
Abstract
Background: The androgen deficiency in the aging male (ADAM) affects physical, sexual, and psychological aspects with characteristics symptoms of middle-aged men. The practice of regular physical activity and physical exercise can attenuate these symptoms. The aim of this randomized clinical trial is to propose a physical exercise protocol based on concurrent training for middle-aged men with ADAM.
Method: Randomized clinical trial with a 6-month intervention will randomly divided into two groups: experimental group (EG) and control group (CG). Four evaluations will be carried out, (1) pre-intervention; (2) in the first month of intervention; (3) in the third month of intervention; (4) post-intervention, evaluating: physical, psychological, sexual, and hormonal aspects. The intervention protocol with concurrent training will have duration of 6 months; frequency of 3 times weekly, with 60 min per session. The two-way ANOVA test will be used for the inter-group and intra-group comparisons with repeated measurements, and also Sydak’s comparison test.
Conclusion: This protocol was developed with the intent of easing the symptoms of ADAM. In addition, it is believed that the concurrent training protocol could be capable to recover hormonal, physical, psychological, and sexual aspect of middle-aged men with ADAM.
Keywords:
Introduction
Globally, the androgen deficiency in the aging male (ADAM) affects from 22.7% to 81.3% of men from 40 years of age [Citation1–3]. It is a process characterized mainly by a decrease in testosterone levels, associated with signs and symptoms that lead to a decline in quality of life and libido [Citation4]. The decrease in testosterone levels in men can be observed soon after the third decade of life, with a decrease of approximately 0.4% per year, and as from 40 years of age this percentage increases to 1% or 2% [Citation5]; being that the lower testosterone levels, the greater the health risks [Citation6], considering that the identification of these levels of testosterone by blood collection may be more effective compared to salivary testosterone [Citation7]. In addition to the physiological aspect, somatic, psychological, and sexual symptoms also appear with slight, moderate, or severe intensity [Citation8]. In this context, many alterations can be observed including the somatic symptoms of a decline in the general sensation of well-being, decrease in muscle strength, muscle and joint pain, insomnia, sweating, and physical exhaustion. Among the alterations related to the psychological symptoms one could cite anxiety, discouragement, depressive state of spirit, irritability, and nervousness. Within the sexual aspects, symptoms appear such as decreases in beard growth, sexual capacity and frequency, sexual desire, and the number of morning erections [Citation8].
Considering these facts, actions are required that serve to ease the symptoms of this phase and their negative effects on health and also act in their prevention, and the national and international literature has verified the important role of physical exercise with respect to these symptoms. If practiced regularly according to the recommendations of the WHO of 150 min/week [Citation9], it contributes to a reduced prevalence of these symptoms [Citation10,Citation11]. In addition, the intensity of the physical activity and the time for which it is practiced can influence both the prevalence of ADAM and the intensity with which the symptoms occur [Citation12].
Although physical activity has already been related to ADAM process, little is known experimentally about the effects of physical exercise; a systematized activity, in the health of men at this stage. These findings are based on the findings of a study on the effects of erectile dysfunction on the erectile dysfunction of men with erectile dysfunction [Citation13]. Furthermore, there is evidence of interventions that showed an improve on total testosterone levels of men [Citation14], in addition, in relation to the general state of health of middle-aged and/or elderly men, physical exercise interventions has reflected an increase in strength, lean mass, metabolic and hormonal responses, and cardiovascular benefits [Citation15–17]. Thus, it is identified that both the study for men with ADAM and for men in middle age acted with aerobic and resisted physical exercises, in moderate to vigorous intensity, with duration of at least 12 weeks, and frequency of 2–3 times weekly [Citation13,Citation16–18].
Thus, it is recommended to combine aerobic and resisted exercise in the same session, aiming at an effective form of physical exercise prescription [Citation19], characterizing the concurrent training. This type of training has been approached in the literature as a model of effective intervention program for the health of men in middle age, verifying positive effects on the components of metabolic syndrome [Citation20], inflammatory biomarkers [Citation21], and cardiovascular diseases [Citation22]. In this way, it is observed that concurrent training can be beneficial for the male population in this age group, being considered a viable option for treatment, maintenance and recovery in the health/disease process of middle-aged men [Citation22].
According to the literature, these benefits occur because concurrent training promotes different cardiovascular and neuromuscular adaptations in the body; since aerobic exercise improves cardiac and respiratory function, increasing the capacity of oxygen uptake and utilization, decreases lipid concentration in the blood, and is able to influence the individual’s psychological aspect, contributing mainly to the reduction of depressive symptoms; and resistance exercises benefit the development of muscle mass and consequently strength, as well as the muscle’s ability to generate and use energy, and may also be associated with mental health by reducing sensitivity to anxiety levels [Citation23–25].
In this way, it is believed that this training can positively impact the ADAM process [Citation26], since the mentioned aspects are negatively affected in this phase of life [Citation8]. In addition, these types of exercises are responsible for the improvement of blood flow and circulation [Citation27], which acts directly and indirectly on the penile vascularization, and consequently contributes to the sexual aspect of man, also intervening in the psychological health [Citation28].
Therefore, the primary aim of this randomized clinical trial is to propose a physical exercise protocol based on concurrent training for middle-aged men with ADAM. The secondary aim will be to evaluate the effects of this protocol on the hormonal aspects (total and free testosterone level); physical (body mass index, percentage of body fat, abdominal obesity, muscular strength, and cardiorespiratory fitness); psychological (depressive symptoms, anxiety, and stress); sexual (erectile function, orgasmic function, sexual desire, sexual satisfaction, and overall satisfaction); and ADAM. The hypothesis of the study is that the concurrent training protocol will promote the improvement in the ADAM symptoms, considering its presence and intensity, as well as the positive impact on the hormonal, physical, psychological, and sexual aspects, being an option allied to the pharmacological therapy in the treatment for men with ADAM.
Methods
Experimental approach to the problem
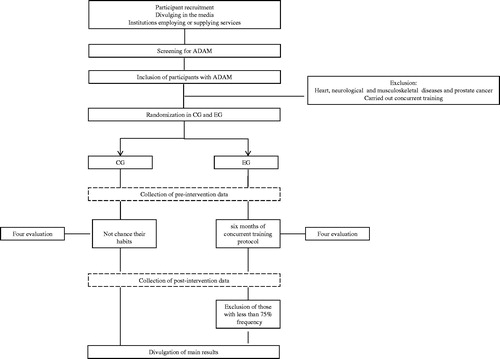
This is a randomized clinical trial with 6 months of intervention and four evaluations, as follows: (1) pre-intervention, (2) in the first month of intervention, (3) in the third month of intervention, and (4) post-intervention. The study will include two groups: the experimental group (EG) and the control group (CG) ().
Figure 1. Study selection and execution schedule.
Participants
Recruitment and selection criteria
The participants in this study will be middle-aged men (40–59 years old) from the cities of Florianopolis and São José in the State of Santa Catarina, Brazil, recruited in the following two ways: (1) divulging of the survey in the media (radio, TV, and Internet) and (2) divulging in institutions employing or supplying services at the levels of education, health, justice, religion, and insurance. The same men will be invited to take part in the study and fill in a questionnaire (Aging Males’ Symptoms scale) for the screening of ADAM. Those presenting a positive score in the questionnaire for ADAM symptoms will be invited to carry out a blood test for screening of the testosterone levels.
The inclusion criteria will be: men presenting ADAM according to their responses on the Aging Males’ Symptoms scale [Citation29] and testosterone levels <317 pmol/L [Citation30]. Those with a history of neurological or musculoskeletal diseases or who have prostate cancer will be excluded, as also those who have been submitted to concurrent training in the 3 months prior to data collection.
Randomization and blinding process
The participants will be distributed at random among the EG and CG in 10-participant blocks, using the Microsoft Excel® program, and blinded to condition them to the attribution.
In the sample selection process, the interviews and data collection will be carried out by researcher A and the application of the concurrent training protocol by researcher B. Researcher B will have no knowledge of the results of the variables collected in the pre-intervention period and subsequent evaluations, characterizing the blinding process of the researcher.
Sample size calculation
Twenty-nine individuals will be designated to each group (EG and CG) according to the sample calculation. The ADAM symptoms score was used as the primary endpoint variable. For the comparison of symptom scores between groups, based on a pilot study with middle-aged men (unpublished data) as proposed by Whitley and Ball [Citation31], the effect size was 0.80, level of significance of 5%, 95% test power, and 20% sample loss.
shows the participant selection process and execution of the study stages.
Outcome measures
Interventions for the middle-aged male population with ADAM are still scarce in the literature and only concern a sexual symptom [Citation16]. However, it can be observed that, in the case of this age group in different health conditions, the studies use the concurrent training as a form of intervention [Citation20–22]. Thus, it is considered that an intervention with this type of training can act in a beneficial way to the physical, psychological, and sexual levels of the men with ADAM, considering all aspects of the symptomatology ().
Table 1. Variables and instruments to be applied in individuals with ADAM.
Control group
Participants randomly selected for the CG will perform the assessments and will be submitted to four evaluations: (1) pre-intervention, (2) in the first month of intervention, (3) in the third month of intervention, and (4) post-intervention. They will be instructed not to make changes in their physical exercise habits over the 6-month study period, in addition, they will receive monthly follow-up visits in order to verify if they are maintaining their usual activities.
After explaining the objectives of the study, the researcher will schedule the interview and data collection with the participant at the Health and Sports Science Center of the Santa Catarina State University.
Experimental group
The EG will be composed of participants randomly placed in this group and will be submitted to four evaluations: (1) pre-intervention, (2) in the first month of intervention, (3) in the third month of intervention, and (4) post-intervention. The importance of assiduity at the classes was reinforced (minimum of 75% frequency) in order to obtain significant health benefits. The evaluation measurements will be obtained by applying a questionnaire and making some physical evaluations. Both the data collection and the intervention will be carried out in an academy in Florianópolis, Santa Catarina, Brazil. After completing the evaluation procedures, the intervention period will be started with a frequency of 3 times a week, each session lasting 60 min, according to the study protocol.
Intervention protocol
In this protocol, participants will perform aerobic and resistance training according to published evidence for middle-aged men [Citation20–22]; characterized as concurrent training [Citation32].
The protocol will last 6 months and will be divided into two trimester. Initial 30 min will be assigned to aerobic training, followed by 30 min of resistance training. Aiming to obtain benefits in the levels of muscular strength, aerobic capacity, body composition, besides positive results in relation to the hormonal adaptations of testosterone, as well as in the psychological well-being of participants.
Classes will occur at a frequency of 3 times weekly, lasting 60 min a session.
Aerobic training
The aerobic training of this protocol will follow the American College of Sports Medicine [Citation33] prescription guidelines for health of healthy adult individuals, according to the characteristics and specifications in .
The aerobic training will be performed on a treadmill, and exercise intensity will be controlled using the Borg CR-10 scale [Citation34]. In addition, the heart rate will be monitored using a digital pulse oximeter.
The Borg CR-10 scale (category ratio) is determined by internal psychophysical criteria. This scale follows a score from 0 to 10 (), in which 0 means absolutely nothing and 10 extremely strong, representing the maximum intensity. CR10 is a general intensity scale for subjective magnitudes, and can be used for the measurement of effort with the possibility of determining relative and absolute levels of intensity () [Citation34].
Table 2. Specifications of aerobic training in the 6 months of intervention.
Table 3. Borg CR-10 scale.
Table 4. Resistance training specifications in the 6-month intervention.
Table 5. Resistance exercise program to be performed in each month of the intervention.
Resistance training
For the development of this protocol, will be followed the guidelines of the American College of Sports Medicine for resistance training for healthy adults [Citation23], as well as evidence published for men in middle age [Citation21,Citation35]. The training specifications in the first and second trimester of the intervention are described in .
The exercises to be performed according to the specifications of will be modified each month, as shown in . The heating in this part of the protocol will consist of a series of 12–15 repetitions with 40% of a maximum repetition (1RM) in the first exercise of each body segment.
Participants will undergo a period of neuromuscular adaptation to resistance training, with the aim of learning and correcting the motor process in each exercise; this period of familiarization will consist of three sessions on alternate days: three series with submaximal load perceived for 12 repetitions, and intervals of 45 s between sets and 60 s between exercises. The following exercises will be performed: bench press machine, leg press 90°, rower machine, leg flexion machine, lateral lifting with halter, and adduction machine.
The prediction of 1RM will be performed by submaximal test. For this test, the equation of Baechle and Groves [Citation36] will be used: 1RM = load × [(0.0375 × repetitions) + 0.978]. First, a warm-up series will be performed, with one exercise for upper limb and one for lower limb with 50% of perceived submaximal load for 12 repetitions; after an interval of 2 min, the test will start. Participants will be instructed to select a load for the maximal perceived effort of 10 repetitions, taking no more than three attempts at 3–5 min intervals to seek the concentric failure of the movement within the boundary margin for the number of set repetitions. It will be considered an attempt fail in which the participant exceeds 10 repetitions. At every attempt, fail the load will be increased by 20%. If the participant exceeds all three attempts, the participant will retake the test after 48 h of interval. The submaximal test for prediction of 1RM will be performed monthly with each training modification, with the exercises corresponding to the new programming; the test will be applied by a Physical Education professional, trained to do so.
Data collection procedure
The project was approved by the Ethics Committee on Research in Human Beings of the State University of Santa Catarina (protocol n. 2.274.655) and registered on the international clinical trial registration platform “Clinical Trials.gov” n. NCT03150225. In a first moment will be made a contact with the men to participate of the study. In this contact will be explained the purpose, importance and all the procedures of the research, as well as the signing of the free and informed consent term. Participants will be submitted to blood collection by a Biochemist of the Laboratory of Multisectorial Analysis of the Health and Sports Science Center of the State University of Santa Catarina; according to the literature recommendation, should be performed between 7:00 AM and 11:00 AM [Citation37]. Blood samples will be collected after a 12-h fasting period. Later, the cardiorespiratory fitness, percentage of body fat, body mass, height, waist circumference, and muscle strength will be collected, as well as the submaximal test for prediction of 1RM, distributed among the researchers of the study.
The same researchers will conduct the interview with the participants inquiring questions related to the general characteristics of the men (age, marital status, schooling, economic level, presence of clinically diagnosed diseases, use of medications, and tobacco consumption); the questionnaire regarding depressive symptoms, anxiety, stress, and the sexual satisfaction questionnaire. The scale of the symptoms of male aging will have been applied in the period prior to all the aforementioned collections, since it will be part of the process of screening the participants.
Each participant will receive a coding number and their name will not be identified. Then, guided by the principal investigator of the study, the concurrent training protocol will be applied to the middle-aged men, without the knowledge of the physical evaluations and the answers of the questionnaires applied. This attempt to blind the researcher to the results of each variable aims at impartiality in determining the intensities and possible stimulations of the researcher in the performance of the participants during the activities.
Statistical analysis
The data will be tabulated and stored in the Microsoft Excel® program and analyzed by the SPSS – IBM (version 20.0) statistical package. All the variables will be analyzed in a descriptive way using simple frequency (categorical variables) or measurements of the position and dispersion (numerical variables). Comparative analyses will be applied between the results of the EG and CG after the 6-month intervention period, and also intra-group pre- and post-tests within both groups in order to observe possible alterations after the intervention. The two-way ANOVA test with repeated measurements and Sydak’s comparison test will be used for these analyses, with the level of significance established at 5%.
Discussion
An increase in the prevalence of ADAM has been observed in men from different countries in the last 10 years [Citation38–40]. As a result, many advances have been made with respect to the pharmacological treatment, as supplementation, for men searching to raise the testosterone levels [Citation41], but in addition to the positive effects, these treatments present some long-term adverse effects, and hence it has become necessary to implement non-pharmacological strategies to ease the negative effects of ADAM in the health of middle-aged men. Hence, the probable influence of physical activity in this process has been verified, although conclusive relationships cannot yet be established [Citation12,Citation42]. However, it has been documented in the literature that testosterone treatment, considered to be usual, associated with physical exercise, produces beneficial cardiovascular effects [Citation43].
Although, in general, the male population is considered sufficiently active, it is notable that as from 40 years of age, the interest in activities modifies, changing from the practice of vigorous physical activities to lighter ones such as walking [Citation44,Citation45]. Although light intensity physical activity shows health benefits, the literature indicates that for significant health benefits, the physical activity practiced by middle-aged men should be at least of moderate intensity [Citation17]. It is important to note that considering the physical aspect as body fat, a lifelong physical exercise practice may indicate higher levels of testosterone in older men [Citation46].
Thus the implementation of physical exercise programs that attend the needs of middle-aged men with ADAM is indispensable, as a means of helping them experience this process in a form less prejudicial to the health, increasing their levels of physical activity. However, specific programs for this population that consider all the blocks of symptoms of ADAM and not just a single symptom are still not available. It is possible that this void is due to the lack of access and/or knowledge of the information concerning the symptoms of ADAM, and also the difficulty of the men to consult a doctor and look for other forms of help in this process [Citation5].
It is considered that a protocol of physical exercise may be relevant to the health of men with ADAM, especially concurrent training, since in combining resistance and aerobic training it is possible to obtain benefits in the hormonal, physical, psychological, and sexual aspects of men. It is important to note that, although there is evidence in the literature that worked with this type of training as a form of intervention for the health of middle-aged men [Citation20–22], identifying improvement of cardiorespiratory fitness, body composition, blood pressure, and lipid profile; until the present moment, there is no knowledge of evidence that has acted with a concurrent training protocol for men with ADAM.
Thus, concurrent training protocol for men with ADAM: a randomized clinical trial, was developed in order to reduce the symptoms of ADAM, and their intensity, as well as to act in modulating testosterone levels, reducing body fat percentage, increase muscle strength, improve cardiorespiratory fitness, minimize depressive symptoms, anxiety, and stress, and contribute to a better quality of sexual life; being of utmost importance since there has been an aggravation to some health conditions in men with advancing age, such as abdominal fat, a predictor aspect of chronic diseases [Citation47]. In addition to this aspect, it also aims to influence and encourage the practice and maintenance of physical exercise at this stage of life, even after the end of the study application period. This protocol is composed of exercises aimed at a wave periodization, always considering the safety of the practice and the individuality of each practitioner. The activities included in the concurrent training protocol follow the indications of what has already been evidenced in the literature for men in middle age [Citation20–22].
Finally, it is considered relevant to implement a concurrent training protocol for men in middle age with ADAM, seeking new knowledge related to this topic of study. In view of the way in which the symptoms affect the life of the man, and considering that the lack of a specific intervention can be aggravating factor of the symptoms with the passage of the years; the practice of physical exercise for this population can enable the reduction of the symptoms of ADAM, maintenance of the associated factors and consequently, help in the improvement of daily activities, contributing to a better quality of life and general health. Also, it should be emphasized that the promotion of physical exercise with a specific protocol for men with ADAM should not only be carried out during a study period, but should be considered as an incentive to regular practice, with policy measures access to long-term benefits.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Blumel JE, Chedraui P, Gili SA, et al. Is the Androgen Deficiency of Aging Men (ADAM) questionnaire useful for the screening of partial androgenic deficiency of aging men? Maturitas. 2009;63:365–368.
- Chueh KS, Huang SP, Lee YC, et al. The comparison of the Aging Male Symptoms (AMS) scale and Androgen Deficiency in the Aging Male (ADAM) questionnaire to detect androgen deficiency in middle-aged men. J Androl. 2012;33:817–823.
- Ichioka K, Nishiyama H, Yoshimura K, et al. Aging Males’ Symptoms scale in Japanese men attending a multiphasic health screening clinic. Urology. 2006;67:589–593.
- Barboza RA, Silva EA, Damião R. Saúde masculina: daem - deficiência androgênica do envelhecimento masculino. Revista HUPE. 2010;9:40–47.
- Harisson J. Talking about my generation: a state-of-the-art review of health information for men in the andropause. Health Info Libr J. 2011;28:161–170.
- Maggio M, Ceda GP, Lauretani F, et al. Gonadal status and physical performance in older men. Aging Male. 2011;14:42–47.
- Hayes LD, Sculthorpe N, Herbert P, et al. Poor levels of agreement between serum and saliva testosterone measurement following exercise training in aging men. Aging Male. 2015;18:67–70.
- Heinemann LA. Aging Males’ Symptoms scale: a standardized instrument for the practice. J Endocrinol Invest. 2005;28:34–38.
- WHO. In: Global recommendations on physical activity for health, 18–64 years old. 2011; [cited 2016 Oct 1]. Available from: http://www.who.int/dietphysicalactivity/physical-activity-recommendations-18-64years.pdf
- Chen RYT, NG KK. Self-referred older Asian males in a men’s health clinic: the inter-relationships between androgens, metabolic parameters and quality of life measures. Aging Male. 2010;13:233–241.
- Corrêa LQ, Rombaldi AJ, Silva MC. Atividade física e sintomas do envelhecimento masculino em uma população do sul do Brasil. Rev Bras Med Esporte. 2011;17:228–231.
- Vieira MCS, Cardoso AA, Guimarães ACA. Male aging symptoms: the positive influence of moderate and total physical activity. Rev Bras Cineantropom Desempenho Hum. 2016;18:460–470.
- Condorelli RA, Calogero AE, Di Mauro M, et al. Effects of tadalafil treatment combined with physical activity in patients with low onset hypogonadism: results from a not-randomized single arm phase 2 study. Aging Male. 2016;6:1–6.
- Hayes LD, Sculthorpe N, Herbert P, et al. Six weeks of conditioning exercise increases total, but not free testosterone in lifelong sedentary aging men. Aging Male. 2015;18:195–200.
- Paunksnis MR, Evangelista AL, La Scala Teixeira CV, et al. Metabolic and hormonal responses to different resistance training systems in elderly men. Aging Male. 2017. DOI:10.1080/13685538.2017.1379489
- Liira H, Engberg E, Leppävuori J, et al. Exercise intervention and health checks for middle-aged men with elevated cardiovascular risk: a randomized controlled trial. Scand J Prim Health Care. 2014;32:156–162.
- Pelletier-Beaumont E, Arsenault BJ, Alméras N, et al. Normalization of visceral adiposity is required to normalize plasma apolipoprotein B levels in response to a healthy eating/physical activity lifestyle modification program in viscerally obese men. Atherosclerosis. 2012;221:577–582.
- Deibert P, Solleder F, König D, et al. Soy protein based supplementation supports metabolic effects of resistance training in previously untrained middle aged males. Aging Male. 2011;14:273–279.
- American College of Sports Medicine (ACSM). ACSM’s guidelines for exercise testing and prescription. 9th ed. Philadelphia (PA): Lippincott Williams and Wilkins; 2014.
- Souza GV, Libardi CA, Rocha JJ, et al. Efeito do treinamento concorrente nos componentes da síndrome metabólica de homens de meia-idade. Fisioter Mov. 2012;25:649–658.
- Libardi CA, Souza GV, Cavaglieri CR, et al. Effect of resistance, endurance, and concurrent training on TNF-α, IL-6, and CRP. Med Sci Sports Exerc. 2012;44:50–56.
- Atashak S, Stannard SR, Azizbeigi K. Cardiovascular risk factors adaptation to concurrent training in overweight sedentary middle-aged men. J Sports Med Phys Fitness. 2016;56:624–630.
- ACSM. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc. 2009;41:687–708.
- Fulks JJB, Kelso K, Zawilinski L. Effects of a single bout of aerobic exercise versus resistance training on cognitive vulnerabilities for anxiety disorders. Cogn Behav Ther. 2015;44:240–251.
- Joutsenniemi K, Tuulio-Henriksson A, Elovainio M, et al. Depressive symptoms, major depressive episodes and cognitive test performance—What is the role of physical activity? Nord J Psychiatry. 2013;67:265–273.
- Signorelli GR, Duarte CV, Ramos OS, et al. Melhoria da Capacidade Funcional Excede à da Condição Aeróbica: dados de 144 pacientes de programa de exercício. Rev Bras Cardiol. 2012;25:299–308.
- Bruning RS, Sturek M. Benefits of exercise training on coronary blood flow in coronary artery disease patients. Prog Cardiovasc Dis. 2015;57:443–453.
- La Vignera S, Condorelli R, Vicari E, et al. Aerobic physical activity improves endothelial function in the middle-aged patients with erectile dysfunction. Aging Male. 2011;14:265–272.
- Heinemann LAJ. The Aging Males’ Symptoms (AMS) scale: update and compilation of international versions. Health Qual Life Outcomes. 2003;1:15.
- Pye SR, Huhtaniemi IT, Finn JD, et al. Late-onset hypogonadism and mortality in aging men. J Clin Endocrinol Metab. 2014;99:1357–1366.
- Whitley E, Ball J. Statistics review 4: sample size calculations. Crit Care. 2002;6:335–341.
- Wilson JM, Marin PJ, Rhea MR, et al. Concurrent training: a meta-analysis examining interference of aerobic and resistance exercises. J Strength Cond Res. 2012;26:2293–2307.
- ACSM. Guidelines for exercise testing and prescription, 7° Edição, Rio de Janeiro: Guanabara Koogan S.A, 2006.
- Borg G. Borg’s perceived exertion and pain scales. Champaign (IL): Human Kinetics; 1998.
- Nikseresht M, Agha-Alinejad H, Azarbayjani MA, et al. Effects of nonlinear resistance and aerobic interval training on cytokines and insulin resistance in sedentary men who are obese. J Strength Cond Res. 2014;28:2560–2568.
- Baechle TR, Groves BR. Treinamento de força: passos para o sucesso. 2nd ed. Porto Alegre: Artmed; 2000.
- Diver M, Imtiaz K, Ahmad A, et al. Diurnal rhythms of serum total, free and bioavailable testosterone and of SHBG in middle-aged men compared with those in young men. Clin Endocrinol (Oxf). 2003;58:710–717.
- Goel A, Sinha RJ, Dalela D, et al. Andropause in Indian men: a preliminary cross-sectional study. Urol J. 2009;6:40–44.
- Lee AM, Chu LW, Chong CS, et al. Relationship between symptoms of androgen deficiency and psychological factors and quality of life among Chinese men. Intern J Androl. 2010;33:755–763.
- Rabah DM, Arafa MA. Validation of an Arabic ADAM questionnaire for androgen deficiency screening in the Arab community. Aging Male. 2009;12:95–99.
- Judge LW, Bellar DM, Hoover DL, et al. Effects of acute androstenedione supplementation on testosterone levels in older men. Aging Male. 2016;19:161–167.
- Corrêa LQ, Silva MC, Rombaldi AJ. Associação entre nível de atividade física nos diferentes domínios e sintomas do envelhecimento masculino. Rev Bras Ativ Fis Saude. 2014;19:186–194.
- Gonçalves L, de Souza RR, Maifrino LB, et al. Resistance exercise and testosterone treatment alters the proportion of numerical density of capillaries of the left ventricle of aging Wistar rats. Aging Male. 2014;17:243–247.
- Mabry RM, Winkler EAH, Reeves MM, et al. Correlates of Omani adults’ physical inactivity and sitting time. Public Health Nutr. 2013;16:65–72.
- Moura BP, Marins JCB, Amorim PRS. Self selected walking speed in overweight adults: is this intensity enough to promote health benefits? Apunts Med Esport. 2011;46:11–15.
- Hayes LD, Sculthorpe N, Herbert P, et al. Resting steroid hormone concentrations in lifetime exercisers and lifetime sedentary males. Aging Male. 2015;18:22–26.
- Goh VH, Hart WG. Association of general and abdominal obesity with age, endocrine and metabolic factors in Asian men. Aging Male. 2016;19:27–33.