
Abstract
Objectives
The negative impact of lower urinary tract symptoms (LUTS) on affected males is substantial. This study aims to assess whether a combined auriculotherapy (AT) using laser AT (LAT) and magneto-AT (MAT) is more effective than using MAT alone or placebo for managing LUTS of aging males.Methods: A randomized controlled, double-blinded trial was conducted. Sixty-two aging males with moderate or severe LUTS symptoms were randomly allocated into groups: Group 1, placebo LAT plus placebo MAT (n = 20); Group 2, combined AT approach using LAT plus MAT (n = 20); and Group 3, placebo LAT followed by MAT (n = 22). Six ear acupoints assumed to be suitable for alleviating LUTS were used. The total treatment period was 4 weeks, with follow-up visits till 3 months. Generalized estimating equations model was used for the examination of the interactions among the groups over time.Results: A combined AT approach exhibited a stronger treatment effect in relieving voiding problems, improving the peak urinary flow rate, and reducing the post-void residual urine than the placebo group or MAT alone.Conclusions: This study demonstrates that the AT protocol used in this study for aging males with LUTS is feasible and can be adopted in future study of increased scale.
Introduction
Lower urinary tract symptoms (LUTS) frequently occur among the elderly male population and are principally caused by benign prostatic hyperplasia (BPH) of the prostate gland [Citation1,Citation2]. The prevalence of moderate-to-severe LUTS among aging males is high and ranges from 22% in 50–59-year-old males to 45% in 70-year-old males and older [Citation1]. LUTS mainly comprise a complex symptom cluster of problems associated with storage (filling problem), voiding, and post-micturition. The characteristics of storage are shown by frequency, urgency, nocturia, and incontinence. Voiding symptoms include factors, such as slow stream, splitting or spraying, intermittency, hesitancy, straining, and terminal dribble. The dribble after micturition and the feeling of incomplete emptying are the symptoms of post-micturition [Citation3].
The impact of LUTS on affected males is substantial and includes a low quality of life, high risk of depression, sleep problems, sexual dysfunction [Citation4–7], and hypogonadism [Citation8]. A recent epidemiology study reported that patients with LUTS may be prone to the development of erectile dysfunction [Citation9]. The treatment modalities for LUTS include observation, pharmacotherapies, minimally invasive therapies, and surgical interventions [Citation10–11]. Alpha-adrenergic blockers, 5-alpha-reductase inhibitors [Citation11–14], selective receptor antagonists [Citation15], and phosphodiesterase type 5 inhibitor [Citation16–18] are commonly used as LUTS pharmacotherapies. Despite the proven effectiveness of these treatments, many elderly men are reluctant to consider their use because of perceived side effects and potential complications [Citation1,Citation13,Citation19]. Prolonged consumption of medication for LUTS leads to numerous adverse effects, such as erectile dysfunction, dizziness, postural hypotension, asthenia, decreased libido [Citation13–14], and abnormal ejaculation [Citation16].
Auriculotherapy (AT) is a therapeutic method of traditional Chinese medicine (TCM), by which specific points on the auricle are stimulated for the management of bodily symptoms [Citation20]. The ear has been widely recognized as a microsystem of the body [Citation21]. Different materials, such as acupuncture needles, press-tack needles, seeds, magnetic pellets, or low-energy laser, are applied on acupoints located on the external ear for therapeutic effect [Citation20–23].
In China, the therapeutic effect of auricular acupuncture on LUTS has been well documented in several clinical studies. Huang and Chen [Citation24] utilized electro-auricular acupuncture on 12 patients and found that the method is effective in managing LUTS symptoms in all the recruited cases. Zhang [Citation25] adopted auricular acupuncture to treat 14 patients with BPH and observed that 93% (n = 13) of the patients either were cured or showed ameliorated LUTS. Tang [Citation26] compared the therapeutic effects of auricular acupuncture, infrared ray therapy, and their composite on three groups of patients with BPH-attributed LUTS and found that the therapies are effective in 83.3%, 76.7%, and 100% of the patients being tested, respectively, of the patients. However, although the therapeutic effects of auricular acupuncture on patients with LUTS are promising as shown in these studies, the use of needles may result in patient discomfort, infection, and inflammation in the puncture sites [Citation27].
The positive effect of magneto-AT (MAT) has been demonstrated in several randomized controlled trials conducted by the research team [Citation28–31]. In contrast, laser AT (LAT) provides a simple, noninvasive, and painless treatment approach that presents no risk of infection [Citation32–33]. Thus, the therapeutic value and synergistic effect of LAT when combined with MAT for managing LUTS problems merit further investigation. Many studies that used AT for LUTS in China have methodological flaws that have rendered the findings unconvincing. Common problems in these studies include the lack of details on how randomization and allocation concealment were conducted, the absence of objective measurements, the absence of a control or placebo group, the failure to report the use of blinding, and the dropout of cases during the research process [Citation34–36]. This study was performed using a scientific approach to assess whether a combined AT approach using LAT plus MAT is more effective than using MAT alone or placebo for managing the LUTS of aging males.
Methods
This study is a randomized controlled and double-blinded trial. Eligible participants were randomly allocated to one of the three groups described below. A computer-generated randomized table was adopted. Blocked randomization in accordance with the equal proportion rule (1:1:1) was used, and random coding was concealed from the participants and the evaluator by using opaque envelopes. Participation in the study was voluntary, and written informed consent was obtained from each participant upon their understanding of the risks and benefits of participating in the study.
Settings and participants
Participants were recruited from the elderly centers in Hong Kong by convenience sampling. The inclusion criteria were as follows: (1) men aged 60 years old or above, (2) with LUTS for at least 2 months, (3) with an International Prostate Symptom Score (IPSS) of ≥12 (i.e. having moderate-to-severe LUTS symptoms), and (4) having a maximum urinary flow rate (Qmax) ranging from 5 ml/s to 15 ml/s. The exclusion criteria were as follows: (1) patients who previously underwent or anticipated to receive minimally invasive therapies or surgical intervention of the genito-urinary tract within 6 months, (2) suffered from a psychiatric illness, (3) have prostate cancer history, (4) have renal failure, (5) unable to understand instructions or give consent, and (6) were suffering from aural injuries or infections.
Intervention
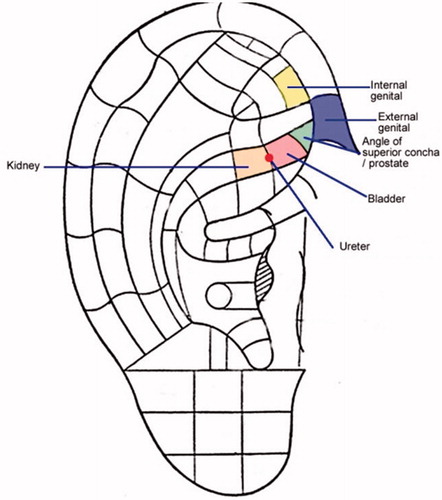
Six ear acupoints () assumed to be suitable for alleviating LUTS were selected. These acupoints included the “angle of the superior concha (prostate),” “kidney,” “bladder,” “ureter,” “external genitals,” and “internal genitals” [Citation37]. The nomenclature and locations of the auricular points published by the China Standardization Organizing Committee (GB/T 13734–2008) [Citation38] were used for locating the acupoints. The therapy was delivered by the research personnel (SY) who had received intensive coaching by the first author (LS). The fidelity of the study was ensured by establishing the inter-rater reliability and accuracy of the ear point identification scheme used.
Figure 1. Selected ear acupoints for lower urinary tract symptoms.
Groupings
Group 1 (Placebo LAT and placebo MAT): Participants received the placebo LAT at “power off” mode (i.e. deactivated laser) for acupoint “stimulation” before the application of plasters centered with a small portion of Junci Medulla (placebo MAT). Junci Medulla is the dried stem of the perennial plant that is soft in texture. This plant material has been successfully adopted as placebo in a previous study because of not inducing any physical pressure on the acupoints of the ear [Citation20].
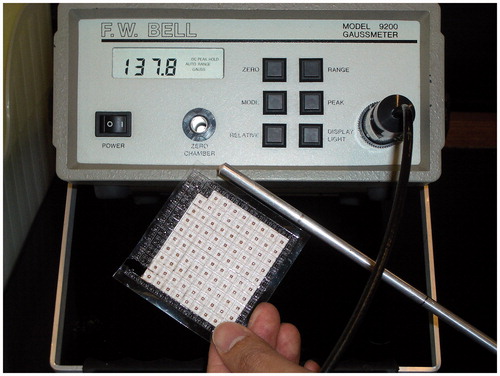
Group 2 (Combined AT): Participants received a combined approach of LAT and MAT. A laser device (Pointer Pulse™) with a wavelength of 650 nm, an average output power of 2.5 mW, an energy density of 1 min with 0.54 J/cm2, and a pulse of 10 Hz was used [Citation39]. This application is a low-energy laser therapy [Citation40–41], in which the energy level emitted from the device is approximately comparable to a teaching pointer. A 1 min treatment using the continuous mode of the device was directly applied to the six ear acupoints detected by an acupoint finder. Laser protective goggles were provided to the participants and the researchers for eye protection (). Thereafter, MAT was applied to the acupoints. Each magnetic pellet has an average gauss/pellet magnetic flux density of ∼130 Gs (13 mT) and a diameter of 1.76 mm ().
Figure 2. Administration of laser auriculotherapy.
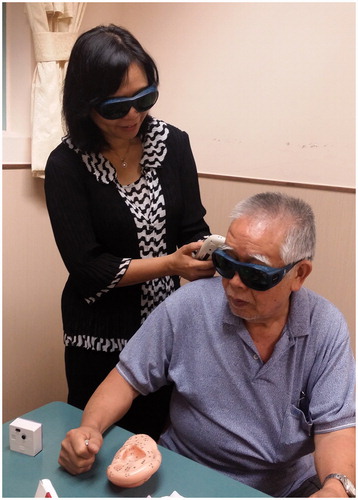
Figure 3. Magnetic flux density of pellets for auriculotherapy.
Group 3 (Placebo LAT and true MAT): To achieve a blinding and placebo effect of the participant, the laser device was switched to “power off” mode (i.e. deactivated laser) for the “stimulation” of six acupoints. The participants were asked to wear a pair of laser protective goggles to “blind” them during treatment. Thereafter, MAT was applied to the acupoints identical to the procedure described in Group 2.
The following procedures were standardized across the three groups for the enhancement of the blinding effect. The auricle of a participant was cleaned with 75% isopropyl alcohol before therapy administration. As a usual practice, only one ear received treatment at a time. Treatment was applied to the right ear in the first visit, followed by the left ear in the subsequent visit, and so on. We replaced the experimental objects (i.e. magnetic pellets for true MAT or Junci Medulla for placebo MAT) every other day, that is, three times a week (except Sunday) to prevent the local irritation of the auricular points. The total treatment period was 4 weeks.
Treatment effect evaluation
Participants were assessed at baseline, 4 weeks (course completion), and during follow-up meetings after 1 and 3 months. The effect of evaluator blinding was achieved by having another researcher, who was unaware of the treatment modality received by the participants, to evaluate the effect. The IPSS–Hong Kong Chinese Version 2 which was used to measure urinary symptoms was considered for the assessment of the primary outcome of the study. This instrument consists of seven Likert-scale questions (scores from 0 [not at all] to 5 [almost always]) that addresses two aspects of LUTS. Three questions involve filling problems (frequency, urgency, and nocturia), and four questions assess voiding problems (emptying, intermittency, weak stream, and straining). The total IPSS from the seven questions ranges from 0 to 35, and the higher score is, the more severe the urinary symptoms are. This version has been certified to be a valid, reliable, and sensitive measure for assessing Chinese populations with LUTS (Cronbach’s alpha coefficient = 0.71, intraclass correlation coefficient of the symptom questions = 0.80) [Citation42].
The secondary outcomes included (1) Quality of life associated with urinary symptoms: this aspect is an additional question of the IPSS scale. It evaluates the feelings of the participants regarding the possibility that they would spend the rest of their lives suffering from their current urinary conditions. The scale ranged from 0 (delighted) to 6 (terrible) [Citation42]. (2) Maximum urinary flow rate (Qmax): the participant was asked to urinate into a special funnel connected to a portable uroflowmeter, which measured the maximum urinary flow rate (mL per second), to assess the severity of urinary obstruction. (3) Post-void residual urine (in mL): this parameter was measured using a portable bladder scanner (BVI-9400) placed on the suprapubic region of each participant. (4) Sleep patterns: the sleeping patterns of the participants were examined with the Pittsburgh sleep quality index (PSQI, Chinese version). The total PSQI score ranges from 0 to 21, and a PSQI score greater than 5 indicates poor sleep quality. Chong and Cheung (2012) validated the Cantonese PSQI and reported a high internal consistency of 0.75 [Citation43]. The participants’ expectations and satisfaction toward the therapy were evaluated using a 10-point scale, with higher scores corresponding to higher expectations/satisfaction towards the therapy [Citation44].
Socio-demographic characteristics, including age, body mass index, marital status, educational level, and smoking and alcohol consumption, co-morbid illnesses, duration of LUTS, and current medications, were obtained. The recruitment rate, compliance rate of the treatment protocol, and the adverse effects arising from the therapy were also monitored.
Data analyses
Descriptive statistics for socio-demographic and clinical characteristics of the participants were presented. The estimated mean and standard error of the outcome variables of each timepoint were computed. The association between categorical variables was examined using χ2 test or Fisher’s exact test. The Kruskal–Wallis test was used for detecting group differences.
Primary analysis was conducted using the Generalized Estimating Equations (GEE) model with an auto-regression correlation structure for the examination of the interactions among the groups over time (baseline to 3-month follow-up) on the primary outcome (i.e. IPSS score) and secondary outcomes (quality of life, Qmax [mL/s], post-void residual urine [mL], and PSQI). Missing data were addressed using the GEE model and assumed to be missed at random [Citation45]. Apart from conducting analyses on all participants, we repeated the main analysis on the completers who had fully accomplished the treatment protocol and all the follow-up time-point measurements (up to 3-month follow-up) for sensitivity analysis. We used the SPSS version 25.0 (IBM Corporation, USA) for all the statistical analyses. All statistical tests were two sided, with the significance level set to 0.05.
Results
The data were collected from January 2015 to January 2017, with a recruitment rate of 78.0%. Sixty-two eligible participants were randomly divided into three groups (Group 1 = 20, Group 2 = 20, Group 3 = 22).
Participants’ characteristics
The recruited participants had an average age of 76.42 years (SD 6.66), with a mean duration of LUTS for 5.37 years (SD 4.91). Over two-thirds of these participants had not received regular follow-ups nor taken any medication for managing LUTS. The groups were essentially comparable and well balanced in their socio-demographic variables, including age, body mass index, education level, marital status, comorbid illnesses, smoking status, and alcohol consumption ().
Table 1. Socio-demographic and clinical characteristics of the participants (n = 62).
Compliance, expectation, and satisfaction toward treatment
The compliance to the intervention protocol was high, with an average of 94.0% (n = 58) completed the 4-week intervention and all follow-up measurements (including post-assessment and 1- and 3-month follow-ups). The flow diagram of the participant of this trial is illustrated in . Although nearly 90% of the participants had not tried complementary and alternative treatment for LUTS, they generally exhibited a strong faith in this treatment approach (7.18 out of 10) and has a relatively high expectation toward the treatment received (7.06 out of 10) before the trial. After the intervention, the participants in Group 2 had the highest satisfaction toward the therapy (7.70), followed by Group 3 (6.65) and Group 1 (6.05). Over half of the participants (n = 33%, 53.2%) indicated that they would definitely recommend this therapy to others (). No specific adverse effects arising from the therapy were observed, except that five cases (8.0%) reported having mild skin irritation on the ears due to the adhesive tapes used for holding the experimental objects in place.
Figure 4. Flow chart of participants in the trial.
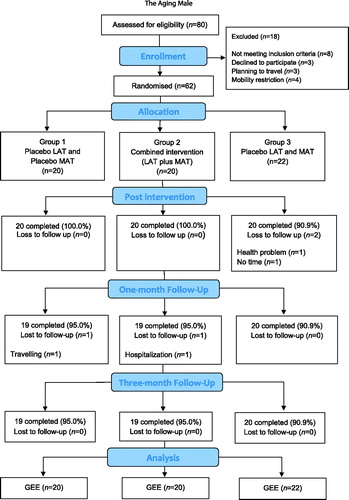
Table 2. Expectations and satisfaction towards the therapy.
Treatment effect
The differences in the IPSS scores of the three groups across different timepoints were compared through GEE model analysis (). Significant reductions in the IPSS scores on urinary symptoms (), especially in those related to the voiding problem (), were noted in the participants of Group 2 relative to those used in Group 1 (p < .01) and Group 3 (p < .05) after the intervention and at the 1-month follow-up. Objective measurements indicated that Qmax gradually increased in Group 2 relative to that in Group 1, with a significant difference at the 3-month follow-up (). A significant reduction in post-void residual urine (mL) was observed in the participants of Groups 2 and 3 relative to those in Group 1 after the therapy and at certain follow-up periods (). No significant change was observed in the quality of life and sleep conditions of the participants among groups. A completers’ analysis showed consistent findings on the primary and secondary outcomes of the trial.
Figure 5. IPSS (Total, 0–35) across time.
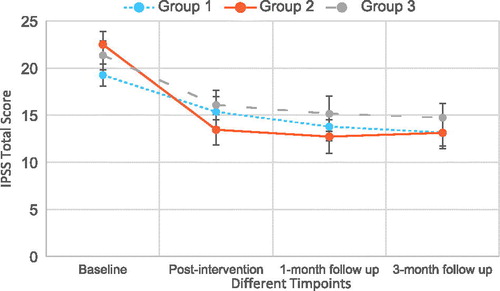
Figure 6. IPSS (Voiding problem, 0–20) across time.
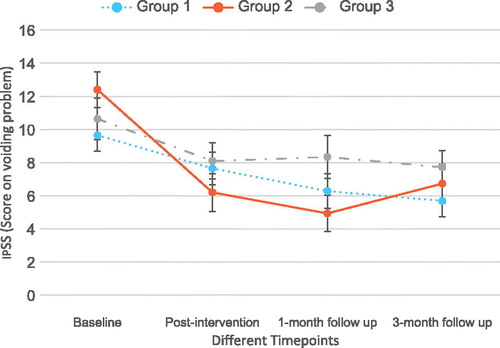
Figure 7. Qmax (mL/sec) across time.
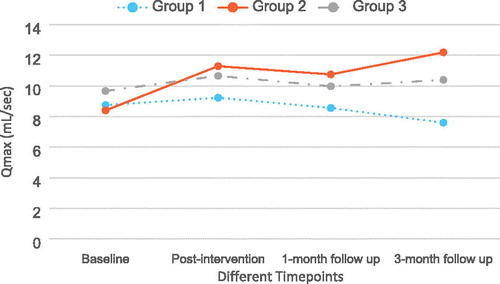
Figure 8. Post-void residual urine (mL) across time.
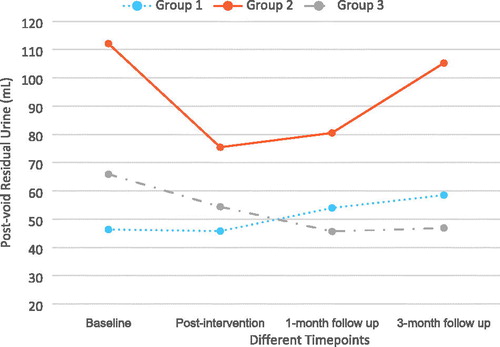
Table 3. Outcome variables across three groups at different timepoints.
Discussions
In a qualitative study, LUTS adversely affected the physical and psychological aspects of aging males because of frequent uncontrolled urinary condition [Citation7,Citation46]. The current study adopted a scientific approach using a double-blinded placebo-controlled trial in the evaluation of the treatment effect. Subjective measures and objective evaluation, including the well-validated IPSS and PSQI scales, change in Qmax (mL/s), and post-void residual urine (mL), were adopted. The effects demonstrated by the objective measures can minimize the subjective measurement bias derived from social desirability.
Preliminary results indicated that the combined AT approach (LAT plus MAT) has a more significant effect on relieving urinary symptoms, especially those related to voiding, and increases the maximum urinary flow rate and emptying rate of the bladder relative to those used in the placebo group (Group 1). The effect was sustained even up to the 3-month follow-up time. In the IPSS scale, the voiding problems associated with LUTS included the sensation of emptying the bladder after urination, the intermittency during urination, the urinary stream (weak vs. strong), and how often one had to push or strain to urinate [Citation42].
When comparing the combined AT approach with MAT alone (Group 3), the former group showed significant improvement in relieving the voiding problems and demonstrated a greater improvement in several parameters than that in the latter. Numerous clinical trials have successfully showed the use of MAT on different disorders, including but not limited to sleep disturbances [Citation28,Citation47], low back pain [Citation29], constipation [Citation30], and obesity [Citation48]. The effectiveness of MAT may be associated with the interaction of magnetic fields with the cutaneous blood flow and interact with the calcium channel protein in the cell membrane that results in the functional change of the body [Citation49–51]. Meanwhile, LAT provides a noninvasive alternative to needle acupuncture [Citation32]. This technique has been previously adopted to manage medical conditions, such as increasing the pain threshold [Citation37,Citation52], alleviating musculoskeletal pain [Citation33], and insomnia [Citation53]. Reports have shown that the laser beam not only irradiates and stimulates the acupoint but also activates the therapeutic effects of energy flow [Qi], regulates the functions of internal organs, and produces a therapeutic effect [Citation32]. We hypothesized that the therapeutic effect will be enhanced by the application of LAT followed by MAT, because the latter approach can offer continuous stimulation of ear acupoints, as long as the magnet pellets are in situ. This synergistic effect can be seen in a double-blind randomized controlled trial for the osteoarthritic knee, in which the subjects who received combined MAT plus LAT exhibited a stronger treatment effect in terms of pain relief, ambulation status, and range of movement of the knees than those of the participants treated with MAT or LAT alone [Citation54].
Basing on the neuro-embryonic theory, Dr. Paul Nogier viewed the auricle as a homunculus of the human body and has a similar shape to an inverted fetus [Citation21]. Performing appropriate stimulation of specific ear acupoints can achieve therapeutic effects [Citation55]. The six ear acupoints being selected were mainly associated with the genito-urinary tract, namely, “angle of the superior concha,” “kidney,” “bladder,” “ureter,” “external genitals,” and “internal genitals” [Citation37]. These acupoints were found to be associated with LUTS in the Chinese aging males, in terms of the tenderness being felt and the electrical conductivity during ear diagnostic examination. Among these acupoints, the “angle of the superior concha” (which is equivalent to the “prostate”) exhibited the highest sensitivity. This auricular point also demonstrated considerable sensitivity, specificity, and positive/negative predictive values on both ears during tenderness testing [Citation56].
Using 5-alpha-reductase inhibitors is a highly common pharmacological approach for relieving LUTS symptoms. However, patients are dissatisfied with the efficacy and the adverse effects of the drugs, and many of these individuals choose not to rely on long-term treatment [Citation13]. Unlike the Western treatment approach, AT presents with minimal adverse effects. Only few participants experienced mild skin irritation (itchiness) due to the use of adhesive tapes and attested that this therapy is safe in application. The irritation was resolved immediately after the adhesive tapes were removed by the participants. The combined AT approach being tested in this study can contribute to a reduction of IPSS score (Beta = −5.15), a sustained improvement in peak urinary flow rate of over 2 ml/s, and a reduction of post-void residual urine of over 30 ml after the treatment course compared with those used in the placebo group. These results are comparable or even slightly better than the efficacy of the long-term use of the 5-alpha-reductase inhibitors observed in previous representative studies [Citation13].
The high compliance rate (94.0%) and the positive impression toward the therapy indirectly indicated that blinding was successful because of the successful application of placebo in the trial. Over half of the participants expressed that they would definitely recommend this therapy to others. The findings of this trial can provide valuable information and increase the understanding of the therapeutic effect of AT, either by using a combined approach or MAT alone. The filling problems (i.e. frequency, urgency, and nocturia) of LUTS, the quality of life, and sleep conditions of the participants did not show substantial differences among groups after the therapy. A longer duration of the therapy may be considered in future trials to see whether these parameters can be improved. As the management of LUTS continues to evolve, this treatment approach can be considered as a noninvasive approach for managing this common problem among aging males. A future study with a large sample size is warranted to generate high-quality evidence to support the use of this therapy as an alternative and complementary option for elders with LUTS.
Limitations and recommendations of study
Given the small number of participants enrolled in this feasibility study, the generalization of results is limited. To substantiate our findings and establish a stronger causal relationship between treatment and effect, future trials must involve a larger sample size than that in this study. Other measures, such as the acute urinary retention rate and surgery risk reduction rate, which indicate clinical relevance, can be included in future studies. Moreover, an increased follow-up duration of up to 6 months to a year is necessary to ascertain the sustained treatment effect.
Conclusion
Preliminary findings indicate that a combined AT approach using LAT and MAT exhibited a stronger treatment effect in relieving voiding problems, greater peak urinary flow rate, and a less post-void residual urine than the approaches used in the placebo group and the MAT alone. This study demonstrated that the AT protocol adopted in this study for aging males with LUTS is feasible and can be adopted in a future study of increased scale. Future trials may consider a longer duration of intervention and follow-up periods than those adopted in the current study to achieve a full understanding of the therapeutic effect of this therapy.
Acknowledgements
The authors wish to acknowledge Mr. Hon Fat Wong (registered TCM practitioner) for the advice on acupoint selection and Dr. Doris Y.P. Leung for the advice on statistical analysis. The authors also extend their appreciation to the elderly centers and participants for the sincere support for this study.
Disclosure statement
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Cindolo L, Pirozzi L, Sountoulides P, et al. Patients’ adherence on pharmacological therapy for benign prostatic hyperplasia (BPH)-associated lower urinary tract symptoms (LUTS) is different: is combination therapy better than monotherapy? BMC Urology. 2015;15:96.
- Robert G, Descazeaud A, Delongchamps NB, et al. Transurethral plasma vaporization of the prostate: 3-month functional outcome and complications. BJU Int. 2012;110:555–560.
- Oelke M, Burger M, Castro-diaz D, et al. Diagnosis and medical treatment of lower urinary tract symptoms in adult men: applying specialist guidelines in clinical practice. BJU Int. 2012;110:710–718.
- Jeong WS, Choi HY, Nam JW, et al. Men with severe lower urinary tract symptoms are at increased risk of depression. Int Neurourol J. 2015;19:286–292.
- Wein AJ, Coyne KS, Tubaro A, et al. The impact of lower urinary tract symptoms on male sexual health: EpiLUTS. BJU Int. 2009;103:33–41.
- Wong SYS, Hong A, Leung J, et al. Lower urinary tract symptoms and depressive symptoms in elderly men. J Affect Disord. 2006;96:83–88.
- Suen LKP, Cheng HL, Yeung SKW, et al. Qualitative insights into the experiences of living with moderate-to-severe lower urinary tract symptoms among community-dwelling ageing males. PLoS One. 2017;12:e0187085.
- Yassin A, Nettleship JE, Talib RA, et al. Effects of testosterone replacement therapy withdrawal and re-treatment in hypogonadal elderly men upon obesity, voiding function and prostate safety parameters. Aging Male. 2016;19:64–69.
- Calogero AE, Burgio G, Condorelli RA, et al. Epidemiology and risk factors of lower urinary tract symptoms/benign prostatic hyperplasia and erectile dysfunction. Aging Male. 2018;1–8. DOI:10.1080/13685538.2018.1434772
- McVary KT, Roehrborn CG, Avins AL, et al. Update on AUA Guideline on the management of benign prostatic hyperplasia. J Urol. 2011;185:1793–1803.
- Pettaway CA, Lamerato LE, Eaddy MT, et al. Benign prostatic hyperplasia: racial differences in treatment patterns and prostate cancer prevalence. BJU Int. 2011;180:1302–1308.
- Haillot O, Fraga A, Maciukiewicz P, et al. The effects of combination therapy with dutasteride plus tamsulosin on clinical outcomes in men with symptomatic BPH: 4-year post hoc analysis of European men in the CombAT study. Prostate Cancer Prostatic Dis. 2011;14:302–306.
- Roehrborn CG. Current medical therapies for men with lower urinary tract symptoms and benign prostatic hyperplasia: Achievements and limitations. Rev Urol. 2008;10:14–25.
- Favilla V, Russo GI, Privitera S, et al. Impact of combination therapy 5-alpha reductase inhibitors (5-ARI) plus alpha-blockers (AB) on erectile dysfunction and decrease of libido in patients with LUTS/BPH: a systematic review with meta-analysis. Aging Male. 2016;19:175–181.
- Kosilov K, Kuzina I, Kuznetsov V, et al. Cognitive functions and health-related quality of life in men with benign prostatic hyperplasia and symptoms of overactive bladder when treated with a combination of tamsulosin and solifenacinin a higher dosage. Aging Male. 2018;21:121–129.
- MacDonald R, Brasure M, Dahm P, et al. Efficacy of newer medications for lower urinary tract symptoms attributed to benign prostatic hyperplasia: a systematic review. Aging Male. 2018;1–11. DOI: 10.1080/13685538.2018.1434503
- Calogero AE, Burgio G, Condorelli RA, et al. Treatment of lower urinary tract symptoms/benign prostatic hyperplasia and erectile dysfunction. Aging Male. 2018;29:1–9.
- Amano T, Earle C, Imao T, et al. Administration of daily 5 mg tadalafil improves endothelial function inpatients with benign prostatic hyperplasia. Aging Male. 2018;21:77–82.
- Spagnul SJT, Cabral PHO, Verndl DO, et al. Adrenergic α-blockers: an infrequent and overlooked cause of priapism. Int J Impot Res. 2011;23:95–98.
- Suen LKP, Wong TKS, Leung AWN. Is there a place for auricular therapy in the realm of nursing? Complement Ther Nurs Midwifery. 2001;7:132–139.
- Oleson T. Auriculotherapy manual (4th ed.). Edinburgh: Churchill Livingstone, Elsevier; 2014.
- Abbate S. Chinese auricular acupuncture (2nd ed). Boca Raton: CRC Press, Taylor & Francis Group; 2015.
- Soliman N. Soliman’s auricular therapy textbook: new localizations and evidence based therapeutic approaches. Bloomington: AuthorHouse; 2008.
- Huang ZH, Chen KF. Auricular electro-acupuncture in the treatment of 12 senile cases of prostatic hyperplasia. Med J Xiangtan Uni. 1997;6:341.
- Zhang GT. Ear acupuncture treatment of 14 cases with benign prostatic hyperplasia. Chin Acupunct & Moxi. 1998;5:316.
- Tang XF. The Auricular combined with the ultrasound infrared photons for benign prostatic hyperplasia. China Asso Acupunct &Moxi. 2000;20:531. 532. Chinese.
- Koh SJ, Song T, Kang YA, et al. An outbreak of skin and soft tissue infection caused by Mycobacterium abscessus following acupuncture. Clin Microbiol Infect. 2010;16:895–901.
- Suen LKP, Wong TKS, Leung AWN. Effectiveness of auricular therapy on sleep promotion in the elderly men. Am J Chin Med. 2002;30:429–449.
- Suen LKP, Wong EMC. Longitudinal changes in disability level of elderly with low back pain after auriculotherapy. Complement Ther Med. 2008;16:28–35.
- Li MK, Lee DTF, Suen LKP. A review on the complementary effects of auriculotherapy in managing constipation. J Altern Complement Med. 2010;16:435–447.
- Suen LKP, Chair SY, Thompson DR, et al. Traditional auriculotherapy for hypertension: a pilot randomized trial. J Cardiovasc Dis. 2014;2:19–24.
- Tian DZ. Laser acupuncture and TCM (Part I). Int J Clin Acupunct. 1996;7:397–399.
- Kneebone WJ. Laser acupuncture as a pain relief modality. Pract Pain Manage. 2008;64–68.
- Di T, Shi X. The therapeutic effect of using auricular acupressure for treating lower urinary tract symptoms. Chin Acupunct & Moxi. 2000;8:459–460.
- Wang Y, Wei R, Shu G, et al. Clinical study on conventional therapy with auricular point sticking for chronic prostatitis. Med Res Edu. 2014;31:36–40.
- Xiang YM, Sun XR. Acupuncture integrated with auricular acupressure for chronic prostatitis on 98 cases. Liaoning J Tradit Chin Med 2002;29:504.
- Wang ZH, Ceng Q, Wang SX, et al. The clinical use of the acupoint: angle of superior concha. Chinese Acupunct 11;1999:673–674.
- Nomenclature and location of auricular points (GB/T 13734-2008). China Standardization Organizing Committee. Beijing: China Zhijian Publishing House and Standards Press of China; 2008.
- Pointer Pulse™ (EC Certificate Reg. No.: DD60075127 0001). Tens Plus Industrial Company, Hong Kong. http://www.mayfairmed.com/web/eng/showpro.asp?product=DD3710
- King CE, Clelland JA, Knowles CJ, et al. Effect of helium-neon laser auriculotherapy on experimental pain threshold . Phys Ther. 1990;70:24–30.
- Round R, Litscher G, Bahr F. Auricular acupuncture with laser. Evid Based Complement Alternat Med. 2013;2013:984763.
- Choi EPH, Lam CLK, Chin WY. Validation of the International Prostate Symptom score in Chinese males and females with lower urinary tract symptoms. Health Qual Life Outcomes. 2014;12:1.
- Chong AML, Cheung CK. Factor structure of a Cantonese-version Pittsburgh Sleep Quality Index. Sleep Biol Rhythms. 2012;10:118–125.
- Kalauokalani D, Cherkin DC, Sherman KJ, et al. Lessons from a trial of acupuncture and massage for low back pain: patient expectations and treatment effects. Spine. 2001;26:1418–1424.
- Bell ML, Horton NJ, Dhillon H, et al. Using generalized estimating equations and extensions in randomized trials with missing longitudinal patient reported outcome data. Psycho-Oncology. 2018;27:2125–2131.
- Noguchi N, Chan L, Cumming RG, et al. A systematic review of the association between lower urinary tract symptoms and falls, injuries, and fractures in community-dwelling older men. Aging Male. 2016; 19:1–7.
- Lo C, Liao WC, Liaw JJ, et al. The stimulation effect of auricular magnetic press pellets on older female adults with sleep disturbance undergoing polysomnographic evaluation. Evid Based Complement Alternat Med. 2013;2013:530438.
- Hsieh CH, Su TJ, Fang YW, et al. Efficacy of two different materials used in auricular acupressure on weight reduction and abdominal obesity. Am J Chin Med. 2012;40:713–720.
- Ramey DW. Magnetic and electromagnetic therapy. Scientific Rev Alternat Med. 1998;2:13–19.
- Henry SL, Concannon MJ, Yee GJ. The effect of magnetic fields on wound healing. J Plastic Surg. 2008;8:393–399.
- Koch CLMB, Sommarin M, Persson BRR, et al. Interaction between weak flow frequency magnetic fields and cell membranes. Bioelectromagnetics. 2003; 24:395–402.
- Sampaio-Filho H, Bussadori SK, Goncalves MLL, et al. Low-level laser treatment applied at auriculotherapy points to reduce postoperative pain in third molar surgery: a randomized, controlled, single-blinded study. PLoS One. 2018;13:e0197989.
- Yao SY. 46 cases of insomnia treated by semiconductor laser irradiation on auricular points. J Tradit Chin Med. 1999;19:298–299.
- Suen LKP, Yeh CH, Yeung SKW. Using auriculotherapy for osteoarthritic knee among elders: a double-blinded randomized feasibility study. BMC Complement Altern Med. 2016;16:257.
- Hou PW, Hsu HC, Lin YW, et al. The history, mechanism, and clinical application of auricular therapy in traditional Chinese medicine. Evid Based Complement Alternat Med. 2015;2015:495684.
- Suen LKP, Yeh CH, Lee WK, et al. Association of auricular reflective points and the status of lower urinary tract symptoms in aging males. Aging Male. 2015;18:149–156.