operation of the entire central nervous system.
Conducting surveys on hormone, comprising, including and determining progesterone is absolutely necessary in all patients after 40 years at any somatic pathology. Need to revision of the standard indicators of progesterone is necessary, as in most laboratories the lower boundary of progesterone norm is zero value!
Deficiency of vitamin D – golden key reproductive health and career longevity: formula 80/120: definition of health and happiness
S. Yu. KalinchenkoE-mail: [email protected]Abstract
Our traditional notion of vitamin D is associated primarily with its important role in calcium and phosphorus homeostasis and the effect on bone mineral density [Citation1].
However, unlike all other vitamins, it is not a classic vitamin because:
first, truely not involved like vitamins as a co-enzyme in any biochemical process;
second, biologically active, and only by a two-stage metabolism in the body it is converted to the active form of the hormone;
third, in the body thereto specialized receptors are expressed, which has none of the known vitamins.
Thus, vitamin D is a potent steroid hormone with a unique spectrum of “non-classical” systemic metabolic effects, which regulates about 3% of the human genome (several tens of thousands of genes), and above all the genes involved in glucose metabolism and steroidogenesis (synthesis of sex hormones).
With current data of vitamin (hormone) D endocrinology, the question arises: is there a connection of its metabolism disorders and infertility, and early menopause, and andropause, which lead to both physical and cognitive ill health and, consequently, reduce the age of professional activity?
In more than 5000 patients in our clinic, we have found that vitamin (hormone) D deficiency, leading to a deficiency of sex hormones, promotes the disruption of relations between lipogenic (prolactin, insulin, cortisol) and lipolytic (growth hormone, catecholamines, thyroid hormones) factors that leads to obesity, which in turn reduces the blood level of circulating 25 (OH) D-vitamin capture due to the increased adipose tissue, which forms a kind of “vicious circle of pathogenesis” characteristic for obesity and diabetes 2 type. At the same time, patients with obesity often avoid sunlight, which is necessary for the synthesis of vitamin D in the skin, as suffering physical illness (especially cardiovascular), not allowing them to stay for a long time in direct sunlight.
Low levels of vitamin (hormone) D must to considered as an independent predictor of initiation and progression of obesity, insulin resistance, and also oxidative stress and depression, as the synthesis of hormones, including serotonin and melatonin, it depends on the level of vitamin D.
Reference
- Schwartz GY. Vitamin D and D-hormone. Moscow: M. Anacharsis; 2005. 152 p. (in Russian)
The link between testis and bone
Z. KamenovE-mail: [email protected]Abstract
Androgens, and in particular, testosterone is substantial for the bone health. It works directly or indirectly through aromatization to estradiol. Even if not everything is clear about the role of both hormones in development and maintenance of bone, clinical data supports the importance of gonad hormones for the prosperity of bone. Considered usually as a female disease, osteoporosis affects men too. Men have fewer fractures, but after femoral fracture, they die twice more often, compared to women.
Accepted usually as an insensible and rigid tissue, recently, the bone gradually showed that it responds to the signals in its own biological language by increasing the insulin sensitivity and secretion, influencing muscles and white adipose tissue, regulating the free fatty acids and the phosphates metabolism.
Only in the last years, it appeared that bone has regulatory functions on the testis. Binding to the G-coupled GPRC6A receptors on the Leidig cells, undecarboxylated osteocalcin is able to induce the production and secretion of testosterone via stimulation of the steroidogenic cytochromes P450scc and P450c17. With different mechanisms, bone increases the reproductive power of the testis. The pancreas–bone–testis axis regulates the testis, independently of and in parallel to the hypothalamus–pituitary–testis axis.
In conclusion, although appearing in the last decade, the bone–testis link is promising in reproductive aspect.
How to reach 90 years with quality of life-preventive strategies
B. LunenfeldE-mail: [email protected]Abstract
Despite the enormous medical progress during the past few decades, the last years of life are still accompanied by increasing ill health and disability. The ability to maintain active and independent living for as long as possible is a crucial factor for ageing in health and dignity. This hopefully should reduce the gap between health and life expectancy. The ultimate goal being “aging in health and dignity”. Therefore, the promotion of healthy ageing and the prevention of disability, must assume a central role in medical research and medical practice as well as in the formulation of national health and social policies. Effective programs promoting healthy active ageing must include components such as: preventive care (clean water, sanitation, vaccination, proper nutrition and physical exercise) early diagnosis of diseases or deficiencies, decreasing, delaying or preventing lung, breast and colon cancer, cardiovascular disease and metabolic syndrome.
Decisions must be based on an understanding of how the determinants of active ageing influence the way that individuals and population age. Such programs will ensure a more efficient use of health and social services and improve the quality of life in older persons by enabling them to remain independent and productive.
Preparing health providers and societies to meet the needs of older populations is essential: training for health professionals on old-age care; preventing and managing age-associated chronic diseases; designing sustainable policies on long-term and palliative care; and developing age-friendly services and settings. If done effectively the above measures should result in an increase in the quality of life with a delay, decrease or prevention of disabilities. This would increase length of productive life of aging populations, decrease dependency, and as a result decrease health costs related to expensive curative and palliative services. A holistic approach will necessitate a quantum leap in multidisciplinary and internationally coordinated research efforts, supported by a new partnership between industry and governments, philanthropic and international organizations. This collaboration we hope will enrich us with a better understanding of health and aging, permit us to help to improve the quality of life, prevent the preventable, and postpone and decrease the pain and suffering of the inevitable.
Declaration of Interest
No conflict of interest.
Molecular pathways of ageing
B. LunenfeldE-mail: [email protected]Abstract
Ageing and noncommunicable diseases (NCDs) have been studied as independent conditions. However, evidence suggests that chronic diseases, cancer and ageing share many molecular pathways. It is difficult to separate and to distinguish between, ageing amplifiers determined by environmental and developmental factors (which can be modified); acute or chronic illness or inter current diseases (which can be prevented, delayed or cured); risk factors due to hormone deficiency (which can be prevented); and the natural ageing process, primarily genetically determined. Whether this can be influenced or changed today is the subject of this review. A major cause of ageing is “oxidative stress.” It is the damage to DNA, mitochondria, proteins and lipids (fats) caused by oxidants, that are partly responsible for most NCDs. There is also evidence that cancer is an ageing-associated disease. Abnormal telomerase expression and telomerase mutations have been associated with many different types of degenerative diseases as well as certain tumours. With the availability of telomerase activators and inhibitors, recent studies proposed telomere based therapeutic approaches as a potential therapeutic target for age-related diseases as well as to treat cancer. Aging may become a treatable medical condition In this review, we briefly discuss the underexplored interaction between the aging process, damage to DNA, mitochondria, proteins and lipids (fats) caused by oxidants, that are partly responsible for most NCDs and cancer as an ageing-associated disease. Identifying intervening biological substrates that could serve as potential treatment targets for NCDs and cancer and resources that may protect or recover individuals from the adverse effects from exposure to chronic oxidative stress should be primary future directions in this field. Understanding the regulation of telomere dynamics and elucidating their role in disease and cancer is a top priority. The fact that while longer telomeres seem to promote healthy ageing, excessive telomerase activity promotes tumour growth, and short telomeres, while inhibiting the growth of tumors, can also promote the early steps in tumor formation, as well as organ dysfunction makes manipulating telomeres and telomerase a challenge for multidisciplinary research.
Androgen deprivation therapy in older patients affected by prostate cancer: a model of frailty
M. MaggioG. CedaG. ValentiE-mail: [email protected]Abstract
Prostate cancer is the most common cancer in men. Androgen-deprivation therapy (ADT) is often employed in the treatment of recurrent and metastatic prostate cancer. Although its use as an adjuvant therapy has resulted in improved survival in a subset of patients, ADT is also characterized by a multitude of endocrine complications including osteoporosis, sexual dysfunction, hot flashes, and gynecomastia and metabolic complications such as adverse body composition, insulin resistance, hyperglycemia and metabolic syndrome [Citation1].
In addition, weight loss, sarcopenia, muscle weakness, fatigue, and reduced activity levels are commonly observed during ADT and are also key components of the most used operationalized definitions of physical frailty [Citation2]. The close overlapping closely between the toxicities of ADT and frailty can explain why ADT can accelerate the development and progression of frailty in vulnerable older men with prostate cancer, independently of confounding effects of cancer or radiotherapy [Citation3].
Thus, the potential consequences of ADT should be considered and/or carefully monitored when initiating therapy in older patients with recurrent prostate cancer. The Frailty Lab of Parma in the context of multidisciplinary team working on prostate cancer has produced preliminary results addressing the role of comprehensive geriatric assessment [Citation4] in different domains of frailty, in selecting candidates to ADT or other aggressive treatment in older patients, to suggest intermittent versus continuous ADT for hormone-sensitive prostate cancer, and monitoring eventual effects associated with ADT.
References
- Harle L, Maggio M, Shahani S, et al. Endocrine complications of androgen-deprivation therapy in men with prostate cancer. Clin Adv Hematol Oncol 2006;4:687–96
- Bylow K, Mohile S, Stadler W, Dale W. Does androgen-deprivation therapy accelerate the development of frailty in older men with prostate cancer? A conceptual review. Cancer 2007;110:2604–13
- Cheung A, Hoermann R, Dupuis P, et al. Relationships between insulin resistance and frailty with body composition and testosterone in men undergoing androgen deprivation therapy for prostate cancer. Eur J Endocrinol 2016;175:229–37
- Della Pepa C, Cavaliere C, Rossetti S, et al. Predictive comprehensive geriatric assessment in elderly prostate cancer patients: the prospective observational scoop trial results. Anticancer Drugs 2016; in press. doi:10.1097/CAD.0000000000000428
Masks of depression in men
H. ManvelyanE-mail: [email protected]Abstract
Although considered as Strong Gender, male patients suffer of depression worse than female because of objective reasons. The stereotypes demand certain behavior, which excludes complains on decreased mood, problems with emotions and health concerns. Female patients are more open to seek help from either relatives (sisters, friends) or medical professionals, but men are hiding the problem, worsening both the condition and possible successful healing.
Comprehensive medical professional must have wider look on complicated health concerns of male patient to be able to recognize masked depression. Therefore it must be excluded in all Autonomic Failures, Panic At-tacks, Anxiety Disorders, Chronic Fatigue Syndrome, Fibromyalgia, Eating Disorderalcoholics, including alcoholics, workaholics, sexaholics, etc.; gamblers.
Only professional unveiling of depression and efficient management will provide the chance on successful treatment.
Age-related growth hormone decline: therapy perspectives and applications
N. A. MazerkinaE-mail: [email protected]Abstract
Growth hormone (GH) is secreted by the pituitary gland. GH-releasing hormone, sex steroids, low glucose blood level, ghrelin, starvation, deep sleep, vigorous exercise stimulate the secretion of GH. Somatostatin, high glucose blood level, hypercortisolism, obesity, sex steroid deficiency inhibit GH secretion. Checking a single blood sample for GH is not helpful, so Insulin Growth Factor-1 (IGF-1) is an indicator, reflecting overall GH secretion.
Growth hormone secretion decreases with age, and this decline has been termed as “somatopause”. In elderly patients, it is so significant that IGF-1 level may be as low, as those encountered in adult patients with GH deficiency. GH decrease causes decrease of lean mass, which translates to reduced bone mineral density, reduced muscle strength and exercise capacity, increased adiposity, dry and thin skin, psychological well being and cognitive impairment. These changes result in a higher overall cholesterol level in blood and impaired cardiac capacity.
Both too high and too low GH and IGF-1 levels are associated with decreased life span in humans. Acromegalic patients have increased cardiovascular death due to apnea and cardiomyopathy, but not to atherosclerosis. There is no data about increased cancer mortality in acromegalic patients.
Patients with GH-deficiency have increased cardiovascular mortality. The landmark study Rudman et al. (NEJM, Citation1990) elicited a lot of studies of GH administration in elderly. This studies demonstrated body composition and cognitive performance improvement, but some side effects, such tissue edema, carpal tunnel syndrome, gynecomastia artralgias and impaired glucose metabolism.
The safety of GH supplementation in aging individuals and possibility of increased risk for cancer with GH supplementation in elderly patients are still a matter of debate because no data exist for long-term treatments.
We have followed 32 patients aged 35–78 years with clinical signs of GH insufficiency and IGF-1 less than 130 ng/ml received GH therapy at a dose 0.2–0.5 mg/day within 3–12 months.
Patients showed bioimpedance score improvement (increase of muscle mass, decrease of fat mass), decrease cholesterol level, memory and sexual function improvement.
There were no adverse events such as tissue edema, carpal tunnel syndrome, gynecomastia artralgias and impaired glucose metabolism.
References
- Rudman D, Feller AG, Nagraj HS, et al. Effects of human growth hormone in men over 60 years old. N Engl J Med 1990;323:1–6
Testosterone treatment in women with poor ovarian response: pregnancy and live birth rates
G MskhalayaM. MalyshevaE. LubimkinaE. EltsovaV. ZaletovaC. NagaevaS. KalinchenkoE-mail: [email protected]Abstract
Objective: To assess the efficacy of pretreatment with oral form of testosterone undecanoate (TU) in poor responders undergoing in vitro fertilization (IVF).
Design: Prospective controlled trial.
Materials and methods: One hundred and twenty-eight women with poor ovarian response, defined according to ESHRE consensus/the Bologna criteria of low ovarian response were included. Patients were randomly divided into two groups: TU treatment group (77 women) or control group (51 women). For TU group, TU oral form 40 mg was given daily for at least 40 days (median – 51 days) preceding COS for IVF. Primary outcome measures were clinical pregnancy (PR) and live birth (LR) rates. Statistical research was made using a soft-ware package statistics (StatSoft Inc., Tulsa, OK, version 12). Quantitative data are presented as median and quartile range. When comparing the quantitative data of two independent groups, Mann–Whitney U test and Fisher exact two-tailed test, were used. Values were considered statistically significant if p < 0.05.
Results: There were no differences in patients’ characteristics between the two groups. There was no significant difference in starting FSH dose or total dose of gonadotropins administered between the groups. There was an increase in number of oocytes retrieved 2 [1; 3] versus 1 [1; 2] in TU group, though it was not significant (p = 0.15). The clinical pregnancy rate (per cycle) was significantly higher in TU group (24.7%) than in control group (7.8%), p = 0.018. Live birth rate was higher in TU group than in control group 18% versus 5.9%, respectively, though the difference was not statistically significant (p = 0.06).
The treatment group was divided into three subgroups according to age:
1st group – less than 35 years old (20 patients);
2nd group – 35–39 years old (26 patients);
3rd group – patients 40 years and older (31 women).
PR and LR were calculated separately to each age group:
1st group: PR – 45%, LR 100%;
2nd group: PR – 35%, LR – 55.6%;
3rd group: PR – 3.2%, LR – 0%.
Conclusions: TU pretreatment may be beneficial in women with diminished ovarian response undergoing IVF. PR and LR rate severely decreased in women 40 years and older, they may need more prolonged pretreatment with TU for better success rate.
New ultrasound marker of insulin resistance
A. G. ParshinR. T. SardinovN. S. LiberanskayaE-mail: [email protected] Sardinov Ruslan T. E-mail: [email protected] Liberanskaya Natalia S. E-mail: [email protected]Abstract
Introduction: Size increasing seminal vesicles (SV) was described for patients with diabetes mellitus type II. However we did not succeed in finding literature data about possible influence of insulin resistance (IR) on SV enlargement.
The aim of the study was to evaluate the impact of IR on increasing the transverse size of the SV above normal values and potential use of increasing SV by transrectal ultrasound (TRUS) as marker of IR.
Material and methods: Our study included 35 patients diagnosed with IR and 20 men in the control group without IR. A total of 55 patients aged from 21 to 67 years. The diagnosis of IR is set based on the combination of at least one risk factor and two symptoms AACE (American Association of Сlinical Еndocrinologists).
All subjects performed the determination of the concentration of glucose, triglycerides, high density lipoproteins of blood serum, blood pressure measurement and determination of the transverse size of SV using TRUS. Normal size SV in the transverse dimension by TRUS was considered to be less than 1.3 cm, inclusive. The study included only men with normal PSA values (up to 2.5 ng/ml at the age 40–49 years, to 3.5 ng/ml – at age 50–59 years, 4.5 ng/ml – at age 60–67 years).
Results: In the group with IR, 16 patients (46%) revealed an increase in the transverse size of SV above the normal values on TRUS. In 13 patients, the increase in SV was two-sides, 3 – at one side. In the control group, only one out of 20 men (5%) identified increase of transverse size SV at one side. On the basis of an increase in SV between the IR group and the control group revealed statistically significant differences by Chi-square (p = 0.001). This means that in the group of patients with IR, statistically significant more often increasing SV above the normal values were found than the control group. Increasing SV patients with IR obviously is due to their neuropathy. As a result, these pelvic organs lose their normal tone and ability to adequately contract.
Conclusion: IR can be the cause of a neuropathy and increasing SV. Enlargement of SV with at least one side exceeding 1.3 cm in transverse dimension can claim the role of ultrasound marker of IR in men.
Profile of men’s health in Volgograd region: problems and challenges
E. A. PopovaV. O. SmirnovaI. N. BarykinaA. S. SalasyukE-mail: [email protected] Viktoriya O. Smirnova, E-mail: [email protected] Irina N. Barykina, E-mail: [email protected] Alla S.Salasyuk, E-mail: [email protected]Abstract
Modern man can extend his men’s health and maintain sexual potential. The secret of the negative impact on the male body lies not so much in the age aspect, as in the improper lifestyle and unhealthy diet, they lead to premature aging of the male body and decrease in the potency.
Materials and methods: During 2014–2016 years, we have examined 227 men at the age of 20 years and more. To assess the quality of life, we used anonymous questionnaire developed by the Department of Therapy and Endocrinology. Main topics included in the questionnaire are: anthropometric and sociodemographic characteristics, behavior, sex life, drug history.
Results: The largest age groups are men between 40 and 49 years old (36.6%), the least – aged more 60 years old (8.4%). The last groups were distributed as: 20–29 years – 16.7%, 30–39 years – 18.5%, 50–59 years – 19.8% respondents, respectively. 73.1% of men are married. 52.4% of men have a weight in the range between 80 and 100 kg. 90.3% respondents do not count calories, 64.8% do not control the weight, 86% – do not control salt consumption, 85.9% – do not control water consumption. Amount of food intake: 44.5% of the respondents – two times per day, 32.1% – 2–3 times per day. 39.2% men do not have bad habits, but 42.7% smoke and 20.3% drink alcohol. Physical activity at least two times a week was noted in 24.2% respondents, three times a week and more – 58.1%, 43.6% are sedentary. Self-monitoring of blood pressure is carried out only by 15% of men. Other respondents measure BP rarely or never. Sixty-seven percent of respondents do not control the level of glucose, and 81.5% – cholesterol. The frequency of sexual intercourse: 14.5% have sex daily, 64.3% – 2–3 times a week, 15.8% – less than one time per week, and 2.2% are not sexually active. Unstable mood (aggression, depression, nervousness, irritability) bother men at 75.3% – sometimes, at 23.8% – often.
Conclusion: According to the analysis of questionnaires, men do not pay enough attention to physical activity, weight and blood pressure control. The overwhelming number of respondents note the deterioration of the quality of life, mood instability and reduced sexual activity. A systematic approach to promotion of healthy lifestyles among men is required.
The evolution of views on the issue of insulin resistance and metabolic syndrome in dermatology and esthetic cosmetology: thesis
A. ShaghbatyanE-mail: [email protected]Abstract
Along with the development of dermatocosmetology as well as our approaches to the examination and formation of treatment protocols, there have been significant changes resulting in a more extensive and comprehensive approach to some issues that may seem simple, such as the correction of localized fat deposits and weight normalization.
The goal of the present report: The goal of this report is to imagine a modern and multifaceted approach to the solution of one of the most current problems of this century such as overweight, abdominal obesity as well as imagine the evolution of the ways of treatment that we had offered to our patients previously, the methods of preventing age-related changes and the introduction of the basics of gerontology in the practice of a dermatologist.
Materials and methods: In the present report, there will be presented the most necessary and minimal set of information in the form of laboratory tests, which are necessary for the full evaluation of all the morphological and pathophysiological changes in the body of men and women who come to the clinic for the purpose of aesthetic rejuvenation, weight loss and correction of localized fat deposits.
Conclusion: There will be presented the treatment protocols of obesity, hyperpigmentation, papillomatosis, alopecia, atony and dryness of the skin which are considered to be masks for insulin resistance as well as for age-related changes in hormonal status. Beauty is first of all-health, isn’t it! Therefore, the literate prevention and treatment of the arising problems as well as the comprehensive approach to the clinical symptoms of global changes in the body – this is exactly what we call MODERN AESTHETIC MEDICINE.
The role of metabolic syndrome in the genesis of erectile dysfunction
V. ShahramanyanE-mail: [email protected]Abstract
Introduction: In recent years, the so called metabolic syndrome, which is a complex of related disorders based on insulin resistance, i.e. insulin sensitivity, carbohydrate, lipid, purine metabolism, abdominal obesity, is paid more and more attention to in literature. For males, in comparison with females, the deposition of adipose tissue is the central character. The greatest accumulation occurs in the abdomen inside, predominantly abdominally or viscerally.
Testosterone stimulates the adrenergic receptors predominated in visceral adipose tissue, while the estrogen/progesterone – mainly the adrenergic receptors of subcutaneous fat. Visceral adipose tissue has a high metabolic activity, aimed at the synthesis of triglycerides and the release of large amounts of fatty acids.
Methods: Hypogonadism, andropause (male menopause) is the state, caused by the decreased production of sex hormones or violation of their actions. The obvious relationship between the lack of function of the gonads and the development of obesity is proved.
Male congenital hypogonadism is also accompanied by obesity. However, obesity can exist without hypogonadism. Therefore, it is necessary to distinguish the hypogonadism obesity as the prime cause of obesity and hypogonadism caused by obesity.
Males have an inverse relationship between testosterone levels and body mass index (BMI), on the one hand, increasing leptin and insulin resistance on the other. They also have an inverse relationship between BMI and free testosterone. Free testosterone concentration is inversely related to the amount of visceral fat and the insulin resistance. It is proved that it was preceded by a decline in testosterone secretion and possibly contributes to visceral obesity.
Results: The correction of hypogonadism with androgens for males with obesity leads to a decrease in BMI by reducing the amount of visceral fat, a decrease in insulin resistance and reduction in diastolic blood pressure, the lipid profile improvement. Aromatase of excess adipose tissue mainly converts androgens-testosterone, and androstenedione into estrogens, which suppress secretion of gonadotropin-like releasing hormone and LH, which is manifested by the decreasing of testosterone secretion by Leydig cells, i.e. secondary hypogonadism. Low testosterone is an independent risk factor for the development of visceral obesity. Hypogonadism with obesity is an important factor in the maintenance and the progression of obesity, as testosterone deficiency greatly reduces the physical activity.
For males with abdominal obesity the testosterone level and gonadotropin-releasing hormone decrease, immune-reactive insulin level increases, the development of tolerance to carbohydrates and dyslipidemia, coronary heart disease and hypertension, and consequently the development of hypogonadism is observed.
Conclusions: In case of PDE-5 inhibitors an inefficient therapy of erectile dysfunction (ED) in metabolic syndrome is caused by the lack of androgens in the body and the existence of neuropathy. The lack of androgens may be mainly caused by the overweight, hypogonadism and andropause. Reducing the level of testosterone can be the reason of libido lose.
Treatment of the ED in combination with androgen insufficiency and obesity must begin with obesity therapy, and then switching to the scheme of therapy PDE-5 inhibitors and androgens.
Efficacy and safety of prolonged-release melatonin in patients with metabolic syndrome and insomnia
V. SmirnovaI. BarykinaA. SalasyukE-mail: [email protected] Viktoriya O. Smirnova, E-mail: [email protected] Irina N. Barykina, E-mail: [email protected] Alla S. Salasyuk, E-mail: [email protected]Abstract
Introduction: Addition of melatonin to the standard therapy of metabolic syndrome (MS) may have advantages for the correction of its various components. The aim of our study was to compare the efficacy and safety of metformin alone and its combination with metformin in correction of anthropometric, metabolic, hemodynamic parameters, adipocytokines levels and insomnia in patients with MS and circadian disorders.
Methodology: The prospective open-label randomized comparative study was conducted in patients with MS (the IDF, Citation2005), arterial hypertension and sleep disorders (less than 19 points on the self-assessment of sleep quality scale). Patients (n = 158, 53.8% men and 46.2% women, mean age – 52.6 + 5.8 years, mean body mass index – 34.1 + 4.3 kg/m2, waist circumference – 108.8 + 11.4 cm) were randomized into two groups. All patients get recommendations about correction of lifestyle (including diet changes, normalization of sleep-wake pattern and physical activity expansion). Patients of Group 1 (n = 80) received monotherapy with metformin 2000 mg per day, participants of Group 2 (n = 78) in addition to metformin received prolonged-release melatonin 2 mg per day. Treatment period was 12 weeks. Changes in anthropometric, biochemical, hemodynamic, metabolic parameters, and the improvements in quality of sleep were considered as the criteria for the effectiveness after 12 weeks of therapy.
Results: By the end of the study in patients who received the combination of metformin and melatonin, body weight decreased for 6.2% versus 5.4% in metformin alone group (p < 0.05). The amount of visceral fat decreased by 5.8% from baseline in Group 2 and by 2.4% in Group 1 (p < 0.05). Patients of Group 2 have noted a positive effect of melatonin on feeding behavior and normalization of sleep–wake pattern, and improved sleep quality. An average result of the subjective assessment of the quality of sleep was 21 points after 12 weeks of treatment, versus 16 points at baseline. There were no significant improvements of the quality of sleep in the metformin alone group. At the end of the study, use of the combination of metformin with melatonin resulted in a greater reduction in total cholesterol and low-density lipoprotein by 5.2% and 11.2%, respectively, versus 3.3% and 6.0% in metformin alone group. The level of high-density lipoprotein has increased on 17.4% in Group 2, and on 9.6% in Group 1. Insulin resistance index HOMA-IR decreased by 29.3% in Group 2 versus 22.6% in Group 1 (p < 0.05). The levels of leptin and C-reactive protein decreased by 16.8% and 25.7% in Group 2, and by 14.4 and 7.0%, respectively, in Group 1 (p < 0.05). The adiponectin concentration increased by 10.8% in Group 2 versus 9.9% in Group 1 (p < 0.05). In addition to the overall beneficial effect on lowering blood pressure (BP), a combination of melatonin and metformin had a positive effect on circadian BP profile. Among this group of patients, the number of “non-dippers” has decreased by 54% and “night-pickers” by 22% according to the results of 24-h BP monitoring (p < 0.05). There were no significant changes in the circadian BP profile of patients in Group 1. Vascular elasticity and arterial stiffness significantly improved: pulse wave velocity decreased by 10.3% in Group 2 (p < 0.05), versus insignificant reduction (2.2%) in Group 1, the augmentation index fell by 17% in Group 2 and by 9.4% in Group 1 (p < 0.05), meanwhile, the rate of flow-dependent vasodilatation of the brachial artery increased by 9.4% in Group 2 and by 8.8% in Group 1 (p < 0.05). No serious adverse events reported during the study.
Conclusion: Findings of our survey showed that the use of prolonged-release melatonin 2 mg per day in addition to standard therapy in patients with MS with manifestations of sleep disorders has led to the effective reduction of body weight and adipocytokines levels, the positive dynamics of the metabolic and hemodynamic parameters, as well as improvement of the sleep quality and the normalization of sleep–wake pattern.
References
- IDF (International Diabetes Federation) The IDF consensus worldwide definition of the metabolic syndrome (booklet online). 2005. Available from: http://www.idf.org/webdata/docs/IDF_Meta_def_final.pdf [last accessed 11 Oct 2014]
The endocrinology of cognitive disorders
Yu. TishovaE-mail: [email protected]Abstract
Age-related (senile) dementia is one of the most important medical and social problems and one of the most complicated conditions for treatment and prophylaxis today. It is known that the development of many age-related diseases is related to insulin resistance (IR). It is known that there are key mechanisms accompanying all age-related changes. In addition to IR, these mechanisms include age-related hormone deficiency (menopause in women and late onset hypogonadism in men – the loss of estrogen, progesterone and testosterone), vitamin and micronutrient deficiency (especially – vitamin D deficiency), oxidative stress, loss of the lean muscle mass and development of the chronic inflammation (so-called “cytokine stress”). All these processes are involved in age-related dementia and memory loss development.
All of the above data, enhanced by unique modern experiments in vivo, suggest that understanding the mechanisms of age-related neurodegeneration and the neuroendocrine relationships of these pathological changes, can help not only in treatment, but also in preventing of the age-related neurodegenerative conditions.
The talk outlines the current understanding of the pathogenesis of age-related neurodegeneration, the role of hyperinsulinemia, insulin signal damage, IR, hormone deficiency, vitamin D deficiency, oxidative stress, etc. in the development of age-related dementia. The novel complex approach to prophylaxis and treatment of age-related memory loss and dementia is suggested.
“Mysterious” DHEA and melatonin: causes, symptoms of deficiency and correction methods
I. TyuzikovE-mail: [email protected]Abstract
Currently, one of the most popular theories of aging and age-related diseases’ pathogenesis is the free radical (theory of oxidative stress) and endocrine (elevation) theories, which were originally formulated independently in the 20th century. However, modern science has shown close relationship between these theories, which is realized through the active participation of hormones in the regulation of the level and direction of redox reactions in the body in health and disease. It is known today that hormones are potent mitochondrial protectors providing adequate function of the mitochondria, in which а key cellular scenario to combat pathological oxidative stress takes place.
In this regard, the study of DHEA endocrinology seems urgent to focus anti-aging medicine as well as a reduction in the level of this hormone after age 30 was significantly associated with oxidative stress, initiating age-related diseases.
DHEA (dehydroepiandrosterone) is a pro-hormone for further synthesis of testosterone and estrogens, therefore hypercortisolemia conditions associated with any stress when traditional synthesis of sex hormones in the gonads is significantly reduced, substantially raise the role of DHEA as a pro-hormone for self-synthesis of required sex hormones by the extragonadal way. It has been found that such extragonadal (intracrine) synthesis of sex hormones from DHEA takes place in breast and prostate, skin, muscle tissue, brain, female vagina, which makes DHEA an extremely important hormone ensuring the functioning of these organs and tissues. In particular, formed by intracrine up to 35% of androgens in males, up to 70% of sex hormones in premenopausal women and up to 100% of all the sex hormones in postmenopausal women are formed by the intracrine way. The identified active participation of DHEA in cell intracrine synthesis of sex steroid hormones in breast tissue and prostate allows today to review the role of sex hormones in the mechanisms of carcinogenesis of these organs. The ability of the vaginal epithelium to intracrine synthesis of testosterone and estrogens from DHEA allows the use of its local agents for topical treatment of genitourinary menopausal syndrome (GUMS) in women who have contraindications to classical hormonal preparations within the menopause hormone therapy (MHT), which has already been reflected in the new IMS 2016 Guidelines.
Nowadays comes the understanding that DHEA is not only a substrate for further synthesis of testosterone and estrogens, but also an independent active multifunctional hormone, the deficiency of which is associated with a wide range of age-associated diseases. In this regard, we are now actively studying the possibility of DHEA replacement therapy in older people, as reported by the currently available meta-analyses.
However, we should not forget that the function of the hypothalamic-pituitary system, which regulates the synthesis of sex hormones, in its turn, is controlled by a key circadian biological mechanism epiphyseal melatonin, which also has an additional range of unique physiological effects because of uniting into a single system with peripheral melatonin, secreting regardless of light level. The secretion of epiphyseal melatonin occurs only in the dark, so taking into account round-the-clock life of the modern people and the redundancy of night lighting in the big cities, for most modern people melatonin synthesis in the pineal gland is greatly disturbed.
Melatonin deficiency at any age leads to insomnia and the whole bouquet of diseases caused by increased oxidative stress, reducing the duration of human life. It closes the “vicious circle of pathogenesis” of age-associated pathology. In these circumstances, it is clear that without the identification and correction of melatonin deficiency it is impossible to deal with age-related pathology and poor quality aging. Today there are effective medications – melatonin analogues, the use of which can significantly optimize the pathogenetic therapy of age-associated diseases.
Thus, in the pathogenetic mechanisms of age-associated pathology close interaction of hormonal factors, among which a significant role belongs to DHEA and melatonin, is observed.
Features of androgen metabolism and their precursors in BPH
I. TyuzikovS. KalinchenkoYu. TishovaE. GrekovL. VorslovVorslov L.O. E-mail: [email protected] Tyuzikov I.A. E-mail: [email protected] Kalinchenko S.Yu. E-mail: [email protected] Tishova Yu. A. E-mail: [email protected] Grekov E.A. E-mail: [email protected]Abstract
Introduction: According to conventional wisdom, benign prostatic hypertrophy (BPH) is considered to be age-associated, prone to chronic progression disease of the prostate, the major pathogenetic mechanisms of which consist in imbalance oolation of cholesterol metabolism, hypoxia and chronic inflammation. Despite the recognized role of sex hormones imbalance in BPH pathogenesis, its hormone therapy is very rarely carried out in practice, and traditional approaches to drug therapy of advanced disease consist in the prescription of drugs exerting their effects mainly in the prostate and adjacent organs (bladder). However, sex hormones are key factors for prostate metabolism because the prostate gland is one of the most hormone-dependent organs. Nowadays the role of testosterone deficiency in BPH pathogenesis is well studied, however, the synthesis of testosterone is a single cycle in which the final biochemical product (testosterone) is formed by the transformation of its metabolic precursors (progesterone and dehydroepiandrosterone (DHEA)), the role of which in the pathogenesis of BPH has almost not been studied.
Objective: To study the correlation between plasma levels of total testosterone, progesterone, DHEA and prostate volume in men with BPH.
Methods: Study group consisted of 40 men with BPH aged 50–65 years (mean age 57.5 ± 2.3 years). All sex steroid hormones were determined in the blood plasma taken in the morning, by gas chromatography–tandem mass spectrometry. The following referent values were accepted as normal for this method: total testosterone – 0.8–2.7 nmol/L, progesterone – 0.8–3.9 nmol/L, DHEA – 15–65 nmol/L. The volume of the prostate by transrectal was determined by standard method of transrectal US and expressed in cm3. Statistical analysis of the material was performed using Statistica 6.0 software (StatSoft, Tulsa, OK), correlation analysis was performed using Pearson’s r co-efficient. Reliability criterion p < 0.05 was considered as statistically significant.
Results: Total blood testosterone level was lowered in 12/40 (30.0%) of men with BPH, the blood progesterone level was in the range of border low level in 15/40 (37.5%) of men with BPH, and the decrease of DHEA plasma levels was found in 19/40 (47.5%) patients with BPH. Plasma levels of these hormones were reducing according to the increase in the age of patients (p < 0.05). The average prostate volume was 38.5 ± 4.6 cm3 (CI: 26–54; p < 0.05). There was a significantly inverse correlation of ultrasound prostate volume with plasma levels of DHEA (r=–0.403; n = 40; p < 0.01), total testosterone (r=–0.283; n = 40; p < 0.01) and progesterone (r=–0.165; n = 40; p < 0.01). These hormonal findings in men with BPH allow to suggest that the age-related decline in testosterone synthesis plays a significant role in the pathogenesis of BPH, however, one of the direct causes of age-related phenomenon can be progressive with age adrenal insufficiency, accompanied by a decrease in progesterone synthesis and especially DHEA, which are biochemical precursors of testosterone deficiency leading to it, and all these factors together are, obviously, trigger mechanisms of 5-α-reductase activation, ending with glandular prostatic proliferation and hyperplasia and the formation of BPH.
Conclusion: BPH is a system dyshormonal age-related disease, reflecting changes in the metabolism of the prostate against a background of the progressive shortage of adrenal prohormones (progesterone and DHEA) and testicular testosterone. Thus, it is the adrenal gland which may play a more critical role in the pathogenesis of BPH than it is commonly believed. Further detailed studies of this question will bring greater clarity to the issue and, obviously, form new pharmacotherapeutic options for more effective management of such common disease as BPH.
Andrology aspects of melatonin deficiency
I. TyuzikovS. KalinchenkoYu. TishovaE. GrekovL. VorslovVorslov L.O. E-mail: [email protected] Tyuzikov I.A. E-mail: [email protected] Kalinchenko S.Yu. E-mail: [email protected] Tishova Yu. A. E-mail: [email protected] Grekov E.A. E-mail: [email protected]Abstract
Introduction: It seems that no one argues with the evident fact that the invention of electricity radically changed the life of a person. Modern man leads an active night life, making transmeridian flights, doing shift work, spending much time on the Internet, so the night Earth from outer space can be seen quite brightly lit (especially over the United States, Europe, Southeast Asia). “Artificial light poisoning” is a new unfavorable trend of the 21th century, which, according to most researchers, threatens us all with electronic insomnia. Sleep hormone – melatonin – is synthesized and secreted by the epiphysis (the pineal gland) at the necessary physiological concentrations only in complete darkness of the night, so it is clear that for Earth inhabitants its synthesis is dramatically disrupted, besides, secretion of melatonin by the pineal gland begins to decline after 25 years and this decline only progresses with the age. However, melatonin in the body forms the whole hormonal system that regulates all the chronobiology (circadian rhythms) and most of the organs and systems because it is the unique “conductor” of hypothalamic-pituitary-gonadal axis, without which virtually none of the physiological processes in the body can take place. Effect of melatonin deficiency on men’s health has been studied extensively, but the question is insufficiently presented in the Russian literature.
Objective: To study the frequency of melatonin deficiency in men and to identify the correlation between the level of melatonin and some indicators of men’s health.
Group for studies and methods: The group for studies consisted of 30 “healthy” men aged 18–60 years, for whom the steroid profile of saliva was carried out to determine the level of melatonin in it. Saliva sampling was produced at the peak of daily melatonin secretion (between 1.00 and 3.00 o’clock in the morning), saliva melatonin levels at this time of day, equaling to 52–149 pg/ml, was taken as the norm. For all men, bioimpedance body examination (determination of the amount and ratio of fat and muscle mass) was performed and the degree of peripheral blood oxygen saturation by pulse-oximetry (rate > 98%) was determined; diagnostics of endothelial dysfunction and oxidative stress according to the age of blood vessels and properties of the vascular wall by the method of contouring photopletizmografic analysis (Angioscan, Rio de Janeiro, Brazil) was carried out. Statistical analysis of the material was performed using Statistica 6.0 program (StatSoft, Tulsa, OK). Reliability criterion p < 0.05 was considered statistically significant.
Results and discussion: In 9/30 (30.0%) surveyed men melatonin deficiency was identified. The bioimpedance analysis showed that men with melatonin deficiency had significantly more fat mass and significantly less muscle mass with comparable indicators of waist circumference and body mass index (BMI), even in the absence of criteria for obesity (p < 0.05). Indicators of oxygen saturation of peripheral blood were insignificantly worse for men with deficiency (93–95% with melatonin deficiency versus 94–97% without its deficiency; p < 0.1), but the elastic properties of blood vessels were significantly worse, and vascular age was significantly older for men with melatonin deficiency (p < 0.05). Identified findings suggest an evident negative impact of the melatonin deficiency on metabolism and health characteristics for men.
Conclusion: Approximately one in three of so called “healthy” men showed a latent melatonin deficiency, which is not manifested as its classical clinical picture of insomnia, but contributes to the inconspicuous progression of obesity, sarcopenia, endothelial dysfunction, hypoxia on the background of oxidative stress. In andrological practice, one should pay more attention to assessing the quantity and quality of nighttime sleep of men, and in the absence of other diagnosed reasons of the metabolic disorders described above, to examine melatonin levels, as the correction of melatonin deficiency will allow to effectively solve the problems of men’s health.
Combination of urological pathology with obesity and metabolic syndrome in men of mature age
O. VasilevaE. NovikovaD. DeevB. PinkhasovV. SelyatitskayaE-mail: [email protected] Novikova Elena Genadyevna, Senior researcher, PhD, E-mail: [email protected] Deev Denis Aleksandrovich, postgraduate, E-mail: [email protected] Pinkhasov Boris Borisovich, Leading researcher, MD, PhD, E-mail: [email protected] Selyatitskaya Vera Georgievna, Chief researcher, PhD, prof, E-mail: [email protected]Abstract
Introduction: Obesity and metabolic syndrome (MS) are key elements of not only the cardiovascular diseases pathogenesis but also urological diseases such as chronic prostatitis, erectile dysfunction, hypogonadism, etc. Obesity is a heterogeneous disease and different types of the obesity, android (abdominal) and gynoid, show various degree of risk of development of the associated diseases. Thus, the abdominal obesity is the main component of the MS, which severity is directly related to expression of cardiometabolic risk in men and women, at the same time gynoid type of obesity has the features of “metabolically healthy” obesity in a greater extent. The purpose of this study was to estimate the frequency and the ratio of obesity types and to establish the relationship between these types and the severity of the MS components in men with urological pathology.
Methods: Men (n = 218) who applied for the ambulatory urological care in the medical center of Novosibirsk with chronic prostatitis and/or the lower urinary tract symptoms (90% and 10% respectively) were examined.
Mean age was 37.2 years (from 20 to 60 years). All men lived in Novosibirsk and Novosibirsk region. Anthropometric indices were determined: body length (BL, m), body weight (BW, kg), waist circumference (WC, cm), hip circumference (HP, cm) and the value of the ratio WC/HP in conventional units. Android type of fat distribution was set at the value of the ratio WC/HP ≥ 0.95; gynoid type – WC/HP < 0.95. Based on the results of anthropometric measurement men were divided into five groups:
group 1 (n = 61) – BMI < 25 (normal weight);
group 2 (n = 51) – 25 ≤ BMI < 30.0; WC/HP < 0.95;
group 3 (n = 41) – 25 ≤ BMI < 30.0; WC/HP ≥ 0.95 (groups 2 and 3 – overweight);
group 4 (n = 13) – BMI ≥ 30.0; WC/HP < 0.95;
group 5 (n = 51) – BMI ≥ 30.0; WC/HP ≥ 0.95 (groups 4 and 5 – obesity).
Criteria of NCEP-ATP III in modification of 2005 were used for identification of MS and its components. Statistical data processing was performed using the “STATISTICA” v.10.0 program (StatSoft, Tulsa, OK).
Results: In the general sample of men of mature age with urological pathology, the frequency of patients with overweight was 42.4%; the obesity was revealed in 29.5% of the examined men. In the sample of men with the overweight and the obesity, the android type of fat distribution was revealed in 58.9% of cases (in 44.6% of men with overweight and in 79.7% of men with obesity), MS – in 51.9% of cases (in 37.0% of men with overweight and in 73.4% of men with obesity). Among men with overweight and obesity, the frequency of the MS components was: abdominal obesity – 47.4%, hypertriglyceridemia – 55.8%, high density lipoprotein low level – 26.3%, hyperglycemia – 27.5%, arterial hypertension – 66.0%. At the same time, the higher frequency of cases of a hyperglycemia (41.3 and 7.8% respectively), arterial hypertension (83.7 and 40.6% respectively) and the MS (72.8 and 21.8% respectively) was characteristic of android type of obesity in comparison with gynoid type.
Comparison of the results with the data of the survey of random sample men in Novosibirsk [Citation1] was showed, that in the structure of MS in men with urological pathology the frequency of abdominal obesity, hypertriglyceridemia, high density lipoprotein low level was 20–30% lower, while the frequency of hyperglycemia and arterial hypertension – does not differ from men of a random sample. In men with urological pathology and android type of fat distribution, the frequency of hyperglycemia was higher compared to men with android type of fat distribution of a random sample.
Conclusion: In men with overweight and obesity, the presence of urological diseases (chronic prostatitis and lower urinary tract symptoms) was associated with increased frequency of hyperglycemia, which confirms the role of insulin resistance in the pathogenesis of these diseases at obesity.
Reference
- Pinkhasov BB, Selyatitskaya VG, Karapetyan AR, Lutov YV. Association of aging-related obesity and metabolic syndrome in men. Adv Gerontol 2016;6:224–30
Estrogens in men – good or evil?
L. VorslovE-mail: [email protected]Abstract
The current scientific data give us a lot of information describing the role of testosterone in men. The diagnosis of testosterone deficiency in men is a clear and simple procedure, and the clinical signs and symptoms of testosterone deficiency are well-defined today.
At the same time it is known, that men also produce estrogens. The circulating estradiol in men is derived from the aromatization of testosterone. But the role of estrogens in men remains mostly unclear, is still poorly understood and underestimated. There is a point of view that estrogens are an “evil” for the male body and so-called “estrogen excess” is the reason for obesity, gynecomastia, erectile dysfunction, infertility and the signs of “feminization”. According to this concept, aromatase inhibitors are widely prescribed “to lower estrogens” in men. Is there any rationale for this therapy?
From the other side, it is obvious, that as serum testosterone levels decline, there is a concomitant decline in serum estradiol levels. Nevertheless, the consequences of male hypogonadism are routinely attributed solely to androgen deficiency; the potential role of the concomitant decline in estrogens is typically ignored.
There are studies, confirming that estrogen deficiency in men may be the key factor in the pathogenesis of bone loss, increase in body fat, decline in sexual function and male infertility.
The talk reviews the basic role and functions of estrogens in men. Possible targets of estrogen action in male body are suggested.
Proper understanding of the role of estrogens in men may provide a rationale for novel physiological approaches to male age-related hormone deficiency treatment.
Which psychosocial risk- and resilience factors are associated with buffered age-related sex steroid decline, deterioration in body composition and decline in sexual function in aging males? Summary of the study men’s health 40+
A. WaltherU. EhlertE-mail: [email protected], [email protected]Abstract
Background: Age-related alterations occur in different dimensions in aging males. A continuous decline in sex steroids, a steady deterioration in body composition, and decreasing sexual health often lead to androgen deficiency, sarcopenia or erectile dysfunction. Specific treatments are offered for each condition, while little is known about the influence of psychosocial risk and resilience factors.
Methods: We, therefore, investigated 271 self-reporting healthy men and obtained psychometric data, data on body composition, and endocrine parameters.
Results: Moderation analysis of the association between age and declining sex steroids revealed significant moderation effects for psychosocial factors such as depression, chronic stress and perceived general health. Moderation analysis of the association between age and body composition revealed significant moderation effects for depression and emotional support. Moderation analysis of the association between age and sexual health revealed significant moderation effects for perceived general health, emotional support and intimacy motivation.
Conclusion: Emerging psychosocial risk and resilience factors play an independent role in maintaining and promoting healthy aging in men. Besides physical, also psychosocial factors should be addressed more accurate from health professionals for maintenance of health in aging.
System of psychotherapeutic correction of sexual disharmony during androgen deficiency
M. ZakaryanE-mail: [email protected] Tel: (+374)-91-42-75-69Abstract
Introduction: Psychotherapeutic correction of sexual disharmony is a system of correcting measures including individual, couple and group psychotherapy methods.
We have modified and adapted the system of psychotherapeutic correction of sexual disharmony for married couples in which males had androgen deficiency and sexual dysfunction.
The development of sexual disharmony of married couples in cases when male suffers from androgen deficiency and sexual dysfunction is dependent not only on sexual function loss caused by main pathology, but also on psychological, sociopsychological and sexual behavioral adaptation.
During differentiated psychotherapeutic correction procedure one must consider clinical form of the androgen deficiency, specific manifestations and personal qualities of the patient.
The psychological correction of patients with androgen deficiency is directed at emotional state normalization, hyper-irritability and affective reactions control, decrease of general and psychic tones.
Methods: During psychotherapeutic correction procedures, we used these common psychotherapeutic methods: hypnose suggestion, emotional-volitional training, rational psychotherapy, autogenic training, sexual behavioral training.
Emotional-volitional trainings were carried out by A.T. Filatov method.
Hypnose suggestion was directed at neurotic process remission and sexual function normalization.
Results: Psychotherapeutic correction of sexual health problems of men with androgen deficiency has a lot of distinctive features. First, it must be directed both at neurotic condition elimination and at sexual function normalization. Second, correction must involve the spouse of the patient also considering their interpersonal relationship. Third, it is important to consider the causes and conditions of personalization disturbance for both spouses.
Listed combination of the methods and techniques of psychotherapeutic correction with consideration of all the components of sexual harmony and their features gave the opportunity of having maximum results.
Summary: We examined the results of correction procedure after each treatment, as well as during revisiting and scheduled visits (1–2 times a year) of treated patients.
We emphasize that the effectivity of psychotherapeutic correction of sexual disharmony not always coincide with effectivity of androgen deficiency treatment.
So, the therapeutic correction of sexual disharmony during androgen deficiency is an optimal method which should be utilized altogether with different techniques and modifications.
Declaration of interest
There were no reports of any potential conflict of interests associated with this article. The authors declare that they have no competing financial interests. The authors assume liability for general content and impartiality of the article.