
Abstract
Purpose
It was aimed to evaluate the changes in quality of life in patients with erectile dysfunction (ED) after inflatable penile prosthesis implantation.
Material and Methods
Forty-one patients who underwent to an inflatable penile prosthesis implantation surgery due to ED were included in the study. The age of the patients, the indications for surgery, and the type of prosthesis implanted were recorded. All patients were implanted two-piece inflatable (AMS Ambicor™) or three-piece inflatable (AMS 700™) prostheses. A 36-item short form (SF-36) was used to assess the life quality of patients. The scores obtained from these forms were recorded and used to compare the preoperative and postoperative quality of life of the patients.
Results
The mean age of the patients was 59.9 (38–78) years. The mean follow-up was 25.1 (12–39) months. A three-piece inflatable penile prosthesis was implanted in 11 (26.8%) of the 41 patients and the others were implanted with a two-piece inflatable penile prosthesis. Average SF-36 scores were increased significantly after surgery in all groups.
Conclusions
Inflatable penile prosthesis implantation is one of the most satisfactory treatment methods of ED and our study shows that with this treatment the patients can be provided a significant improvement in life quality.
Introduction
Erectile dysfunction (ED) is defined as "the continuation of insufficient penile erection to provide or maintain a satisfactory sexual relationship" [Citation1]. ED not only affects both the patient and the partner sexually but also reduces the quality of life. It is the most common sexual dysfunction in men. It is highly related to age. This disease is seen in 2–28.9% of males between 30 and 39 years old and 41.9–83% in males between 70 and 80 years old [Citation2]. ED can occur due to vascular disease, neurological disease, hormonal insufficiency or diseases that lead to cavernosal fibrosis such as Peyronie's disease, ischemic priapism or diabetes mellitus (DM) [Citation3].
ED is a disease that significantly disturbs one's quality of life. People with impaired sexual function tend to be depressed in their daily lives, have poor social relationships, and are low self-esteem. On the other hand, those who experience negative social life, also experience inefficiency in their business life and a socioeconomically negative picture emerges. All of these situations lead to one's psychological problems. In psychologically damaged individuals, ED increases and thus a vicious cycle occurs. Effective treatment of ED is very important in terms of breaking this loop [Citation4].
Currently, phosphodiesterase 5 inhibitors, intracavernosal injections, vacuum erection devices, and intraurethral alprostadil preparations are used in ED treatment. Surgical treatment is usually used in patients who cannot respond to these treatment methods or in patients who do not prefer one of these treatment methods for any reason [Citation5]. Inflatable penile prostheses are frequently used in surgical treatment. These prostheses provide better sexual function and higher patient satisfaction than other treatment methods [Citation6].
In this study, it was aimed to measure the quality of life, before and after the implantation of two and three pieces penile prosthesis and to investigate the difference between these levels among ED patients. The presence of any clinical parameters affecting the quality of life scores before and after implantation will also be investigated in this study.
Material and methods
Fifty-nine patients who underwent penile prosthesis implantation in Eskisehir Osmangazi University Faculty of Medicine Urology Department due to severe ED in the past 5 years, were evaluated. Forty-one patients who completed a 1-year follow-up and who underwent an inflatable penile prosthesis were included in the study. During the 1-year follow-up period, experiencing an important event that could lead to significant changes in quality of life (serious new disease, trauma, occupational change, change in familial status, etc.) was accepted as a criterion for exclusion. The age of the patients included in the study, the indications for surgery, and the type of prosthesis implanted were recorded. All patients were implanted two-piece inflatable (AMS Ambicor™) or three-piece inflatable (AMS 700™) prostheses. All surgeries were performed by one surgeon in the same center.
An informed consent form was obtained from all patients before operation, including information about the operation and possible complications. In addition, all patients included in the study have signed proclamation forms containing information about the study. The study was approved by the ethics committee of Osmangazi University.
A 36-item short form (SF-36) was used to assess the life quality of patients. It was constructed to survey health status in the Medical Outcomes Study [Citation7]. The SF-36 was designed for use in clinical practice and research, health policy evaluations, and general population surveys. The SF-36 includes one multi-item scale that assesses eight health concepts: (1) limitations in physical activities because of health problems (PF), (2) limitations in social activities because of physical or emotional problems (SF), (3) limitations in usual role activities because of physical health problems (RP), (4) bodily pain (BP), (5) general mental health (psychological distress and well-being) (MH), (6) limitations in usual role activities because of emotional problems (RE), (7) vitality (energy and fatigue) (VT), and (8) general health perceptions (GH). Items 1, 3, 4, and 8 are evaluated together to form a general physical score (PHY) and other items form a psychosocial (SOC) score. All patients completed the Turkish validated version of the SF-36 form prior to surgery and 1 year after surgery to assess their quality of life [Citation8]. The scores obtained from these forms were recorded and used to compare the preoperative and postoperative quality of life of the patients.
IBM SPSS v25.0 program was used for statistical analysis. Dependent variables t-test and Wilcoxon signed rank test were used to analyze the change of SF-36 scores before and after surgery. The Mann–Whitney U test was used to assess the difference between the groups in the mean of pre-op and post-op quality of life scores. p values less than .05 were considered statistically significant.
Results
The mean age of the patients was 59.9 (38–78) years. The mean follow-up was 25.1 (12–39) months. A three-piece inflatable penile prosthesis was implanted in 11 (26.8%) of the 41 patients and 30 (73.2%) patients were implanted with a two-piece inflatable penile prosthesis. There was no significant difference in mean age between patients with two and three-piece inflatable prosthesis implantation (p = .469). When the patients were grouped according to the type of prosthesis placed, there was no difference between the preoperative and postoperative SF-36 average scores.
Diabetes mellitus was found among the etiologic agents of ED in 21 (51.2%) of 41 patients, and DM was absent in 20 (48.8%) patients. When patients were grouped according to whether they have DM or not, it was found that pre-operative quality of life scores were statistically lower in all SF-36 parameters except VT in patients with DM. Likewise, postoperative quality of life scores were found to be lower for patients with DM except for VT.
Of all patients undergoing penile prosthesis implantation, 28 (68.3%) were found to have cardiovascular disease and 13 (31.7%) were not. When patients were grouped according to whether they had cardiovascular disease or not, there was no statistically significant difference between preoperative and postoperative mean quality of life scores between these groups.
History of radical pelvic surgery (RPS) (radical prostatectomy, radical cystectomy, colectomy, etc.) was positive in 16 of 41 (39%) patients and 25 of them (61%) had no such history. When the patients were grouped according to the history of RPS; RP, GH, PHY, and SOC were found to be statistically higher in pre-operative SF-36 parameters in RPS positive patients. PF, RE, GH, PHY, and SOC scores were higher in the same patient group after the operation as well.
The preoperative mean SF-36 scores of the patients were summarized in , and the postoperative scores were summarized in .
Table 1. Preoperative mean SF-36 scores of patients classified with penile prosthesis type and etiology (mean ± SD).
Table 2. Postoperative mean SF-36 scores of patients classified with penile prosthesis type and etiology (mean ± SD).
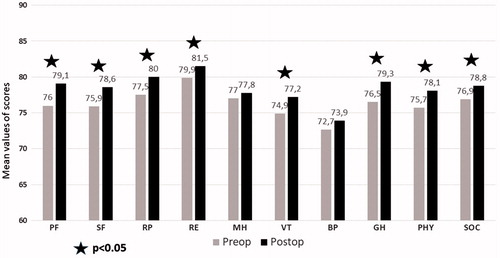
When all patients were evaluated together, postoperative average scores of SF-36 were found to be significantly higher than preoperative average scores (). When diabetic patients were analyzed, it was observed that all the parameters increased after the operation. All of these increases were statistically significant except MH and VT (). Patients with any cardiovascular disease show a significant increase in all post-operative parameters (). Patients with the history of RPS showed a significant increase in all post-operative parameters except BP (). When the patients are classified according to the type of prosthesis applied; all SF-36 parameters increased significantly after surgery in two-piece prosthesis implantation group, whereas all parameters except BP, increased significantly after operation in three-piece prosthesis implantation group ( and ).
Figure 1. Mean values of life quality scores before and after implantation among all patients.
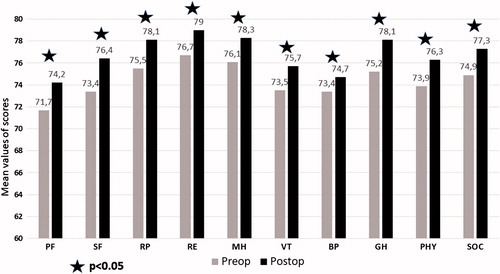
Figure 2. Mean values of life quality scores before and after implantation among diabetic patients.
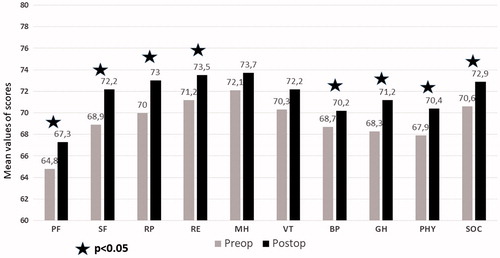
Figure 3. Mean values of life quality scores before and after implantation among patients with cardiovascular disease.
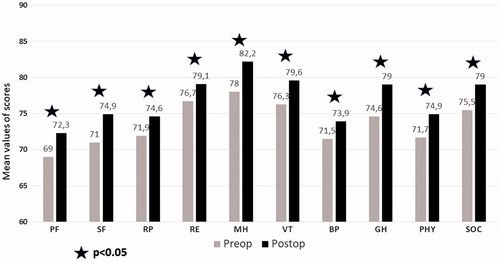
Figure 4. Mean values of life quality scores before and after implantation among patients with history of radical pelvic surgery.
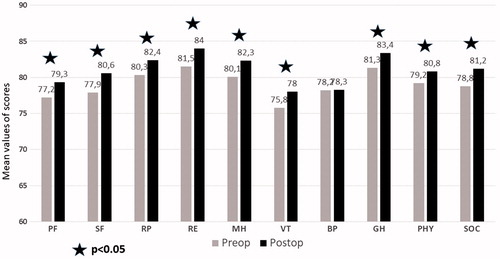
Figure 5. Mean values of life quality scores before and after implantation among patients who were implanted two-piece penile prosthesis.
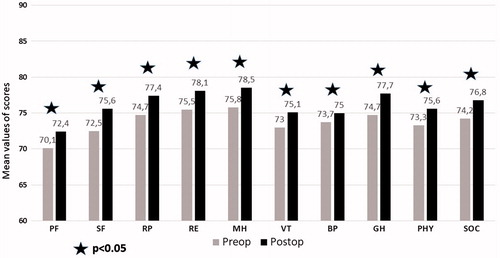
Figure 6. Mean values of life quality scores before and after implantation among patients who were implanted three-piece penile prosthesis.
Discussion
Erected penis has been accepted as a symbol of manhood and sexual power for ages. Men with erectile dysfunction are not only sexually but also psychologically and socially dissatisfied. For this reason, proper treatment of erectile dysfunction will both contribute positively to the sexual life of the man and his partner as well as to the psychosocial aspect. Several studies have shown that erectile dysfunction affects the quality of life negatively even without a comorbid disease [Citation4,Citation9,Citation10]. Especially in elderly patients, if late onset hypogonadism is present, quality of life should be increased by administering testosterone treatment if necessary [Citation11]. In our study, it was investigated the quality of life changes after ED treatment with penile prosthesis implantation. Findings suggest that penile prosthesis treatment significantly improves the quality of life in ED patients. In a recent study, post-implantation quality of life and treatment satisfaction levels of patients who underwent a penile implantation after radical prostatectomy were measured [Citation12]. In this study, 94% of the patients were found to have high satisfaction rates and high quality of life values after treatment. In this study, the authors used scales such as Expanded Prostate Cancer Index Composite Short Form (EPIC-26), Erectile Dysfunction Inventory of Treatment Satisfaction (EDITS), Prostate Cancer-Related Quality of Life Scale, and Self-Esteem and Relationship Questionnaire (SEAR). In our study, the SF-36 questionnaire was used which was completely independent of a specific disease or treatment method. The study by Afsharnia et al. [Citation13] is an example of the use of the SF-36 questionnaire in the area of male sexual health. In our knowledge, there are very few studies using SF-36 to measure the quality of life in ED patients. The most comprehensive of these is the study on 2476 Spanish patients who have ED [Citation14]. In this study, it was emphasized and demonstrated that erectile function significantly affects the male quality of life.
In another study in which SF-36 was used, Mondaini et al. [Citation15] measured the postoperative quality of life of patients who underwent laparoscopic radical prostatectomy and simultaneous penile prosthesis implantation and found that the median quality of life score was increased from the value of 97–99 after operation. The findings of this study support the findings of our study. However, the average scores of quality of life are very high in this study when compared to ours. The reason for this may be that the number of patients in Mondaini's study is only 10. The average scores of SF-36 which were obtained in our study are similar to those in the study which was conducted by Demiral et al. [Citation16], which shows the norm values of SF-36 for Turkish society.
DM is one of the most important risk factors for ED. Both the disease itself and its complications affect the quality of life [Citation17,Citation18]. At the same time, DM is one of the most important factors increasing the infection which is the most important complication of penile prosthesis implantation. In a recent study, HbA1c, dyslipidemia, hypertension, Peyronie’s Disease and duration of the procedure were found to be the predictives of infection [Citation19]. The high level of HbA1c is the most important finding, indicating that DM regulation is impaired. It has been shown that people with HbA1c levels of 8.5% or higher increase the risk of infection [Citation20]. Nevertheless, there are studies in the literature showing no relation between HbA1c and prosthetic infection [Citation21]. In a study of 253 patients, Malavige et al. [Citation10] showed that the presence of erectile dysfunction in diabetic patients is a significant factor in reducing quality of life. In this regard, in a study conducted in 2011 by Avasthi et al. who compared ED patients with non-ED patients and patients with ED showed lower quality of life scores [Citation9]. In our study, the average quality of life of patients with diabetes before penile prosthesis implantation was found to be lower than those without diabetes in terms of most of the parameters. After the implantation of the penile prosthesis, the average quality of life scores in diabetic patients are significantly increased, especially in physical parameters, but the mean values of diabetic patients are still lower than those of non-diabetic patients. These findings show how DM affects the quality of life and how ED treatment can increase the quality of life. Another group of diseases that can make erectile dysfunction so severe that penile prosthesis implantation becomes necessary, is cardiovascular diseases [Citation2]. However, in our study, there was no difference in the quality of life among people with cardiovascular diseases when compared to those without cardiovascular disease. In view of this finding, it can be said that cardiovascular diseases in ED patients do not impair the quality of life as much as DM.
To the best of our knowledge, there are two studies in the literature that analyze patient satisfaction after two-piece penile prosthesis implantation [Citation22,Citation23]. Both studies show a high satisfaction rate in patients after two-piece penile prosthesis implantation. However, our study does not measure patient satisfaction but measures quality of life differently from these studies. In this respect, it can be said that this is the first research in the literature. According to the results of our study, after the implantation of the two-piece penile prosthesis, there was a significant increase in the quality of life of the patients both physically and psychosocial. After implantation of a three-piece penile prosthesis, a significant increase was observed especially in physical parameters. These findings are similar to findings we have in diabetic patients. This may be due to the fact that most of the diabetic patients prefer three-piece prosthesis.
As a conclusion, erectile dysfunction is a disease that disrupts the quality of life of people by all means. If ED derives from a co-morbidity like DM, the quality of life deteriorates worse. Implantation of penile prosthesis, which is one of the most effective treatment methods of ED, may be an important step to improve the quality of life that is deteriorated in all patient groups.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Song W-D, Yuan Y-M, Cui W-S, et al. Penile prosthesis implantation in Chinese patients with severe erectile dysfunction: 10-year experience. Asian J Androl. 2013;15:658–661.
- Antonini G, Busetto GM, De Berardinis E, et al. Minimally invasive infrapubic inflatable penile prosthesis implant for erectile dysfunction: evaluation of efficacy, satisfaction profile and complications. Int J Impot Res. 2016;28:4–8.
- Liu D-F, Jiang H, Hong K, et al. [Epidemiological changes of ED patients: investigations in 11 Chinese cities during the past 5 years]. Zhonghua Nan Ke Xue 2009;15:724–726.
- Idung AU, Abasiubong F, Udoh SB, et al. Quality of life in patients with erectile dysfunction in the Niger Delta region, Nigeria. J Ment Health. 2012;21:236–243.
- Pozza D, Pozza M, Musy M, et al. 500 penile prostheses implanted by a surgeon in Italy in the last 30 years. Arch Ital Urol Androl. 2015;87:216–221.
- Minervini A, Ralph DJ, Pryor JP. Outcome of penile prosthesis implantation for treating erectile dysfunction: experience with 504 procedures. BJU Int. 2006;97:129–133.
- Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30:473–483.
- Kocyigit H, Aydemir O, Fisek G, et al. Validity and reliability of Turkish version of Short form 36: a study of a patients with romatoid disorder. Drug Therapy. 2018;2:102–106.
- Avasthi A, Grover S, Bhansali A, et al. Erectile dysfunction in diabetes mellitus contributes to poor quality of life. Int Rev Psychiatry. 2011;23:93–99.
- Malavige LS, Jayaratne SD, Kathriarachchi ST, et al. Erectile dysfunction is a strong predictor of poor quality of life in men with Type 2 diabetes mellitus. Diabet Med. 2014;31:699–706.
- Meuleman EJH, Legros J-J, Bouloux PMG, et al. Effects of long-term oral testosterone undecanoate therapy on urinary symptoms: data from a 1-year, placebo-controlled, dose-ranging trial in aging men with symptomatic hypogonadism. Aging Male. 2015;18:157–163.
- Pillay B, Moon D, Love C, et al. Quality of life, psychological functioning, and treatment satisfaction of men who have undergone penile prosthesis surgery following robot-assisted radical prostatectomy. J Sex Med. 2017;14:1612–1620.
- Afsharnia E, Pakgohar M, Khosravi S, et al. Examining the effect of the computer-based educational package on quality of life and severity of hypogonadism symptoms in males. Aging Male. 2018;21:85–92.
- Sánchez-Cruz JJ, Cabrera-León A, Martín-Morales A, et al. Male erectile dysfunction and health-related quality of life. Eur Urol. 2003;44:245–253.
- Mondaini N, Cai T, Sarti E, et al. A case series of patients who underwent laparoscopic extraperitoneal radical prostatectomy with the simultaneous implant of a penile prosthesis: focus on penile length preservation. World J Mens Health 2018;36:132–138.
- Demiral Y, Ergor G, Unal B, et al. Normative data and discriminative properties of short form 36 (SF-36) in Turkish urban population. BMC Public Health. 2006;6:247.
- Walders-Abramson N. Depression and quality of life in youth-onset type 2 diabetes mellitus. Curr Diab Rep. 2014;14:449.
- Ionova TI, Odin VI, Nikitina TP, et al. Quality of life and hypoglycemia burden in patients with type 2 diabetes mellitus on basal-bolus insulin therapy. Klin Med (Mosk). 2014;92:52–59.
- Madbouly K, AlHajeri D, Habous M, et al. Association of the modified frailty index with adverse outcomes after penile prosthesis implantation. Aging Male. 2017;20:119–124.
- Habous M, Tal R, Tealab A, et al. Defining a glycated haemoglobin (HbA1c) level that predicts increased risk of penile implant infection. BJU Int. 2018;121:293–300.
- Canguven O, Talib R, El Ansari W, et al. Is Hba1c level of diabetic patients associated with penile prosthesis implantation infections? Aging Male. 2018;1–6. DOI:10.1080/13685538.2018.1448059
- Gentile G, Franceschelli A, Massenio P, et al. Patient’s satisfaction after 2-piece inflatable penile prosthesis implantation: an Italian multicentric study. Arch Ital Urol Androl. 2016;88:1–3.
- Lux M, Reyes-Vallejo L, Morgentaler A, et al. Outcomes and satisfaction rates for the redesigned 2-piece penile prosthesis. J. Urol. 2007;177:262–266.