
Abstract
Shared decision making is a collaborative process intended to develop a treatment plan that considers both the patient’s preferences and the health provider’s medical recommendations. It is one approach to reducing healthcare disparities by improving patient-provider communication and subsequent health outcomes. This study examines shared decision making about HIV pre-exposure prophylaxis (PrEP) with Black transgender women in Chicago, Illinois, USA, given high prevalence of HIV and disparities in PrEP use. Black transgender women were recruited online and in-person to participate in semi-structured interviews (n = 24) and focus groups (2; n = 14 total), conducted between 2016 and 2017. Iterative thematic content analysis took place. Analysis revealed that internalised transphobia and racism, combined with stigma from service providers, prevented disclosure of gender and sexual identity to providers. Stigma about PrEP as it relates to Black transgender women results in stereotype threat, which undermines patient-provider trust and deters shared decision making for PrEP. Shared decision making promotes cultural competence and humility and builds trust within the patient-provider relationship, leading to better communication and less stigma. The involvement of peers may be one way to mitigate stigma for Black transgender women around PrEP, promote cultural competence within organisations, and empower engagement in shared decision making for HIV prevention.
Introduction
Black transgender women face many health disparities, most glaringly seen in high rates of HIV transmission. In the USA, transgender women of all racial/ethnic backgrounds are estimated to have approximately 22% community prevalence of HIV (Baral et al. Citation2013). A meta-analysis of studies published from 2006-2017 reported that Black transgender women had a significantly higher HIV prevalence estimate of 44.2% (95% CI 23.2, 67.5) compared to white transwomen and those of other races/ethnicities (Becasen et al. Citation2019). Relatedly, an analysis of data from the National HIV Surveillance System revealed that Black transgender women accounted for 51% (n = 1002/1974) of all new HIV diagnoses among transgender women in the USA between 2009-2014 (Clark et al. Citation2017).
Intersectionality theory posits that multiple systems of social stratification interact to affect an individual’s experiences, leading to compounded social advantage or disadvantage within a matrix of domination: a system of interwoven mechanisms for social stratification and oppression (e.g. racism, sexism, homophobia, transphobia) with broad downstream impact on life outcomes, including health (Peek et al. Citation2016; Crenshaw Citation1991; Institute of Medicine Citation2011; Crenshaw Citation1995). In a society marked by pervasive racism and structured around heterosexual, cisgender norms, Black transgender women are a multiply marginalised group as the result of intersecting social positions: race, gender/gender identity, and sometimes sexual orientation and class. Black transgender women experience multi-faceted oppression underscored by the interrelated factors contributing to HIV incidence. These include social factors (e.g. sexual networks); behavioural factors (e.g. condomless anal intercourse, sex work); and structural factors (e.g. systemic racism, discrimination, socioeconomic status, underemployment, incarceration) (Grant et al. Citation2011; Ezell et al. Citation2018; Denson et al. Citation2017; Herbst et al. 2008; Nemoto et al. Citation2004; Poteat et al. Citation2017; Brennan et al. Citation2012).
While not a solution to the underlying factors contributing to HIV transmission, HIV pre-exposure prophylaxis (PrEP) is effective at reducing incidence of HIV in transgender persons but is highly dependent on uptake and adherence (Grant et al. 2014; Deutsch et al. Citation2015), and has been underutilised by transgender people (Sevelius et al. Citation2020). As with many medical advances, PrEP too has been plagued by disparities across race/ethnicity and gender, with the majority of prescriptions being provided to white men as compared to Black men and women (Huang et al. Citation2018). Understanding the full extent of HIV- and PrEP-related disparities in Black transgender women and the contributing elements is difficult since Black transgender women are underrepresented in HIV research. Furthermore, Black- and transgender-specific results have often been aggregated with those of Black men who have sex with men or across transwomen of all racial/ethnic backgrounds, which does not allow us to delve into their intersectional nature (Sevelius et al. Citation2016; Poteat et al. Citation2019). Despite gaps, there are important details to be gleaned from the literature on this topic.
Previous studies have shown that transgender women, including transwomen of colour, are interested in using biomedical interventions such as PrEP (Golub et al. Citation2013; Sevelius et al. Citation2016; Poteat et al. Citation2019). A recent study among 201 Black and Latina transgender women found that 87% had heard of PrEP but only 17% of those aware had ever taken it, despite 75% of HIV negative participants citing willingness to take PrEP (Poteat et al. Citation2019). Barriers included concern about drug interactions with hormone therapy, medical mistrust, PrEP stigma and side effects (Poteat et al. Citation2019). Other challenges cited are low awareness of PrEP and lack of perceived benefit of taking PrEP (Kuhns et al. Citation2016; Garnett et al. Citation2018; Brooks et al. Citation2019; Klein and Golub Citation2019), as well as limited provider knowledge and comfort in prescribing PrEP, and provider bias (Petroll et al. Citation2017; Krakower et al. Citation2017; Marcus et al. Citation2019). Conversely, facilitators of PrEP uptake have included free or low-cost PrEP and sexual health care, access to counselling and support around PrEP use, and ability to obtain PrEP from a trans-competent provider (Golub et al. Citation2013; Sevelius et al. Citation2016). A qualitative analysis of young multiracial transgender women found that PrEP acceptability was associated with having a provider who met their health needs (Restar et al. Citation2018).
Shared decision making (SDM) is a collaborative process between patients and providers intended to develop a treatment plan that considers both the patient’s needs and preferences and the health provider’s recommendations (Charles, Gafni, and Whelan Citation1997; Barry and Edgman-Levitan Citation2012). SDM has been shown to increase patient satisfaction, adherence to the chosen treatment plan and engagement in care (Stewart Citation1995; Peek et al. Citation2016). It has been identified as a key patient-centred strategy for improving clinical outcomes and reducing healthcare disparities primarily by improving communication and the quality of the patient-provider relationship (King, Eckman, and Moulton Citation2011; Peek et al. Citation2016; Durand et al. Citation2014).
Communication is central to the SDM process yet can contribute to healthcare disparities among marginalised populations (Johnson et al. Citation2004). Transgender persons of colour face widespread discrimination in healthcare ranging from refusal of care to microaggression such as misgendering (Grant et al. Citation2011; Nordmarken and Kelly Citation2014; Hudson Citation2019; Howard et al. Citation2019). In a study of people living with HIV, transgender women (63% of whom were Black) described fewer positive interactions with providers than their non-transgender peers and were less likely to report adherence to antiretroviral medications (Sevelius, Carrico, and Johnson Citation2010). Negative healthcare experiences, compounded by stigma and discrimination within and beyond healthcare settings, lead to poor communication, distrust and avoidance of care, perpetuating health disparities (Li et al. Citation2015; James, Brown, and Wilson Citation2017; Hudson Citation2019).
While SDM has been studied in a variety of populations and conditions, it may be particularly appropriate to use in discussion about PrEP with Black transgender women given the aforementioned disparities. Yet, little is known about SDM for PrEP with patients who identify with multiple socially vulnerable groups (Peek et al. Citation2016; Ng Citation2016). In this study, we aimed to explore perspectives of Black transgender women on SDM about PrEP with their providers, identifying individual, interpersonal, community, and healthcare factors that impact the SDM process, taking into account the intersectional experiences of Black transgender women.
Methods
Conceptual model
The Peek Model for SDM served as the conceptual framework for this study () (Peek et al. Citation2016), guiding qualitative interview guide development and analysis of the results. This model was developed to provide an understanding of SDM with Black lesbian, gay, bisexual, transgender and queer persons () (Peek et al. Citation2016). It has been previously applied to understanding the relationship between intersectionality and SDM for anal cancer screening among Black gay and bisexual men (Acree et al. Citation2019).
Figure 1. Peek Model for Shared Decision Making (Peek et al. Citation2016). This is copyright material reprinted with permission from Springer.
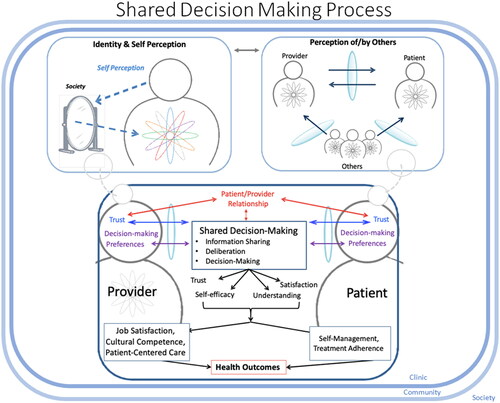
In the Peek Model, the patient, the health provider and their relationship are viewed in multiple ways (Acree et al. Citation2019; Peek et al. Citation2016). The individual level, or the level of self-perception, describes how both the patient and provider view themselves in the context of their identity (e.g. race, ethnicity, sexuality, socioeconomic status) and their lived experiences of social advantage or disadvantage. Perception of and by others outlines the influence of stereotypes, prejudices and implicit biases. Self-perceived identities interact with perception of/by others to influence the patient-provider relationship, occurring within the larger context of community and society (Peek et al. Citation2016).
Engagement in SDM (i.e. information sharing, deliberation, and decision-making) is determined by the patient-provider relationship, mutual trust and decision-making preferences (Peek et al. Citation2016). Downstream effects of successful SDM include self-efficacy, satisfaction, trust and understanding between patient and provider. These lead to improved self-management and treatment adherence for the patient, as well as job satisfaction, cultural competence and ability to provide patient-centred care for the provider (Peek et al. Citation2016). The end result is improved health outcomes for the patient through better care delivery (Acree et al. Citation2019; Peek et al. Citation2016).
Setting and participants
Data were collected in Chicago, Illinois between 2016 and 2017. Participants were recruited through a variety of sources: online advertisements (Facebook), in person at community-based clinics and organisations, and at community events. Participants were eligible if they were English speaking, at least 18 years of age, identified as an African American or Black transgender woman and reported having sex with men within the past two years. Participants were excluded if they did not meet these criteria.
Data collection
We conducted semi-structured individual interviews (n = 24) and focus groups (2; n = 14) between 2016 and 2017. Participants were offered the choice between an individual interview or focus group. Semi-structured qualitative interview guides were developed by the research team – an example is provided in online supplemental material (Appendix A). Questions were designed around the Peek Model for SDM (Peek et al. Citation2016); topics included participants’ identities, disclosure of gender and sexual identities in healthcare settings, healthcare experiences, SDM process for PrEP, and advice for healthcare providers to improve SDM. Community members who identified as transgender women or non-binary persons of colour were recruited and trained to conduct interviews and serve as focus group moderators. Community members piloted the qualitative interview guides and provided feedback, resulting in further edits. Verbal consent was obtained from participants prior to the start of the interview or focus group. Participants also completed a self-administered survey; items included demographics, medical history, and experiences within healthcare. Upon completion of the interview, participants received a US$40 cash stipend and were provided with information on community resources for LGBTQ persons of colour. Interviews and focus groups were audio recorded and professionally transcribed. The Institutional Review Board at the University of Chicago approved the study.
Measures and analysis
Data were analysed using iterative thematic content analysis. Interview transcripts were assessed for themes as they emerged from the text and in relation to the Peek Model for SDM (Peek et al. Citation2016). These themes served as the basis for the initial codebook. Following this process, at least two members of the research team independently coded each transcript. The codebook was updated as new themes emerged, and all transcripts were subsequently re-coded. Any discrepancies in coding were resolved through review of the transcript and discussion until agreement was reached. Data were coded using qualitative data analysis software (Nvivo, Version 11.4.1; QSR International Citation2017). Themes were reviewed for interpretation across transcripts and to identify patterns. Illustrative quotes were chosen.
Results
describes the self-reported sociodemographic characteristics of participants based on survey completion (n = 38). Most participants identified as transgender women (97.4%), while one (2.6%) identified as genderqueer. Of participants who reported employment status, the majority either did not work or worked part time and reported less than US$20,000 annual income (68.4%). Twenty-two (57.9%) participants reported public insurance as their primary health insurance, while an additional ten (26.4%) participants reported no insurance or receiving healthcare at a free or low-cost clinic.
Table 1. Sociodemographic and health characteristics of participants.
In the following sections, we identify themes as they relate to the Peek Model. We present participants’ experiences of social identity/self-perception as a reflection of societal views with impact on healthcare engagement; provider perceptions and anticipated stigma that affect sharing identity; interplay of PrEP stigma with self-perception and perception by others; qualities of the patient-provider relationship that foster SDM for PrEP; and participant preferences for information sharing, deliberation and making decisions about PrEP. In order to protect confidentiality, participants' names used in conjunction with the direct quotes below are pseudonyms.
Social identity and self-perception: intersection of race, gender and sexuality
The Peek Model describes self-perception as a reflection of societal views about one’s identity (Peek et al. Citation2016). Participants described negative messages about their racial and gender identity within society and the communities they identified with:
…there is so much that’s imposed in the community that apparently says that transwomen, black transwomen, are – that there is something wrong with us. You know that there is something about us that needs corrected. And usually the way that they attempt to correct that is by attacking us in some way. Or by forcing us to behave in ways that we might not necessarily want to because that’s what society agrees with…if you’re a Black transwoman in this country it’s hard to feel anything other than like fear, sometimes. (Keyonna, 27 years old)
This same participant described external threats to identity as a result of societal transphobia and racism, which led to internalised stigma. In stating that society ‘forces us to behave in ways that we might not necessarily want…’ Keyonna implied that some behaviours are maladaptive as a result of society’s expectations of who a Black transgender woman is and how she is expected to act, as well as wider societal oppression. Keyonna expressed psychological distress compounded by internalised transphobia, homophobia and racism.
The psychological distress triggered by stigma also occurs within healthcare settings, with deleterious effects on health. Trauma was frequently experienced by participants; in survey responses, 42% of participants reported having been treated differently within a healthcare setting due to transphobia, homophobia or racism (). In the individual interviews, nearly all participants described some form of negative experiences within healthcare related to identity as Black transgender women.
Table 2. Healthcare experiences of participants.
…when I was going through my transition…my first doctor was not pleasant…they barely want to…hold a stethoscope…where they check your heart, breathing and stuff. You know, it’s just like, they come in the room straight automatically with a mask and gloves on…so that made me feel uncomfortable. I actually stopped going to the doctor and taking my meds for about two years. That was hurtful. (Shante, 35 years old)
This same participant, who self-reported as living with HIV, described avoidance of healthcare and decreased adherence to medications after a negative healthcare experience. The resulting psychological distress contributed directly to loss of engagement in care.
Perception of and by others: sharing aspects of identity with providers
Participants described how health provider perceptions of Black transgender women impacted decisions to disclose gender and sexual identities with providers, with occasions where they felt that revelation of their gender identity changed or might have changed a providers’ perception of them.
Well, when I first meet a doctor, I kind of somewhat don’t [disclose my gender identity] …Because sometimes you be wanting the doctor to kind of get the feel of you. Just who you are…Sometimes if you do tell your doctor, he kind of has an eye open of who you are…And sometimes you don’t because you don’t want them to judge you. (Ty, 26 years old)
Some participants avoided transphobia by not disclosing transgender identity until being comfortable with a provider. However, Ty recognised that when a provider was aware of her gender identity, they were able to provide more relevant health information and guidance.
Patient provider communication about sexual identity and practices (i.e. what type of sex, with whom and how often) is part of engaging in SDM for PrEP. Yet, fewer participants had discussed sexual identity and practices with their provider compared to gender identity, and these discussions were considered more difficult: ‘Very awkward. Because I’m very proud of my transness, but I’m very perceptive of how people are going to handle my sexuality’ (Tiffany, 23 years old). Several participants stated that appropriate gendering was more important than sharing their sexual orientation and sexual practices:
And as me being respectful, to let a person that I’m trying to take care of business with, and get my healthcare done with…I told them about me. But to be honest, it’s none of their concern, about my sexual orientation. Only thing that matters is if you get my gender pronoun right. My sexual orientation don’t have nothing to do with it. (Crystal, 24 years old)
PrEP in relation to self-perception and perception of/by others
Participants identified certain aspects of PrEP that impacted SDM, particularly PrEP stigma, relationship of PrEP to other transgender-related health priorities such as hormone replacement therapy, and peer opinions about PrEP. Perceived and anticipated PrEP-related stigma specific to Black transgender women was described:
I think there is just stigma around why Black trans women would want or need PrEP…There is a stigma that like: Oh, you are just going to be sleeping around with everyone… we deal with…this very white Christian idea of what sex is and isn’t and who has the right to have that and when. And so I think there is a lot of…stigma, the culture that says that if someone is taking a medication that makes it easier for them to have safer sex, then they’re a slut…there is just a lot of negative reinforcement around that. (Keyonna, 27 years old)
The interplay between PrEP stigma and self-perception and perception by others affected the patient-provider relationship and SDM process. Some participants described HIV stigma as connected to their Blackness, while others described how providers conflate their identity as a Black transgender women with HIV risk, regardless of behaviour. Reecey (age unknown) described provider assumptions that impacted discussions about PrEP, ‘…You know, because I’m trans, I’m a prostitute. Or because I’m trans…I already got HIV. So, it’s gonna play a part, you know. And I could be one of those who don’t have an STD, or don’t have HIV, but it would be an assumption…’. Another participant, Zella (26 years old) stated ‘…if [Black transgender women] ask for PrEP, the provider will automatically think they’re like a sex worker or like a slut, or something like that’.
SDM for PrEP will remain difficult so long as this stigma exists, yet the use of the SDM may also be a method for reducing stigma around HIV prevention and PrEP:
… if I were a healthcare provider, [I] would be like: ‘Yeah, we should check in with our patients more about those things [HIV risk, HIV prevention, gender identity and sexual orientation] and hopefully that can remove the stigma a little bit’. …if we treat them as very common things that we can take care of because human beings are human beings and this is a part of who they are…then maybe people would want to talk about it more often. (Keyonna, 27 years old)
Routinely engaging in SDM about PrEP can normalise the conversation about HIV prevention, thereby reducing stigma. One participant described her experience with SDM for PrEP as free of perceived racial and transgender bias and stigma, respectful of the individual and of individual autonomy.
I liked the conversation [about PrEP], because it was something that could benefit me for saving myself from going out here to get exposed to HIV…They respected my wishes, my ideas, and my suggestions…They didn’t misgender me. They didn’t treat me like no other type of person. They didn’t racial profile me. (Crystal, 24 years old)
Patient-provider relationship: trust and respect for lived experience
In the Peek Model, the patient-provider relationship is a key component of the SDM process, however racism and transphobia in clinical encounters erode trust. Mistrust was commonly reported by participants; 57.9% of participants said that it prevented them from accessing healthcare, disclosing sexual practices, discussing PrEP, or taking a provider’s recommendations.
Having a provider with similar lived experiences could build trust and facilitate discussion of PrEP. One participant described how having a provider of their same racial/ethnic identity and ideally same gender identity would enable the provider to empathise with her experience:
…they ID as a non-binary person, but they’re also White, so they are not someone who I can really be, or feel, comfortable around… if I want to have these conversations [about PrEP] with a provider…I want that provider to be either Black or of colour to have an open discussion, or like, in a perfect world, to be black and also within the TG or T community…Because, as someone…who is within the community but… hasn’t lived an experience that’s anything close to what I have, they aren’t going to realise…[what] I take with me, and how to handle that. (Tiffany, 23 years old)
Participants also felt that the presence of other Black transgender women working within healthcare settings would create culturally competent environments and encourage rapport.
I think the best way to do that [enable shared decision making for PrEP] is to…have a transgender African American woman working there, volunteering…so they can not only enlighten the staff, but even just make the people that come in, the girls that come in there, feel a little bit more at ease. (Shante, 35 years old)
Yet, cultural competence alone may not be enough. Validation of individual experiences and cultural humility in the form of openness to continuously learning from and about the patient (Tervalon and Murray-Garcia Citation1998; Hook and Davis Citation2017) were seen as important in relationship building.
…at the end of the day, yeah, you [the provider] have this training…this expertise. But if you’re looking at a human being and telling them that the things they feel and experience aren’t valid all the time then they are not going to trust you. There could be things that they don’t know about and it’s your responsibility to inform that patient without contradicting them and making them feel like shit. (Keyonna, 27 years old)
Shared decision-making: preferences for information sharing, deliberation and decision making about PrEP with a provider
Twenty-eight (80%) participants reported having had a conversation about PrEP with a health provider. Most participants preferred information about PrEP be delivered in a one-on-one, face-to-face setting. They also wanted to receive supplemental material.
Well, face-to-face, you can get more understanding, because anything that you don’t understand, they can explain it to you. And then the written material is stuff that you can constantly go back in to check for, like if you forgot something, or something that you didn’t understand, you can go back and research it, or you can go back and review it. (Jasmine, 63 years old)
Participants identified peers as important for disseminating trusted information about PrEP:
…I think it would be a very, very good format to have a panel discussion, and to have your veteran patients up there to be a leeway to the newer patients…I think they’ll receive it [information about PrEP] more from their peers than…they can receive it from the doctor…to have somebody experience what I experience. (Reecey, unknown age)
Several participants reported that the decision-making process for PrEP may continue outside of the clinical encounter or span multiple visits: ‘Normally, [I get information] from my provider… I may not always get the responses that I need to make sound decisions, so that's when that decision is put on hold and is deferred until I can really gather as good of an understanding…’ (Penny, 27 years old)
Finally, this same participant described how information sharing within a collaborative provider-patient partnership supported agency in the decision-making process, thereby also increasing self-efficacy and satisfaction with the treatment decision:
So if you are given more variety of options, you will feel more comfortable even partaking of the medication [PrEP] then. Because you made the decision, or you had the option, and this is what you picked. (Shante, 35 years old)
Discussion
Our study found that Black transgender women face previously documented forms of PrEP- and HIV-related stigma in addition to unique forms of stigma towards their intersectional minority identities. Findings suggest that SDM can serve as a tool for reducing stigma by normalising conversations about HIV prevention and promoting providers’ cultural competence and cultural humility, building trust in the patient-provider relationship.
Participants described stereotype threat in healthcare settings in response to PrEP- and HIV-related stigma as it relates to their intersectional identities as Black transgender women. Previous research has demonstrated that stereotype threat contributes to diminished trust, poor communication, and decreased engagement in healthcare (Burgess et al. Citation2010; Aronson et al. Citation2013), while stereotypes about who needs PrEP (e.g. promiscuous, irresponsible, etc.) are barriers to PrEP use (Quinn, Bowleg, and Dickson-Gomez Citation2019; Jackson et al. Citation2021; Quinn, Dickson-Gomez et al. Citation2019). Ultimately these negative associations result in fewer conversations about PrEP, limiting the use of SDM for patients who may benefit most.
Intersectional stigma uniquely affects Black transgender women’s opportunities to discuss PrEP. Due to intersectional stigma, some Black transgender women may not be comfortable self-identifying as transgender within certain healthcare settings (Iantaffi and Bockting Citation2011). Yet, because providers’ decisions to discuss PrEP are often based on patient membership in certain ‘risk’ groups, this mechanism by which to avoid anticipated stigma from providers may simultaneously reduce the likelihood of providers engaging patients in SDM around PrEP – particularly if providers assume that cisgender women are less likely to benefit from PrEP (Calabrese et al. Citation2019). Furthermore, transgender persons with higher levels of gender nonaffirmation are less likely to use PrEP (Sevelius et al. Citation2020), making it important for providers to create safe spaces in which to freely discuss identity and receive information in a non-judgemental way.
Providers’ assumptions about HIV risk further contribute to the intersectional stigma surrounding PrEP. Multiple studies suggest that discussions about PrEP be incorporated into routine preventive care for all patients, at each encounter (Calabrese, Krakower, and Mayer Citation2017; Quinn, Dickson-Gomez et al. Citation2019; Golub Citation2018). Recent findings identify ‘active provider engagement’, or proactive information-sharing and ongoing conversations about PrEP, to improve interest and use by transgender women, 30% of whom were Black (Klein and Golub Citation2019). Improving communication through SDM may reduce assumptions providers make about Black transgender women, resulting in tailored discussions about PrEP with the potential to reduce stigma. SDM has been associated with lower levels of stigma around mental health conditions and treatment (Butler Citation2014); more research is needed to better understand the role of SDM in stigma reduction for PrEP.
Peer involvement is one method of sharing PrEP information that is particularly relevant to lived experiences of Black transgender women. Peer interventions are important for stigma reduction (Quinn, Bowleg, and Dickson-Gomez Citation2019) and have been used with success for HIV prevention (Kelly Citation2004; Schneider et al. Citation2021). Peer interventions for PrEP that are specific to transgender women are limited (Poteat et al. Citation2017). However, there are successful peer navigation programmes that have included a sample of transgender women of colour (Reback et al. Citation2019). Peer interventions for PrEP specific to Black transgender women should continue to be developed, as should methods for incorporating Black transgender women in the healthcare workforce in all roles to support the provision of gender-affirming healthcare and facilitate SDM (Sullivan Citation2004; Cohen, Gabriel, and Terrell Citation2002).
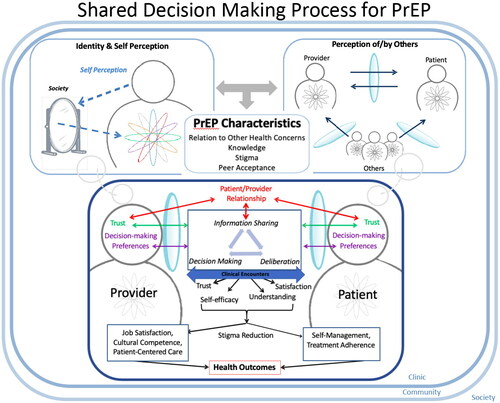
In the light of our experience in this study, we modified the SDM model as depicted in to incorporate findings of importance (). SDM is influenced by identity and self-perception and perception of and by others, but also by characteristics of PrEP including provider and patient knowledge and stigma. The SDM process is displayed as cyclical and longitudinal in nature, which reflects preferences for ongoing discussions around PrEP. In addition to outcomes in the original Peek model, effective SDM contributes to reducing stigma.
Figure 2. Adapted Peek Model for Shared Decision Making for PrEP between Black Transgender Women and Healthcare Providers.
Limitations
This study has several limitations. Participants were recruited from an urban area and organisations that provide gender-affirming care, thus they may have had more opportunities to discuss PrEP than others in rural, suburban or less affirming contexts (Whitehead, Shaver, and Stephenson Citation2016). The study included both HIV positive and negative individuals, however, we did not ask participants to talk about their HIV status or directly ask how their status shaped their views on SDM about PrEP during the qualitative interviews unless initiated by the participant for reasons of confidentiality. Finally, the study did not assess provider perspectives on SDM about PrEP, which is an important component of the interaction.
Conclusion
Shared decision making for PrEP has the potential to reduce HIV-related healthcare disparities for Black transgender women by improving patient-provider interactions and enabling informed health decision making, which are key to improving clinical outcomes. This study provides insight into the compounding barriers that Black transgender women face to engaging in SDM about PrEP, in particular intersectional PrEP- and HIV- related stigma that leads to stereotype threat, diminished trust and engagement. The SDM process for PrEP prioritises patient lived experience and may allow providers to actively ameliorate these barriers by promoting positive, trusting, and empowering patient-provider interactions, in the process reducing stigma. These findings are acutely salient as the USA works towards HIV elimination, which depends on delivering PrEP to the populations most impacted by HIV.
Supplemental Material
Download MS Word (14.5 KB)TCHS-2019-0272-File005.pptx
Download MS Power Point (806.5 KB)Acknowledgements
We thank Your Voice! Your Health! participants for their contribution to this study. We acknowledge Devin Niecy for contributions on transgender health. Morten Group recruited and interviewed participants. We thank members of the Your Voice! Your Health! Study team, particularly those who provided feedback on this manuscript and the principal investigator, Marshall Chin.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Acree, M. E., M. McNulty, O. Blocker, J. Schneider, and H. S. Williams. 2019. “Shared Decision-Making around Anal Cancer Screening among Black Bisexual and Gay Men in the USA.” Culture, Health & Sexuality 22 (2): 201–216.
- Aronson, J., D. Burgess, S. M. Phelan, and L. Juarez. 2013. “Unhealthy Interactions: The Role of Stereotype Threat in Health Disparities.” American Journal of Public Health 103 (1): 50–56.
- Baral, S. D., T. Poteat, S. Strömdahl, A. L. Wirtz, T. E. Guadamuz, and C. Beyrer. 2013. “Worldwide Burden of HIV in Transgender Women: A Systematic Review and Meta-Analysis.” The Lancet Infectious Diseases 13 (3): 214–222.
- Barry, M. J., and S. Edgman-Levitan. 2012. “Shared Decision Making – Pinnacle of Patient-Centered Care.” The New England Journal of Medicine 366 (9): 780–781.
- Becasen, J. S., C. L. Denard, M. M. Mullins, D. H. Higa, and T. A. Sipe. 2019. “Estimating the Prevalence of HIV and Sexual Behaviors among the US Transgender Population: A Systematic Review and Meta-Analysis, 2006-2017.” American Journal of Public Health 109 (1): e1–e8.
- Brennan, J., L. M. Kuhns, A. K. Johnson, M. Belzer, E. C. Wilson, and R. Garofalo. 2012. “Syndemic Theory and HIV-Related Risk among Young Transgender Women: The Role of Multiple, Co-Occurring Health Problems and Social Marginalization.” American Journal of Public Health 102 (9): 1751–1757.
- Brooks, R. A., A. Cabral, O. Nieto, A. Fehrenbacher, and A. Landrian. 2019. “Experiences of Pre-Exposure Prophylaxis Stigma, Social Support, and Information Dissemination among Black and Latina Transgender Women Who Are Using Pre-Exposure Prophylaxis.” Transgender Health 4 (1): 188–196.
- Burgess, D. J., J. Warren, S. Phelan, J. Dovidio, and M. van Ryn. 2010. “Stereotype Threat and Health Disparities: What Medical Educators and Future Physicians Need to Know.” Journal of General Internal Medicine 25 (S2): 169–177.
- Butler, A. M. 2014. “Shared Decision-Making, Stigma, and Child Mental Health Functioning among Families Referred for Primary Care–Located Mental Health Services.” Families, Systems & Health 32 (1): 116–121.
- Calabrese, S. K., D. S. Krakower, and K. H. Mayer. 2017. “Integrating HIV Preexposure Prophylaxis (PrEP) into Routine Preventive Health Care to Avoid Exacerbating Disparities.” American Journal of Public Health 107 (12): 1883–1889.
- Calabrese, S. K., M. Tekeste, K. H. Mayer, M. Magnus, D. S. Krakower, T. S. Kershaw, A. I. Eldahan, L. A. Gaston Hawkins, K. Underhill, N. B. Hansen, et al. 2019. “Considering Stigma in the Provision of HIV Pre-Exposure Prophylaxis: Reflections from Current Prescribers.” AIDS Patient Care and STDS 33 (2): 79–88.
- Charles, C., A. Gafni, and T. Whelan. 1997. “Shared Decision-Making in the Medical Encounter: What Does It Mean? (or It Takes at Least Two to Tango).” Social Science & Medicine 44 (5): 681–692.
- Clark, H., A. S. Babu, E. W. Wiewel, J. Opoku, and N. Crepaz. 2017. “Diagnosed HIV Infection in Transgender Adults and Adolescents: Results from the National HIV Surveillance System, 2009-2014.” AIDS & Behavior 21 (9): 2774–2783.
- Cohen, J. J., B. A. Gabriel, and C. Terrell. 2002. “The Case for Diversity in the Health Care Workforce.” Health Affairs 21 (5): 90–102.
- Crenshaw, K. 1991. “Mapping the Margins: Intersectionality, Identity Politics, and Violence against Women of Color.” Stanford Law Review 43 (6): 1241–1299.
- Crenshaw, K. W. 1995. “The Intersection of Race and Gender.” In Critical Race Theory: The Key Writings That Formed the Movement, edited by K. W. Crenshaw, N. Gotanda, G. Peller, and K. Thomas, 357–383. New York: The New Press.
- Denson, D. J., P. M. Padgett, N. Pitts, G. Paz-Bailey, T. Bingham, J. A. Carlos, P. McCann, N. Prachand, J. Risser, and T. Finlayson. 2017. “Health Care Use and HIV-Related Behaviors of Black and Latina Transgender Women in 3 US Metropolitan Areas: Results from the Transgender HIV Behavioral Survey.” Journal of Acquired Immune Deficiency Syndromes 75 (Suppl 3): S268–S275.
- Deutsch, M. B., D. V. Glidden, J. Sevelius, J. Keatley, V. McMahan, J. Guanira, E. G. Kallas, S. Chariyalertsak, and R. M. Grant. 2015. “HIV Pre-Exposure Prophylaxis in Transgender Women: A Subgroup Analysis of the iPrEx Trial.” Lancet HIV 2 (12): e512–e519.
- Durand, M. A., L. Carpenter, H. Dolan, P. Bravo, M. Mann, F. Bunn, and G. Elwyn. 2014. “Do Interventions Designed to Support Shared Decision-Making Reduce Health Inequalities? A Systematic Review and Meta-Analysis.” PLoS One 9 (4): e94670.
- Ezell, J. M., M. J. Ferreira, D. T. Duncan, and J. A. Schneider. 2018. “The Social and Sexual Networks of Black Transgender Women and Black Men Who Have Sex with Men: Results from a Representative Sample.” Transgender Health 3 (1): 201–209.
- Garnett, M., Y. Hirsch-Moverman, J. Franks, E. Hayes-Larson, W. M. El-Sadr, and S. Mannheimer. 2018. “Limited Awareness of Pre-Exposure Prophylaxis among Black Men Who Have Sex with Men and Transgender Women in New York City.” AIDS Care 30 (1): 9–17.
- Golub, S. A. 2018. “PrEP Stigma: Implicit and Explicit Drivers of Disparity.” Current HIV/AIDS Reports 15 (2): 190–197.
- Golub, S. A., K. E. Gamarel, H. J. Rendina, A. Surace, and C. L. Lelutiu-Weinberger. 2013. “From Efficacy to Effectiveness: Facilitators and Barriers to PrEP Acceptability and Motivations for Adherence among MSM and Transgender Women in New York City.” AIDS Patient Care and STDs 27 (4): 248–254.
- Grant, J. M., L. A. Mottet, J. Tanis, J. Harrison, J. L. Herman, and M. Keisling. 2011. Injustice at Every Turn: A Report of the National Transgender Discrimination Survey. Washington, DC: National Center for Transgender Equality and National Gay and Lesbian Task Force.
- Grant, R. M., P. L. Anderson, V. McMahan, A. Liu, K. R. Amico, M. Mehrotra, S. Hosek, C. Mosquera, M. Casapia, O. Montoya, et al. 2014. “Uptake of Pre-Exposure Prophylaxis, Sexual Practices, and HIV Incidence in Men and Transgender Women Who Have Sex with Men: A Cohort Study.” The Lancet Infectious Diseases 14 (9): 820–829.
- Herbst, J. H., E. D. Jacobs, T. J. Finlayson, V. S. McKleroy, M. S. Neumann, N. Crepaz, and HIV AIDS Prevention Research Synthesis Team. 2008. “Estimating HIV Prevalence and Risk Behaviors of Transgender Persons in the United States: A Systematic Review.” AIDS & Behavior 12 (1): 1–17.
- Hook, J., N., and D. E. Davis. 2017. “Cultural Humility.” In The International Encyclopedia of Intercultural Communication, edited by Y. Y. Kim, 1–5. New York: Wiley Blackwell.
- Howard, S. D., K. L. Lee, A. G. Nathan, H. C. Wenger, M. H. Chin, and S. C. Cook. 2019. “Healthcare Experiences of Transgender People of Color.” Journal of General Internal Medicine 34 (10): 2068–2074.
- Huang, Y. A., W. Zhu, D. K. Smith, N. Harris, and K. W. Hoover. 2018. “HIV Preexposure Prophylaxis, by Race and Ethnicity – United States, 2014-2016.” MMWR. Morbidity and Mortality Weekly Report 67 (41): 1147–1150.
- Hudson, K. D. 2019. “(Un)Doing Transmisogynist Stigma in Health Care Settings: Experiences of Ten Transgender Women of Color.” Journal of Progressive Human Services 30 (1): 69–87.
- Iantaffi, A., and W. O. Bockting. 2011. “Views from Both Sides of the Bridge? Gender, Sexual Legitimacy and Transgender People's Experiences of Relationships.” Culture, Health & Sexuality 13 (3): 355–370.
- Institute of Medicine. 2011. The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding. Washington, DC: The National Academies Press.
- Jackson, G. Y., C. K. Darlington, H. Van Tieu, B. M. Brawner, D. D. Flores, J. A. Bannon, A. Davis, V. Frye, D. Chittamuru, P. Gugerty, et al. 2021. “Women's Views on Communication with Health Care Providers About Pre-Exposure Prophylaxis (PrEP) for HIV Prevention.” Culture, Health & Sexuality 4:1–16.
- James, S. E., C. Brown, and I. Wilson. 2017. 2015 U.S. Transgender Survey: Report on the Experiences of Black Respondents. Washington, DC and Dallas, TX: National Center for Transgender Equality, Black Trans Advocacy, & National Black Justice Coalition.
- Johnson, R. L., D. Roter, N. R. Powe, and L. A. Cooper. 2004. “Patient Race/Ethnicity and Quality of patient-physician communication during medical visits.” American Journal of Public Health 94 (12): 2084–2090.
- Kelly, J. A. 2004. “Popular Opinion Leaders and HIV Prevention Peer Education: Resolving Discrepant Findings, and Implications for the Development of Effective Community Programmes.” AIDS Care 16 (2): 139–150.
- King, J. S., M. H. Eckman, and B. W. Moulton. 2011. “The Potential of Shared Decision Making to Reduce Health Disparities.” Journal of Law, Medicine & Ethics 39 (S1): 30–33.
- Klein, A., and S. A. Golub. 2019. “Increasing Access to Pre-Exposure Prophylaxis among Transgender Women and Transfeminine Nonbinary Individuals.” AIDS Patient Care and STDS 33 (6): 262–269.
- Krakower, D. S., N. C. Ware, K. M. Maloney, I. B. Wilson, J. B. Wong, and K. H. Mayer. 2017. “Differing Experiences with Pre-Exposure Prophylaxis in Boston among Lesbian, Gay, Bisexual, and Transgender Specialists and Generalists in Primary Care: Implications for Scale-Up.” AIDS Patient Care and STDS 31 (7): 297–304.
- Kuhns, L. M., S. L. Reisner, M. J. Mimiaga, T. Gayles, M. Shelendich, and R. Garofalo. 2016. “Correlates of Prep Indication in a Multi-Site Cohort of Young HIV-Uninfected Transgender Women.” AIDS & Behavior 20 (7): 1470–1477.
- Li, C. C., A. K. Matthews, F. Aranda, C. Patel, and M. Patel. 2015. “Predictors and Consequences of Negative Patient-Provider Interactions among a Sample of African American Sexual Minority Women.” LGBT Health 2 (2): 140–146.
- Marcus, J. L., K. A. Katz, D. S. Krakower, and S. K. Calabrese. 2019. “Risk Compensation and Clinical Decision Making – The Case of HIV Preexposure Prophylaxis.” The New England Journal of Medicine 380 (6): 510–512.
- Nemoto, T., D. Operario, J. Keatley, and D. Villegas. 2004. “Social Context of HIV Risk Behaviours among Male-to-Female Transgenders of Colour.” AIDS Care 16 (6): 724–735.
- Ng, H. H. 2016. “Intersectionality and Shared Decision Making in LGBTQ Health.” LGBT Health 3 (5): 325–326.
- Nordmarken, S., and R. Kelly. 2014. “Limiting Transgender Health: Administrative Violence and Microaggressions in Health Care Systems.” In Health Care Disparities and the LGBT Population, edited by V. L. Harvey and T. H. Housel, 143–166. Plymouth: Lexington Books.
- Peek, M. E., F. Y. Lopez, H. S. Williams, L. J. Xu, M. C. McNulty, M. E. Acree, and J. A. Schneider. 2016. “Development of a Conceptual Framework for Understanding Shared Decision Making among African-American LGBT Patients and Their Clinicians.” Journal of General Internal Medicine 31 (6): 677–687.
- Petroll, A. E., J. L. Walsh, J. L. Owczarzak, T. L. McAuliffe, L. M. Bogart, and J. A. Kelly. 2017. “PrEP Awareness, Familiarity, Comfort, and Prescribing Experience among US Primary Care Providers and HIV Specialists.” AIDS & Behavior 21 (5): 1256–1267.
- Poteat, T., M. Malik, A. Scheim, and A. Elliott. 2017. “HIV Prevention among Transgender Populations: Knowledge Gaps and Evidence for Action.” Current HIV/AIDS Reports 14 (4): 141–152.
- Poteat, T., A. Wirtz, M. Malik, E. Cooney, C. Cannon, W. D. Hardy, R. Arrington-Sanders, M. Lujan, and T. Yamanis. 2019. “A Gap between Willingness and Uptake: Findings from Mixed Methods Research on HIV Prevention among Black and Latina Transgender Women.” Journal of Acquired Immune Deficiency Syndromes 82 (2): 131–140.
- QSR International Pty Ltd. 2017. NVivo (Version 11), https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home
- Quinn, K., L. Bowleg, and J. Dickson-Gomez. 2019. ““The Fear of Being Black Plus the Fear of Being Gay": The Effects of Intersectional Stigma on PrEP Use among Young Black Gay, Bisexual, and Other Men Who Have Sex with Men.” Social Science & Medicine 232:86–93.
- Quinn, K., J. Dickson-Gomez, M. Zarwell, B. Pearson, and M. Lewis. 2019. ““A Gay Man and a Doctor Are Just Like, a Recipe for Destruction": How Racism and Homonegativity in Healthcare Settings Influence PrEP Uptake among Young Black MSM.” AIDS & Behavior 23 (7): 1951–1963.
- Reback, C. J., K. A. Clark, D. Runger, and A. E. Fehrenbacher. 2019. “A Promising PrEP Navigation Intervention for Transgender Women and Men Who Have Sex with Men Experiencing Multiple Syndemic Health Disparities.” Journal of Community Health 44 (6): 1193–1203.
- Restar, A. J., L. Kuhns, S. L. Reisner, A. Ogunbajo, R. Garofalo, and M. J. Mimiaga. 2018. “Acceptability of Antiretroviral Pre-Exposure Prophylaxis from a Cohort of Sexually Experienced Young Transgender Women in Two U.S. Cities.” AIDS & Behavior 22 (11): 3649–3657.
- Schneider, J. A., L. Young, A. Ramachandran, S. Michaels, H. Cohen, I. Robinson, L. Alon, et al. 2021. “A Pragmatic Randomized Controlled Trial to Increase PrEP Uptake for HIV Prevention: 55-Week Results from PrEP Chicago.” Journal of Acquired Immune Deficiency Syndromes 86 (1): 31–37.
- Sevelius, J. M., A. Carrico, and M. O. Johnson. 2010. “Antiretroviral Therapy Adherence among Transgender Women Living with HIV.” The Journal of the Association of Nurses in Aids Care 21 (3): 256–264.
- Sevelius, J. M., J. Keatley, N. Calma, and E. Arnold. 2016. “‘I Am Not a Man': Trans-Specific Barriers and Facilitators to PrEP Acceptability among Transgender Women.” Global Public Health 11 (7-8): 1060–1075.
- Sevelius, J. M., T. Poteat, W. E. Luhur, S. L. Reisner, and I. H. Meyer. 2020. “HIV Testing and PrEP Use in a National Probability Sample of Sexually Active Transgender People in the United States.” Journal of Acquired Immune Deficiency Syndromes 84 (5): 437–442.
- Stewart, M. A. 1995. “Effective Physician–Patient Communication and Health Outcomes: A Review.” Canadian Medical Association Journal 152:1423–1433.
- Sullivan, L. W. 2004. Missing Persons: Minorities in the Health Professions, a Report of the Sullivan Commission on Diversity in the Healthcare Workforce. The Sullivan Commission.
- Tervalon, M., and J. Murray-Garcia. 1998. “Cultural Humility Versus Cultural Competence: A Critical Distinction in Defining Physician Training Outcomes in Multicultural Education.” Journal of Health Care for the Poor and Underserved 9 (2): 117–125.
- Whitehead, J., J. Shaver, and R. Stephenson. 2016. “Outness, Stigma, and Primary Health Care Utilization among Rural LGBT Populations.” PLoS One 11 (1): e0146139.
