
ABSTRACT
The purpose of this study was to investigate the associations between self-reported schoolwork pressure and family factors with psychosomatic problems, and to investigate possible moderators of these associations. We examined self-efficacy as a personal resource that may be directly associated with psychosomatic problems, as well as serve as a moderator between stress exposure and psychosomatic problems. Furthermore, we examined sex as a possible moderator. The data were collected in 2010 among 2,004 pupils, aged between 13 and 15 years, in all schools in the municipality of Karlstad, Sweden. Multinomial logistic regression analysis showed that self-efficacy did not moderate the relationships between any of the school- and family-related factors and psychosomatic problems. However, self-efficacy had a direct effect on psychosomatic problems. Based on the results from the study, we concluded that health promoting and preventive work by the school health team should focus on strengthening pupils’ self-efficacy and target schoolwork pressure. Special attention needs to be given to girls and adolescents living with a single parent or no parents.
SAMMANFATTNING
Syftet med denna studie var att undersöka relationen mellan självrapporterad press i skolan, familjefaktorer och psykosomatiska besvär samt undersöka eventuella moderatorer mellan dessa faktorer. Vi undersökte tilltro till sin förmåga som en personlig resurs som kan ha en direkt relation till psykosomatiska besvär och också fungera som en moderator mellan påfrestningar och psykosomatiska besvär. Dessutom undersökte vi huruvida kön inverkar på relationen mellan påfrestningar och psykosomatiska besvär. Data samlades in 2010 i alla kommunala skolor i Karlstad kommun i Sverige. Enkäten besvarades av 2004 elever mellan 13 och 15 år. Multinomial logistisk regressions analys visade att tilltro till sin förmåga inte påverkade relationen mellan några av de skol- eller familjerelaterade påfrestningarna och psykosomatiska besvär. Tilltro till sin förmåga hade dock en direkt inverkan på psykosomatiska besvär. Baserat på resultaten från studien är våra slutsatser att Elevhälsans förebyggande och hälsofrämjande arbete bör fokusera på att stärka elevers tilltro till sin förmåga samt bekämpa press i skolan. Dessutom behövs ett särskilt fokus på tjejer då de tillhör en riskgrupp i vissa avseenden samt på ungdomar som bor med en ensamstående förälder eller de som bor utan sina föräldrar.
Introduction
Research shows that an increasing proportion of adolescents is reporting mental health problems. A systematic literature review showed that the prevalence of externalising symptoms, for example defiance, aggressiveness and impulsiveness, appears to be stable whereas internalising problems, for example psychosomatic problems, anxiety and depression seem to have increased in the twenty-first century, particularly in adolescent girls (Bor, Dean, Najman, & Hayatbakhsh, Citation2014). In Sweden, research on trends has shown increasing rates of older adolescents reporting internalising mental health problems since the 1980s (Bremberg, Citation2015; Petersen et al., Citation2010). The Public Health Agency of Sweden (Citation2018) reported that the proportion of Swedish girls and boys aged 13 and 15 years reporting recurrent psychosomatic problems has doubled since the mid-1980s. Previous research demonstrated that school-related stress may be connected to mental health problems (e.g. Eriksson & Sellström, Citation2010; Hjern, Alfven, & Östberg, Citation2008; Torsheim, Aaroe, & Wold, Citation2003), and a report from the Organisation for Economic Co-operation and Development (OECD) (Citation2013) concluded that the Swedish school health service does not have sufficient resources to contend with this increase in mental health problems among adolescents.
Research showed that low or incomplete marks on leaving compulsory school at 16 years of age increased the risk of future social problems (such as suicide, criminality and drug abuse) (Vinnerljung, Hjern, & Berlin, Citation2010). Backlund, Högdin, and Weitz Spånberger (Citation2017) declared that, to ensure that young people are not faced with social- and health-related problems in the future, one of the most important areas for school social work is to ensure that pupils complete their education. In Sweden, the school is responsible for upholding the right of all children to an equal education, regardless of their social background. The intention of the Swedish Education Act (SFS Citation2010:Citation800) is that school health teams, including school social workers, should primarily work with prevention and health promotion. One of school social workers’ responsibilities is to ensure that all pupils attain the required knowledge and that they develop socially and emotionally in an environment that promotes learning. School social workers are also expected to contribute with knowledge about risks and protective factors concerning health, social situation, learning and development (National Board of Health Welfare and National Agency for Education, Citation2016). To prevent mental health problems and decrease the risk of future social problems, we need to know which factors underlie the development of mental health problems.
The purpose of this study is to investigate the associations between school- and family-related stress with psychosomatic problems, and investigate possible moderators of these relationships. Below, the theoretical framework for this study and its applications in a model of analysis is described.
Theoretical framework
This study is rooted in Pearlin’s stress process model (Citation1989) and the work by Turner (Citation2010) elaborating on this model. Pearlin’s idea was that the process of social stress could be seen as combining three major conceptual domains: the source of stress, the mediators (and moderators) of stress and the manifestation of stress. The manifestation of stress can be either psychological, physical or behavioural in nature. Aspects that play a mediating or moderating role between the stress exposure and the manifestation included aspects such as self-concepts, coping styles and social support. Turner (Citation2010) contributed to the development of the model by expanding the range of resources that could be included in the study of stress and adverse outcomes. Stress exposure arises out of the context of people’s lives, and these experiences can be traced back to social structures, such as systems of stratification including social and economic class, race and ethnicity, gender and age (Pearlin, Citation1989). Pearlin (Citation1989) also argued that stressful experiences may occur in the context of social roles.
The model of analysis
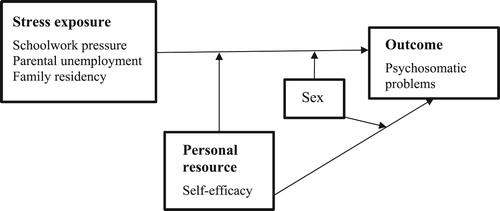
Based on Pearlin’s theoretical work, we constructed a model of analysis according to the purpose of the study. The model integrates the concepts of stress exposure, moderators and the manifestation of stress in the form of psychosomatic problems. We investigated the relationship between different kinds of stress exposure and psychosomatic problems in adolescents, and whether these relationships were conditional upon personal resources and sex. We also investigated the relationship between personal resources and psychosomatic problems, and examined if this was conditional upon adolescents’ sex. Below we describe the different domains included in the model.
Stress exposure
According to the stress process model (Pearlin, Citation1989; Turner, Citation2010), stress exposure can take the form of lifetime traumas, chronic stress and recent stressful events such as job loss or divorce in adults’ lives or school transitions for children and adolescents. Chronic strain is one central aspect of stress exposure. Chronic strains can be stressors that arise within the boundaries of major social roles (Pearlin, Citation1989), and could be linked to difficulties in the job, marriage, parenthood or friendship. Apart from chronic strain being found in connection to major social roles, Pearlin (Citation1989) also acknowledged that severe strains could be found in the experience of living in or close to poverty or having a serious chronic illness. One could argue from a theoretical standpoint that adolescents’ friendships and relations to teachers could be potentially stressful. School-related stress in the form of social relations to peers and teachers have been well studied (e.g. Beckman, Hagquist, & Hellström, Citation2012; Murberg & Bru, Citation2004; Torsheim et al., Citation2003). Pearlin (Citation1989) also described the importance of values (what is socially good, desirable and prized) when it comes to identification and specification of stressors. It has been argued that we currently live in a knowledge society and thus children’s and adolescents’ education plays a pivotal role in young people’s lives (Backe-Hansen & Frønes, Citation2012). It follows that schoolwork pressure can be considered a stressor in adolescents’ lives.
Another aspect of the stress process model is that disruption in one context is likely to cause disruption in another context of a person’s life (Pearlin, Citation1989). Therefore, it is important not to just look at one setting in adolescents’ lives when it comes to stress and adverse outcomes. Another researcher that linked different contexts and how they affect children’s and adolescents’ development is Bronfenbrenner (Citation1977, Citation1994). School and family, among others, are contexts that Bronfenbrenner referred to as microsystems, social environments within which a majority of children’s and adolescent’s interaction take place. In our model of analysis, we therefore include stressors from another central area in adolescents’ lives, namely family. In addition, a principal feature of the stress process model is to understand how social structures have a pervasive influence on individuals’ exposure to stressors and their responses to these experiences (Avison, Citation2009). Therefore, we included family-level factors that may influence adolescents’ lives, and could be considered a part of the process of developing mental health problems.
School-related stress exposure and mental health problems
In Sweden, school demands have increased, according to adolescent self-reports between 1988 and 2011 (Nygren & Hagquist, Citation2017). An OECD report (Citation2016) stated that, in Sweden, pupils aged 11–15 from lower socioeconomic backgrounds feel more pressure from schoolwork than those from higher socioeconomic backgrounds. Previous research showed that schoolwork pressure relates to an increased risk of mental health problems (Gerber & Pühse, Citation2008; Hjern et al., Citation2008; Murberg & Bru, Citation2004; Natvig, Albrektsen, Anderssen, & Qvarnstrom, Citation1999). Results from the Swedish Health Behaviour of School-aged Children study showed that the proportion of adolescents experiencing school-related stress was greatest among 15-year-olds (Public Health Agency of Sweden, Citation2014). Between 1997 and 2014, the proportion of girls who reported feeling stressed by their schoolwork ranged from 50% to almost 70% and for boys the proportion ranged from 30% to 45%. Because of this evidence for sex differences, we investigate sex as a possible moderator between schoolwork pressure and psychosomatic problems.
Family-related stress exposure and mental health problems
From a theoretical standpoint, a stressful event can lead to chronic strain and vice versa (Pearlin, Citation1989). Parental unemployment might be an event in parents’ lives that might result in chronic strain for adolescents. Parental unemployment implies lost earnings, which in turn could lead to a decrease in both the quality and quantity of material resources (Mörk, Sjögren, & Svaleryd, Citation2014). According to Mörk et al. (Citation2014) parents could also suffer from status loss, stress, poor health or conflicts between parents, which in turn could affect the home environment for adolescents. Regarding the relation between parental unemployment and mental health problems, studies showed conflicting results. Some observed that parental unemployment was associated with a higher prevalence of psychosomatic problems in children and adolescents from Nordic countries (Petersen et al., Citation2010) and with depressive symptoms in Finnish and Norwegian adolescents (Fröjd, Marttunen, Pelkonen, Von der Pahlen, & Kaltiala-Heino, Citation2006; Kaltiala-Heino, Rimpelä, Rantanen, & Laippala, Citation2001; Sund, Larsson, & Wichstrøm, Citation2003). Some of those results showed different associations between boys and girls. However, a Hungarian study (Piko & Fitzpatrick, Citation2001) showed that adolescents with unemployed mothers reported fewer psychosomatic symptoms. Other research showed no statistically significant correlations between parental unemployment and mental health problems among adolescents (Östberg, Alfven, & Hjern, Citation2006; Sleskova et al., Citation2006). One study examining potential risk factors for mental health problems among adolescents found that parental unemployment was not a significant predictor of adolescents’ mental health after adjusting for other factors such as conflicts in the family, parental strain and living with a step-parent (Wille, Bettge, & Ravens-Sieberer, Citation2008).
Another factor related to the family situation that may affect adolescents is family residency. The relationship between family residency and mental health problems has been studied using different outcomes and different definitions, and classifications. Some studies compared single-parent families with two-parent families, whereas others included stepparent families and alternating residency (living an equal time with both parents, alternating between households). Living in non-intact families compared to intact families, research showed associations with depressive symptoms in Finnish adolescents (Fröjd et al., Citation2006; Kaltiala-Heino et al., Citation2001), and an increased probability of psychosomatic problems for children and adolescents in the Nordic countries (Pedersen & Madsen, Citation2002), and also for Swedish adolescents (Östberg et al., Citation2006). One study concluded that family type contributed more to the distribution of ill health among children in the Nordic countries than did parental unemployment (Pedersen & Madsen, Citation2002). As with the association between parental unemployment and mental health problems, the relation between family residency and mental health problems may be different for boys and girls (Bergman & Scott, Citation2001; Fröjd et al., Citation2006). Therefore, we included sex as a potential moderator of the relationship between family-related stressors (parental unemployment and family residency) and psychosomatic problems.
Personal resources
According to Turner’s (Citation2010) elaborated theoretical model, it is hypothesised that concepts like sense of control, self-esteem, emotional reliance, and mattering (belief in our own relevance to others) are linked to mental health problems. In particular, these concepts have shown either moderating or mediating effects on the relationship between stress exposure and mental health problems (Turner, Citation2010). Turner (Citation2010) pointed out that other personal resources and attributes may influence mental health problems directly or affect stress exposure and its relation to mental health problems, but this has not received as much attention in research. Therefore, we included self-efficacy in our model, both as a direct effect and as a moderator of the relation between stress exposure and psychosomatic problems. Moreover, it is a stated goal in the Swedish school curriculum to ensure that pupils develop and maintain self-efficacy (Swedish National Agency for Education, Citation2016).
Self-efficacy and mental health
Self-efficacy is defined as an individual’s belief in their ability to perform the behaviours required to produce a desired outcome (Bandura, Citation1977). Drawing from the stress process model, we hypothesised that self-efficacy could be a personal resource. Research showed that self-efficacy is directly associated with mental health; however, mixed results were reported regarding the relation between psychosomatic problems and self-efficacy. One Norwegian study (Natvig et al., Citation1999) found that, for girls, an increasing degree of general self-efficacy increased the risk of feeling low, having backaches and experiencing dizziness. Results from the same study also showed that the association between school alienation and psychosomatic problems was strongest among pupils with low self-efficacy. In another study, the same research group found that adolescents’ self-efficacy had a positive effect on their wellbeing (Natvig, Albrektsen, & Qvarnstrøm, Citation2003). Therefore, self-efficacy was included both as a personal resource that may moderate the relation between stress exposure and psychosomatic problems, and as a direct effect on psychosomatic problems. In addition, research showed that self-efficacy may be higher among boys compared to girls (Lönnfjord & Hagquist, Citation2017). Therefore, we investigated whether sex was a possible moderator between self-efficacy and psychosomatic problems. The model of analysis is depicted in .
Figure 1. Model of analysis.
Method
Material
Data were collected in conjunction with a Swedish national project for the prevention of mental health problems in school (Public Health Agency of Sweden, Citation2012). At the local level, the project was a collaboration between Karlstad municipality and the Centre for Research on Child and Adolescents Mental Health (CFBUPH) at Karlstad University and carried out between 2009 and 2012. Data on social relationships, classroom climate, bullying and mental health were collected, see e.g. Beckman (Citation2013) for more information about the entire local project and the different data collections that were conducted.
Data collection
The data used in this study were collected with questionnaires in 2010 among pupils aged between 13 and 15 years (Swedish school year 7–9) in all municipality-run schools in Karlstad municipality, Sweden. A research team at CFBUPH carried out the data collection. All pupils received written and oral information about the aim of the study, stating that their participation was voluntary and that they had the right to withdraw their participation at any time. For children under the age of 15, written information was given to the parents, and those who did not want their child to participate were asked to notify the class teacher. shows the number of participants and non-participants.
Table 1. Participants and non-participants.
Measures and variable definitions
Psychosomatic problems
The outcome measure used was the Psychosomatic Problems Scale (Hagquist, Citation2001), which has been shown to be a reliable and valid scale for measuring psychosomatic problems among adolescents (Hagquist, Citation2008). It is an eight-item scale (e.g. Suffered from headaches, Felt sad) with five response options (Never to Always). A higher score implies more psychosomatic problems. The psychometric properties of the scale were analysed using Rasch Measurment Theory (Andrich, Citation1988; Rasch, Citation1960/Citation1980). The Rasch model enables independent and separate estimations of item and person parameters, which is a requirement for invariant measurement. This means that the person parameters do not depend on which items are used in the estimation. Given that the data fit the Rasch model, linear person measures are provided that do not depend on the distribution of the persons in the sample. These person measures are nonlinearly transformed raw scores (logit values) (Andrich, Citation1988).
Because the Psychosomatic Problems scale showed good psychometric properties, the person estimates generated by the Rasch analysis were used in the statistical analysis. The logit values ranged from −4.873 to 4.524. In order to compare distinct groups of adolescents according to their degree of psychosomatic problems, i.e. comparing adolescents at both ends of the continuum, the variable was trichotomised, based on percentile values. Adolescents as close to and over the 75th percentile constituted the category Higher degree of psychosomatic problems, adolescents above the 25th but below the 75th percentile constitute the category Moderate degree of psychosomatic problems, and adolescents as close to and below the 25th percentile constituted the category Lower degree of psychosomatic problems. Similar categorisations of variables measuring psychosomatic problems have been used in previous studies (e.g. Carlerby, Viitasara, Knutsson, & Gillander Gådin, Citation2012; Hellström, Beckman, & Hagquist, Citation2017).
Schoolwork pressure
To measure schoolwork pressure, we chose relevant variables based on questions that had been used in previous research to measure different aspects of school-related stress (Murberg & Bru, Citation2004). The questionnaire used in the data collection included 16 questions about school-related stress in areas such as difficulties with peers in school, worries about school achievement, schoolwork pressure and conflict with parents and/or teachers. There were five response options (Never to Always), with higher scores indicating a higher degree of school-related stress. In order to identify which questions could be used for a composite measure of school-relates stress, a psychometric analysis was carried out. Based on this analysis, four items were included in a measure we labelled schoolwork pressure. This four-item measure showed good fit to the Rasch model, had acceptable reliability, showed invariance among items and had a response format that worked well. The following items were used: You think that schoolwork has been too demanding, You have had too many things to do outside of school, You have not had enough help and guidance with your schoolwork, You have been concerned about schoolwork you have not done or that you have not done well. Since the data had an acceptable fit to the Rasch model, the person estimates were used in the statistical analysis, and the logit values ranged from −3.294 to 3.029. The variable on schoolwork pressure was trichotomised, following the same principles as described above for psychosomatic problems.
Self-efficacy
The Swedish version of the General Self-Efficacy (GSE) scale (Koskinen-Hagman, Schwarzer, & Jerusalem, Citation1999; Schwarzer & Jerusalem, Citation1995) was used to measure self-efficacy. It consists of ten items (e.g. It is easy for me to stick to my aims and accomplish my goals, I can solve most problems if I invest the necessary effort) with four response options (Not at all true to Exactly true). The responses to the items are summarised across respondents, yielding a total score between 10 and 40; higher scores indicate higher self-efficacy. The Swedish version of the GSE scale was previously psychometrically evaluated based on adolescent data (Lönnfjord & Hagquist, Citation2017). Item six (I can remain calm when facing difficulties because I can rely on my coping abilities) showed evidence of Differential Item Functioning [DIF] (Hagquist & Andrich, Citation2017) across sexes. Given the same location on the variable, boys scored higher than girls on that item. In order to resolve this DIF, item 6 was split into two sex-specific items, one for boys and one for girls. Hence, nine items were intact and one item split into two. This eleven-item measure was used. We judged the fit acceptable to the Rasch model thus the person estimates were used in the analysis and the logit values ranged from −5.270 to 5.864. The variable was trichotomised, following the same principles as described above for psychosomatic problems.
Parental unemployment
Parental unemployment was self-reported by adolescents. The variable used in the analysis was whether one or both parents were unemployed. The proportion of adolescents reporting one or both their parents as unemployed was 11.7%.
Type of family residency
The type of family residency variable consisted of two questions concerning the family situation. The responses to these two questions were recoded into one variable with the following categories (proportion of adolescents in parenthesis): Living with both parents (63.1%); Living with a single parent (15.8%) (either mother or father); Alternating residency (12.8%), such as one week with one parent, the next with the other parent (joint/shared physical custody/residence); Living mostly with one parent (6.8%); and Living with someone else or living alone (1.5%).
Statistical analysis
The analyses were conducted using the statistical software program SPSS, version 22. We used contingency tables to illustrate the different characteristics of the groups under comparison. Differences in proportions were tested using z-tests (two-tailed), and a p value of <0.05 was set as the level of statistical significance. We used multinomial logistic regression in the main analysis to examine the associations between psychosomatic problems and schoolwork pressure, parental unemployment, family residency and self-efficacy, focusing both on single main effects (model A) and a multivariate main effects model including all independent variables (model B). We adjusted for school year and sex. Associations between the variables were presented in odds ratios (OR) with 95% confidence intervals. In order to investigate possible moderating effects between the different independent variables and sex, and to investigate whether self-efficacy moderated the association between the other independent variables and psychosomatic problems, seven separate models including an interaction term were tested (schoolwork pressure by sex, parental unemployment by sex, family residency by sex, self-efficacy by sex, schoolwork pressure by self-efficacy, parental unemployment by self-efficacy and family residency by self-efficacy). The interactions were analysed using log likelihood ratio tests, comparing the multivariate main effects model (B) with each of the seven models with an interaction term, as listed above. Only one interaction effect was significant (self-efficacy by sex), and only these results are reported. In order to investigate contrasts between different combinations of sex and degree of self-efficacy, we performed manual calculations. First, logarithmic beta values for main and interaction effects were summarised to a total beta value for each subgroup. Second, the subgroup in focus was contrasted with a reference subgroup. Third, in order to get an odds ratio, the differences in beta value between the focus and reference groups were exponentiated.
Results
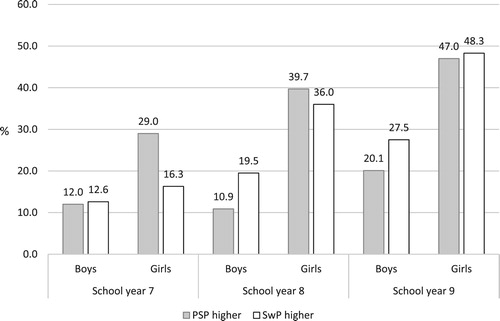
shows that girls reported having more psychosomatic problems compared to boys, and the difference was statistically significant. Also seen in , the proportion of adolescents having a higher degree of psychosomatic problems increases with age, and differences in proportions were statistically significant; in other words, the older the adolescents become, the more likely they are to report a higher degree of psychosomatic problems. Another notable result is that, among girls in school year 9, almost half were categorised as having a higher degree of psychosomatic problems. also shows that the experience of schoolwork pressure varied according to sex and age: girls reported a higher degree of schoolwork pressure than boys did, and the proportion of adolescents reporting a higher degree of schoolwork pressure increased with age. Both of these differences in proportions were statistically significant. The distribution of adolescents reporting lower self-efficacy did not differ significantly with regard to sex (boys 23.0%, girls 25.5%) or school year (boys year; 7: 21.8%, 8: 23.5%, 9: 23.7%, girls year; 7: 24.9%, 8: 28.3%, 9: 23.7%).
Figure 2. Proportions of adolescents categorised as having a higher degree of psychosomatic problems (PSP), and a higher degree of schoolwork pressure (SwP), broken down by sex and school year. Higher degree: 75th–100th percentile. Swedish school year 7 starts at 13 years, year 8 at 14 years and year 9 at 15 years.
presents the results from the multinomial logistic regression analysis investigating the relation between the explanatory variables schoolwork pressure, parental unemployment, family residency and self-efficacy and the outcome variable psychosomatic problems. Bivariate regressions showed that all independent variables demonstrated statistically significant effects on psychosomatic problems (, model A). The likelihood ratio test showed that the model with the interaction term ‘self-efficacy by sex’ fit the data significantly better than the multivariate main effects model (, model B). This interaction implies that sex significantly modified the association between self-efficacy and psychosomatic problems.
Table 2. Multinomial logistic regression of a higher versus lower degree of psychosomatic problems, showing odds ratios (OR) and confidence intervals (CI).
Regarding schoolwork pressure (, model C), the odds of having a higher degree of psychosomatic problems compared to a lower degree of psychosomatic problems were 14.33 times higher among adolescents experiencing a higher degree of schoolwork pressure than among adolescents experiencing lower degree of schoolwork pressure, controlling for parental unemployment, family residency, school year and the interaction between self-efficacy and sex. Regarding parental unemployment (, model C), the odds of having a higher degree of psychosomatic problems compared to a lower degree of psychosomatic problems were 1.71 times higher when the adolescent reported having one or two unemployed parents compared to those who reported no parental unemployment, controlling for the other independent variables and the interaction. Regarding family residency (, model C), the odds for having a higher degree of psychosomatic problems compared to a lower degree were 6.62 times higher when the adolescents reported living alone or with someone other than their parents compared to adolescents living with both parents, controlling for the other independent variables and the interaction. The odds of having a higher degree of psychosomatic problems compared to a lower degree were 2.74 times higher when the adolescent reported living with a single parent compared to those who reported living with both parents, controlling for the other independent variables and the interaction. In addition, the odds of having a higher degree of psychosomatic problems compared to a lower degree were 1.65 times higher when the adolescent reported alternating residency compared to those who reported living with both parents, controlling for the other independent variables and the interaction.
shows the summated beta values for each subgroup subjected to analysis. The results (not shown in table) showed that girls with lower self-efficacy were 9.68 times more likely than girls with higher self-efficacy to have a higher degree of psychosomatic problems compared to having a lower degree (CI 11.10–44.01). Similarly, boys with lower self-efficacy were 3.29 times more likely than boys with higher self-efficacy to have a higher degree of psychosomatic problems compared to a lower degree (CI 1.73–6.24). In addition, girls with lower self-efficacy were 8.58 times more likely than boys with lower self-efficacy to have higher degree of psychosomatic problems (CI 4.10–18.01). Since this was the only interaction that showed statistical significance, it implies two things: (1) that sex did not moderate the relation schoolwork pressure, parental unemployment and family residency and the outcome variable psychosomatic problems; and (2) there was no interaction between self-efficacy and any of the school- and family-related explanatory variables and the outcome psychosomatic problems.
Table 3. Beta values (B) [log-odds/logits] for the variables in the interaction (model C in ).
Discussion
We investigated possible impacts of stress exposure from two contexts in adolescent’s lives. In accordance with previous research (e.g. Fröjd et al., Citation2006; Hjern et al., Citation2008; Natvig et al., Citation2003; Petersen et al., Citation2010) we identified schoolwork pressure, living with a single parent or no parent, and low self-efficacy as potential risk factors for mental health problems. These risk factors need to be addressed in school health promotion and preventive work, in accordance with the intentions in the Swedish Education Act (SFS Citation2010:Citation800). Previous research showed that family type contributed more to the distribution of ill health among children in the Nordic countries than parental unemployment did (Pedersen & Madsen, Citation2002), and the results of the present study confirm these findings. Due to the lack of data in this study, the adolescents’ relationship with their parents was not included in the analysis. This family factor could contribute to adolescents’ mental health or mental health problems according to both theory (Bronfenbrenner, Citation1977; Pearlin, Citation1989; Turner, Citation2010) and research (see e.g. Wille et al., Citation2008).
This study identified a specific risk group: girls with low self-efficacy. The results showed that the relation between self-efficacy and a higher degree of psychosomatic problems was modified by sex, i.e. the association was stronger for girls than for boys. Inversely, high self-efficacy could be considered a protective factor. Since self-efficacy is a personal resource that is possible to influence, measures to strengthen self-efficacy among girls as well as boys should be considered. Such efforts may include health promotion work at the individual, group and structural levels in which the school health team, in particular the school social workers, can play an important role.
In addition, the results from the present study suggest that the school year and sex deserve attention in the preventive work of the school health team. In accordance with previous research (Eriksson & Sellström, Citation2010; Hagquist, Citation2009, Citation2013; Murberg & Bru, Citation2004), girls reported a higher degree of both psychosomatic problems and schoolwork pressure compared to boys. Furthermore, the proportions of adolescents reporting a higher degree of both psychosomatic problems and schoolwork pressure increased with age. Previous research has also showed that school-related problems were perceived as more stressful by older compared to younger adolescents (Seiffge-Krenke, Weidemann, Fentner, Aegenheister, & Poeblau, Citation2001). The implication for practice is that health promotion and preventive work need to start before school year 9 and also that girls should be considered a risk group, both when it comes to schoolwork pressure and psychosomatic problems.
Turner (Citation2010) suggested that social characteristics like gender may affect both the experience of stress exposure and the development of personal resources. In addition, research showed that efforts to behave according to gender-specific norms concerning schoolwork was connected to mental health (Landstedt, Asplund, & Gillander Gådin, Citation2009). This might explain why girls experienced more schoolwork pressure in the current study.
Limitations
Due to the cross-sectional design of this study, we were not able to investigate social stress as a process as theorised by Pearlin (Citation1989). Nor is it possible to determine the direction of the relationships between schoolwork pressure, parental unemployment, family residency and psychosomatic problems. While we interpret our findings hypothesising a specific direction, it could be that psychosomatic problems affect schoolwork pressure or that adolescents’ psychosomatic problems affect parents’ employment options. Similarly, the degree of psychosomatic problems for an adolescent before a parental split up, leading to a change in family residency, is also unknown.
The data collection took place in 2010; according to the Public Health Agency of Sweden (Citation2014, Citation2018) both self-reported internalising mental health problems and schoolwork pressure have increased since then. This could imply that the relationships between the variables under investigation could vary if examined using data that are more recent.
Unfortunately, there is no way to identify what constituted the group of adolescents who reported living alone or with someone else, e.g. whether they were living with other relatives, in foster care, or in residential care. In addition, the CI for this OR was wide. That could be due to low a number of observations in the outcome category. The same could apply for the broad CI for higher degree of schoolwork pressure.
Conclusion
We conclude that adolescents experiencing schoolwork pressure and adolescents living with a single parent or no parent are more likely to experience a higher degree of psychosomatic problems, regardless of the adolescent’s sex, school year, self-efficacy or parental unemployment. In addition, the results showed that the association between self-efficacy and psychosomatic problems was significantly moderated by sex. Since this was the only significant interaction, it implies that sex alone did not moderate the relation between the explanatory variables schoolwork pressure, parental unemployment, family residency and the outcome variable psychosomatic problems. It also implies that there was no interaction between self-efficacy and any of the school- and family-related explanatory variables and the outcome psychosomatic problems. In order to reduce psychosomatic problems, health promoting and preventive work by the school health team should focus on strengthening pupils’ self-efficacy and target schoolwork pressure. Special attention needs to be given to girls and adolescents living with a single parent or no parents.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes on contributors
Victoria Lönnfjord
Victoria Lönnfjord is a PhD student in social work at Karlstad University and her doctoral studies are conducted at the Centre for Research on Child and Adolescent Mental Health. Previously, she worked as an investigator at FoU Välfärd Värmland, a regional research and development unit for the Swedish social services.
Curt Hagquist
Curt Hagquist is Professor of Public Health and the founding director of the Centre for Research on Child and Adolescent Mental Health. He is a trained social worker and gained his PhD in social work at the University of Gothenburg. He is the initiator of the study Young in Värmland and the principal investigator of several other studies on child and adolescent health. His research fields include epidemiology, psychometrics (Rasch measurement theory), health promotion and social determinants of health.
References
- Andrich, D. (1988). Rasch models for measurement. Newbury Park, CA: Sage.
- Avison, W. R. (2009). Family structure and women’s lives: A lifecourse perspective. In W. R. Avison, C. S. Aneshensel, S. Schieman, & B. Wheaton (Eds.), Advances in the conceptualization of the stress process (pp. 71–92). New York: Springer.
- Backe-Hansen, E., & Frønes, I. (2012). Hvordan forske på og med barn og unge? In E. Backe-Hansen, & I. Frønes (Eds.), I Metoder og perspektiver i barne-og ungdomsforskning (pp. 11–32). Oslo: Gyldendal Norsk Forlag.
- Backlund, Å, Högdin, S., & Weitz Spånberger, Y. (2017). Skolsocialt arbete – en introduktion. In Å Backlund, S. Högdin, & Y. Weitz Spånberger (Eds.), Skolsocialt arbete - Skolan som plats för och del i det sociala arbetet (pp. 15–20). Malmö: Gleerups.
- Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84(2), 191–215. doi: 10.1037/0033-295X.84.2.191
- Beckman, L. (2013). Traditional bullying and Cyberbullying among Swedish adolescents: Gender differences and associations with mental health (Doctoral thesis). Karlstad: Karlstad University.
- Beckman, L., Hagquist, C., & Hellström, L. (2012). Does the association with psychosomatic health problems differ between cyberbullying and traditional bullying? Emotional and Behavioural Difficulties, 17(3-4), 421–434. doi: 10.1080/13632752.2012.704228
- Bergman, M. M., & Scott, J. (2001). Young adolescents’ wellbeing and health-risk behaviours: Gender and socio-economic differences. Journal of Adolescence, 24(2), 183–197. doi: 10.1006/jado.2001.0378
- Bor, W., Dean, A. J., Najman, J., & Hayatbakhsh, R. (2014). Are child and adolescent mental health problems increasing in the 21st century? A systematic review. Australian & New Zealand Journal of Psychiatry, 48(7), 606–616. doi: 10.1177/0004867414533834
- Bremberg, S. (2015). Mental health problems are rising more in Swedish adolescents than in other Nordic countries and the Netherlands. Acta Paediatrica, 104(10), 997–1004. doi: 10.1111/apa.13075
- Bronfenbrenner, U. (1977). Toward an experimental ecology of human development. American Psychologist, 32(7), 513–531. doi: 10.1037/0003-066X.32.7.513
- Bronfenbrenner, U. (1994). Ecological models of human development. International Encyclopedia of Education, 3(2), 37–43.
- Carlerby, H., Viitasara, E., Knutsson, A., & Gillander Gådin, K. (2012). How discrimination and participation are associated with psychosomatic problems among boys and girls in northern Sweden. Health, 4(10), 866–872. doi: 10.4236/health.2012.410132
- Eriksson, U., & Sellström, E. (2010). School demands and subjective health complaints among Swedish schoolchildren: A multilevel study. Scandinavian Journal of Social Medicine, 38(4), 344–350.
- Fröjd, S., Marttunen, M., Pelkonen, M., Von der Pahlen, B., & Kaltiala-Heino, R. (2006). Perceived financial difficulties and maladjustment outcomes in adolescence. European Journal of Public Health, 16(5), 542–548. doi: 10.1093/eurpub/ckl012
- Gerber, M., & Pühse, U. (2008). “Don’t crack under pressure!”—Do leisure time physical activity and self-esteem moderate the relationship between school-based stress and psychosomatic complaints? Journal of Psychosomatic Research, 65(4), 363–369. doi: 10.1016/j.jpsychores.2008.06.012
- Hagquist, C. (2001). Evaluating composite health measures using Rasch modelling: An illustrative example. Sozial-und Präventivmedizin, 46(6), 369–378. doi: 10.1007/BF01321663
- Hagquist, C. (2008). Psychometric properties of the PsychoSomatic problems scale: A Rasch analysis on adolescent data. Social Indicators Research, 86(3), 511–523. doi: 10.1007/s11205-007-9186-3
- Hagquist, C. (2009). Psychosomatic health problems among adolescents in Sweden—are the time trends gender related? The European Journal of Public Health, 19(3), 331–336. doi: 10.1093/eurpub/ckp031
- Hagquist, C. (2013). Ungas psykiska hälsa i Sverige–komplexa trender och stora kunskapsluckor. Socialmedicinsk tidskrift, 90(5), 671–683.
- Hagquist, C., & Andrich, D. (2017). Recent advances in analysis of differential item functioning in health research using the Rasch model. Health and Quality of Life Outcomes, 15(1), 181. doi: 10.1186/s12955-017-0755-0
- Hellström, L., Beckman, L., & Hagquist, C. (2017). Does the strength of the association between peer victimization and psychosomatic health problems depend on whether bullying or peer aggression is measured? Child Indicators Research, 10(2), 447–459. doi:10.1007/s12187-016-9390 doi: 10.1007/s12187-016-9390-2
- Hjern, A., Alfven, G., & Östberg, V. (2008). School stressors, psychological complaints and psychosomatic pain. Acta Paediatrica, 97(1), 112–117. doi: 10.1111/j.1651-2227.2007.00585.x
- Kaltiala-Heino, R., Rimpelä, M., Rantanen, P., & Laippala, P. (2001). Adolescent depression: The role of discontinuities in life course and social support. Journal of Affective Disorders, 64(2), 155–166. doi: 10.1016/S0165-0327(00)00233-0
- Koskinen-Hagman, M., Schwarzer, R., & Jerusalem, M. (1999). Swedish version of the gereral self-efficacy scale. Retrieved from http://userpage.fu-berlin.de/~health/swedish.htm
- Landstedt, E., Asplund, K., & Gillander Gådin, K. (2009). Understanding adolescent mental health: The influence of social processes, doing gender and gendered power relations. Sociology of Health & Illness, 31(7), 962–978. doi: 10.1111/j.1467-9566.2009.01170.x
- Lönnfjord, V., & Hagquist, C. (2017). The psychometric properties of the Swedish version of the general self-efficacy scale: A Rasch analysis based on adolescent data. Current Psychology, 37(4), 703–715. doi: 10.1007/s12144-016-9551-y
- Mörk, E., Sjögren, A., & Svaleryd, H. (2014). Parental unemployment and child health. CESifo Economic Studies, 60(2), 366–401. doi: 10.1093/cesifo/ifu016
- Murberg, T. A., & Bru, E. (2004). School-related stress and psychosomatic symptoms among Norwegian adolescents. School Psychology International, 25(3), 317–332. doi: 10.1177/0143034304046904
- National Board of Health Welfare, & National Agency for Education. (2016). Vägledning för elevhälsan. Stockholm: Socialstyrelsen & Skolverket.
- Natvig, G. K., Albrektsen, G., Anderssen, N., & Qvarnstrom, U. (1999). School-related stress and psychosomatic symptoms among school adolescents. Journal of School Health, 69(9), 362–368. doi: 10.1111/j.1746-1561.1999.tb06430.x
- Natvig, G. K., Albrektsen, G., & Qvarnstrøm, U. (2003). Associations between psychosocial factors and happiness among school adolescents. International Journal of Nursing Practice, 9(3), 166–175. doi: 10.1046/j.1440-172X.2003.00419.x
- Nygren, K., & Hagquist, C. (2017). Self-reported school demands and psychosomatic problems among adolescents–changes in the association between 1988 and 2011? Scandinavian Journal of Public Health, 174–181. doi: 10.1177/1403494817725687
- OECD. (2013). Mental health and work: Sweden. Paris: OECD Publishing.
- OECD. (2016). Promoting well-being and inclusiveness in Sweden. Paris: OECD Publishing.
- Östberg, V., Alfven, G., & Hjern, A. (2006). Living conditions and psychosomatic complaints in Swedish schoolchildren. Acta Paediatrica, 95(8), 929–934. doi: 10.1080/08035250600636545
- Pearlin, L. I. (1989). The sociological study of stress. Journal of Health and Social Behavior, 30, 241–256. doi: 10.2307/2136956
- Pedersen, C. R., & Madsen, M. (2002). Parents’ labour market participation as a predictor of children’s health and wellbeing: A comparative study in five Nordic countries. Journal of Epidemiology & Community Health, 56(11), 861–867. doi: 10.1136/jech.56.11.861
- Petersen, S., Bergström, E., Cederblad, M., Ivarsson, A., Köhler, L., Rydell, A.-M., … Hägglöf, B. (2010). Barns och ungdomars psykiska hälsa i Sverige -En systematisk litteraturöversikt med tonvikt på förändringar över tid. Stockholm: Hälsoutskottet, Kungliga Vetenskapsakademien.
- Piko, B., & Fitzpatrick, K. M. (2001). Does class matter? SES and psychosocial health among Hungarian adolescents. Social Science & Medicine, 53(6), 817–830. doi: 10.1016/S0277-9536(00)00379-8
- Public Health Agency of Sweden. (2012). Slutredovisning av uppdraget Lokalt sektoröverskridande hälsofrämjande arbete för barn och ungdomar - Slutrapport för åren 2009–2011. Stockholm: Statens folkhälsoinstitut.
- Public Health Agency of Sweden. (2014). Svenska skolbarns hälsovanor 2013/14. Stockholm: Folkhälsomyndigheten.
- Public Health Agency of Sweden. (2018). Varför har den psykiska ohälsan ökat bland barn och unga i Sverige: Utvecklingen under perioden 1985–2014. Stockholm: Folkhälsomyndigheten.
- Rasch, G. (1960/1980). Probabilistic models for some intelligence and attainment tests. Chicago: The University of Chichago Press.
- Schwarzer, R., & Jerusalem, M. (1995). Generalized self-efficacy scale. In J. Weinman, S. Wright, & M. Johnston (Eds.), Measures in health psychology: A user’s portfolio. Causal and control beliefs (Vol. 1, pp. 35–37). Windsor: NFER-Nelson.
- Seiffge-Krenke, I., Weidemann, S., Fentner, S., Aegenheister, N., & Poeblau, M. (2001). Coping with school-related stress and family stress in healthy and clinically referred adolescents. European Psychologist, 6(2), 123–132. doi: 10.1027//1016-9040.6.2.123
- SFS 2010:800. Skollagen. Stockholm: Utbildningsdepartementet.
- Sleskova, M., Salonna, F., Geckova, A. M., Nagyova, I., Stewart, R. E., van Dijk, J. P., & Groothoff, J. W. (2006). Does parental unemployment affect adolescents’ health? Journal of Adolescent Health, 38(5), 527–535. doi: 10.1016/j.jadohealth.2005.03.021
- Sund, A. M., Larsson, B., & Wichstrøm, L. (2003). Psychosocial correlates of depressive symptoms among 12–14-year-old Norwegian adolescents. Journal of Child Psychology and Psychiatry, 44(4), 588–597. doi: 10.1111/1469-7610.00147
- Swedish National Agency for Education. (2016). Läroplan för grundskolan, förskoleklassen och fritidshemmen 2011 (Ny rev. utg.). Stockholm: Skolverket.
- Torsheim, T., Aaroe, L. E., & Wold, B. (2003). School-related stress, social support, and distress: Prospective analysis of reciprocal and multilevel relationships. Scandinavian Journal of Psychology, 44(2), 153–159. doi: 10.1111/1467-9450.00333
- Turner, R. J. (2010). Understanding health disparities: The promise of the stress process model. In W. R. Avison, C. S. Aneshensel, S. Schieman, & B. Wheaton (Eds.), Advances in the conceptualization of the stress process (pp. 3–21). New York: Springer.
- Vinnerljung, B., Hjern, A., & Berlin, A. M. (2010). Skolbetyg, utbildning och risker för ogynnsam utveckling hos barn In Social rapport 2010. Stockholm: Socialstyrelsen.
- Wille, N., Bettge, S., & Ravens-Sieberer, U. (2008). Risk and protective factors for children’s and adolescents’ mental health: Results of the BELLA study. European Child & Adolescent Psychiatry, 17(1), 133–147. doi: 10.1007/s00787-008-1015-y