
Abstract
This paper explores individual, interpersonal- and household-level factors influencing HIV-related sexual risk behaviour among adolescent girls who participated in an intervention to reduce HIV risk in a rural setting in Mozambique. Twenty-eight adolescent girls ages 13–19, 30 heads of household, and 53 influential men participated in in-depth interviews at two time points. Comparative analysis compared girls who reported reducing risk behaviours over time to girls who did not and identified factors that respondents described as influential to behaviour change. Among the twenty girls self-reporting sexual risk at the first time point, half had reduced these behaviours one year later. Changes in girls’ behaviours were contingent upon household- and interpersonal-level factors, particularly households’ economic stability and family members’ financial support. Future interventions with adolescents in similar settings should evaluate and leverage household and family support to achieve sexual risk reduction.
Introduction
Adolescent girls and young women disproportionately bear the burden of new HIV infections, particularly in sub-Saharan Africa (UNAIDS Citation2015a; Bekker and Hosek Citation2015; Dellar, Dlamini, and Karim Citation2015), and experience heightened vulnerability to HIV due to biological, social, and structural factors (Jewkes and Morrell Citation2010). Recent global guidance prioritises research on adolescent girls and young women in sub-Saharan Africa to assess and effectively respond to this population’s unique HIV prevention needs (UNAIDS Citation2015b; UNICEF Citation2016b, Citation2016a).
Social factors have a particular influence on HIV risk and risk reduction among girls and young women in sub-Saharan Africa. Research has established relationships between risk behaviours such as condom use and intergenerational sex and factors including orphan status, school attendance, household economic status, poor social relationships and community supportiveness of girls (Underwood et al. Citation2011; Underwood and Schwandt Citation2015; Schaefer et al. Citation2017; Hendriksen et al. Citation2007; Davidoff-Gore Citation2011). Qualitative research similarly points to the influence of individual- and household-level economic status, relationship dynamics, cultural practices and gender norms on HIV risk (Psaros et al. Citation2017; Harper et al. Citation2014). In some settings, sexual activity among adolescent girls and young women is framed positively through positive attitudes towards women initiating multiple concurrent relationships with men (Agnarson et al. Citation2015), encouraging girls’ participation in sexual initiation rites (Skinner et al. Citation2013) and assigning significant meaning to exchanges in transactional sex (Ranganathan et al. Citation2017; Leclerc-Madlala Citation2008). These findings demonstrate the complexity, diversity and setting-specificity of these factors.
Mozambique had an estimated 8.85 new HIV infections per 1,000 adults (ages 15-49) in 2017, among the highest incidence rates globally (UNAIDS Citation2019). In Zambézia Province, an estimated 14% of young women (ages 15-24) were living with HIV in 2015, more than three times higher than the estimated prevalence among men the same age (Instituto Nacional Saúde, Instituto Nacional Estatística, ICF Internacional Citation2015). Few studies have explored the factors driving these high rates of transmission in Zambézia, but data suggest relationships between gender, power differentials, economic status and HIV risk in Mozambique more broadly (Bandali Citation2013, Citation2014; Pons-Duran et al. Citation2016). Pervasive gender inequity has been documented in Mozambique through the country’s high gender inequity ranking (UNDP Citation2016) and rates of intimate partner violence (UNAIDS Citation2019). Furthermore, research in Zambezia and other provinces has documented high rates of sexual violence against women and girls (Parkes et al. Citation2016) and gender roles that position men as economic providers and sources of authority over women (Macia, Maharaj, and Gresh Citation2011; Lenzi et al. Citation2019). Despite evidence of shifting norms in some areas (Bandali Citation2011b, Citation2011a), local research partners have confirmed that these changes have yet to touch the province’s rural communities. Female sexual initiation rites and lobolo exchanges of cattle or money before traditional marriage are largely still in effect and the persistence of similar practices has been documented elsewhere in the region (Makusha and Richter Citation2016; Bagnol Citation2013). Furthermore, rural Zambézia depends primarily on subsistence agriculture and is among the country’s most impoverished provinces, with many areas lacking access to electricity, improved sanitation and healthcare infrastructure (Baez Ramirez et al. Citation2018).
In 2010, a combined economic and social empowerment intervention was implemented in Zambézia to address adolescent girls’ vulnerability to HIV and gender-based violence. A post-intervention evaluation found mixed impacts on girls’ self-reported HIV-related sexual risk behaviour (Burke et al. Citation2017). To contextualise these findings, this paper describes girls’ self-reported risk behaviours and uses a social ecological model (SEM) to identify multi-level factors beyond the intervention that drove engagement in risk behaviours and/or facilitated risk reduction.
Materials and methods
Intervention and parent study
The Women First intervention aimed to reduce girls’ (ages 13-17) vulnerability to HIV through education and economic empowerment (Burke et al. Citation2019). The intervention included an educational component with a structured curriculum that covered topics including HIV prevention, condom use, and gender equity. A simultaneous small business component taught business skills and provided subsidised products for girls to sell, including household items and ingredients for baked goods. The intervention was implemented over a five-year period through September 2015, taking place in 22 rural communities in Zambézia with approximately 300 vulnerable adolescent girls. Girls were considered vulnerable if they had lost one or both parents, lived in a child-headed household, or engaged in transactional sex or other HIV-related sexual risk behaviours.
The data used in this analysis were collected through in-depth interviews (IDIs) conducted during a mixed-methods evaluation of the Women First intervention (Burke et al. Citation2019, Citation2017). The evaluation was reviewed and approved by the federally registered institutional review boards of FHI 360 and Vanderbilt University and the National Bioethics Committee for Health in Mozambique. All participants provided written informed consent or parental/guardian consent plus participants’ informed assent for participants under 18 years. Participants were not given reimbursements or incentives for participation. The qualitative component of the parent study was shaped by a social ecological model (SEM) to better understand intervention impacts on the individual, interpersonal, household and community levels (McLeroy et al. Citation1988). The SEM outlined by McLeroy et al. is a theory-based framework for understanding the multifaceted and interactive effects of personal and environmental factors that influence behaviour; this framework recognises multiple levels of influence on behaviour as well as reciprocal causation between an individual and their social environment.
Data collection
Qualitative data for the parent study were collected between August-October 2015 (Time 1), shortly after the intervention ended in most communities, and one year later, August-October 2016 (Time 2) and included IDIs with adolescent girl intervention participants, girls’ heads of household and influential men. These salient references were included to obtain more nuanced detail about intervention impacts on girls’ lives; discern impacts on the interpersonal, household and community levels and references’ attitudes towards the said impacts; and triangulate information by comparing data within each ‘cluster’ of an adolescent girl and her salient reference(s). Girls selected to identify salient references were asked to invite their head of household and/or five non-head of household men with whom she felt most close to contact study staff if they were interested in participating in an interview; staff contacted influential men from the list until three agreed. This paper uses data from the 28 ‘clusters’ of girls who were randomly selected to also have one or both types of salient reference participate in IDIs.
Trained qualitative interviewers used semi-structured interview guides to explore girls’ participation in the intervention; changes in girls’ relationships; girls’ community involvement; girls’ attitudes towards sex, dating and marriage; and girls’ goals for the future. IDIs were conducted one-on-one in a private location and lasted about one hour. All IDIs were audio-recorded, transcribed and translated simultaneously from local languages to Portuguese, then professionally translated into English. The primary analysis used codebooks developed a priori with emergent thematic codes added during analysis. IDIs were coded in Nvivo 11, with teams of two analysts (among co-authors KR, CP and RL) independently coding 12.5% of transcripts to assess inter-coder reliability (QSR Citation2015).
Analysis
The analysis used qualitative data from the 28 clusters of adolescent girls and salient references who participated in IDIs at Times 1 and 2. After a team of three analysts (KR, CP, RL) conducted a primary analysis, the first author reviewed all included transcripts at Times 1 and 2 and identified factors described as influential to girls’ risk behaviours, using an inductive approach. The first author organised social and economic factors on the individual, interpersonal, household and community levels to correspond with the SEM (McLeroy et al. Citation1988) then completed a structured matrix for each cluster to document the presence of each factor, changes over time and any discrepancies between a cluster’s respondents. Respondents who contradicted themselves or were silent on a topic were excluded from relevant areas of the matrix.
Each girl’s sexual behaviour was characterised as either ‘continued risk’ over time, ‘reduced risk’ over time, or never sexually active. Risk behaviours included: (1) ‘dating,’ ‘walking around’ or ‘playing’ with men or boys (confirmed by local research partners as euphemisms for being sexually active, often also for having transactional sex or multiple partners); (2) never or rarely using condoms; (3) engaging in transactional sex (both formal ‘commercial sex’ as sometimes referred to in IDIs as well as informal exchanges of sex for school-related expenses, food, or money; both typically occurred with older adult men and were thus also intergenerational); and (4) having multiple concurrent sexual partners. Girls’ behaviour was determined to be ‘reduced risk’ if, by Time 2, they were described as: (1) having engaged in any of the above behaviours at or before Time 1 and no longer doing so; (2) becoming monogamous after previously having multiple sexual partners; (3) using condoms frequently or consistently after engaging in any of the above behaviours at or before Time 1. Other behaviours or experiences known to contribute to HIV risk were also considered, including experiencing gender-based violence from a sexual partner (Dunkle et al. Citation2004; Jewkes et al. Citation2010) and getting married before age 18 (Clark Citation2004). Pregnancy and childbearing were considered proxy indicators of a girl being sexually active. Descriptions of girls ‘dating’ always started before girls were 18 and therefore indicated early sexual debut (Pettifor et al. Citation2004).
The analysis used a comparative approach to synthesise data, identify common features across clusters and draw comparisons between girls who reduced their sexual risk behaviours over time and those who did not. Within-case comparative analysis focuses on contextual factors affecting each case and allows for a precise understanding of a particular case (Bazeley Citation2013), while cross-case comparative analysis identifies commonalities and synthesises data across sets of cases with shared features (Bazeley Citation2013; Ayres, Kavanaugh, and Knafl Citation2003). This analysis first used a within-case comparative approach to compare respondents’ responses related to girls’ risk behaviours and identify influential factors within each cluster, and then used a cross-case comparative approach to summarise and compare influential factors common to girls who reduced their risk behaviours and separately among girls who continued the risk behaviours. For each group, shared thematic narratives were summarised descriptively and the inter-relatedness of themes was highlighted using an illustrative example (see and ).
Figure 1. Poor household economic status and inequitable relationship with husband drive transactional sex and low condom use.
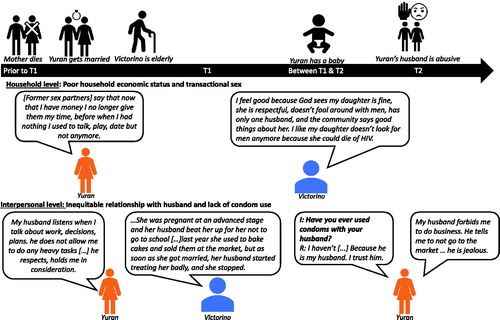
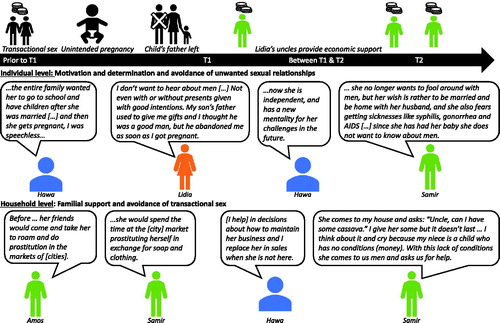
Figure 2. Individual motivation and familial support facilitate avoidance of unwanted relationships and transactional sex.
Throughout this paper, the term ‘respondents’ refers to girls, heads of households, and influential men collectively; ‘salient references’ refers to only heads of households and influential men. To ensure confidentiality, pseudonyms are used to identify participants, salient references’ ages are presented as young adult (15-25 years), adult (26-55 years), and older (56-80 years) and the names of locations have been removed from quotes.
Results
Data were available from 28 clusters and a total of 111 unique respondents: 28 girls, 30 heads of household, and 53 influential men. All girls participated in the intervention and were interviewed at both Time 1 and Time 2; 16 heads of household and 19 influential men were also interviewed at both time points. The remaining salient references differed between Times 1 and 2 as girls were asked to identify their current salient references at each time point. Heads of household were on average 46 years old and were most frequently girls’ mothers or aunts. Influential men had an average age of 34 years and often were uncles, brothers and cousins. Twenty adolescent girls were described as engaging in HIV-related sexual risk behaviours at or before Time 1 and were included in the comparative analysis. Eight girls reported that they had never had sex, which was confirmed by their salient references; these girls were among the youngest in the sample and often stated they had not yet reached puberty. Given this paper’s focus on factors influencing sexual risk reduction, data from these girls and their salient references were excluded from the comparative analysis.
HIV-related sexual risk behaviours and emergent influential factors
Adolescent girls included in the comparative analysis had a mean self-reported age of about 16 years at Time 1; almost two-thirds were single or double orphans (one or no parents living), and a few also reported not living with immediate family ().
Table 1. Self-reported demographics of sexually active adolescent girls by risk category.
Adolescent girls in 10 clusters reported HIV-related sexual risk behaviours at Time 1 that continued through Time 2 and were categorised as having ‘continued risk’. These girls and their salient references described girls engaging in multiple risk behaviours that often varied over time, including transactional sex and/or having multiple concurrent sexual partners, getting married for financial reasons or before age 18, not using condoms and having unintended pregnancies. Although participants were not always asked about girls’ husbands, available information indicated that husbands were typically older than girls by three or more years, were involved in local business, and that these marriages provided girls greater financial security. Girls’ families received financial benefits through lobolo bride price exchanges and reduced financial responsibility for girls.
Ten girls who had engaged in HIV-related sexual risk behaviours at or before Time 1 reported that they had stopped or reduced these behaviours by Time 2 and were considered to have ‘reduced risk’. Seven girls substantially reduced risk behaviours by Time 2; respondents reported that girls had stopped engaging in transactional sex, became monogamous, stopped dating, used condoms consistently, or avoided an unwanted marriage. Among the remaining three girls, respondents reported that they believed the girls stopped engaging in transactional sex or reduced the number of sexual partners but had a child between Times 1 and 2, were still ‘dating’ or having sex, or were not using condoms consistently at Time 2.
About one-third of girls reported being economically self-sufficient at Time 1, and far fewer reported the same at the second time point. The majority of girls who reported economic self-sufficiency were categorised as having reduced risk. Less than half of girls at both time points were enrolled in school; this number remained stable for girls that reduced risk but dropped for girls who had continued risk at Time 2.
Multiple interrelated factors influenced girls’ risk behaviours or facilitated risk reduction, with clear distinctions between adolescent girls who had ‘continued risk’ and reduced risk (see online supplemental appendices 1 and 2). Some factors, such as orphan status and community-level poverty and famine, were present and similar among both groups of girls. Findings on the most meaningful differences between the two groups are presented by SEM level below. Full details on each participant are available as online supplemental material.
Individual level
Among both groups, girls’ individual economic self-sufficiency and self-reliance were described as influential to reduced risk behaviour. At Time 1, only one girl who had continued risk was economically self-sufficient compared to five girls who had reduced risk and only reduced risk girls were able to maintain financial independence at Time 2. Individual motivation and determination were described as facilitating reductions in risk behaviour only among ‘reduced risk’ girls.
At Time 1, five reduced risk girls were described as economically self-sufficient after the intervention ended. These girls and their salient references stated that girls’ small businesses provided economic independence from both families and sexual partners. Girls described that they had stopped engaging in transactional sex, particularly with older men, due to the money they earned through their small businesses.
Interviewer: What changes did you notice with regard to sexual partners?
Rabia: They say that now because we do our own business, we don’t want to date them anymore: ‘These girls dodge us now because of the money they earn in the program.’ And I like when they say that […] I am the boss now. Men don’t fool around with me anymore because I have my own money. They are the ones who are after us.
Interviewer: What did you notice with regard to your parents?
Rabia: They say we don’t have to sleep with men for money: ‘You now have your own money. Make an effort to have much more to avoid pregnancy, HIV, and to continue to study.’
Interviewer: So, you used to date many men in search for money?
Rabia: (laughs) Just a little, auntie.
(Rabia, 18 years, Time 1)
Fewer respondents described girls being economically self-sufficient at Time 2, over one year after the intervention and its small business component ended in most communities. Although some girls described being able to continue with their businesses, others relied on family members for financial support (see below) or, in the case of one girl, married a man ‘for love’ who was also able to provide financial support.
Five girls with ‘reduced risk’ were described as avoiding risk behaviours at Time 2 because they were particularly motivated to achieve their goals or determined to avoid HIV or pregnancy. In some cases, respondents described girls working hard and being determined to expand their small businesses after the intervention ended. Saquina’s uncle, for example, stated that, ‘Her worry now is to do business, prepare her business. In the morning she goes to school and in the afternoon when she goes back home, she takes her products to sell’ (Aderito, Saquina’s uncle, older, Time 2). In other cases, girls’ motivation and determination related more directly to their desire to avoid marriage or sexual partners; some of these described having negative experiences with sexual partners at or before Time 1 which had shaped their determination to avoid men and dating at Time 2. One adolescent girl, Rabia, stated that, ‘I am no longer a little girl to be mistreated by men’, and highlighted how her negative experience with a previous partner had caused her to change her attitudes towards relationships:
Ma’am, I used to be with the father of my son all the time. […] He used me, got me pregnant, and abandoned me with a child in my hands. I stopped going to school, and now I am here at home, not studying. Now I don’t date anybody. (Rabia, 18 years, Time 2)
Other girls and their salient references described girls were previously ‘abandoned,’ ‘deceived’ or ‘mistreated’ by their partners. Similarly, some girls described that their experiences of having an unintended pregnancy made them determined to use condoms consistently with sexual partners and decline sex with men unwilling to use condoms. One girl, for example, described that, ‘I never thought that I would become pregnant so soon, I had sex without a condom and I became pregnant but I did not expect it, nor did I want a child so early. It happened, for that reason I will use it (a condom) in the future for it not to happen again’ (Abelina, 18 years, Time 2).
Notably, simply possessing negative attitudes towards men, sex, or dating did not seem to be sufficient to protect girls from re-engaging in risk behaviours. Girls who avoided risk behaviours for these reasons were also described as either economically self-sufficient or receiving financial support from family members.
Interpersonal level
At the interpersonal level, inequitable relationships with husbands and other sexual partners served as a barrier to reducing sexual risk behaviours while financial support from extended family members facilitated risk reduction.
Several of the girls who had continued risk had inequitable relationships with their husbands or were unable to use condoms within their marriages, according to girls and their salient references. Despite girls’ knowledge of and desire to use condoms, their use was limited by their husbands’ preferences and local norms against using condoms while married; some explicitly stated that their husbands refused to use condoms. All six girls who described not using condoms were also married and stated that they did not use condoms (or used them very infrequently) because their husbands do not ‘accept’ using condoms, or expressed that using a condom with their husband would be distrustful or ‘abusive’:
My thoughts on condoms have not changed, I know that it’s for our protection against HIV/AIDS and other sexually transmitted diseases. Just my husband doesn’t accept it anymore, we used it 2 or 3 times and he doesn’t accept it anymore. He says that he can just use it with a whore that he finds on the street. (Yadira, 18 years, Time 2)
Interestingly, one girl was married and had an extramarital partner and stated that although she did not use condoms with her husband, she used them ‘every time’ with her other partner. Among girls who were not married, condom use was similarly inconsistent, but girls provided little information as to their reasons for infrequent condom use. Two girls experienced physical and emotional gender-based violence from their husbands; although both girls described these marriages as ones of love and mutual interest rather than financial necessity at Time 1, by Time 2 they and their salient references stated that the husbands had developed controlling behaviour and had ‘beaten’ and ‘insulted’ the girls.
Household level
At the household level, all girls with continued risk came from households that were unable to provide for girls’ basic needs and educational expenses, which often drove girls to engage in transactional sex and early marriage as alternative sources of financial support. In contrast, most girls with reduced risk behaviours received support from household members to continue their businesses, support their everyday needs, and continue their education, which facilitated avoiding sexual risk behaviour.
Respondents in all 10 of the continued risk clusters described how girls’ households were unable to afford basic necessities. Many respondents stated that girls’ households lacked food or clothing; or had household heads who were older, had died, or had become sick during the study period, which had negative economic repercussions for the entire household.
I don’t do any business anymore and my father doesn’t do anything, he is sick. My mother can’t work at the farm anymore because of her age. We have no way to live, all we do is suffer. (Kiri, 18 years, Time 1)
Eight of the 10 girls were single or double orphans or lived with extended family members; these girls described a particularly severe lack of resources. Some girls described that their households became more impoverished after a parent died or that their surviving parent struggled to provide for their family, while those living with extended family often found their households lacked sufficient resources to provide for them. One girl’s head of household, her grandmother, stated that ‘she is an orphan and came to live with me, her grandmother, and I have nothing, I can’t afford to buy her anything’ (Themba, Blessing’s grandmother, head of household, older, Time 1). In some households, economic instability was compounded by an unusually severe drought that occurred in some regions at Time 2.
A lack of household economic resources was frequently linked to girls’ engagement in transactional sex prior to Time 1, and girls and their salient references often described girls engaging in transactional sex because they lacked basic necessities, particularly school supplies or uniforms. Similarly, among the girls who got married between Times 1 and 2, nearly all described getting married earlier than they had intended or earlier than the age they stated was ideal for marriage. They described doing so because of their worsening economic status after the end of the intervention.
I got married before I was 18 years old because my father died … I’m very sad. My sister and I stopped studying because we don’t have anything, my mother is not able to buy clothes and notebooks because she also doesn’t have anything. When she goes to the farm is just for us to eat; all the plans I had went under. (Yadira, 18 years, Time 2)
Respondents related to seven of the 10 girls with reduced risk described how girls received support from family members at one or both time points; respondents’ descriptions most often included financial resources but also included encouragement and helping girls prepare products to sell. Respondents typically described girls’ fathers, other heads of households, and male extended family members giving girls money for their basic needs; in cases where a girl’s household economic status was especially poor, uncles and cousins often served as alternative sources of support. One adolescent girl described how her family would be able to provide financial support to her if her savings from her small business were to run out, protecting her from an early marriage:
I don’t think about getting married early because I want to study first and only get married when I’m a grown up. I still have my money to buy my school supplies, and even if I didn’t have money my parents would sell corn and beans to buy books for us. (Abelina, 15 years, Time 1)
Her father similarly described providing financial support for her to do a small business venture prior to Time 1, stating that, ‘before she had her money, I would give her money here at home to also do business, and when the programme appeared, she continued to do business.’ (Faizal, Abelina’s father, head of household, adult, Time 1).
Four girls with reduced risk described receiving significant support from their households specifically to continue with their education, such as living with grandparents or cousins in neighbouring communities to attend school, moving with their parents or receiving money for school fees. Respondents described how this support allowed girls to fulfil their goals of staying in school and attending secondary school and higher education, which often was described as prohibitively expensive for other adolescent girls. In one case, a girl was economically self-sufficient at Time 2, and a cousin stated that both she and her father (the girl’s uncle) encouraged the girl to continue with school and stated that ‘Father tells her ‘You have to keep going to school, you can’t stop going to school’‘(Delma, Lidia’s cousin, head of household, adult, Time 2). For others, girls’ ability to remain in school was contingent on their households’ ability to provide economic support. For example, Nura’s cousin described that her mother was unable to support her living in another city to attend school: ‘She travelled to [city name] and stayed there for one month. She lived with a cousin. She went there to study because her mom could not afford her going to school, but she ended up coming back’ (Luis, Nura’s cousin, influential male, adult, Time 2). Although girls and their salient references did not explicitly say that girls’ school attendance reduced their risk behaviour, these adolescent girls stand in direct contrast to the continued risk girls who lacked household support and got married or engaged in transactional sex to pay for their educational expenses.
Community level
Although few community-level differences emerged in this analysis, distance to and cost of secondary education were often driving factors for engagement in sexual risk behaviour among girls with continued risk who had lower household-level financial resources. The economic hardship experienced by these girls’ families sometimes compounded with the distance to and cost of attending secondary education for girls that finished primary school. In some cases, this drove some girls to get married before they wanted or intended to. Primary education was typically available within girls’ communities but attending secondary school required girls in some communities to travel long distances or to move to larger cities. Two girls described getting married with the intent to receive financial support to attend secondary school, and their salient references confirmed that girls and their households lacked the economic resources to provide for girls’ education. At Time 2, one adolescent girl described recently getting married when she was 15 due to financial need as well as her desire to continue with her education, stating that, ‘I rushed to get married before 18 years old because I have no means, and I married my husband to help me so I wouldn’t give up studying’ (Ernestina, 15 years). This same respondent also described that she now rented a house with her husband in another community so that she could continue attending school and that her husband, although only one year her senior, refused to use condoms.
Discussion
In this sample, adolescent girls’ HIV-related sexual risk behaviours were largely influenced by interpersonal- and household-level factors beyond their immediate control, indicating that young women in this setting are still largely dependent upon and influenced by their families and social relationships. Household-level economic status, equitability of relationships with sexual partners and support from immediate and extended family members all occurred within a broader resource-poor context with limited access to secondary education and inequitable gender norms that reinforced girls’ reliance on sexual risk behaviours to meet their basic financial needs. Research among adolescent girls elsewhere in Mozambique has found that similar factors are associated with girls’ ability to refuse condom-less sex (Underwood and Schwandt Citation2016), negotiation power in relationships (Machel Citation2001) and dependence on sexual partners. Employing a social ecological framework to the analysis demonstrated that although structural factors such as a lack of infrastructure and widespread poverty were rarely acknowledged as drivers of girls’ risk behaviour, they clearly were responsible for many of the household- and community-level factors that influenced girls’ behaviour, such as household economic status and accessibility to secondary education. Policies and programmes that aim to effect and sustain individual-level behaviour change must adequately consider and address these broader influences on the structural level, rather than placing the onus on individuals or households to change within a highly constrained environment.
Married adolescent girls were overwhelmingly categorised as continued risk, and marriage, family support, school attendance and risk behaviours were often interrelated. Married girls and young women frequently had reduced ability to negotiate condom use compared to their unmarried counterparts, received less financial support from family members once married, and were unable to continue attending school. Other research has similarly found that marriage or cohabitation was a leading reason for girls dropping out of school in Mozambique (Lloyd and Mensch Citation2008). Although respondents in this study did not always describe girls’ school enrolment as directly related to their risk behaviour, girls who did not receive financial support from family to attend school often married earlier than they intended or wanted or engaged in transactional sex to pay for school-related necessities and stay in school. Multiple studies have identified marriage as a risk factor for HIV among adolescent girls and young women and attributed this increased risk to age disparities, barriers to negotiating condom use and frequency of sex, sexual debut and husbands’ extramarital partners (Clark, Bruce, and Dude Citation2006; Glynn et al. 2001; Kelly et al. Citation2003). Although girls in this study often sought marriage to gain financial support, once married they paradoxically were limited in their ability to reduce their sexual risk behaviours due to these social and structural factors. Given the marked differences between married and unmarried adolescent girls in this sample, and the unique barriers that married adolescents faced in reducing risk behaviours, future research and interventions targeting married adolescent girls as well as their husbands and communities is warranted.
Girls who reduced HIV-related sexual risk behaviours over time sometimes received additional economic support from the extended family, typically uncles or male cousins who gave girls money for school fees, supplies or basic needs. This type of economic support was not described among girls who continued to be at risk and may indicate that families with broader networks of available resources may be better equipped to support vulnerable (particularly orphaned) adolescent girls and young women, thus potentially reducing their need to rely on transactional sex or marriage for financial reasons. Although girls’ determination and motivation to continue their small businesses or avoid HIV sometimes enabled them to reduce or avoid risk behaviours, the impact of these individual-level factors was contingent upon girls’ economic self-sufficiency or their households’ ability to provide financial support. Interventions to improve household-level economic security may increase the impact of HIV prevention interventions in these settings. Cash transfers, for example, have shown promise in reducing HIV infections among adolescent girls and young women in sub-Saharan Africa and warrant further exploration (Pettifor et al. Citation2012; Baird et al. Citation2012). Similarly, interventions that aim to reduce HIV risk by providing social services and leveraging social protection may be particularly beneficial to adolescents with limited household resources (Cluver, Orkin, Meinck, et al. Citation2016; Cluver, Orkin, Yakubovich, et al.. 2016).
Strengths and limitations
Strengths of this analysis include the novel use of clustered, longitudinal qualitative data to explore multi-level factors and changes over time. This approach produced rich, contextual information on factors related to sexual risk reduction and achieved saturation for all emergent thematic narratives. Agreement between salient references and with each adolescent girl was high and respondents rarely contradicted themselves (within an interview) or each other (within a cluster) regarding the topics of interest in this analysis.
Salient references were often girls’ primary sources of support and this analysis was significantly strengthened by their inclusion. In other settings, it may be unusual to find adult salient references who are as knowledgeable of an adolescent girls’ relationships and sexual behaviours. In these small communities that espouse rigid gender norms, girls’ behaviour is often under scrutiny and heads of household and male relatives often had direct knowledge or could infer girls’ behaviour (i.e. seeing girls spending time with men in local markets, leaving the home at night, a boyfriend introducing himself to a head of household).
The use of multiple respondents and repeated interviews over time also helped identify responses that may have been influenced by social desirability bias. For example, some girls initially stated that they had never had sex or chose not to answer questions about their sexual activity at Time 1, but by Time 2 were more open with interviewers and described their prior engagement in transactional sex. The few instances of contradictions or mixed information within a cluster were noted to avoid misinterpretation of data; these instances did not weaken the analysis because multiple other respondents were able to provide information about a particular girl’s behaviour. Comparative analysis approaches are not commonly used in HIV prevention research, but the findings here demonstrate their utility, particularly for research on the interpersonal and household levels. This approach may be particularly salient when comparing related respondents’ answers to sets of questions or when investigating topics that may be less socially acceptable for discussion, such as sexual behaviour.
Limitations include the fact that although all interview guides included questions about girls’ sexual activity, attitudes towards dating, sex and marriage, and experience doing small business activities at both time points, not all respondents were asked every interview question consistently or were consistently probed for greater detail. Data on emergent factors such as household-level financial support were not included in interview guides and analysis relied on information volunteered spontaneously. Social desirability bias may additionally have influenced respondents’ responses, particularly given that prevailing gender norms highly stigmatise sexual activity among unmarried girls, which sometimes resulted in girls and salient references using ambiguous language to describe sexual behaviours and may have influenced the way that respondents described girls’ sexual behaviours. The intervention that girls participated in also included information on HIV-related sexual risk behaviours; girls and salient references may have overstated reductions in girls’ risk behaviours due to this information, the desire to reflect positively on the intervention, or to encourage its return to their communities. However, the fact that the same interviewers conducted interviews with respondents at both time points appeared to help build rapport and encourage respondents to speak more honestly.
Conclusion
Taken together, findings from this study provide a context-specific understanding of the complexities of HIV-related sexual risk behaviours among adolescent girls in a rural area of Mozambique. They also provide support for the broader evidence that adolescent girls are particularly and uniquely vulnerable to HIV due to diverse individual, social, and structural factors. The factors identified, and their influence on risk behaviours may be transferable to other similar settings.
Appendix 2.docx
Download MS Word (20.7 KB)Appendix 1.docx
Download MS Word (20.2 KB)Disclosure statement
The authors have no conflicts of interest to declare.
References
- Agnarson, A. M., S. Stromdahl, F. Levira, H. Masanja, and A. E. Thorson. 2015. “Female-Driven Multiple Concurrent Sexual Partnership Systems in a Rural Part of a Southern Tanzanian Province.” PLoS One 10 (12): e0145297. doi:10.1371/journal.pone.0145297
- Ayres, L., K. Kavanaugh, and K. A. Knafl. 2003. “Within-Case and across-Case Approaches to Qualitative Data Analysis.” Qualitative Health Research 13 (6): 871–883. doi:10.1177/1049732303013006008
- Baez Ramirez, J. E., G. D. Caruso, C. Niu, and C. A. Myers. 2018. Strong but Not Broadly Shared Growth: Mozambique Poverty Assessment. Washington, D. C.: World Bank.http://documents.worldbank.org/curated/en/248561541165040969/pdf/Mozambique-Poverty-Assessment-Strong-But-Not-Broadly-Shared-Growth.pdf
- Bagnol, B. 2013. “Female Initiation Rituals and Sexualities in Northern Mozambique.” In The Essential Handbook of Women’s Sexuality, edited by D. Castañeda, 143–165. Santa Barbara: ABC-CLIO.
- Baird, S. J., R. S. Garfein, C. T. McIntosh, and B. Ozler. 2012. “Effect of a Cash Transfer Programme for Schooling on Prevalence of HIV and Herpes Simplex Type 2 in Malawi: A Cluster Randomised Trial.” The Lancet 379 (9823): 1320–1329. doi:10.1016/S0140-6736(11)61709-1
- Bandali, S. 2011a. “Exchange of Sex for Resources: HIV Risk and Gender Norms in Cabo Delgado, Mozambique.” Culture, Health & Sexuality 13 (5): 575–588. doi:10.1080/13691058.2011.561500
- Bandali, S. 2011b. “Norms and Practices within Marriage Which Shape Gender Roles, HIV/AIDS Risk and Risk Reduction Strategies in Cabo Delgado, Mozambique.” AIDS Care 23 (9): 1171–1176.
- Bandali, S. 2013. “HIV Risk Assessment and Risk Reduction Strategies in the Context of Prevailing Gender Norms in Rural Areas of Cabo Delgado, Mozambique.” Journal of the International Association of Providers of AIDS Care (JIAPAC) 12 (1): 50–54.
- Bandali, S. 2014. “Women Living with HIV in Rural Areas. Implementing a Response Using the HIV and AIDS Risk Assessment and Reduction Model.” Clinical Medicine Insights. Women's Health 7: 25–35. doi:10.4137/CMWH.S11071
- Bazeley, P. 2013. “Comparative Analysis as a Means of Furthering Analysis.” In Qualitative Data Analysis: Practical Strategies, edited by P. Bazeley, 254–281. Thousand Oaks, CA: SAGE.
- Bekker, L.-G., and S. Hosek. 2015. “HIV and Adolescents: Focus on Young Key Populations.” Journal of the International AIDS Society 18 (2 Suppl 1): 20076. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4581085/ doi:10.7448/IAS.18.2.20076
- Burke, H. M., C. Packer, L. González-Calvo, K. Ridgeway, R. Lenzi, A. F. Green, and T. D. Moon. 2019. “A Longitudinal Qualitative Evaluation of an Economic and Social Empowerment Intervention to Reduce Girls’ Vulnerability to HIV in Rural Mozambique.” Evaluation and Program Planning 77 (2019): 101682. doi:10.1016/j.evalprogplan.2019.101682
- Burke, H. M., C. Packer, L. González-Calvo, S. Field, M. Eichleay, K. Ridgeway, et al. 2017. “Final Report: A Mixed Methods Evaluation of a Social and Economic Empowerment Intervention to Reduce Adolescent Girls’ Vulnerability to HIV in Zambézia Province, Mozambique.” Durham: FHI 360.
- Clark, S. 2004. “Early Marriage and HIV Risks in Sub‐Saharan Africa.” Studies in Family Planning 35 (3): 149–160. doi:10.1111/j.1728-4465.2004.00019.x
- Clark, S., J. Bruce, and A. Dude. 2006. “Protecting Young Women from HIV/AIDS: The Case against Child and Adolescent Marriage.” International Family Planning Perspectives 32 (02): 079–088. doi:10.1363/3207906
- Cluver, L. D., F. M. Orkin, A. R. Yakubovich, and L. Sherr. 2016. “Combination Social Protection for Reducing HIV-Risk Behavior among Adolescents in South Africa.” Journal of the Acquired Immune Deficiency Syndromes 72 (1): 96–104. doi:10.1097/QAI.0000000000000938
- Cluver, L. D., F. M. Orkin, F. Meinck, M. E. Boyes, and L. Sherr. 2016. “Structural Drivers and Social Protection: Mechanisms of HIV Risk and HIV Prevention for South African Adolescents.” Journal of the International AIDS Society 19 (1): 20646. doi:10.7448/IAS.19.1.20646
- Davidoff-Gore, A. 2011. “Dimensions of Poverty and Inconsistent Condom Use among Youth in Urban Kenya.” AIDS Care 23 (10): 1282–1290. doi:10.1080/09540121.2011.555744
- Dellar, R. C., S. Dlamini, and Q. A. Karim. 2015. “Adolescent Girls and Young Women: Key Populations for HIV Epidemic Control.” Journal of the International AIDS Society 18 (2 Suppl 1): 19408. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4344544/ doi:10.7448/IAS.18.2.19408
- Dunkle, K. L., R. K. Jewkes, H. C. Brown, G. E. Gray, J. A. McIntryre, and S. D. Harlow. 2004. “Gender-Based Violence, Relationship Power, and Risk of HIV Infection in Women Attending Antenatal Clinics in South Africa.” The Lancet 363 (9419): 1415–1421. doi:10.1016/S0140-6736(04)16098-4
- Glynn, J. R., M. Caraël, B. Auvert, M. Kahindo, J. Chege, R. Musonda, F. Kaona, and A. Buvé. and Study Group on the Heterogeneity of HIV Epidemics in African Cities. 2001. “Why Do Young Women Have a Much Higher Prevalence of HIV than Young Men? a Study in Kisumu, Kenya and Ndola, Zambia.” AIDS 15: S51–S60. doi:10.1097/00002030-200108004-00006
- Harper, G. W., A. J. Riplinger, L. C. Neubauer, A. G. Murphy, J. Velcoff, and A. K. Bangi. 2014. “Ecological Factors Influencing HIV Sexual Risk and Resilience among Young People in Rural Kenya: Implications for Prevention.” Health Education Research 29 (1): 131–146. doi:10.1093/her/cyt081
- Hendriksen, E. S., A. Pettifor, S. J. Lee, T. J. Coates, and H. V. Rees. 2007. “Predictors of Condom Use among Young Adults in South Africa: The Reproductive Health and HIV Research Unit National Youth Survey.” American Journal of Public Health 97 (7): 1241–1248. doi:10.2105/AJPH.2006.086009
- Instituto Nacional Saúde, Instituto Nacional Estatística, ICF Internacional. 2015. Inquérito de Indicadores de Imunização, Malária e HIV/SIDA em Moçambique 2015. Relatório Preliminar de Indicadores de HIV. Maputo, Moçambique. Rockville, USA: INS, INE e ICF.
- Jewkes, R. K., K. Dunkle, M. Nduna, and N. Shai. 2010. “Intimate Partner Violence, Relationship Power Inequity, and Incidence of HIV Infection in Young Women in South Africa: A Cohort Study.” The Lancet 376 (9734): 41–48. doi:10.1016/S0140-6736(10)60548-X
- Jewkes, R., and R. Morrell. 2010. “Gender and Sexuality: Emerging Perspectives from the Heterosexual Epidemic in South Africa and Implications for HIV Risk and Prevention.” Journal of the International AIDS Society 13 (1): 6–6. doi:10.1186/1758-2652-13-6
- Kelly, R. J., R. H. Gray, N. K. Sewankambo, D. Serwadda, F. Wabwire-Mangen, T. Lutalo, and M. J. Wawer. 2003. “Age Differences in Sexual Partners and Risk of HIV-1 Infection in Rural Uganda.” Journal of the Acquired Immune Deficiency Syndromes 32 (4): 446–451. doi:10.1097/00126334-200304010-00016
- Leclerc-Madlala, S. 2008. “Age-Disparate and Intergenerational Sex in Southern Africa: The Dynamics of Hypervulnerability.” AIDS 22 (Suppl 4): S17–S25. doi:10.1097/01.aids.0000341774.86500.53
- Lenzi, R., C. Packer, K. Ridgeway, T. D. Moon, A. F. Green, L. González-Calvo, and H. M. Burke. 2019. “Exploring Intersections of Localised Gender Norms and Unanticipated Effects of a Sexual and Reproductive Health Intervention: Implications of respect and Being a “Good Girl” in Zambézia Province, Mozambique.” Culture, Health & Sexuality 21 (5): 575–590. doi:10.1080/13691058.2018.1498540
- Lloyd, C. B., and B. S. Mensch. 2008. “Marriage and Childbirth as Factors in Dropping out from School: An Analysis of DHS Data from Sub-Saharan Africa.” Population Studies 62 (1): 1–13. doi:10.1080/00324720701810840
- Machel, J. Z. 2001. “Unsafe Sexual Behaviour among Schoolgirls in Mozambique: A Matter of Gender and Class.” Reproductive Health Matters 9 (17): 82–90. doi:10.1016/S0968-8080(01)90011-4
- Macia, M.,. P. Maharaj, and A. Gresh. 2011. “Masculinity and Male Sexual Behaviour in Mozambique.” Culture, Health & Sexuality 13 (10): 1181–1192. doi:10.1080/13691058.2011.611537
- Makusha, T., and L. Richter. 2016. “Gatekeeping and Its Impact on Father Involvement among Black South Africans in Rural Kwazulu-Natal.” Culture, Health & Sexuality 18 (3): 308–320. doi:10.1080/13691058.2015.1083122
- McLeroy, K. R., D. Bibeau, A. Steckler, and K. Glanz. 1988. “An Ecological Perspective on Health Promotion Programs.” Health Education Quarterly 15 (4): 351–377. doi:10.1177/109019818801500401
- Parkes, J., J. Heslop, F. Januario, S. Oando, and S. Sabaa. 2016. “Between Tradition and Modernity: Girls’ Talk about Sexual Relationships and Violence in Kenya, Ghana and Mozambique.” Comparative Education 52 (2): 157–176. doi:10.1080/03050068.2016.1142741
- Pettifor, A. E., A. Van Der Straten, M. S. Dunbar, S. C. Shiboski, and N. S. Padian. 2004. “Early Age of First Sex: A Risk Factor for HIV Infection among Women in Zimbabwe.” AIDS 18 (10): 1435–1442. doi:10.1097/01.aids.0000131338.61042.b8
- Pettifor, A., C. MacPhail, N. Nguyen, and M. Rosenberg. 2012. “Can Money Prevent the Spread of HIV? a Review of Cash Payments for HIV Prevention.” AIDS & Behavior 16 (7): 1729–1738. doi:10.1007/s10461-012-0240-z
- Pons-Duran, C., R. Gonzalez, L. Quinto, K. Munguambe, J. Tallada, D. Naniche, C. Sacoor, and E. Sicuri. 2016. “Association between HIV Infection and Socio-Economic Status: Evidence from a Semirural Area of Southern Mozambique.” Tropical Medicine & International Health 21 (12): 1513–1521. doi:10.1111/tmi.12789
- Psaros, C., C. Milford, J. A. Smit, L. Greener, N. Mosery, L. T. Matthews, A. Harrison, et al. 2017. “HIV Prevention among Young Women in South Africa: Understanding Multiple Layers of Risk.” Archives of Sexual Behavior 47 (7): 1969–1982. doi:10.1007/s10508-017-1056-8
- QSR. 2015. Nvivo Qualitative Data Analysis Software. Doncaster., Australia: QSR International Pty Ltd.
- Ranganathan, M., C. MacPhail, A. Pettifor, K. Kahn, N. Khoza, R. Twine, C. Watts, and L. Heise. 2017. “Young Women’s Perceptions of Transactional Sex and Sexual Agency: A Qualitative Study in the Context of Rural South Africa.” BMC Public Health 17 (1): 666. doi:10.1186/s12889-017-4636-6
- Schaefer, R., S. Gregson, J. W. Eaton, O. Mugurungi, R. Rhead, A. Takaruza, R. Maswera, and C. Nyamukapa. 2017. “Age-Disparate Relationships and HIV Incidence in Adolescent Girls and Young Women: Evidence from Zimbabwe.” AIDS 31 (10): 1461–1470. doi:10.1097/QAD.0000000000001506
- Skinner, J., C. Underwood, H. Schwandt, and A. Magombo. 2013. “Transitions to Adulthood: Examining the Influence of Initiation Rites on the HIV Risk of Adolescent Girls in Mangochi and Thyolo Districts of Malawi.” AIDS Care 25 (3): 296–301. doi:10.1080/09540121.2012.701721
- UNAIDS. 2015a. “Leaders from Around the World Are All in to End the AIDS Epidemic Among Adolescents.” http://www.unaids.org/en/resources/presscentre/pressreleaseandstatementarchive/2015/february/20150217_PR_all-in
- UNAIDS. 2015b. “AIDSInfo Map.” http://aidsinfo.unaids.org/
- UNAIDS. 2019. “All In to #EndAdolescentAIDS.” UNAIDS, Accessed January 5, 2018. http://www.unaids.org/sites/default/files/media_asset/20150217_ALL_IN_brochure.pdf
- Underwood, C. R., and H. M. Schwandt. 2016. “Assessing Girls’ HIV Vulnerability: Evidence from Botswana, Malawi and Mozambique.” Health Policy and Planning 31 (6): 729–735. doi:10.1093/heapol/czv123
- Underwood, C., and H. M. Schwandt. 2015. “Community Support and Adolescent Girls’ Vulnerability to HIV/AIDS: Evidence from Botswana, Malawi, and Mozambique.” International Quarterly of Community Health Education 35 (4): 317–334. doi:10.1177/0272684X15592762
- Underwood, C., J. Skinner, N. Osman, and H. Schwandt. 2011. “Structural Determinants of Adolescent Girls’ Vulnerability to HIV: Views from Community Members in Botswana, Malawi, and Mozambique.” Social Science & Medicine 73 (2): 343–350. doi:10.1016/j.socscimed.2011.05.044
- UNDP. 2016. “Human Development Report 2016: Human Development for Everyone.” New York, NY: United Nations Development Programme. http://hdr.undp.org/sites/default/files/2016_human_development_report.pdf
- UNICEF. 2016a. “For every child, end AIDS - Seventh Stakeholding Report.” New York, NY. http://st7.childrenandaids.org/sites/default/files/STR%202016%20Report%2012_9%20LR_.pdf
- UNICEF. 2016b. “Turning the Tide Against AIDS Will Require More Concentrated Focus on Adolescents and Young People.” Accessed November 23 2016. https://data.unicef.org/topic/hivaids/adolescents-young-people/#
