
Abstract
Urethral amyloidosis (UA) is a very rare condition. We here report the case of a 63-year-old male patient who was admitted to our outpatient department due to aggravating dysuria, frequent urination, pain during intercourse, and a gradually enlarging mass at the ostium of his urethra, which he first notice one year earlier. Pathological tissue biopsy of urethral ostium mass confirmed UA. Intermittent urethra infusion of dimethyl sulfoxide was performed and the treatment effect is satisfactory.
Introduction
Urethral amyloidosis (UA) is a rare clinical disease. Ever since UA was first reported in 1909 [Citation1], mere dozens of cases have been recorded. UA usually is a long course before diagnosis, and the process of definite diagnosis is complex. The treatment has always been controversial, because urethral dilatation or fistulation through bladder or perineal is prone to relapse, and resection and urethra replantation treatment cannot retain organ tissue, so there is the absence of satisfactory methods. This case reported herein is unique in that we tried to treat UA with dimethylsulfoxide urethral perfusion for the first time, which could maintain the patient’s tissues and organs, and therapeutic effect is satisfactory.
Case report
A 63-year-old male patient was admitted to our outpatient department for aggravation of pain while urinating, difficulty voiding, frequent urination, and pain during intercourse going back one year. None of the patient’s personal, family history was unusual, and the patient had no history of urinary trauma or urethral surgery. Physical examination revealed normal developmental nutrition, normal liver and spleen volume, normal kidney, and bladder. The patient had a normal penis at the time of examination, and there was a light red mass around the ostium of urethra at the glans. The palpable mass ran along the urethra toward the base of the penis. The mass was about 7 cm long. Urinalysis showed white blood cells 10–20, red blood cells 20–30, and urine protein negative. Blood biochemistry, blood glucose, and prostate-specific tumor antigen findings were normal. Abdominal ultrasound and chest radiograph were normal.
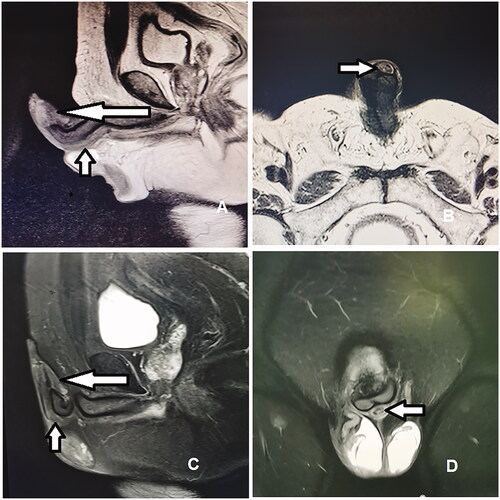
The patient was diagnosed with inflammatory disease and received intermittent antibiotic treatment for about 6 months with unsatisfactory results. The patient’s difficulty voiding worsened and the volume of the mass increased (). The duration of each voiding was about 2–3 min. () scans were performed on the penis and urethra, and MRI sagittal T2-weighted images showed iso-low signal in the glans (long white arrow) and the cavernous body in the urethra (short white arrow). A biopsy of the mass was performed and the biopsy was positive with Congo red staining, which confirmed that the patient had UA (). The symptoms of dysuria were severe and his maximal flow rate was 5 mL/s. Several invasive treatments were recommended, but the patient expressed concerns and declined.
Figure 1. (A) The mass located around ostium of urethra at the glans increased in volume and was pale red. (B) The mass at the outism of urethra and penile urethral decreased significantly.
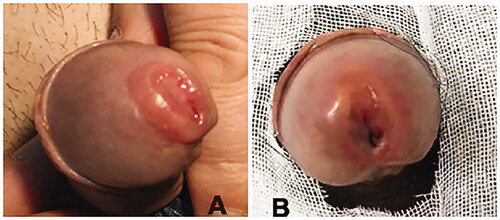
Figure 2. (A) The biopsy of the mass was stained with Congo red, and a clear circle appeared around the cells. (B) F10 Foley catheter.
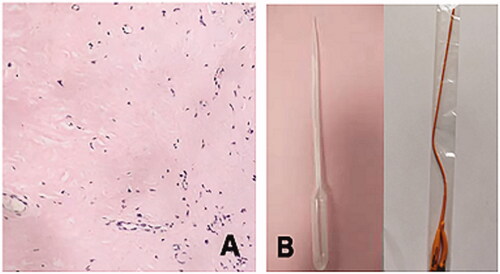
After consultation with the patient, he signed a consent form to allow administration of the special drug. Furthermore, this study was approved by the Ethics Committee of the Beijing Aerospace General Hospital. The patient was treated with urethral opening dripping and intraurethral perfusion with dimethylsulfoxide. A sterile soft laboratory tube was used for instillation, and a F10 Foley catheter was used for perfusion (). During the perfusion process, the perineal urethra was pressed by the patient himself to prevent the perfusion fluid into the bladder. Each perfusion was about 10 mL for about 10 min. There was a momentary stinging at the beginning of the perfusion, and the irritation symptoms disappeared after the end of the perfusion. Perfusion was performed once every 5 d. Perfusion with a concentration of 50% was given at the beginning and a concentration of 100% after signing another consent form 4 weeks later. After 18 months of treatment, the physical examination revealed that the volume of the mass at the outism of urethra and penile urethral decreased significantly (). MRI ()) sagittal fat inhibition T2-weighted MR images showed a reduced range of iso-low signal in the glans (long white arrow) and the cavernous body in the urethra (short white arrow). The urine maximal flow rate at 18 months was 17 mL/s and the patient’s urinary tract irritation symptoms disappeared, the urethral mass decreased in size, and his urination and sexual function improved. The patient was satisfied with the treatment.
Figure 3. (A) Sagittal MRI scan of penis and urethra. (B) Transverse MRI of penis and urethra. (C) Sagittal MRI scan of penis and urethra after treatment. (D) Transverse MRI of penis and urethra after treatment.
Discussion
Amyloidosis was first discovered by Virchow in 1854. It is a group of diseases that are characterized by the extracellular deposition of amyloid proteins in tissues or organs. The cause of amyloidosis is hypothesized that it is related to immune dysfunction, gene mutation, and excessive production of amyloid during chronic diseases [Citation2]. UA was first reported in 1909 and there are currently about 50 cases reported in the literature, most in men, and only one case has been reported in women [Citation1,Citation3].
The natural history, clinical symptoms, diagnostic methods, and treatment methods of UA cases in the past 20 years were reviewed (). The result showed that UA usually has a long course when it develops, and it often has such symptoms as mass, hematuria, blood sperm, and dysuria. Imaging examinations, such as ultrasound, scans, and MRI, are often used to diagnose urethral abnormalities, but MRI is more helpful in determining the extent of lesion invasion [Citation4]. The definite diagnosis of UA requires tissue biopsy and special pathological staining. Treatment strategies for UA remain controversial for limited number of case reports and large differences in treatment options [Citation5]. Thus, the treatment may be selected according to patient’s individual symptoms including cystostomy, intermittent urethral dilatation, and urethroplasty with buccal mucosa or perineal skin flap (). Yao et al. [Citation6] reported 4 cases of UA, and found that urethral dilatation and transperineal urethrotomy had recurrence, while urethroplasty did not have recurrence and had a good effect.
Table 1. Clinical characteristics of diagnosis and treatment for patients with urethral amyloidosis on PubMed in recent 20 years.
Unlike previous reports, the initial symptoms of this patient were mainly dysuria and long urination time. The patient urinates for 2–3 min each time, with a maximum flow rate of 5 mL/s, and has sexual dysfunction. After the initial anti-inflammatory treatment was ineffective, the mass at the ostium of urethra increased significantly, and was confirmed by Congo red staining biopsy ().
In this patient, the symptoms of dysuria progressed rapidly, and the external urethral mass grew rapidly. After confirmation of diagnosis, the patient was advised to perform cystostomy or urethroplasty. Considering the quality of life after cystostomy and the ethical and spiritual impact of removal of the glans via urethroplasty, the patient declined treatment. The patient was informed that there were only reports of dimethylsulfoxide infusion for bladder amyloidosis and no previous studies covering urethral infusion. He signed a consent form, and the study was reported to the Medical Ethics Committee of the Beijing Aerospace General Hospital.
The treatment of this patient with dimethylsulfoxide was based on the findings of previous studies: that dimethylsulfoxide can be mixed with water to form a polar aprotic solvent, and it can dissolve many polar and non-polar small-molecule substances with significant anti-inflammatory effect [Citation7,Citation8]. Fifty percent is commonly used concentration of dimethylsulfoxide [Citation9]. The patient had no significant adverse effects after 4 weeks of perfusion and 100% concentration perfusion was treated after signing another consent form. Physical examination, urinary flow rate, and MRI showed that the effects were significant 18 months after treatment, and the patient’s urinary tract irritation symptoms disappeared, the urethral mass decreased in size, and his urination and sexual function improved. The patient was satisfied with the effects, probably because dimethylsulfoxide can block the generation of oxygen free radicals, remove existing free radicals, reduce the production of inflammatory substances, and relieve anti-inflammatory and antioxidative stress.
Author contributions
All authors had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: Xiaoxing Liao; Acquisition of data: Jianghua Yang, Rongzhen Ye, and Xiaofeng Zheng; Analysis and interpretation of data: Xiaoxing Liao, and Jianghua Yang; Drafting of the manuscript: Yunzhi Li, Guojing Gao, and Xiaoxing Liao; Critical revision of the manuscript for important intellectual content: Xiaoxing Liao; Study supervision: Xiaoxing Liao.
Ethical approval
The report of this study was approved by the ethics committee of the Beijing Aerospace General Hospital, and written informed consent was obtained from the patient.
Disclosure statement
The authors report there are no competing interests to declare.
References
- Tilipe A. Ueber locales tumorformiges amyloid der harnrohrezentralbl. Allg Pathol. 1909;20:913–916.
- Gertz MA, Lacy MQ, Dispenzieri A, et al. Amyloidosis: diagnosis and management. Clin Lymphoma Myeloma. 2005;6(3):208–219.
- Kageyama S, Suzuki K, Ushiyama T, et al. Primary localized amyloidosis of the urethra in a woman. Br J Urol. 1998;81(6):918–919.
- Kawashima A, Alleman WG, Takahashi N, et al. Imaging evaluation of amyloidosis of the urinary tract and retroperitoneum. Radiographics. 2011;31(6):1569–1582.
- Mangera A, Linton KD, Fernando M, et al. What is the evidence for the management of urethral amyloidosis? A systematic review of the literature. BJU Int. 2012;109(12):1858–1861.
- Yao X, Yuan Y, Fang J, et al. Benefits of urethroplasty for managing urethral amyloidosis: a case report. Exp Ther Med. 2017;14(4):3519–3522.
- Misuri L, Cappiello M, Balestri F, et al. The use of dimethylsulfoxide as a solvent in enzyme inhibition studies: the case of aldose reductase. J Enzyme Inhib Med Chem. 2017;32(1):1152–1158.
- Elisia I, Nakamura H, Lam V, et al. DMSO represses inflammatory cytokine production from human blood cells and reduces autoimmune arthritis. PLoS One. 2016;11(3):e0152538.
- Liu P, Zhang M, Shoeb M, et al. Metal chelator combined with permeability enhancer ameliorates oxidative stress-associated neurodegeneration in rat eyes with elevated intraocular pressure. Free Radic Biol Med. 2014;69:289–299.