
Abstract
Introduction and objective: With the world's older population continuing to grow, andropause (male menopause or late-onset hypogonadism) is considered as one of the most important issues of this era. In this study, we aimed to assess the effect of andropause health education on the level of knowledge and attitude of retired men.
Methods: This controlled trial was conducted on 80 retired men (40 in intervention group, 40 in control group), who had been employed by the Department of Education, Shiraz, Iran. Data collection tool was a 38-item questionnaire, designed by the researcher, on participants' knowledge and attitude about andropause. Data were analyzed using SPSS software, version 22 and statistical tests such as independent and paired t tests were used.
Findings: There was no significant difference between the intervention and control groups before the intervention. There was a significant difference in knowledge and attitude scores in each group immediately and 1 month after the intervention. The mean score of knowledge in the intervention group increased from 2.92 ± 1.68 before to 16.22 ± 1.34 after the intervention, and the attitude score increased from 14.9 ± 1.08 to 28.52 ± 1.44. Comparison of the two groups and repeated score analysis showed that there was a significant difference between the two groups over the time (p < .001).
Conclusion: Educational intervention improved the knowledge and attitude of retired men toward andropause, which can have a positive impact on the timely recognition and proper treatment of the complications of andropause.
Introduction
During middle ages, men and women experience changes that affect different aspects of their lives including their relationships with their partners [Citation1]. Men experience changes from middle ages onwards because of the gradual decline in testosterone and male hormones called andropause. The severity of these changes is not the same in all men. Like menopausal women, men experience a gradual process of andropause too [Citation2,Citation3]. The term “male menopause” first appeared in 1944 for describing various complaints of aging men, which were partially similar to women’s menopausal symptoms. Various terms have been used for signs and symptoms of male hormone deficiency including male climacteric, androclise, androgen decline in aging male (ADAM), late onset hypogonadism (LOH), and partial androgen deficiency of the aging male (PADAM) [Citation2].
The onset of hormonal changes in men occurs between 40 and 55 years of age, and about 70% of men in this age range experience symptoms of testosterone deficiency [Citation4]. The most common symptoms include sexual dysfunction, decreased libido, general malaise, mood swings, cognitive impairment, irritability, performance difficulties, decline in enjoyment of life and general well-being, night sweats, sleep disturbances, and palpitations [Citation5–9]. Men's health and health problems at different ages have received more attention in recent decades. Andropause has been recognized as a hidden threat to men's family life. Most men feel anxious about andropausal changes and do not know the cause. Some studies showed a link between the onset of symptoms of andropause and some psychological changes such as depression. Andropause and depression are associated with decreased male hormones [Citation10]. Numerous studies worldwide have found that the symptoms of affective disorders are associated with hormonal changes and andropause. Middle-aged men and older might experience moodiness, irritability, nervousness, depression, aggravation, fatigability, poor concentration, and deteriorating memory. Mismanagement of stress and stress coping techniques lead some men to hate enjoyable activities and prolong the course of the above mentioned disorders [Citation11]. One study showed that 21% of men aged 51–59 years, 26% of men aged 60–69 years, and 31% aged 70–86 did not have normal testosterone levels [Citation12].
Another study aimed at determining the prevalence of andropause in Iranian men aged 40–85 years who referred to southwestern health centers in Iran, showed that only 15.5% of men had normal testosterone levels. There was a statistically significant relationship between the severity of andropause symptoms and quality of life in different dimensions. There was also a significant relationship between the prevalence of andropause and age, low education, depression, coronary artery disease, and urinary incontinence [Citation13].
There are different views among specialists regarding the causes, treatment, and follow-up on these symptoms [Citation14]. And various ways to reduce symptoms and systemic complications are suggested [Citation15]. Therefore, prevention and selfcare can be effective and acceptable solutions.
Identifying and planning for andropause period are necessary in order to prevent the unpleasant effects on different aspects of men's lives. Research shows that changes in lifestyle and some of the day-to-day habits are needed to cope positively with and reduce the negative effects of this period [Citation16]. Despite the importance of understanding sign and symptoms and different needs of the andropause period, numerous studies in Asia, Europe, and the U.S. reported a lack of knowledge and awareness of andropause [Citation17–20].
Currently, attention to men's health is of great value. Because andropause can pose significant problems to the physical, mental, and sexual health of men and their spouses, and due to the importance of education in promoting men's knowledge about andropause, in this research, we aimed to study the impact of andopause health education on the level of knowledge and attitudes of men referring to the Retirement Center of Shiraz Department of Education, Shiraz, Iran.
Materials and methods
The present study is a controlled trial registered in the Iranian Registry of Clinical Trials (IRCT) as IRCT2016120127216N5. Ethics Committee of Shiraz University of Medical Sciences approved this study under registration number of IR.SUMS.REC.1395.93.
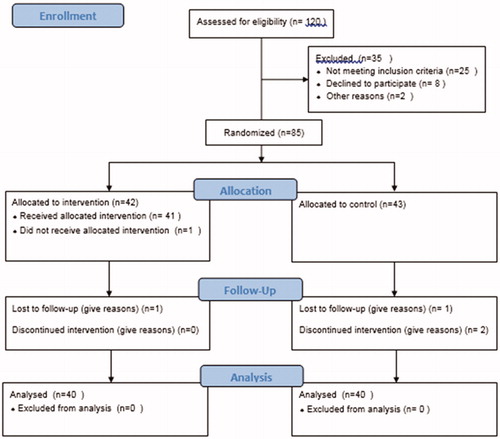
The study population consisted of all retired men over 60 years old in the Department of Education. The sample size was 80. The study was conducted from March 2016 to February 2017. For ease of access to the samples, first the number of retired men in the Department in the previous 5 years were identified, and based on the number in each year, the percentage of samples in that year was determined. Next, a random number was selected from the list of names of each year and the subjects were selected according the percentage allocation of that year (for example, if the number five was selected, the corresponding names with numbers 5, 10, 15, etc. were nominated until the quota was completed for each year). Next, the subjects were randomly divided into intervention and control groups (40 in each group).
Inclusion criteria were agreeing to participate in the study and having no specific physical or mental limitations for learning. Exclusion criteria were refusal to participate in the study, having a history of attending similar educational classes, and missing more than one class session ().
Figure 1. Flow diagram of enrollment.
Data collection tool was a questionnaire, designed by the researcher, examining the knowledge and attitudes of the men over 40 years old about andropause based on two studies in Canada and China (mentioned above), and urology books. The questionnaire consisted of three sections: (1) Demographic data (age, marital status, level of education, occupation, chronic disease); (2) Knowledge about andropause consisting of 20 questions (andropause concept – five questions, reasons for andropause – three questions, common andropausal symptoms – seven questions, premature andropause – two questions, diagnostic methods – one question, treatments – two questions); (3) Attitude toward andropause consisting of 18 questions.
To determine the validity and reliability of the results, 10 medical experts including nursing school instructors and urologists evaluated the questionnaire. The impact factor for all the items in the questionnaire was greater than 1.5 and content validity index was 0.9–1. The reliability of the questionnaire was measured by Cronbach's alpha coefficient, which was 0.81 for knowledge and 0.9 for the attitude questions. The entire questionnaire consisted of multiple choice questions and was based on the Likert rating scale. In the knowledge section, the correct answer to each question had a score of 1 and the total score range was 0–20. Scores 15–20 indicated high level of knowledge, 9–14 moderate, and below 9 low level of knowledge.
The attitude section was designed for the responses of agree, disagree, and undecided with a score of 2 for agree, 1 for disagree, and 0 for undecided. With a total score of 0–36, a score of 16–36 indicated positive attitude, and below 16 indicated a negative attitude toward andropause.
Educational intervention included lectures, group discussions, and question and answer sessions comprised one session per week for 4 weeks and each session for 60 min. The participants in the intervention group were educated on physiological changes during andropause, healthy lifestyles during older adulthood (about nutrition, physical activity, sleep, and rest), and how to deal with andropause changes. They received an educational booklet at the last session. The control group did not receive any education and only received the educational booklet after the study. Both groups completed the questionnaire before the intervention, immediately, and 1 month after the intervention.
Data analysis
The data were analyzed using SPSS software, version 22 (Chicago, IL, USA). Descriptive statistics such as frequency distribution, mean, and standard deviation to describe sample characteristics; inferential statistics including Pearson correlation coefficient, independent t test for comparison of both groups individually before and after the intervention; and repeated measures test before, after, and 1 month after the intervention were used as appropriated. p < .05 was considered as a significant level for all the tests.
Results
The mean age of the subjects was 68.37 ± 6.87 years. 61 (76.3%) subjects were married, 34 (42.5%) had a bachelor’s degree, and 26 (32.5%) had three children. 43 (53.8%) subjects had a history of prostate disease and 37 (46.3%) had a history of surgery. Only three (3.8%) subjects reported a history of hormone therapy. 43 (53.8%) had completed men's health screenings in the past year. compares the demographic characteristics of the intervention and control groups, showing no statistically significant differences between the two groups.
Table 1. Comparison of demographic characteristics of the participants.
According to independent t test before, immediately after, and 1 month after the intervention, there was a significant difference between the knowledge and attitude scores of the two groups. Moreover, repeated measure analysis showed significant differences within each group over time ( and ).
Table 2. Comparison of mean score of knowledge between intervention and control groups before and after the intervention.
Table 3. Comparison of mean score of attitudes between intervention and control groups before and after intervention.
There was no statistically significant relationship between the demographic characteristics of the participants and the mean scores of knowledge and attitude; however, Pearson correlation coefficient showed that there was a significant positive relationship between the mean scores of knowledge and attitude tests (p < .0001, Pearson correlation = 0.95).
Discussion
In recent decades, the issue of men's health has received more attention. Men's health in Iran is one of the new topics for which the health system has developed a program called Iranian Men's Health for the middle Ages and thereafter within the elderly care program. Most studies in this field are descriptive [Citation21]. The present interventional study aimed to assess the effects of education on men's knowledge and attitude about andropause. It should be noted that in most societies with similar cultures as Iran, andropause is a very new subject, which creates various reactions from men. Most of men are surprised and even deny it. At the beginning of the present study, the participants had poor knowledge and negative attitudes toward andropause, and some even sought to change the title of the class to Men's Health. However, the knowledge of the interventional group increased after the educational sessions [Citation21]. A study by Samipour and colleagues (2017) aimed to investigate the level of knowledge and experience of men referring to health centers about andropause. The result of the study showed that even though 6.73% of the subjects had experienced andropause symptoms, their awareness was deficient and only 15.5% had sufficient knowledge of this physiological process [Citation2]. Another study in India conducted by Puri and colleagues (2015) also showed inadequate levels of knowledge of Indian men (16.98%) despite experiencing the symptoms of andropause (82.82%) [Citation4]. Another study in Turkey was conducted on men over 40 and examined men's experience and awareness of andropause. The result of the study showed that 16.9% of the subjects had experienced the symptoms but 46% of them did not have adequate knowledge about andropause [Citation5].
Al-Sejari's study in Kuwait that aimed to examine the level of awareness and understanding of men about andropause showed that 36% of men were familiar with the subject, 38.4% thought men would never experience andropause, and 53.4% did not know the age of onset for andropause [Citation22]. A study by Kino and colleagues in Japan examined the level of knowledge and awareness of 2800 nurses and staff about andropause showed that female nurses were significantly more aware of male climacteric than female employees who were not a nurse. Nurses who had experienced symptoms of menopause were more interested in understanding andropause [Citation19].
A quasi-experimental research by Afsharnia and colleagues (2018) studied the effects of electronic learning on the quality of life and symptoms of hypogonadism in working men. They showed that compared with the control group, there was a statistically significant difference in quality of life and symptoms in the intervention group immediately and two months after the intervention [Citation21]. A clinical trial by de Carvalho and colleagues (2018) examining the effect of exercise on androgen deficiency symptoms showed that an exercise routine reduced the symptoms of andropause and improved physical, hormonal, psychological, and sexual changes caused by male hormone deficiency [Citation23].
In the present study, there was no statistically significant relationship between the demographic characteristics of the subjects and their attitudes and knowledge. The results of a study on andropause in Iran in 2017 did not show a significant statistical relationship between the demographic characteristics, age, and some health habits such as smoking [Citation2]. The results of a study in Kuwait showed a significant relationship between men’s awareness of andropause and level of education, age group, and marital status [Citation18].
A study by Kargar and colleagues (2016) examining general practitioners' knowledge and attitudes toward andropause showed that the knowledge of the physicians and their demographic characteristics were not correlated, but there was a correlation between the attitude of the participants in the study and their attitude towards andropause [Citation24].
Another cross-sectional study in Kuwait on 214 men over the age of 40 found that there was a significant relationship between the level of education of subjects and the symptoms of andropause in men over 50 years of age. This study also emphasized on the importance of education about symptoms, prevention, and coping with andropausal changes [Citation18]. The variation in study results may be due to social and cultural differences between the target groups in different studies.
Conclusion
Different aspects of men's health, especially their sexual health, are still a new and controversial topic. Health education about andropause helps men better adjust to the gradual changes in older ages and ultimately increases their sense of well-being and prevents further difficulties. We suggest including education about andropause and sexual health in middle and old ages in men's care programs.
Limitations
One of the limitations of this study was that the subjects were retired male employees of only one establishment, the Department of Education. Studying various populations is necessary for more accurate results.
Acknowledgments
This article was extracted from a research project, which was financially sponsored by Vice-Chancellery for Research Affairs of Shiraz University of Medical Sciences (No.10597). The authors would like to thank all individuals who participated in and assisted with this study and also Shiraz University of Medical Sciences for their financial support.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Jannini E, Nappi R. Couplepause: a new paradigm in treating sexual dysfunction during menopause and andropause. Sex Med Rev. 2018;6(3):384–395.
- Samipoor F, Pakseresht S, Rezasoltani P, et al. Awareness and experience of andropause symptoms in men referring to health centers: a cross-sectional study in Iran. Aging Male. 2017;20(3):153–160.
- Singh P. Andropause: current concepts. Indian J Endocr Metab. 2013;17(9):621–629.
- Puri S, Singh A. ADAM and AMS scale for assessing andropause among aging Indian men. Int J Pharm Pharm Sci. 2015;7:453–458.
- Akkuzu G, Dogan N, Karahan A. What do individuals aged 40-64 think about midlife events and their experiences: menopause and andropause. Global J Adv Pure Appl Sci. 2014;4:283–290.
- Yuen J, Ng C-F, Chiu P, et al. Aging males” symptomsand general health of adult males: a cross-sectionalstudy. Aging Male. 2016;19(2):71–78.
- Shigehara K, Konaka H, Sugimoto K, et al. Sleep disturbanceas a clinical sign for severe hypogonadism:efficacy of testosterone replacement therapy on sleepdisturbance among hypogonadal men withoutobstructive sleep pnea. Aging Male. 2018;21(2):99–105.
- Charandabi SM, Rezaei N, Hakimi S, et al. Sleep disturbancesand sexual function among men aged 45–75years in an urban area of Iran. Sleep Sci. 2016;9(1):29–34.
- Kaya E, Sikka SC, Kadowitz PJ, et al. Aging and sexualhealth: getting to the problem. Aging Male. 2017;20(2):65–80.
- Rabijewski M, Papierska L, Kuczerowski R, et al. Hormonal determinants of the severity of andropausal and depressive symptoms in middle-aged and elderly men with prediabetes. Clin Interv Aging. 2015;10:1381–1391.
- Jakiel G, Makara-Studzińska M, Ciebiera M, et al. Andropause – state of the art 2015 and review of selected aspects. Prz Menopauzalny. 2015;14:1–6.
- O’Donnell A, Travison T, Harris S, et al. Testosterone, dehydroepiandrosterone, and physical performance in older men: results from the Massachusetts Male Aging Study. J Clin Endocrinol Metab. 2006;91:425–431.
- Rezaei N, Azadi A, Pakzad R. Prevalence of andropause among Iranian men and its relationship with quality of life. Aging Male. 2018;7:1–8.
- Lunenfeld B, Mskhalaya G, Zitzmann M, et al. Recommendations on thediagnosis, treatment and monitoring of hypogonadism in men. Aging Male. 2015;18(1):5–15.
- Ruige J, Ouwens D, Kaufman J. Beneficial and adverse effects of testosterone on the cardiovascular system in men. J Clin Endocrinol Metab. 2013;98(11):4300–4310.
- Camacho EM, Huhtaniemi IT, O'Neill TW, et al. Age-associated changes in hypothalamic-pituitary-testicular function in middle-aged and older men are modified by weight change and lifestyle factors: longitudinal results from the European Male Ageing Study. Eur J Endocrinol. 2013;168(3):445–455.
- Odu O, Olajide A, Olajide F, et al. Awareness and perceptionof androgen deficiency of aging males (ADAM) among men in Osogbo, Nigeria. J Commun Med Primary Health Care. 2014;25(2):42–52.
- Maha AS. Prevalence of andropausal symptoms among Kuwaiti males. Am J Mens Health. 2013;7(6):516–522.
- Kino A, Uemura H, Yasui T. Different levels of awareness and knowledge of male climacteric in female nurses and female office workers. Maturitas. 2015;80(2):198–204.
- Tsujimura A. The relationship between testosteroned deficiency and men’s health. World J Mens Health. 2013;31(2):126–135.
- Afsharnia E, Pakgohar M, Khosravi S, et al. Examining the effect of the computer-based educational package on quality of life and severity of hypogonadism symptoms in males. Aging Male. 2018;21(2):85–92.
- Al-Sejari M. Awareness and knowledge of andropause among Kuwaiti males. J Soc Sci. 2013;41(1):9–25.
- Vieira MCS, Leitão AE, Vieira G, et al. Concurrent training protocol for men with androgen deficiency in the aging male: a randomized clinical trial. Aging Male. 2018;21(3):149–157.
- Kargar M, Abootalebi M, Jahanbin I, et al. Knowledge and attitude about andropause among general physicians in Shiraz, Iran 2014. Int J Community Based Nurs Midwifery. 2016;4(1):27–35.