
ABSTRACT
Crowdfunding is becoming a popular way of financing healthcare. Some commentators suggest that crowdfunding could serve as a new institution that fills gaps in conventional safety nets. Others suggest that crowdfunding is simply another way of obtaining help from family, friends, and local associations, and has little transformative potential. We provide one of the first quantitative analyses of medical crowdfunding, and the first to model the broader societal context in which campaigns are situated. We scraped data on US medical campaigns from the leading platform and combined them with county-level socioeconomic data, to model predictors of campaign frequency and success. Our findings suggest that many seek help from crowdfunding when both formal and informal conventional safety nets fail them. Significantly more campaigns are initiated in US counties with poorer private insurance coverage, lower social security provision, fewer social associations, and weaker cultures of giving. However, few campaigns reach their goals where most needed. More successful campaigns are found in counties that are wealthier and healthier and have more social associations. Crowdfunding is not merely ‘friendfunding’: fundraisers can increase their chances of success by having their appeals widely shared on social media. However, the returns to sharing are greater for campaigns initiated in wealthier areas. Overall, our findings suggest that medical crowdfunding is an entrepreneurial safety net: one where protection is not afforded universally or on the basis of need, but on the basis of one’s ability to appeal to the audience and out-compete rivalling needfuls.
Introduction
Charitable crowdfunding is an increasingly popular way of financing social services such as healthcare, education, and housing assistance. GoFundMe, the largest crowdfunding platform designed for charitable and personal causes, has raised more than $5 billion since it was launched in 2010. The largest category on the platform is medical crowdfunding: approximately a third of all funds raised on the platform have been for medical costs. According its CEO Rob Solomon, GoFundMe was never designed to focus on medical crowdfunding; medical simply turned out to be the category with the greatest need. About 250,000 medical campaigns are created annually, raising approximately $650 million globally (Bluth, Citation2019).
It is frequently postulated that the popularity of medical crowdfunding reflects deficiencies in conventional safety net institutions, especially in the United States (Berliner & Kenworthy, Citation2017; Sisler, Citation2012; Snyder et al., Citation2017). Health insurance providers and other formal safety net institutions leave significant gaps in Americans’ care. Many have no formal recourse when illness strikes. Solomon suggests that his platform has thus inadvertently become ‘an indispensable institution’ (Bluth, Citation2019). ‘We’re the digital safety net’, he suggests in an interview (Harries, Citation2017).
Is crowdfunding really a transformative new institution that can fill the gaps in conventional safety nets? Campaigns often appear to appeal to family and friends: ‘I’m guessing that if you’re reading this, you know and love Steve’ (Snyder et al., Citation2017, p. 365). Informal safety nets formed by family, friends, and local social associations have always been an important source of caregiving and financial help (Agarwal et al., Citation2011; Blakemore & Warwick-Booth, Citation2013; Verbakel, Citation2018). These informal safety nets are a natural fallback when formal safety net institutions fail (Gilbert & Terrell, Citation2002; Morduch, Citation1999). If charitable crowdfunding is ‘friendfunding’ (Borst et al., Citation2018) – if all it does is to provide a new medium for these old social processes (English, Citation2013) – then it is unlikely to transform access to healthcare in any significant way. It will replicate and may even widen pre-existing divides, favoring those who are already highly educated, tech-savvy, and socially well-connected (Berliner & Kenworthy, Citation2017).
However, there are some indications that crowdfunding might be doing more than simply reproducing existing social processes. For instance, one fundraiser suggested that 20% of donations to her medical crowdfunding campaign came from people she did not know (Kim et al., Citation2017). By enabling a new mode of communication centering around the use of social media, crowdfunding can potentially match donors and beneficiaries beyond established networks and geographic boundaries (Durand et al., Citation2018; Kang et al., Citation2017). As a result, crowdfunding could potentially help address gaps in both formal and informal conventional safety nets (Burtch & Chan, Citation2014; Renwick & Mossialos, Citation2017). Crowdfunding could thus potentially represent a transformational new institution in the funding of healthcare, with distributional effects distinct from the established ones.
Empirical research on charitable crowdfunding in general and medical crowdfunding in particular remains very limited. Much of the literature consist of opinions, commentaries, and perspective pieces. The few empirical studies that exist mostly revolve around examining which individual campaign attributes predict crowdfunding success. Little is known about how the popularity of medical crowdfunding is related to formal and informal safety net institutions, and to what extent it addresses unmet needs. Overall, there remains a substantial gap in the crowdfunding literature on its relationship with broader societal factors, which is argued to require further conceptual and empirical exploration (Shneor & Vik, Citation2020), especially from institutional perspectives (Kshetri, Citation2015). In this article, we address this gap with findings from one of the first quantitative analyses of medical crowdfunding, and the first one to model the broader societal context in which crowdfunding campaigns are situated.
We explore following questions. First, we explore how the popularity of medical crowdfunding is related to deficiencies of conventional formal safety nets. More specifically, we ask if people initiate more crowdfunding campaigns where formal safety nets are weak, and if these campaigns succeed. Second, we explore how medical crowdfunding is associated with conventional informal safety nets; if the strength of informal safety nets predicts the frequency of campaigns and their success. Lastly, we explore to what extent technological affordances of crowdfunding, such as sharing campaigns on social media, can explain the fundraising performance. To answer these questions, we scraped data on US-based medical campaigns from GoFundMe and combined them with county-level socioeconomic data to model campaign frequency and success.
Our findings are consistent with the interpretation that many people seek help from medical crowdfunding when both formal and informal conventional safety nets fail them. Significantly more campaigns are initiated in US counties with poorer private medical insurance coverage, lower public social security provision, fewer social associations, and weaker cultures of giving. However, at the same time, few medical crowdfunding campaigns reach their funding goals where they are most needed. The highest numbers of successful campaigns are found in counties that are wealthier and healthier and have more social associations. Crowdfunding is not merely ‘friendfunding’: fundraisers can increase their chances of success if they can get their appeals to be widely shared on social media. However, the returns to sharing are greater for campaigns initiated in wealthier areas. Overall, our findings suggest that medical crowdfunding is an entrepreneurial safety net: one where protection is not afforded universally or on the basis of need, but on the basis of one’s ability to appeal to the audience and out-compete rivalling needfuls.
Background and research questions
Deficiencies of formal safety net institutions in the US
The field of healthcare provision and financing can be conceptualized as consisting of a variety of institutions and organizational forms (Gilbert & Terrell, Citation2002; Glennerster, Citation2003; Narayan, Citation1999). These include formal safety net institutions, such as public healthcare programs and employer-based health insurance programs, as well as informal safety net institutions, such as charitable associations and family networks. presents a simplified sketch of the different institutions, organizational forms, and types of provision.
Table 1. Institutions and key players in healthcare provision and finance.
The US healthcare system is unique among advanced industrialized countries in that it does not have universal public program; it is a hybrid system where most citizens are covered by combinations of private and government insurance (Department for Professional Employees, Citation2016). The Affordable Care Act (ACA), enacted in 2010, stresses shared responsibility between the government, employers, and individuals for everyone’s access to affordable and good quality health insurance (The Commonwealth Fund, Citation2020). The ACA has decreased the number of uninsured people by about 19 million, particularly benefiting low-income households by expanding Medicaid (Blumberg et al., Citation2018). Despite this improvement, health insurance coverage remains fragmented, with numerous private insurance plans and wide gaps in coverage across the population. In 2018, 8.5% of people or 27.5 million did not have health insurance in the US (The Commonwealth Fund, Citation2020).
Private health insurance coverage (67.2%) is more prevalent than government coverage (33.7%) (Berchick et al., Citation2018). Americans are paying an increasingly large share of their income into insurance premiums. However, many Americans who cannot afford high-quality private plans decide to remain uninsured, or opt for cheaper, low-quality plans (Berliner & Kenworthy, Citation2017; Collins et al., Citation2019; Sisler, Citation2012). These plans do not offer adequate coverage and leave subscribers underinsured, with the consequence that serious illness is still likely to plunge them into financial crisis (Collins et al., Citation2019). The ACA provides no protection against financial vulnerability caused by these gaps in the private insurance system (Collins et al., Citation2019). Against this background, journalists and scholars have started to conjecture that the rise of medical crowdfunding is attributable to deficiencies in America’s healthcare system, and of its formal safety net institutions more generally (Berliner & Kenworthy, Citation2017; Sisler, Citation2012; Snyder et al., Citation2016).
Conceptualizing medical crowdfunding
The popularity of medical crowdfunding seems natural when tens millions of Americans are completely uninsured (Sisler, Citation2012). But what exactly is medical crowdfunding? Unlike entrepreneurial crowdfunding platforms for raising money for business ventures, some platforms are explicitly designed for charitable intentions (Agrawal et al., Citation2011). Crowdfunding platforms broadly speaking follow four different types of fundraising models: donation-based, equity-based, reward-based, and peer-to-peer lending. Charitable crowdfunding platforms fall into the donation-based category. Contributions are given in the form of a donation, and donors receive no tangible benefits in return, such as money, perks, or equity (Bone & Baeck, Citation2016; Dushnitsky & Marom, Citation2013). Examples of platforms include GoFundMe, Youcaring (which became a part of GoFundMe in 2018), Crowdrise (which became a part of GoFundMe in 2018), GiveForward (which became a part of Youcaring in 2017 and then GoFundMe in 2018), and JustGiving. Users initiate campaigns on the platforms for personal causes such as medical costs, education costs, memorial costs, housing emergencies, volunteering, and animal welfare, of which the medical category is the most popular one on leading platforms (Bluth, Citation2019; Snyder et al., Citation2016). Other users donate money to campaigns of their choice.
There is no single, common definition of medical crowdfunding. Based on the previous definitions of crowdfunding and crowdsourcing (Belleflamme et al., Citation2014; Bouncken et al., Citation2015; Howe, Citation2006; Mollick, Citation2014; Tomczak & Brem, Citation2013), we define medical crowdfunding as the act of financing healthcare through voluntary donations solicited via an open call to an undefined group of people on the Internet.
Crowdfunding platforms can be conceptualized as a new institution in the field of financing healthcare. The term ‘institutions’ is often used in the social sciences to refer to enduring structures and patterns of social life. According to an influential definition, institutions are seen as ‘the rules of the game of a society’ or more formally, ‘the humanly-devised constraints that structure human interaction’ (North, Citation1995, pp. 5–6). Institutions consist of formal rules, informal rules, and enforcement characteristics of both. Formal rules include laws, regulations, policies, contracts, and firms. Informal rules include conventions, norms, taboos, social values, and religions (Kherallah & Kirsten, Citation2002; North, Citation1991; Williamson, Citation2000). Formal and informal institutions both constrain and enable ordered thought, belief, and action, as they structure social interaction in a given context (Hodgson, Citation2006). Institutions are interrelated (Granovetter, Citation1985; Williamson, Citation2000). For instance, one’s economic action can be constrained by the contract (formal rule); the contract is structured and constrained by property rights (formal rule); operations of property rights are situated in informal social norms (Williamson, Citation2000).
Crowdfunding platforms enable people’s social and economic behaviors by allowing donors and beneficiaries to find each other. This enabling feature has been highlighted in most crowdfunding literature (e.g., Burtch & Chan, Citation2014; Renwick & Mossialos, Citation2017). But platforms also confine and structure social and economic interactions through various formal and informal rules. Formal rules include terms of use, the platform fee, regional availability, fundraiser eligibility rules, modes of communication, design of visibility, and fraud detection mechanisms. For example, GoFundMe removed a campaign page for ‘anti vaxxers’ in March 2019 as campaigns promoting misinformation about vaccines violate GoFundMe’s terms of service (ABC News, Citation2019a). The formal and informal rules of a platform are interrelated. For instance, the available modes of communication such as updates and comments (formal rule) structure user interaction, and shape informal norms such as trust and reciprocity (Kim et al., Citation2016; Kim et al., Citation2017; Tanaka & Voida, Citation2016; Wang et al., Citation2019). However, not every platform provides such communication modes (Tanaka & Voida, Citation2016).
Medical crowdfunding and formal safety nets: is crowdfunding a gap filler?
It is plausible that many of the sizeable portion of Americans who neither qualify for public health coverage nor have enough purchasing power for adequate private insurance might now be resorting to medical crowdfunding instead. Gaps in other formal government safety nets such as social security and public assistance programs could also be related to the popularity of medical crowdfunding: fundraisers often express concerns about lost wages due to illness and the costs of childcare during treatment (Berliner & Kenworthy, Citation2017).
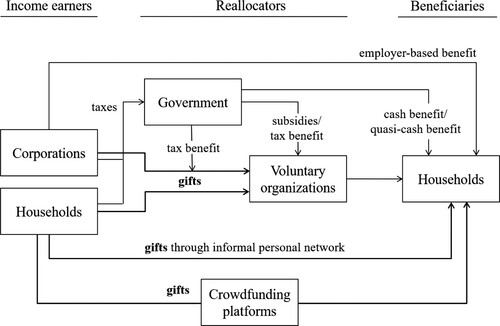
Previous literature suggests that medical crowdfunding can work where conventional formal institutions fail, by virtue of its unique features. In conventional government funding of healthcare, funds from individual taxpayers are redistributed to relevant organizations, which then disburse the funds to beneficiaries according to institutional rules (). But medical crowdfunding is played according to different rules. Individuals donate directly to other individuals, without conventional intermediaries. Individuals who are not eligible for state benefits can freely raise funds in crowdfunding platforms. Individuals whose potential treatments are not covered by private health insurance programs can also raise funds to cover such treatments. Potential donors gain access to individual-level information about the beneficiaries: they can read the fundraiser’s story, communicate with the fundraiser if necessary, and choose which campaigns to finance.
Figure 1. Pathways of financing healthcare for households. Source: Conventional income earners, reallocators, and beneficiaries are adapted from Glennerster (Citation2003) and List (Citation2011).
Some previous studies also support this interpretation of medical crowdfunding. In one study, some interviewees had initiated crowdfunding because they did not have health insurance; others had insurance, but it did not cover certain types of care (Gonzales et al., Citation2016). Another study found that 1,000 campaigns in the US and Canada had raised a total of $6 million for experimental or scientifically controversial treatments that were unlikely to be covered by formal health insurers (Vox et al., Citation2018). Potential donors also actively sought information about fundraisers’ medical situations (e.g., illness and treatments) and alternative funding sources (e.g., public and private insurance coverage) before deciding whether to donate (Kim et al., Citation2016).
Nonetheless, there is still some doubt as to how strongly the popularity of medical crowdfunding is related to the deficiencies of formal safety nets. Most previous studies are based on qualitative interviews (Gonzales et al., Citation2016; Kim et al., Citation2017; Renwick & Mossialos, Citation2017) and content analysis (Berliner & Kenworthy, Citation2017; Kim et al., Citation2016; Snyder et al., Citation2017), which provide ample illustration of the potential mechanisms, but establish no quantitative association. In our study, we thus first seek to address the following question:
RQ1. Are medical crowdfunding campaigns more popular where formal safety nets are weak?
By ‘popularity’ we mean both the popularity of initiating campaigns and of donating to campaigns. Based on the previous literature, we expect that the popularity of medical crowdfunding is negatively associated with formal health-specific safety nets (e.g., public and private health insurance coverage). We also expect the popularity of medical crowdfunding to be negatively associated with formal non-health specific social safety nets (e.g., social security income, supplemental security income, public/cash assistance coverage).
Similarities between medical crowdfunding and informal safety nets: is crowdfunding just another example of ‘friendfunding’?
While some suggest that medical crowdfunding could act as a substitute to formal safety net institutions (e.g., Burtch & Chan, Citation2014), others suggest that it might not be different from conventional informal safety nets. As seen in , direct giving from one individual to another makes crowdfunding look very similar to many existing practices. Informal personal networks, including families, friends, neighbors, and social associations (e.g., sports clubs) have always been an integral resource of caregiving and financial help at different stages of a person’s life (Agarwal et al., Citation2011; Blakemore & Warwick-Booth, Citation2013; Donelan et al., Citation2002). Even with deficiencies in both public safety nets and private insurance markets, households are not completely exposed to financial risk, thanks to these ‘informal insurance’ providers based on individual and community actions, including reciprocal exchanges of gifts (Morduch, Citation1999; Verbakel, Citation2018) (also see ). Indeed, medical crowdfunding campaigns often appeal to friends and families in the tone of an open letter to these groups (Snyder et al., Citation2017). The appeals often suggest that these informal and personal networks have an obligation to donate (e.g., ‘The home team of her friends, colleagues and family must be there for as long as she needs us’ (Snyder et al., Citation2017, p. 365)). Moreover, it appears to be common that people organize campaigns as fundraisers to help others who are members of their informal networks (Snyder et al., Citation2017).
If the role of medical crowdfunding is to merely provide a new medium for conventional social processes in which informal social safety nets provide benefits to participants in a network, in the forms of money, information, personal connections, or the opportunity to organize activities (Paxton, Citation1999; Coleman, Citation1988), then it is unlikely to have significant transformational effects on access to healthcare. Rather, it is likely to reproduce or even deepen existing social, economic and geographic inequalities. The greatest beneficiaries of medical crowdfunding might be those who are highly educated, tech-savvy, socially well-connected, and based in wealthy urban areas where their residents already enjoy benefits of social associations and culture of giving (Kshetri, Citation2015). Kenworthy and Berliner suggest that ‘crowdfunding seems to be best for people who are of a dominant social group who have fallen on hard times’, since well-off people can tap into networks of well-off friends (Jopson, Citation2018).
No previous studies to date have attempted to quantify the effect of these informal safety nets at both personal and local levels on the popularity of medical crowdfunding. Research on other types of crowdfunding has documented such an effect, however. For instance, education crowdfunding was found to be mainly funded by friends and families (English, Citation2013). The major initial source of music-related crowdfunding was ‘friends and family’ money (Agrawal et al., Citation2011). Also, a large online social network size (i.e., Facebook friends) of the fundraisers was found to be a success factor for commercial crowdfunding campaigns (Mollick, Citation2014). Borst et al. (Citation2018) referred to this type of funding as ‘friendfunding’, in which funds come from family members, friends, and close acquaintances, in contrast to undefined ‘crowds’.
Relatedly, previous research also suggests that spatial factors play a role in crowdfunding. Mollick (Citation2014) reported that crowdfunding campaigns for for-profit, artistic, and cultural ventures were unevenly distributed across geography; the popularity of certain project types was influenced by geographic factors, such as presence of industries in the local area and the share of workers in creative occupations in the area. For instance, Los Angeles was dominated by film crowdfunding campaigns, and San Francisco had many more technology, games, and design projects. They were more likely to be successful when the region had a greater share of population working in creative jobs (Mollick, Citation2014). Davies (Citation2015) found that the popularity of crowdfunding for civic needs (e.g., building a community center) was highly concentrated in large metropolitan areas; one possible reason might be that these areas are resourceful in terms of income, digital literacy, and human capital that can spread campaigns out (Davies, Citation2015). In this respect, medical crowdfunding might also be linked to the major industries in the local communities, such as finance, healthcare, and information industries. It might also favor populous geographic areas where community members already enjoy wealth and strong social associations.
Literature on conventional charitable giving also suggests that income equality within a region can positively influence the amount of donations within the region (Bielefeld et al., Citation2005; Payne & Smith, Citation2015), since charitable giving often involves richer people donating to poorer people (Bielefeld et al., Citation2005). However, how this dynamic plays out in the context of crowdfunding is not clear. Charitable crowdfunding matches potential donors with beneficiaries in need, but the contribution per person is typically small, so that donations can potentially come also from less wealthy individuals.
In summary, we are interested in assessing to what extent medical crowdfunding is an extension or reproduction of conventional informal safety nets. We, thus ask:
RQ2. Does the strength of informal safety nets predict the popularity of medical crowdfunding campaigns?
Based on the literature discussed above, we expect to find that the popularity of medical crowdfunding is positively associated with the strength of informal safety nets (e.g., number of social associations and the strength of culture of giving in the county). We also expect that the popularity of medical crowdfunding is associated with the socioeconomic characteristics of the area (e.g., wealth, income inequality, education, and health problems) in the same ways as informal safety nets are.
Differences between crowdfunding and informal safety nets: technological affordances for tapping into the ‘crowd’
There are also studies that suggest that crowdfunding may be doing more than simply extending existing social processes. It is claimed that crowdfunding distinguishes itself from conventional informal safety nets by allowing fundraisers to reach into the undefined group of individuals (i.e., ‘crowd’) outside their pre-existing social associations. For instance, one medical fundraiser said that 20% of donations came from people she did not know at all (Kim et al., Citation2017). Studies on general crowdfunding also argue that successful crowdfunding typically features small contributions by large numbers of funders, to an extent that a mere friendfunding network could not deliver (Mollick, Citation2014).
A set of dynamics that may influence distributional outcomes results from the fact that members of the ‘crowd’ do not know the fundraisers personally. They also cannot rely on conventional intermediaries such as government regulators, charities, and third-party watchdogs that could assess and monitor the validity of the campaigns or beneficiaries (Kim et al., Citation2016). To successfully appeal to the ‘crowd’, individual fundraisers must therefore work to establish trust with the audience (Borst et al., Citation2018; Tanaka & Voida, Citation2016). Given the risk of fraudulent campaigns, potential donors and social media users often seek information about fundraisers’ identities and their relationships with the beneficiaries, if different. For instance, when a fundraiser’s name did not match, potential donors explicitly asked for further information about the fundraiser; having a social media account linked to the campaign added to its credibility (Kim et al., Citation2016). GoFundMe provides a technological affordance for fundraisers to indicate whom they are fundraising for (‘on behalf of [name of beneficiary]’). Fundraisers can also display their Facebook account and the number of Facebook friends on the campaign page.
Some studies suggest that to win over the audience, fundraisers in charitable crowdfunding must also foster social relationships and community spirit around their campaigns (Borst et al., Citation2018; Tanaka & Voida, Citation2016). Indeed, studies suggest that well-crafted messages, frequent interactions with potential donors on the platform, and active use of social media are important for crowdfunding success (Borst et al., Citation2018). More specifically, the use of photographs in the appeal can be effective in inducing sympathy, which is one of the key mechanisms of giving (Bielefeld et al., Citation2005). Potential donors in medical crowdfunding tended to take a thorough look into the campaigns’ photos to evaluate the credibility of the campaign (Kim et al., Citation2016). Platforms such as GoFundMe also explicitly advise fundraisers to add photos to medical campaigns. Detailed messages are also important for signalling the credibility (Kim et al., Citation2016) and quality of the campaign (Bi et al., Citation2017). Furthermore, regular use of the platforms’ ‘updates’ feature is considered particularly significant. Fundraisers used regular updates to inform donors and assure them of how the funds were being used (Tanaka & Voida, Citation2016). Sufficiently frequent updates can be perceived as an indicator of the fundraiser’s credibility (Kim et al., Citation2016) and can attract more potential donors (Wang et al., Citation2019).
In addition, the funding goal set for the campaign is likely to affect donations. In charitable crowdfunding (including GoFundMe), fundraisers typically receive any funds pledged regardless of whether the funding goal was met or not, which makes the goal less important than in forms of crowdfunding where payment hinges on the goal being met. But the goal is still likely to influence donor behavior; according to the charitable giving literature, perceived needs affect giving: if beneficiaries are perceived as more needy, donors are likely to give more (Bekkers & Wiepking, Citation2010). In one study on medical crowdfunding, potential donors assessed whether the funding goal was reasonable (Kim et al., Citation2016); another study reported that the funding goal and the amount of donations were positively associated in organ transplantation crowdfunding (Durand et al., Citation2018). In the commercial crowdfunding literature, it has been found that the amount of funds raised increases with the funding goal (Gleasure & Feller, Citation2016), but the probability the campaign successfully reaching its goal decreases (Cordova et al., Citation2015; Giudici et al., Citation2013).
All of these dynamics are likely to feed back into not just how much money people donate, but how willing they are to spread the word about the campaign further. One of the highlighted enabling features of crowdfunding is its technological affordance pertaining to the use of social media. Not only fundraisers but also other platform participants can share campaigns on social media, such as Facebook and Twitter, and thus spread the word about the campaign to ‘crowds’ on the Internet. Previous literature suggests that sharing on social media increases the visibility of the need and helps fundraisers to connect with family and friends, and most importantly, with potential funders outside their existing personal networks (Hui & Gerber, Citation2015; Kang et al., Citation2017). This could potentially help to more efficiently match beneficiaries and donors beyond established networks and geographic boundaries (Kang et al., Citation2017).
In this respect, medical crowdfunding could represent a transformational new institution in the funding of healthcare, with distributional effects distinct from both formal and informal conventional safety nets. Indeed, GoFundMe claims that sharing via Facebook increases donations by ‘350%’. A strong positive correlation was also found between the times shared in social media and the amount raised in organ transplantation crowdfunding (Durand et al., Citation2018). In another study on charitable crowdfunding, use of social media helped to improve campaign popularity, and as a result, increased donation intention (Liu et al., Citation2017). Studies on crowdfunding for creative projects find similar effects (e.g., Lu et al., Citation2014). Sharing is thus a key variable that encapsulates much of what is expected to be distinct about crowdfunding in comparison to conventional informal safety nets. Word-of-mouth effects also exist in conventional personal networks-based giving, but hardly to the extent that the message would be passed on thousands of times, as we shall see can happen in medical crowdfunding.
To assess whether medical crowdfunding has distributional effects that make it distinct from conventional informal safety nets, we ask the following question:
RQ3. To what extent do the funds raised via crowdfunding depend on sharing and other uses of crowdfunding-specific technological affordances?
We expect that the number of times a campaign is shared via social media is positively associated with the funds raised, as are the fundraiser’s use of photos, level of detail in messages, frequency of updates, size of the funding goal, information about the fundraiser’s identity, and their number of Facebook friends.
Research design
Our overall research process was as follows. We scraped data on US campaigns from GoFundMe, the largest crowdfunding platform for charitable and personal causes. We combined this with county-level socioeconomic data from the US Census and other public sources and produced regression models estimating campaign frequency and campaign success. We then interpreted model coefficients to address the research questions.
We targeted GoFundMe, the largest though not the only donation-based crowdfunding platform for charitable and personal causes. Different platforms provide different modes of communication and also affect users’ perceptions of campaign credibility in different ways (Kim et al., Citation2016). Targeting one platform helps to exclude such platform effects. We focused on campaigns initiated in the US due to the availability of comparable county-level data across the country.
There are three ways to access medical campaigns through the US version of the GoFundMe website: accessing a list of 1,000 campaigns selected algorithmically by the site, listed in the ‘Medical’ category of the ‘Discover’ page; searching for campaigns with a specific keyword (e.g., ‘cancer’); or obtaining a direct link to a campaign through social media or similar means. Like other recent research on GoFundMe (Ren et al., Citation2020; Saleh et al., Citation2020), we used the first approach, since it is in practice the most viable means of obtaining a wide variety of campaigns across the US that are guaranteed to be in the medical category. The most viable alternative would be to use the search feature, but that would limit results to campaigns that match pre-defined keywords. As is typical in research based on data scraped from transaction platforms, our sample is thus not a probabilistic sample; it does not afford statistical generalizations to the universe of medical crowdfunding campaigns, but it allows us to examine associations between variables in the sample.
We scraped relevant data from each of the 1000 campaigns on 19 October 2018, including the fundraiser’s location, the amount of funds raised, funding goal, campaign duration, campaign description, the number of photos, the number of updates, whether the campaign was created on behalf of someone else, the number of Facebook friends the fundraiser has, and the number of times the campaign was shared on social media. All information collected was publicly accessible. Personal identifiers such as photos were not collected.
GoFundMe does not explain how its algorithm chooses the list of 1000 campaigns that we used; however, a regional manager indicated that real-time traffic and donation amounts play a role in how campaigns get featured on the site’s main page (ABC News, Citation2019b). In practice, the sample we obtained consists of campaigns that were initiated up to six months before the data collection date and had raised between $26,600 and $317,351 (). If, as seems likely, the sample excludes less successful campaigns, then our coefficient estimates in models predicting fundraising success are probably conservative. Still, we were able to find recent medical campaigns outside the sample that had raised more money that the sample average, so the sample is not simply a list of highest-earning campaigns.
Table 2. Descriptive statistics of main variables scraped from Gofundme.
To address RQ1 and RQ2, we aggregated the campaign data to the level of counties and combined it with county-level sociodemographic data. Many studies that investigate community-level factors in US healthcare use county-level data (Slack et al., Citation2014). Counties are a particularly important territorial scale for spatial inequalities, as county governments provide a set of social services that affect local economic development and human capital, and that serve safety net functions (Lobao et al., Citation2007). US territories not supported by GoFundMe (e.g., American Samoa, Guam, Puerto Rico) were excluded from the resulting county-level data set (GoFundMe, Citation2020). Seven campaigns where location information was missing or ambiguous were likewise excluded.
We used two dependent variables to capture different aspects of the popularity of medical crowdfunding in a given county: the number of campaigns initiated in the county and the number of campaigns that met their funding goal. Crowdfunding success at the county-level could in principle also be measured as the ratio of campaigns that meet their goal (Shneor & Vik, Citation2020). However, this creates methodological difficulties, as the success ratio distribution is dominated by extreme values (0% and 100% success ratios) resulting from single-campaign counties. The absolute number of successful campaigns is also a more relevant measure for understanding crowdfunding’s practical impact in a county; a high success rate based on a tiny handful of cases is misleading in this respect. Therefore, and following previous studies analyzing medical crowdfunding at territorial levels (Bassani et al., Citation2019; Berliner & Kenworthy, Citation2017; Burtch & Chan, Citation2014), we measured success as the absolute number of campaigns in a county that met their goal. However, we also estimate an additional model in which campaign frequency is included as a control, allowing us to assess relative success factors.
Our data set thus consisted of 3,141 US counties, of which 353 had campaigns initiated in them. Since the distribution of the number of campaigns initiated per county had a large number of zeroes, we estimated two models for it: a binary logistic regression model to predict whether any campaigns had been initiated in a county at all, and a log transformed linear regression model to predict the number of campaigns initiated per county. The largest numbers of campaigns came from Los Angeles (5.3%), followed by San Diego (2.5%), and Cook, Illinois (2.4%). In terms of states, the largest shares came from California (16.9%), followed by New York (9.4%), Texas (7.9%), and Florida (6.7%). No single county or state thus dominated the data set. Since county-level socioeconomic variables (e.g., income, education, broadband subscriptions) are usually correlated as also in our dataset, we checked the Variance Inflation Factor (VIF) and found it to be within a commonly acceptable bounds for all our models (<10) (Cohen et al., Citation2013).
To address RQ3, we performed hierarchical regression analysis on the individual campaign-level data, using the amount of funds raised as the dependent variable. Campaign-level success could also be measured in other ways, including whether the goal was met, the ratio of funds pledged versus the goal, and the number of donors (Shneor & Vik, Citation2020). Our choice of dependent variable is consistent with other recent studies that examine medical crowdfunding success at the campaign level (e.g., Barcelos & Budge, Citation2019; Durand et al., Citation2018). As a robustness check, we also estimated a logistic regression model using goal attainment (yes/no) as the dependent variable, with results that are not inconsistent with our main models. We excluded campaigns that were ‘complete and no longer active’ (n = 62) as some relevant information had been removed. A total of 914 cases were used for the individual campaign-level analysis.
Appendix A lists all the variables and their sources and how they were measured. As is typical in web-scraped data, distributions of variables collected from GoFundMe were often skewed and were transformed accordingly for regression analysis. Untransformed descriptive statistics are shown in Table 2 and Appendix B. Log-transformed correlation matrices are shown in Appendix C and Appendix D.
Findings
County-level analyses (RQ1 and RQ2)
First, we estimated a binary logistic regression model to predict the appearance of medical crowdfunding campaigns in a county (). Among variables measuring formal safety nets (RQ1), private health insurance coverage rate had a significant negative association with the dependent variable. A one-percent increase in private insurance coverage in the county decreases the probability of crowdfunding campaigns appearing in that county roughly by 4.5% (after accounting for the log-transformation). No statistically significant associations were observed with the public insurance coverage rate, the uninsured rate, and the non-health-specific safety net variables. No associations were likewise observed with informal safety nets (RQ2). Interestingly, health problems had a negative association: medical crowdfunding was less likely to appear in counties where people experienced poorer health, even after controls such as income and education were applied.
Table 3. Logistic regression model to predict the appearance of campaigns.
Second, we estimated linear regression models to predict the number of medical crowdfunding campaigns and the number of successful campaigns in a county (). The results were in line with the results of the binary logistic regression model, but several additional variables were statistically significant.
Table 4. Multiple regression models to predict the number and success of campaigns.
Several formal safety net institution variables (RQ1) had a negative association with the number of campaigns initiated. Private insurance coverage was also negatively associated with campaign success. Contrary to expectations, informal safety nets (RQ2) were likewise negatively associated with crowdfunding initiation. Informal safety nets were measured by the number of social associations and the strength of the culture of giving in the county. For crowdfunding success, the effect was reversed: a high number of social associations was positively associated with campaign success, while the culture of giving had no significant effect.
As suggested in the charitable giving literature, income inequality was positively associated with campaign initiation, though not with campaign success. The presence of information industry in a county was positively associated with crowdfunding popularity, as also observed in studies of commercial crowdfunding. Health problems were once again negatively associated with medical crowdfunding popularity.
We also estimated a model of campaign success that includes the number of campaigns initiated in the county as a control variable (Appendix E). This allows us to examine the predictors of relative as opposed to absolute campaign success. Unsurprisingly, the number of campaigns initiated in a county explains a substantial amount of the variation in the number of campaigns that met their goal (delta R2 = 26 p.p.), making most other predictors insignificant. However, the effect of high social association on campaign success remains significant. Campaigns initiated in counties with a high number of social associations are more likely to meet their goal.
Campaign-level analysis (RQ3)
Finally, we analyzed the individual campaign dataset (N = 914) to examine how the funds raised by a campaign are explained by the crowdfunding-specific behavior and characteristics of the campaign and the fundraiser as well as by the socioeconomic characteristics of the county in which they are situated. Using hierarchical multiple regression analysis (), campaign-level variables were inputted in the first block, followed by county-level variables in the second block. In the final block, an interaction term was inserted. The hierarchical design allows us to examine the relative importance of the different factors in explaining variance in fundraising success.
Table 5. Hierarchical multiple regression model to predict the amount of funds raised by campaign.
In line with previous crowdfunding literature, the results suggest that several characteristics and behaviors of the fundraiser and the campaign are predictive of the amount of funds raised. The size of the funding goal, number of photos, and message length were associated with more donations. As for the frequency of updates, the most funds accrued to campaigns updated 2–3 times per month. The number of the fundraiser’s Facebook friends was not generally significant. The exception was that having a low number of Facebook friends (in the bottom quartile) was worse than having no Facebook account linked at all. The number of times a campaign was shared via Facebook had a significantly positive association with donations (RQ3).
Campaign-level variables together explained 24% of the variance in funds raised. Adding the county-level variables to the model increases the share of variance explained by 2 percentage points; the increase in the F value is statistically significant (p<.05). The only county-level variable that we could detect having a direct statistically significant association with funds raised in crowdfunding campaigns initiated in that county was the county’s income level.
Finally, we inserted an interaction term between county income and the most significant crowdfunding-specific variable of interest: the number of times the campaign was shared. The sharing feature has been highlighted in the literature as one of the most distinctive elements of crowdfunding, which could potentially overcome geographic constraints by propagating the message beyond the fundraiser’s personal network (Hui & Gerber, Citation2015; Kang et al., Citation2017). We wanted to examine how this feature interacts with spatial variables, but we focused on income only since it was the only one with a statistically significant main effect. We found a significant positive interaction between these variables: when a campaign is frequently shared, the income of the county where the campaign is initiated becomes an even stronger predictor of funds raised by the campaign. This once again reinforces the importance of sharing but does not sit well with the notion that sharing is effective because it helps the message to reach people far beyond the fundraiser’s locale.
Discussion
Is medical crowdfunding a transformative new ‘digital safety net’ that can fill gaps left by conventional safety nets, as suggested by the CEO of the biggest fundraising platform? Or is it just another instance of ‘friendfunding’, of people relying on their personal networks in times of need, with the consequence that some are better protected and others not at all? The stakes are high. Formal safety net institutions in the US and post-austerity Europe are leaving millions of people without adequate cover. Informal safety nets are likewise under strain, as economic inequality deepens and communities struggle to maintain solidarity, even before the COVID-19 pandemic. Many people are understandably turning to charitable crowdfunding, but we understand very little about what kind of an alternative it provides. In one of the first quantitative analyses of medical crowdfunding, and the first to assess its relationship with broader society, we were able to produce some tentative answers to these questions.
Crowdfunding sought as a substitute to failing formal safety nets
We found evidence that the number of medical crowdfunding campaigns initiated was greater in US counties with weaker formal safety nets (RQ1). These findings are consistent with the notion that people are attempting to use medical crowdfunding as means to address gaps left by formal safety nets.
Of the three variables measuring health-specific safety nets, private health insurance coverage rate was negatively associated with crowdfunding popularity. Public insurance coverage rate and the uninsured rate did not have separate statistically significant effects. This is natural, because the three variables are mutually related. When people do not qualify for public insurance, they or their employers in most cases obtain private insurance for them. Public and private insurance together determine the uninsured rate. The interpretation is thus straightforward: people are more likely to resort to crowdfunding in counties where the insurance coverage is low. Indeed, there are many journalistic accounts of uninsured people, when struck with serious illness, seeking to crowdfund life-saving treatments for themselves (Sisler, Citation2012).
We also found that variables measuring non-health-specific formal safety nets, namely social security income and public assistance benefits, could be used to predict the number of crowdfunding campaigns initiated in a county. Specifically, weaker non-health-specific safety nets were associated with more crowdfunding campaigns. This is consistent with qualitative research finding that many medical crowdfunding fundraisers were seeking funds not only for medical expenses but also to cover the loss of income from unpaid sick leave or costs associated with caring for family members during sickness (Berliner & Kenworthy, Citation2017).
We found more evidence of an association between formal safety nets and crowdfunding initiation, and less evidence of an association between formal safety nets and crowdfunding success. In part this is likely to reflect methodological limitations (smaller sample size). But in part it is likely to reflect the fact that more people are seeking relief from crowdfunding sites than are actually obtaining it.
A notable limitation of our study was that we lacked variables to examine the effects of underinsurance on crowdfunding popularity. Qualitative research suggests that not only outright lack of insurance coverage but also the lack of adequate coverage could be an important factor of crowdfunding popularity (Gonzales et al., Citation2016).
Crowdfunding sought as substitute to fraying informal safety nets
We also asked how medical crowdfunding was associated with informal safety nets, such as kinship networks and social associations, which people often turn to when formal safety nets fail them (RQ2). Previous research suggests that much of crowdfunding may be essentially ‘friendfunding’ (e.g., English, Citation2013), that is, the funds are obtained from existing personal networks, and the digital platform is simply a novel way of accessing one’s pre-existing informal safety net (Borst et al., Citation2018). Contrary to our expectations, we found that crowdfunding campaign initiation was negatively associated with variables measuring the strength of informal safety nets in a county.
The two measures of informal safety nets at our disposal were the number of social associations in a county and the strength of the county’s culture of giving (Kshetri, Citation2015). These are far from perfect measures, as they do not directly address the most important element of informal safety nets, which are personal networks. However, our measures are an improvement on previous charitable and medical crowdfunding research, which has so far not attempted to quantify the effects of informal safety nets in the local communities at all (nor of related concepts such as regional social capital). Moreover, in the campaign-level analyses, we did examine the relationship between fundraisers’ Facebook network size and fundraising performance and found no positive associations.
Existing discourses around medical crowdfunding have focused on how they might address failing formal safety nets; our findings are consistent with an interpretation that people are seeking to use medical crowdfunding as a substitute to failing formal safety nets as well as to fraying informal safety nets. Informal safety nets in local communities typically play a crucial role in providing and financing healthcare, and mitigating financial risks from ill health (Agarwal et al., Citation2011; Gilbert & Terrell, Citation2002; Narayan, Citation1999). If communities are experiencing a weakening of social associations and cultures of giving, it is inevitable that this leaves people with more unmet care needs, which leads more people to seek help from medical crowdfunding.
However, when we examine the relationship between informal safety nets and crowdfunding success, we find that the relationship is reversed: counties with a low number of social associations experience less crowdfunding success than counties with a high number of social associations. This suggests that while weak informal safety nets may be driving more people to seek help from crowdfunding, actually getting that help remains easier in counties with strong informal safety nets. We return to this finding below.
Sharing pays off – especially in wealthier areas
We also asked to what extent medical crowdfunding success is associated with the use of technological affordances that are distinct to crowdfunding (RQ3). This question further addresses the similarity or distinctiveness of crowdfunding as opposed to conventional informal safety nets. In particular, we were interested in the ability of fundraisers and their contacts to share the campaign appeal on social media. Sharing is posited to be a key affordance that allows campaigns to reach beyond personal networks and transform from conventional ‘friendfunding’ into true crowdfunding (Durand et al., Citation2018; Hui & Gerber, Citation2015; Kang et al., Citation2017; Lu et al., Citation2014).
Indeed, we found that the number of times a campaign was shared on social media was strongly predictive of the amount of funds raised. On average, campaigns were shared 1385 times; since our sample was not probabilistic, the figure is not generalizable to the universe of medical crowdfunding, but it illustrates the scale that many campaigns apparently achieve. In line with previous crowdfunding literature, we found that fundraisers who were more engaged in communicating with potential beneficiaries generally speaking succeeded in raising more funds.
In contrast to some previous research (e.g., Mollick, Citation2014), we found that the size of the fundraiser’s social media network was not positively associated with the amount of funds raised. Instead, we found that having a small number of Facebook friends was less effective than having no Facebook account at all. A likely explanation is that when potential donors evaluate the fundraisers’ social media accounts to assess campaign credibility (Kim et al., Citation2016; Liu et al., Citation2017), a very small number of friends is seen as a sign of a potentially inactive, fake, or throwaway account. Taken together, these findings are consistent with an interpretation that medical crowdfunding is not merely friendfunding: fundraising success is determined not only by the fundraiser’s immediate network, but by the extent to which they are able to get the appeal to spread further afield via social media.
However, we also found that there was a significant positive interaction between sharing and the income level of the county where the fundraiser was located. Sharing yielded significantly more donations for campaigns initiated in wealthier counties. This suggests that it may not be accurate to think that sharing causes the appeal to reach a random ‘crowd’ on the Internet. Sharing causes the message to propagate beyond the fundraiser’s immediate network, but not necessarily much further than to their friends’ friends, who are still disproportionately likely to be geographically proximate to them. This is unfortunate for fundraisers located in poorer counties, but consistent with a wealth of research showing that digital media tend to fall short of expectations in overcoming spatial inequalities. Further emphasizing the spatially contingent nature of medical crowdfunding, we found that there were more successful campaigns in counties that were wealthier and healthier and had relatively more people working in information industries. We also found that campaigns initiated in counties with high numbers of social associations were relatively more likely to succeed. Studies of other types of crowdfunding have uncovered similar spatial inequalities (e.g., Davies, Citation2015; Mollick, Citation2014).
An entrepreneurial safety net
To illustrate the interplay of location effects and individual agency in determining medical crowdfunding success, we can compare the least privileged counties with the most privileged ones, defined as being below/above median on all of the aforementioned four county-level determinants of crowdfunding success. Fundraisers from the most privileged counties (n = 99) set much bigger funding goals on average ($85,266) than those from the least privileged counties (n = 72; $54,942), but raised on average only somewhat more money ($52,980 vs. $44,389). Campaigns from the least privileged counties were shared on average 1830 times, which is about 780 more than campaigns from the most privileged counties (1049). All comparisons are statistically significant at the p<.05 level (Appendix F). One possible interpretation is that these fundraisers from less privileged locations had to some extent succeeded in compensating for their disadvantage by making more or better use of the technological affordances presented to them; that is, by working harder for their healthcare.
Overall, medical crowdfunding seems to serve as a new safety net institution for financing healthcare, which some people are resorting to as both formal and informal safety nets are failing them. It is distinct from formal safety nets in that it matches donors directly with beneficiaries. It is also distinct from conventional informal safety nets in that a large part of its success is based on making it possible for people in need to appeal to donors beyond their personal networks. Yet medical crowdfunding does not overcome distance altogether: success is still influenced by how well-off the fundraiser’s local community is, probably in part because the appeal does not in reality reach undefined crowds across the Internet. Areas of greatest need – the poorest, sickest, and least socially connected counties – have the lowest numbers of successful campaigns. This places doubts on medical crowdfunding’s transformative potential.
Having said that, the behaviors and characteristics of the individual campaigns and fundraisers explained more of the variance in outcomes than county-level factors did. By crafting detailed messages, posting lots of photos, and sharing their campaigns on social media, fundraisers can significantly influence their chances of success. One way of characterizing medical crowdfunding is thus that it is an entrepreneurial safety net: one where protection is not afforded universally or on the basis of need, but on the basis of one’s ability to appeal to the audience and out-compete rivaling needfuls. Since success in such competition is likely to depend on similar personal characteristics and endowments as success in the market economy more generally, crowdfunding seems poorly positioned to provide protection for those who most need it.
Limitations and future research
As one of the very first quantitative studies on charitable crowdfunding, and the first one to consider broader societal factors, this study was exploratory; we for instance experimented with different model specifications to detect nonlinear relationships. As the body of evidence on charitable crowdfunding builds up, future studies should consider pre-registering their hypotheses. They could also focus on specific regional variables and develop a best-fit model. As acknowledged earlier, our measures are far from perfect. Much work could be done experimenting with data on the types and distributions of health-specific NGOs and public health facilities across counties. Future research could move to state-level analysis, which could include state health expenditure, state safety net hospital access, and political opinion factors. Content analysis could be used to add variables to the campaign-level data, such as race, gender, fundraiser age (Barcelos & Budge, Citation2019), type of illness (e.g., chronic disease vs. acute disease) (Berliner & Kenworthy, Citation2017; Sisler, Citation2012), and types of treatment sought (e.g., experimental treatments), and to see how those campaign features interact with society-level factors to predict success. A potential problem with using goal attainment as a measure of success is that it could also reflect more modest or more skilled goal setting. Future work could also consider subjective measures of success, such as fundraisers’ and donors’ satisfaction, sense of achievement, and self-efficacy (Shneor & Vik, Citation2020). Better understanding of these mechanisms could also potentially allow platform designers to reduce barriers that cause disadvantage.
Future research could also consider how other types of crowdfunding besides charitable crowdfunding may be altering the institutional makeup of health finance; for instance, peer-to-peer lending platforms can also be used for medical expenditures (Chen et al., Citation2020), while equity-based crowdfunding platforms are supporting companies seeking to develop new healthcare technologies (Bassani et al., Citation2019).
Acknowledgements
The authors wish to thank Jonathan Bright, Patrick Gildersleve, Otto Kässi, Fabian Stephany, and two anonymous reviewers for their valuable comments and advice at different stages of the research.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Notes on contributors
Sumin Lee
Sumin Lee is a DPhil candidate at the Oxford Internet Institute, University of Oxford. Her research interests center around information and communications technologies and prosocial behaviours online. In particular, she is interested in how the society and platforms shape one's social and economic actions that concern well-being and welfare of another.
Vili Lehdonvirta
Vili Lehdonvirta is Professor of Economic Sociology and Digital Social Research at the Oxford Internet Institute, University of Oxford. Lehdonvirta is an economic sociologist whose research focuses on digital technologies, such as apps, platforms, and marketplaces - how they are governed, how they shape the organization of economic activities, and with what implications to workers, consumers, businesses, and policy.
References
- ABC News. (2019a, March 26). GoFundMe bans anti-vaxxers in fight against vaccine “misinformation.” ABC News (Australian Broadcasting Corporation). Retrieved from https://www.abc.net.au/news/2019-03-26/gofundme-crackdown-anti-vaccination-campaigns-social-media/10936724
- ABC News. (2019b, November 17). Crowdfunding platform GoFundMe helps those in need — but there’s a forgotten side. ABC News (Australian Broadcasting Corporation). Retrieved from https://www.abc.net.au/news/2019-11-17/gofundme-folau-factor-helped-marko-but-not-raaf-vet/11696444.
- Agrawal, A., Catalini, C., & Goldfarb, A. (2011). The Geography of Crowdfunding (National Bureau of Economic Research Working Paper No.16820). https://doi.org/https://doi.org/10.3386/w16820
- Barcelos, C. A., & Budge, S. L. (2019). Inequalities in crowdfunding for Transgender health care. Transgender Health, 4(1), 81–88. https://doi.org/https://doi.org/10.1089/trgh.2018.0044
- Bassani, G., Marinelli, N., & Vismara, S. (2019). Crowdfunding in healthcare. Journal of Technology Transfer, 44(4), 1290–1310. https://doi.org/https://doi.org/10.1007/s10961-018-9663-7
- Bekkers, R., & Wiepking, P. (2010). A literature Review of empirical studies of Philanthropy: Eight mechanisms that Drive charitable giving. Nonprofit and Voluntary Sector Quarterly, 40(5), 924–973. https://doi.org/https://doi.org/10.1177/0899764010380927
- Belleflamme, P., Lambert, T., & Schwienbacher, A. (2014). Crowdfunding: Tapping the right crowd. Journal of Business Venturing, 29(5), 585–609. https://doi.org/https://doi.org/10.1016/j.jbusvent.2013.07.003
- Berchick, E. R., Hood, E., & Barnett, J. C. (2018). Current Population Reports,P60-264, Health Insurance Coverage in the United States: 2017. Washington, DC.
- Berliner, L. S., & Kenworthy, N. J. (2017). Producing a worthy illness: Personal crowdfunding amidst financial crisis. Social Science & Medicine, 187, 233–242. https://doi.org/https://doi.org/10.1016/j.socscimed.2017.02.008
- Bi, S., Liu, Z., & Usman, K. (2017). The influence of online information on investing decisions of reward-based crowdfunding. Journal of Business Research, 71, 10–18. https://doi.org/https://doi.org/10.1016/j.jbusres.2016.10.001
- Bielefeld, W., Rooney, P., & Steinberg, K. (2005). How Do need, Capacity, geography, and Politics influence giving?. In A. Brooks (Ed.), Gifts of Money in Americas Communities (pp. 127–158). Rowman & Littlefield Publishers.
- Blakemore, K., & Warwick-Booth, L. (2013). Social Policy: An Introduction. McGraw-Hill Education.
- Blumberg, L. J., Holahan, J., Karpman, M., & Elmendorf, C. (2018). Characteristics of the Remaining Uninsured: An Update. www.healthpolicycenter.org
- Bluth, R. (2019, January 16). GoFundMeCEO: ‘Gigantic Gaps’ In Health System Showing Up In Crowdfunding. Kaiser Health News. https://khn.org/news/gofundme-ceo-gigantic-gaps-in-health-system-showing-up-in-crowdfunding/
- Bone, J., & Baeck, P. (2016). Crowdfunding good causes. https://www.nesta.org.uk/sites/default/files/crowdfunding_good_causes-2016.pdf
- Borst, I., Moser, C., & Ferguson, J. (2018). From friendfunding to crowdfunding: Relevance of relationships, social media, and platform activities to crowdfunding performance. New Media & Society, 20(4), 1396–1414. https://doi.org/https://doi.org/10.1177/1461444817694599.
- Bouncken, R. B., Komorek, M., & Kraus, S. (2015). Crowdfunding: The current state of research. International Business & Economics Research Journal (IBER), 14(3), 407–416. https://doi.org/https://doi.org/10.19030/iber.v14i3.9206.
- Burtch, G., & Chan, J. (2014, December). Reducing medical Bankruptcy through crowdfunding: Evidence from GiveForward. Proceedings of the International Conference on Information Systems (ICIS), Association for Information Systems.
- Chen, X., Huang, B., & Ye, D. (2020). Gender gap in peer-to-peer lending: Evidence from China. Journal of Banking and Finance, 112, 105633. https://doi.org/https://doi.org/10.1016/j.jbankfin.2019.105633
- Cohen, J., Cohen, P., West, S., & Aiken, L. (2013). Applied multiple regression/correlation analysis for the Behavioral sciences. Routledge.
- Coleman, J. S. (1988). Social capital in the creation of human capital. American Journal of Sociology, 94, S95–S120. https://doi.org/https://doi.org/10.1086/228943.
- Collins, S. R., Bhupal, H. K., & Doty, M. M. (2019). Issue Brief - Health Insurance Coverage Eight Years After the ACA. https://www.commonwealthfund.org/publications/issue-briefs/2019/feb/health-insurance-coverage-eight-years-after-aca
- The Commonwealth Fund. (2020, June 5). International Health Care System Profiles - United States. Retrieved October 8, 2020, from https://www.commonwealthfund.org/international-health-policy-center/countries/united-states
- Cordova, A., Dolci, J., & Gianfrate, G. (2015). The determinants of crowdfunding success: Evidence from technology projects. Procedia-Social and Behavioral Sciences, 181, 115–124. https://doi.org/https://doi.org/10.1016/j.sbspro.2015.04.872
- Davies, R. (2015). Three provocations for civic crowdfunding. Information, Communication & Society, 18(3), 342–355. https://doi.org/https://doi.org/10.1080/1369118X.2014.989878
- Department for Professional Employees. (2016). The U.S. Health Care System: An International Perspective. https://dpeaflcio.org/programs-publications/issue-fact-sheets/the-u-s-health-care-system-an-international-perspective/
- Donelan, K., Hill, C. A., Hoffman, C., Scoles, K., Feldman, P. H., Levine, C., & Gould, D. (2002). Challenged to care: Informal caregivers in a changing health system. Health Affairs, 21(4), 222–231. https://doi.org/https://doi.org/10.1377/hlthaff.21.4.222
- Durand, W. M., Peters, J. L., Eltorai, A. E. M., Kalagara, S., Osband, A. J., & Daniels, A. H. (2018). Medical crowdfunding for organ transplantation. Clinical Transplantation, 32(6), e13267. https://doi.org/https://doi.org/10.1111/ctr.13267
- Dushnitsky, G., & Marom, D. (2013). Crowd Monogamy. Business Strategy Review, 24(4), 24–26. https://doi.org/https://doi.org/10.1111/j.1467-8616.2013.00990.x
- English, R. (2013). Rent-a-crowd? Crowdfunding academic research. First Monday, 19(1), https://doi.org/https://doi.org/10.5210/fm.v19i1.4818
- Gilbert, N., & Terrell, P. (2002). Dimensions of social welfare policy. Allyn & Bacon.
- Giudici, G., Guerini, M., & Rossi-Lamastra, C. (2013). Why crowdfunding projects can succeed: The role of proponent’s individual and territorial social capital. SSRN Electronic Journal, 2255944, 1–20. https://doi.org/https://doi.org/10.2139/ssrn.2255944
- Gleasure, R., & Feller, J. (2016). Does Heart or Head rule donor behaviors in charitable crowdfunding markets? International Journal of Electronic Commerce, 20(4), 499–524. https://doi.org/https://doi.org/10.1080/10864415.2016.1171975
- Glennerster, H. (2003). Understanding the financing of welfare. The Policy Press and the Social Policy Association.
- GoFundMe. (2020). What countries are supported on GoFundMe? Retrieved August 11, 2020, from https://support.gofundme.com/hc/en-us/articles/360001972748.
- Gonzales, A. L., Kwon, E. Y., Lynch, T., & Fritz, N. (2016). “Better everyone should know our business than we lose our house”: costs and benefits of medical crowdfunding for support, privacy, and identity. New Media & Society, 20(2), 641–658. https://doi.org/https://doi.org/10.1177/1461444816667723
- Granovetter, M. (1985). Economic action and social structure: The problem of Embeddedness. American Journal of Sociology, 91(3), 481–510. https://doi.org/https://doi.org/10.1086/228311
- Harries, A. (2017, February 13). How Crowdfunding Platform GoFundMeHas Created A $3 Billion Digital Safety Net - The future of business. Fast Company. https://www.fastcompany.com/3067472/how-crowdfunding-platform-gofundme-has-created-a-3-billion-digital
- Hodgson, G. M. (2006). What are institutions. Journal of Economic Issues, 40(1), 1–26. https://doi.org/https://doi.org/10.1080/00213624.2006.11506879
- Howe, J. (2006, June 2). Crowdsourcing: Crowdsourcing: A Definition. Retrieved September 28, 2020, from https://crowdsourcing.typepad.com/cs/2006/06/crowdsourcing_a.html
- Hui, J. S., & Gerber, E. M. (2015, February). Crowdfunding science: Sharing research with an extended audience. CSCW 2015 - Proceedings of the 2015 ACM International Conference on Computer-supported Cooperative work and social Computing (pp. 31–43). Association for Computing Machinery. https://doi.org/https://doi.org/10.1145/2675133.2675188
- Jopson, B. (2018, January 11). Why are so many Americans crowdfunding their healthcare? Financial Times. https://www.ft.com/content/b99a81be-f591-11e7-88f7-5465a6ce1a00
- Kang, L., Jiang, Q., & Tan, C. H. (2017). Remarkable advocates: An investigation of geographic distance and social capital for crowdfunding. Information and Management, 54(3), 336–348. https://doi.org/https://doi.org/10.1016/j.im.2016.09.001
- Kherallah, M., & Kirsten, J. F. (2002). The new institutional economics: Applications for agricultural policy research in developing countries. Agrekon, 41(2), 110–133. https://doi.org/https://doi.org/10.1080/03031853.2002.9523589
- Kim, J., Kong, H., Karahalios, K., Fu, W., & Hong, H. (2016, May). The power of collective endorsements: Credibility factors in medical crowdfunding campaigns. Proceedings of the 2016 CHI Conference on Human Factors in Computing Systems (pp. 4538–4549). Association for Computing Machinery. https://doi.org/https://doi.org/10.1145/2858036.2858289
- Kim, J., Vaccaro, K., Karahalios, K., & Hong, H. (2017, February). “Not by money alone”: social support opportunities in medical crowdfunding campaigns. Proceedings of the ACM Conference on Computer supported Cooperative work, CSCW (pp. 1997–2009). Association for Computing Machinery. https://doi.org/https://doi.org/10.1145/2998181.2998245
- Kshetri, N. (2015). Success of crowd-based Online technology in fundraising: An institutional perspective. Journal of International Management, 21(2), 100–116. https://doi.org/https://doi.org/10.1016/j.intman.2015.03.004
- List, J. A. (2011). The market for charitable giving. Journal of Economic Perspectives, 25(2), 157–180. https://doi.org/https://doi.org/10.1257/jep.25.2.157
- Liu, L., Suh, A., & Wagner, C. (2017, January). Donation behavior in Online Micro charities: An Investigation of charitable crowdfunding projects. Proceedings of the 50th Hawaii International Conference on system sciences.
- Lobao, L. M., Hooks, G., & Tickamyer, A. R. (2007). The sociology of spatial inequality. SUNY Press. https://doi.org/https://doi.org/10.1080/00045600801944194
- Lu, C. T., Xie, S., Kong, X., & Yu, P. S. (2014, February). Inferring the impacts of social media on crowdfunding. WSDM 2014 - Proceedings of the 7th ACM International Conference on Web search and data Mining (pp. 573–582). Association for Computing Machinery. https://doi.org/https://doi.org/10.1145/2556195.2556251
- Mollick, E. (2014). The dynamics of crowdfunding: An exploratory study. Journal of Business Venturing, 29(1), 1–16. https://doi.org/https://doi.org/10.1016/j.jbusvent.2013.06.005
- Morduch, J. (1999). Between the state and the market: Can informal insurance Patch the safety Net? The World Bank Research Observer, 14(2), 187–207. https://doi.org/https://doi.org/10.1093/wbro/14.2.187
- Narayan, D. (1999). Bonds and bridges: Social capital and poverty. World Bank Publications (Vol. 2167). https://doi.org/https://doi.org/10.1086/452436
- North, D. (1991). Institutions, institutional Change, and economic performance. The Journal of Economic Perspective, 5(1), 97–112. https://doi.org/https://doi.org/10.2307/2234910
- North, D. (1995). The New Institutional Economics and Third World Development. The New Institutional Economics and Third World Development (Vol. 21). https://doi.org/https://doi.org/10.1080/713701070
- Paxton, P. (1999). Is social capital declining in the United States? A multiple indicator assessment. American Journal of Sociology, 105(1), 88–127. https://doi.org/https://doi.org/10.1086/210268
- Payne, A., & Smith, J. (2015). Does income inequality increase charitable giving? Canadian Journal of Economics, 48(2), 793–818. https://doi.org/https://doi.org/10.1111/caje.12144
- Ren, J., Raghupathi, V., & Raghupathi, W. (2020). Understanding the dimensions of medical crowdfunding: A visual analytics approach. Journal of Medical Internet Research, 22(7), e18813. https://doi.org/https://doi.org/10.2196/18813
- Renwick, M. J., & Mossialos, E. (2017). Crowdfunding our health: Economic risks and benefits. Social Science and Medicine, 191, 48–56. https://doi.org/https://doi.org/10.1016/j.socscimed.2017.08.035
- Saleh, S. N., Ajufo, E., Bch, B. M., Lehmann, C. U., & Medford, R. J. (2020). Crowdfunding Medical Care: A Comparison of Online Medical Fundraising in Canada, the United Kingdom, and the United States. MedRxiv. https://doi.org/https://doi.org/10.1101/2020.03.26.20044669
- Shneor, R., & Vik, A. A. (2020). Crowdfunding success: A systematic literature review 2010–2017. Baltic Journal of Management, 15(2), 149–182. https://doi.org/https://doi.org/10.1108/BJM-04-2019-0148.
- Sisler, J. (2012). Crowdfunding for medical expenses. CMAJ : Canadian Medical Association Journal, 184(2), E123–E124. https://doi.org/https://doi.org/10.1503/cmaj.109-4084
- Slack, T., Myers, C. A., Martin, C. K., & Heymsfield, S. B. (2014). The geographic concentration of us adult obesity prevalence and associated social, economic, and environmental factors. Obesity, 22(3), 868–874. https://doi.org/https://doi.org/10.1002/oby.20502
- Snyder, J., Crooks, V. A., Mathers, A., & Chow-White, P. (2017). Appealing to the crowd: Ethical justifications in Canadian medical crowdfunding campaigns. Journal of Medical Ethics, 43(6), 364–367. https://doi.org/https://doi.org/10.1136/medethics-2016-103933
- Snyder, J., Mathers, A., & Crooks, V. A. (2016). Fund my treatment!: A call for ethics-focused social science research into the use of crowdfunding for medical care. Social Science and Medicine, 169, 27–30. https://doi.org/https://doi.org/10.1016/j.socscimed.2016.09.024
- Tanaka, K. G., & Voida, A. (2016, May). Legitimacy work: Invisible work in Philanthropic crowdfunding. Proceedings of the 2016 CHI Conference on human factors in Computing Systems (pp. 4550–4561). Association for Computing Machinery. https://doi.org/https://doi.org/10.1145/2858036.2858110
- Tomczak, A., & Brem, A. (2013). A conceptualized investment model of crowdfunding. Venture Capital, 15(4), 335–359. https://doi.org/https://doi.org/10.1080/13691066.2013.847614
- Verbakel, E. (2018). How to understand informal caregiving patterns in Europe? The role of formal long-term care provisions and family care norms. Scandinavian Journal of Public Health, 46(4), 436–447. https://doi.org/https://doi.org/10.1177/1403494817726197
- Vox, F., Folkers, K. M. B., Turi, A., & Caplan, A. L. (2018). Medical crowdfunding for scientifically Unsupported or potentially Dangerous treatments. JAMA - Journal of the American Medical Association, 320(16), 1705–1706. https://doi.org/https://doi.org/10.1001/jama.2018.10264
- Wang, T., Li, Y., Kang, M., & Zheng, H. (2019). Exploring individuals’ behavioral intentions toward donation crowdfunding: Evidence from China. Industrial Management and Data Systems, 119(7), 1515–1534. https://doi.org/https://doi.org/10.1108/IMDS-10-2018-0451
- Williamson, O. E. (2000). The New institutional Economics: Taking Stock, Looking Ahead. Journal of Economic Literature, 38(3), 595–613. https://doi.org/https://doi.org/10.2307/2565421
