
Abstract
Objectives: We investigate the effects of Ojayeonjonghwan (KH-204) in men with late-onset hypogonadism (LOH) symptoms.
Material and methods: Initial PSA, testosterone, lipid profile and questionnaires about LOH-related symptoms were checked. After 8 weeks of the treatment (control or KH-204), questionnaires and serological tests were repeated to evaluate the efficacy of the agent. The changes of variables in each group and the difference between two groups were compared.
Results: A total of 78 men were enrolled, and randomly assigned to the control group (n = 39) or KH-204 group (n = 39). Baseline characteristics of both group are comparable. AMS total score of control and KH-204 group were both improved at 8 weeks (p = .010, <.001), and there was a statistically significant difference between the two groups (favorable in KH-204 group, p = .006). At 8 weeks, total IIEF score of control and KH-204 group were both improved, and there was no statistically significant difference in the degree of improvement between the two groups (p = .303). There was no statistically significant difference of laboratory findings, in intra-group changes and inter-group comparisons.
Conclusions: KH-204 was found to be effective in all LOH symptoms without changing of laboratory results. KH-204 may be safely used for treatment of male with LOH-related symptoms.
Introduction
Population aging, which is a shift in the distribution of population toward older ages due to development of medical technology, has become an important issue in recent years. The aging of the population is widespread across the world, but the rate of aging of Korean is very fast, so that the ratio of elderly people over 65 is now reaching 14%. As life expectancy increases, the quality of life of elderly people as well as geriatric diseases is also an important concern. Especially, the effects of a reduction in sexual function on quality of life and psychological aspects of aging male are serious [Citation1].
The deficiency of serum testosterone in aged men causes various symptoms that reduce the quality of life. The concept of male andropause is originated in 1946 by Werner, who first called ‘Male climacteric’ as a relative concept in women’s menopause [Citation2]. Recently, this concept is named as late-onset hypogonadism (LOH) at the 4th ISSAM meeting in 2004. LOH-related symptoms are known to be closely associated with a decrease in serum testosterone levels. They are characterized as follows: (1) reduced sexual desire, impotency, (2) decreased intellectual activity, cognition, strength, (3) emotional changes involving fatigue, depression, and haste, (4) sleep disturbance, (5) body fat and weight loss associated with decreased muscle mass and strength, (6) increased internal fat, (7) decreased body hair and change of skin, (8) decreased bone density, resulting in osteoporosis and high risk of fractures, (9) increased risk of cardiovascular disease [Citation3–11].
Testosterone is not an essential hormone for maintaining life, but as a major sex hormone in men, it is important for sexual differentiation, masculinity, maintenance of sexual and erectile physiology [Citation12–14]. Testosterone secretion is reduced by about 0.8% per year in men after 30 s [Citation15], and about 30–50% of 50–70 men develop various climacteric symptoms. About 5.6% of aging male between 30 and 79 ages has symptomatic androgen deficiency and increasing feature with aging [Citation16]. According to Massachusetts Male Aging Study (MMAS), LOH is predicted to reach 481,000 new cases each year in USA [Citation17]. In Korea, 64.6% of men between the ages of 40 and 70 LOH-related symptoms.
The treatment of LOH is a androgen replacement therapy (ART) and the testosterone intramuscular injection, patches, and gel preparation are mainly used. However, ART have problems such as induction of testosterone concentration higher than physiological blood level, instability in action time, skin reactions. In addition, ART cannot be performed in patients with cardiovascular disease, prostate cancer, or polycythemia. Several studies have been conducted to overcome the limitations of ART, and clinical study in Japan has reported the improvement of LOH symptom without increasing testosterone after the administration of herbal medicine [Citation18,Citation19]. In our previous study, we performed in vivo test in rat about anti-oxidative effect was identified because oxidative stress is one of the causes of LOH [Citation20]. We used herbal formulation Ojayeonjonghwan, known as KH-204, which protects testis as antioxidants.
The objective of this study is to investigate the effect of KH204 on the improvement of symptoms in men with LOH-related symptoms.
Materials and methods
Ethical approval
Institutional ethics review was sought and approved by Catholic University of Korea, Institutional Review Board (approval number: KC17HESI0109).
Preparation of herbal mixture
KH-204 was consisted of 5 seed of 5 different kinds of berry plants; It included Cornus Officinalis Sieb. Et Zucc, Lycium chinense Mill, Rubus coreanus Migquel, Cuscutachicuscut Lamark, and Schizandra chinensis Baillon. At previous study in rat, effective dose was 400 mg/kg/day, and human equivalent dose (HED) of mixture was confirmed 4.2g/day [total tablet dose 7.92 g (12 tablet)/day] at 60 kg adult weight.
Study design
This study was designed for parallel group, randomized, double-blind, placebo-controlled formation. All subjects agreed to participate in the study after the explanation and had a 4-week wash-out period. Before starting the study, we checked the vital signs, body mass index (BMI), comorbidities, and serum tests such as PSA, testosterone, free testosterone, lipid profile (total cholesterol, triglyceride, HDL, LDL), AST, ALT and creatinine. Aging male symptoms (AMS) questionnaire, androgen deficiency in aging males (ADAM) questionnaire, International Index of Erectile Function (IIEF), International Prostate Symptom Score (IPSS) questionnaire were collected as a subjective assessment of symptoms. All subjects took the tablets 3 times per day (30 min after meal) and continued to take it for 8 weeks. At 4 and 8 weeks after treatment, all subjects were reexamined the questionnaire, laboratory findings and the adverse events.
Inclusion and exclusion criteria
Men over 40 years old who complained of LOH-related symptoms with AMS score of 27 or more was included in this study. Person who had more than 50 points in total AMS scale and serum testosterone level was below 2.31 ng/ml (8 nmol/L) was excluded in this study. And patients who were suspicious prostate cancer and serum PSA level over 4.0 ng/ml also excluded. Severe obese men who had more than BMI >35 kg/m2 were not included in this study. Untreated or uncontrolled comorbidity such as uncontrolled hypertension (SBP ≥140 mmHg or DBP ≥90), type 1 diabetes or diabetes patients who had taken insulin treatment for glucose control, tuberculosis, asthma, glaucoma, multiple sclerosis, major depression with psychotic feature, bipolar disorder, schizophrenia, bulimia, anorexia nervosa, hepatic failure 2.5 times higher than normal limit in AST/ALT, Total bilirubin, alkaline phosphatase level, had a history of chronic hepatitis B infection or hepatitis B virus carrier, medical history of renal failure or with a serum creatinine value more than 2.5 mg/dl or higher, patients who was diagnosed hypothyroidism, Cushing syndrome, or related medication, have taken medicines such as appetite suppressant, oral steroids, thyroid hormone, amphetamines, cyproheptadine, and phenothiazine within three months and epilepsy were also excluded.
Medication which had effect to testosterone level or patients who were taking or had taken hormone replacement therapy within 6 months, person who was taken combined food or medicine (health function food like combination of extracts such as dandelion, maca gelatinized powder, saw palmetto extracts, herbal or oriental medicine whish was affected to male andropause) was also excluded. If subject had hypersensitive reaction against the product, history of cancer within five years, severe obstructive sleep apnea, alcohol abuse or history of drug abuse, history of heart failure, angina, myocardial infarction, cerebrovascular accident and cerebral hemorrhage within recent 6 months, they were also excluded.
Outcome measures
The primary outcome was improvement of LOH-related symptom as assessed using AMS questionnaire 8 weeks after taking medicine. Secondary outcomes were changes from subjective questionnaires (ADAM, IIEF, IPSS) and laboratory findings.
AMS questionnaire contains 17 self-rating symptom-based questions, including 5 psychological (questionnaire 6, 7, 8, 11, 13), 7 somatic (1, 2, 3, 4, 5, 9, 10) and 5 sexual (12, 14, 15, 16, 17) subscales. We used AMS Korean validation. Each question is answered by 5-point scale (1–5) and is analyzed as follows: no symptoms (from 17–26), mild (27–36), moderate (37–49), severe (more than 50).
ADAM questionnaire was consisted of 10 questions. Each question was answered by “Yes” or “No”. If the answer to question 1 or 7 is yes, or if three or more of the other 8 questions are answered to yes, it is estimated to be male andropause.
IIEF questionnaire was consisted of 15 questions about erectile function (1, 2, 3, 4, 5, 15), orgasmic function (9, 10), sexual desire (11, 12), intercourse satisfaction (6, 7, 8), and overall satisfaction (13, 14). Results was assessed as follows: (1) erectile dysfunction subscale, severe (0–6), moderate (7–12), mild to moderate (13–18), mild (19–24), and no dysfunction (25–30); (2) orgasmic dysfunction subscale, severe (0–2), moderate (3–4), mild to moderate (5–6), mild (7–8), and no dysfunction (9–10); (3) sexual desire subscale, severe (0–2), moderate (3–4), mild to moderate (5–6), mild (7–8), and no dysfunction (9–10); (4) intercourse satisfaction subscale, severe (0–3), moderate (4–6), mild to moderate (7–9), mild (10–12), and no dysfunction (13–15); (5) overall satisfaction subscale, severe (0–2), moderate (3–4), mild to moderate (5–6), mild (7–8), and no dysfunction (9–10).
IPSS questionnaire was consisted of 7 questions about urinary symptoms, and one question relating to overall quality of life. The answers about urinary symptoms are assigned points from 0 to 5, the total score can therefore range from 0 to 35. The categorized symptom severity according to the symptom score is as follows: mild (0–7), moderate (8–19), severe (20–35).
Statistical analysis
The paired t-test and Student t-test were performed when the data were in normal distribution, and Wilcoxon's signed-rank test and Wilcoxon's rank sum test were used for non-normal distribution. The p values of less than .05 is considered statistically significant. For statistical analysis, SPSS 18.0 was used.
Results
Patients characteristics
A total of 78 men were enrolled, and randomly assigned to the control group (n = 39) or KH-204 group (n = 39). None of both groups were dropped out (). Mean ages of patients, vital sign, BMI did not differ between two groups. Comorbidity such as diabetes, hypertension and dyslipidemia also showed no significant differences ().
Figure 1. Flow diagram of study participants.
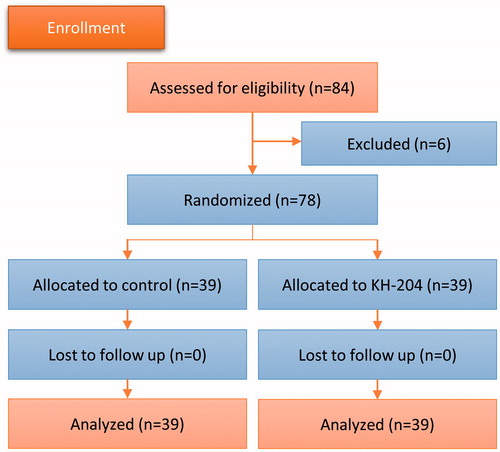
Table 1. Baseline characteristics.
AMS questionnaire
Baseline AMS total score of both groups were comparable. AMS total score of control and KH-204 group were both improved at 4 weeks (p = .027, .003) and 8 weeks (p = .010 vs <.001) (). AMS total score was decreased at 8 weeks compared to baseline (5.67 points in the KH-204 group vs 2.28 points in the control group), and there was a statistically significant difference between the two groups (p = .0061) ().
Figure 2. Results of aging male symptoms (AMS) questionnaire of control group and KH-204 group. *Total AMS score of both group were improved at 4 and 8 weeks. †Total AMS score of KH-204 group was more improved than control group after 8 weeks (p = .006).
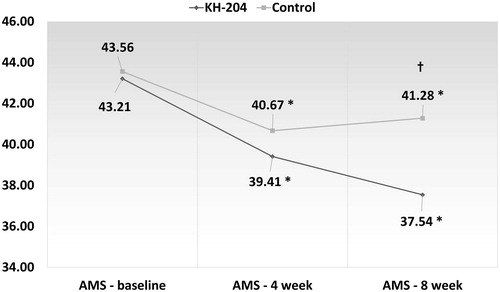
Table 2. Time courses of questionnaire scores related symptoms of aging in males.
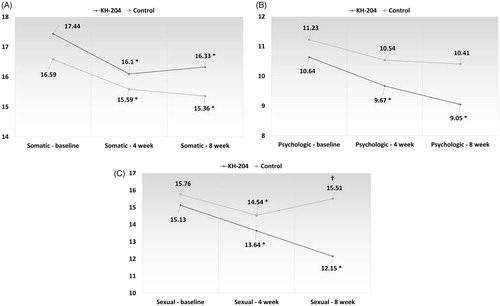
In the comparison of the subscale of the AMS, only the somatic subscale was significantly improved in the placebo group, while all three subscales were significantly improved in the KH-204 group, and the degree of improvement in the sexual subscale was significantly different from the placebo group (p < .001) ().
Figure 3. Subscales of aging male symptoms (AMS) questionnaire. Somatic subscale (A), Psychologic subscale (B), and Sexual subscale (C). *All three subscales were significantly improved in the KH-204 group. †AMS sexual subscale of KH-204 group was more improved than control group after 8 weeks (p < .001).
ADAM questionnaire
The androgen deficiency male, which was classified according to ADAM questionnaire, was 39 patients in both groups. The number of androgen deficiency male in control group was changed to 34 at 4 weeks and 36 at 8 weeks. On the other hand, in the KH-204 group, it decreased to 32 at 4 weeks and 24 at 8 weeks, showing a statistically significant difference from the control group (p = .013).
IIEF questionnaire
Total IIEF score of KH-204 group was improved at 4 weeks (+6.47, p = .004), but not in the control group (+0.87, p = .0175). At 8 weeks, total IIEF score of control (+3.82, p = .025) and KH-204 (+6.21, p = .001) group were both improved, and there was no statistically significant difference in the degree of improvement between the two groups (p = .303).
IPSS questionnaire
At 4 and 8 weeks, the total IPSS score of the KH-204 group was not improved (p = .616, .475), whereas the control group showed a significant improvement (p = .001, .003). But there was no statistically significant difference of total IPSS score change between the two groups at 8 weeks (p = .150).
Testosterone, free testosterone and PSA
The increase in total testosterone was 0.91 ng/mL in the control group and 0.20 ng/mL in the KH-204 group after 8 weeks of treatment, and there was no statistically significant difference between the two groups (p = .142) (). Free testosterone decreased by 0.38 pg/mL in the control group and 1.22 pg/mL in the KH-204 group after treatment, and there was no statistically significant difference between the two groups (p = .215). Serum PSA decreased by 0.03 ng/dL in the control group and increased by 0.01 ng/dL in the KH-204 group, but there was no statistically significant difference between the two groups (0.337).
Table 3. Laboratory values before and after treatment.
Lipid profile (total cholesterol, triglyceride, LDL, HDL)
Total cholesterol, triglyceride, LDL were slightly decreased and HDL was increased in KH-204 group, but there were no statistical significant changes (p = .351, .593, .488, .805). In control group, all lipid profile was increased without statistically significance, and there was no significant difference between control and KH-204 group (p = .422, .932, .360, .959).
Safety profile
Mild adverse events were noted in three participants of KH-204 group (loose stool, common cold, dry eye), but they were recovered without treatment.
Discussions
The efficacy of the five herbal mixtures constituting KH-204 is generally known as follows: Cornus Officinalis Sieb. Et Zucc had effect to bladder overactivity, diabetes and related diabetic nephropathy, neuroprotection, inflammation and erectile dysfunction [Citation21–25]. Lycium chinense Mill. had benefit of hepatoprotection, antihypertensive effect, vision protection. Rubuscoreanus Migquel had anti-inflammatory, anti-oxidant effects and erectile function [Citation26–29]. Cuscutachinensis Lamark was characterized anti-oxidant activities [Citation30,Citation31]. Schizandra chinensis Baillon had beneficial effects for fatigue, diabetes, lipid metabolism, antioxidant [Citation32,Citation33]. Previous animal model studies reported that KH-204 activates the nitric oxide pathway and has a preventive effect on oxidative stress [Citation34–36]. It is well known that antioxidant effect and activation of the nitric oxide pathway plays an important role in erectile dysfunction, which accounts for a large proportion of LOH-related symptoms.
Clinical trial conducted of KH-204 in patients with erectile dysfunction reported that IIEF of KH-204 group improved after treatment (11.13 ± 11.83), showing significantly better than that of placebo group (6.57 ± 11.72) (p < .05). Particularly in patients with severe sexual dysfunction, the improvement in sexual function was better. In terms of safety, there were some patients with headache and nausea but had a lower incidence of adverse events (3 of 43 patients, 7.5%) than PDE-5 inhibitors (43 of 159 patients, 27%) safety was confirmed due to mild symptoms resolved without any treatment [Citation22,Citation37].
In oriental medicine, each herb or seed has its own effects, but when mixed it is known to increase the effect, increase the effect of the others, or inhibit other effects or side effects [Citation38]. In Japan, herbal medications, also called “Kampo medicine”, are widely used in urology clinics and are covered by insurance [Citation19]. In Korea, these herbal medications are not classified as specialty medicines, but they are used for the classification of health functional foods. It is preferable that such health functional foods are effective for improving symptoms such as diseases or syndromes without directly causing significant serological or other clinically significant changes in the human body.
ART is an established treatment for LOH. Testosterone replacement agents include oral, injection, and transdermal agents. Oral agents have a disadvantage in that it is difficult to maintain serum concentrations. Injection and transdermal agents are useful for maintaining testosterone levels in the blood, but they are inconvenient to use. Although the understanding of the relationship between prostate cancer and ART is changing recently, the use of ART in patients at high risk for prostate cancer is still limited [Citation39]. In addition, patients who are treated with ART are still recommended to follow-up serum PSA for monitoring of prostate cancer development.
In this study, KH-204 improved LOH-related symptoms without changing laboratory findings. Serum PSA and testosterone level of KH-204 group did not rise, and side effects that of KH 204 were minimal and recovered without any treatment. Therefore, KH-204 can be considered as an alternative drug in patients with mild LOH-related symptoms who cannot be treated with testosterone due to adverse events such as dyslipidemia, sleep apnea, polycythemia, prostate cancer. Especially, as mentioned above, ART is still controversial in patients who are diagnosed with or at risk for prostate cancer. In this case, KH-204, which does not affect serum testosterone and PSA, may be a good alternative. In addition, KH-204 has the advantage of high patient compliance because of its ease of administration and less side effects, which is supported by the lack of follow-up loss in this study. However, the limit of this study is a short study period of only 8 weeks, and therefore long-term research is needed to demonstrate the long-term effects of the drug.
As a result, in this study using KH-204, the overall LOH-related symptoms were improved, and these results were obtained without any significant changes in PSA or testosterone. Especially, the significant improvement in sexual function of KH-204 may facilitate to alleviate LOH-related symptoms without testosterone changes.
Conclusions
KH-204 was found to be effective in all LOH-related symptoms without changing of laboratory results. KH-204 may be safely used for treatment of aging male with LOH-related symptoms.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Chew KK, Bremner A, Stuckey B, et al. Sex life after 65: how does erectile dysfunction affect ageing and elderly men? Aging Male. 2009;12:41–46.
- Werner AA. The male climacteric. J Am Med Assoc. 1946;132:188–194.
- Schubert M, Jockenhövel F. Late-onset hypogonadism in the aging male (LOH): definition, diagnostic and clinical aspects. J Endocrinol Invest. 2005;28:23–27.
- Wang C, Nieschlag E, Swerdloff R, et al. ISA, ISSAM, EAU, EAA and ASA recommendations: investigation, treatment and monitoring of late-onset hypogonadism in males. Int J Impot Res. 2009;21:1–8.
- Yassin AA, Nettleship JE, Almehmadi Y, et al. Is there a relationship between the severity of erectile dysfunction and the comorbidity profile in men with late onset hypogonadism? Arab J Urol. 2015;13:162–168.
- Almehmadi Y, Yassin DJ, Yassin AA. Erectile dysfunction is a prognostic indicator of comorbidities in men with late onset hypogonadism. Aging Male. 2015;18:186–194.
- Salman M, Yassin DJ, Shoukfeh H, et al. Early weight loss predicts the reduction of obesity in men with erectile dysfunction and hypogonadism undergoing long-term testosterone replacement therapy. Aging Male. 2017;20:45–48.
- Yassin A, Almehmadi Y, Saad F, et al. The Author's Reply: Changing testosterone had no direct effect on HbA1c or weight in diabetic men when TRT was interrupted and then resumed. Clin Endocrinol. 2016;85:500–501.
- Yassin AA, Saad F, Haider A, et al. The role of the urologist in the prevention and early detection of cardiovascular disease. Arab J Urol. 2011;9:57–62.
- Ho CH, Wu CC, Chen KC, et al. Erectile dysfunction, loss of libido and low sexual frequency increase the risk of cardiovascular disease in men with low testosterone. Aging Male. 2016;19:96–101.
- Smith ML, Honore Goltz H, Ahn S, et al. Correlates of chronic disease and patient-provider discussions among middle-aged and older adult males: Implications for successful aging and sexuality. Aging Male. 2012;15:115–123.
- Foresta C, Caretta N, Rossato M, et al. Role of androgens in erectile function. J Urol. 2004;171:2358–2362.
- Yassin A, Nettleship JE, Talib RA, et al. Effects of testosterone replacement therapy withdrawal and re-treatment in hypogonadal elderly men upon obesity, voiding function and prostate safety parameters. Aging Male. 2016;19:64–69.
- Leoni LA, Fukushima AR, Rocha LY, et al. Physical activity on endothelial and erectile dysfunction: a literature review. Aging Male. 2014;17:125–130.
- Feldman HA, Longcope C, Derby CA, et al. Age trends in the level of serum testosterone and other hormones in middle-aged men: longitudinal results from the Massachusetts male aging study. J Clin Endocrinol Metab. 2002;87:589–598.
- Araujo AB, Esche GR, Kupelian V, et al. Prevalence of symptomatic androgen deficiency in men. J Clin Endocrinol Metab. 2007;92:4241–4247.
- O'Donnell AB, Araujo AB, McKinlay JB. The health of normally aging men: The Massachusetts Male Aging Study (1987-2004). Exp Gerontol. 2004;39:975–984.
- Tsujimura A, Takada S, Matsuoka Y, et al. Clinical trial of treatment with saikokaryukotsuboreito for eugonadal patients with late-inset hypogonadism-related symptoms. Aging Male. 2008;11:95–99.
- Amano T, Imao T, Takemae K. Clinical efficacy of Japanese traditional herbal medicine (Kampo) in patients with late-onset hypogonadism. Aging Male. 2010;13:166–173.
- Bae WJ, Zhu GQ, Choi SW, et al. Antioxidant and Antifibrotic Effect of a Herbal Formulation In Vitro and in the Experimental Andropause via Nrf2/HO-1 Signaling Pathway. Oxid Med Cell Longev. 2017;2017:6024839.
- Hsu PC, Tsai YT, Lai JN, et al. Integrating traditional Chinese medicine healthcare into diabetes care by reducing the risk of developing kidney failure among type 2 diabetic patients: a population-based case control study. J Ethnopharmacol. 2014;156:358–364.
- Kam SC, Choi SM, Jeh SU, et al. Efficacy and Safety of a Herbal Formula that Mainly Consists of Cornus Officinalis for Erectile Dysfunction: A Double-blind, Placebo-controlled Study. Korean J Urol. 2007;48:741–747.
- Kang DG, Choi DH, Lee JK, et al. Endothelial NO/cGMP-dependent vascular relaxation of cornuside isolated from the fruit of Cornus officinalis. Planta Med. 2007;73:1436–1440.
- Lee WC, Wu CC, Chuang YC, et al. Ba-Wei-Die-Huang-Wan (Hachimi-jio-gan) can ameliorate cyclophosphamide-induced ongoing bladder overactivity and acidic adenosine triphosphate solution-induced hyperactivity on rats prestimulated bladder. J Ethnopharmacol. 2016;184:1–9.
- Zhao M, Qian D, Shang EX, et al. Comparative pharmacokinetics of the main compounds of Shanzhuyu extract after oral administration in normal and chronic kidney disease rats. J Ethnopharmacol. 2015;173:280–286.
- Jeon JH, Shin S, Park D, et al. Fermentation filtrates of Rubus coreanus relax the corpus cavernosum and increase sperm count and motility. J Med Food. 2008;11:474–478.
- Lee JE, Cho SM, Park E, et al. Anti-inflammatory effects of Rubus coreanus Miquel through inhibition of NF-κB and MAP Kinase. Nutr Res Pract. 2014;8:501–508.
- Lee JH, Chae MR, Sung HH, et al. Endothelium-independent relaxant effect of Rubus coreanus extracts in corpus cavernosum smooth muscle. J Sex Med. 2013;10:1720–1729.
- Zhao C, Kim HK, Kim SZ, et al. What is the role of unripe Rubus coreanus extract on penile erection? Phytother Res. 2011;25:1046–1053.
- Kim J-O, Kim J-B, Kim H-Y. Anti-oxidative activity of the herb mixture prescribed to induce blood glucose level and effect on the differentiation of 3T3-L1 fibroblast. Korean J Food Preserv. 2009;16:115–121.
- Ko SH, Choi SW, Ye SK, et al. Comparison of anti-oxidant activities of seventy herbs that have been used in Korean traditional medicine. Nutr Res Pract. 2008;2:143–151.
- Park JY, Shin HK, Choi YW, et al. Gomisin A induces Ca2+-dependent activation of eNOS in human coronary artery endothelial cells. J Ethnopharmacol. 2009;125:291–296.
- Xia P, Sun LJ, Wang J. [Effects of fructus schisandrae on the function of the pituitary-testis axis and carbohydrate metabolism in rats undergoing experimental navigation and high-intensity exercise]. Zhonghua Nan Ke Xue 2011;17:472–476.
- Jang H, Bae WJ, Kim SJ, et al. The herbal formula KH-204 is protective against erectile dysfunction by minimizing oxidative stress and improving lipid profiles in a rat model of erectile dysfunction induced by hypercholesterolaemia. BMC Complement Altern Med. 2017;17:129.
- Moon HW, Park JW, Lee KW, et al. Administration of Goji (Lycium chinense Mill.) Extracts Improves Erectile Function in Old Aged Rat Model. World J Mens Health. 2017;35:43–50.
- Sohn DW, Kim HY, Kim SD, et al. Elevation of intracavernous pressure and NO-cGMP activity by a new herbal formula in penile tissues of spontaneous hypertensive male rats. J Ethnopharmacol. 2008;120:176–180.
- Meuleman E, Cuzin B, Opsomer RJ, et al. A dose-escalation study to assess the efficacy and safety of sildenafil citrate in men with erectile dysfunction. BJU Int. 2001;87:75–81.
- Minagawa T, Ishizuka O. Status of urological Kampo medicine: a narrative review and future vision. Int J Urol. 2015;22:254–263.
- Bell MA, Campbell JD, Joice G, et al. Shifting the paradigm of testosterone replacement therapy in prostate cancer. World J Mens Health. 2018;36:103–109.