
Abstract
Objectives: Aging populations are contributing to an increased volume of osteoporotic fractures. The goals of this study were to (1) develop a scorecard on epidemiological burden, policy framework, service provision, and service uptake for osteoporosis in Saudi Arabia and (2) estimate the direct costs of managing osteoporotic fractures in Saudi Arabia.
Methods: Osteoporosis data specific to Saudi Arabia were collected through a systematic literature review and surveys with osteoporosis experts. The data were used to build a scorecard, as done previously for the European Union and select Latin American countries. The scorecard applied traffic light colour coding to identify areas of risk in Saudi Arabia’s management of osteoporosis. The data were also used to parameterize a burden of illness model. The model estimated the direct medical costs of fractures among adults aged 50–89 years in Saudi Arabia. The model included hospitalization, testing, hip fracture surgery, and drug costs.
Results: In Saudi Arabia, the Ministry of Health was aware of impending increases in the number of fractures and had prioritized osteoporosis on the national agenda. Accordingly, reimbursement restrictions for osteoporosis diagnosis and treatment were minimal. However, a national fracture registry and unified system for monitoring care were not in operation. This represents a critical gap in care that will continue to contribute to the underdiagnosis and undertreatment of osteoporosis if not addressed. In total, 174,225 osteoporosis-related fractures were estimated to occur in Saudi Arabia in 2019, with an annual cost of SR2.38 billion ($636 million USD; $1.55 billion PPP). Hospitalization was the primary cost driver.
Conclusions: In 2019, Saudi Arabia was expected to incur SR2.38 billion ($636 million USD; $1.55 billion PPP) in costs owing to 174,225 osteoporosis-related fractures. The establishment of a national fracture registry and implementation of fracture liaison services will be paramount to reducing the fracture burden.
Introduction
Osteoporosis is a chronic skeletal condition that negatively impacts both sexes but is more common in females. Osteoporosis most frequently affects postmenopausal women and elderly menCitation1. The risk of osteoporosis is also modified in patients with diabetes and obesity, both of which are highly prevalent in Saudi ArabiaCitation2–4. The hallmark feature of osteoporosis is the progressive loss of bone densityCitation1. This leads to increased bone fragility, thereby increasing the risk of fractureCitationi. The sites most prone to osteoporotic fracture are the hip, spine, and wristCitation1. When an initial fracture occurs, the risk of subsequent fracture is compoundedCitation5. Osteoporotic fractures are serious health events that associate with heightened morbidity, mortality, and economic costs. In Saudi Arabia, only one in two patients presenting with an index hip fracture will return to their pre-fracture mobility statusCitation6. Patients with assisted walking needs or a wheelchair at the time of fracture may become bedridden, and survival is also reducedCitation6. The 1-year mortality rate associated with hip fractures in Saudi Arabia is 27%Citation6, which is markedly higher than the regional average of 18% reported in the literatureCitation7. On account of population growth and increased longevity, the lifetime cost of hip fractures in Saudi Arabia is expected to reach SR35 billion ($9.34 billion USD) by 2025Citation8. In spite of this significant burden, osteoporosis remains underdiagnosed and undertreated. Most fracture patients are not aware of their underlying osteoporosis prior to fracture and are, therefore, treatment-naïveCitation8.
Worldwide there is a wealth of information on osteoporosis. However, studies on osteoporosis that are specific to Saudi Arabia are limited. For example, there is a peer-reviewed scorecard to compare osteoporosis management across the 27 countries of the European Union (EU)Citation9. An analogous tool does not exist for Saudi Arabia. A small number of studies have estimated fracture burden in Saudi Arabia, but these studies were restricted to hip fracturesCitation8,Citation10. Given the aforementioned research gaps, we set out to collect information on osteoporosis via a systematic review of the literature and discussions/surveys with osteoporosis experts. We used this information to create a scorecard of osteoporosis care in Saudi Arabia and to quantify the direct medical costs of osteoporotic fractures in Saudi Arabia.
Methods
Data collection
We conducted a systematic literature review to collect data for our scorecard and economic model. We developed our systematic review protocol using the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) guidelinesCitation11.
A senior medical information specialist performed the database search of the published literature on 2 January 2018. The search strategy was executed in Ovid MEDLINE1, Embase, and the Cochrane Library (Supplementary Appendix S1). A previous version of the search strategy was peer reviewed by a second senior medical information specialist using the PRESS Checklist and has since informed multiple publicationsCitation12–14. We also performed targeted grey literature searches using the Canadian Agency for Drugs and Technologies in Health (CADTH) Grey Matters Tool, which was modified to align with our eligibility criteriaCitation15.
We included articles of any study design with information on the prevalence, incidence, health resource utilization (direct and indirect costs), treatment, and management of osteoporosis and osteoporosis-related fractures in adults ≥18 years of age in Saudi Arabia. We considered published journal articles in English and grey literature in English or Arabic. We excluded articles published prior to 2010, unless recommended for inclusion by the osteoporosis experts.
One reviewer independently screened the titles/abstracts followed by the full-text articles identified in the search (Supplementary Appendix S2). The reviewer then cross-referenced the reference lists of existing systematic reviews and meta-analyses with our search results to look for additional studies. Finally, the reviewer extracted relevant information from all the included articles using a standardized template.
To supplement gaps in the literature, we surveyed two osteoporosis experts from Saudi Arabia using an adaptation of an International Osteoporosis Foundation (IOF) questionnaireCitation16. We also held discussions with the experts to resolve discrepancies in their questionnaire responses.
Scorecard
We compiled pertinent data from our systematic review and expert surveys into a scorecard. We sought to replicate the Scorecard for Osteoporosis in Europe (SCOPE) project, which assessed the epidemiology and management of osteoporosis across four domains: (1) burden of disease, (2) policy framework, (3) service provision, and (4) service uptakeCitation9. We used the scoring thresholds from the SCOPE project wherever possible. We note changes to the SCOPE methodology herein. We assigned each score a corresponding colour: red indicating high risk, yellow indicating moderate risk, green indicating low risk, or black indicating no data.
Burden of disease
We altered the SCOPE (European Scorecard)Citation9 scoring thresholds for age standardized incidence of hip fracture in women to align with the thresholds established by a broader Kanis et al.Citation17 systematic review of hip fracture incidence worldwide. However, we did not use the initial score for Saudi Arabia as presented in the Kanis et al.Citation17 review because it was based on a study from 1995Citation18. Instead, we identified a more recent study (Sadat-Ali et al.Citation8) of hip fracture incidence in Saudi Arabia from our own systematic review. We then age-standardized the hip fracture incidence for females (as reported in Sadat-Ali et al.Citation8) to the 2010 world populationCitation19 to replicate the Kanis et al.Citation17 methods and ensure comparability.
We used our burden of illness (BOI) model to calculate the total number of fragility fractures in men and women per 1,000 of the population aged 50–89 years for 2015 and to determine the per cent increase in the annual number of fractures from 2015 to 2030. We selected 2015 as the starting point because at the time this study was conducted, it was the most recent estimate availableCitation19. We projected fractures over a 15-year window to match the timeframe selected for the SCOPE projectCitation9. We describe the model calculations in detail below.
The SCOPE project assessed lifetime hip fracture probability at the age of 50 years among womenCitation9. We adapted this element to align with the Kanis et al.Citation17 systematic review which looked at the 10-year probability of a major osteoporotic fracture worldwide. We made this adaptation because we anticipated the clinical scenario would be easily replicable where fracture risk assessment (FRAX) models were available. The clinical scenario was a woman aged 65 years with a prior fragility fracture and no other clinical risk factors at the threshold of osteoporosis as judged by bone mineral density at the femoral neck (i.e. a T-score of −2.5 SD) and with a body mass index of 24 kg/mCitation2,Citation17.
Unlike the SCOPE project, we did not have access to distributions of FRAX probabilitiesCitation9. Therefore, we were not able to calculate the proportion of the population aged 50–89 years with a 10-year probability of major fracture that is 10% or more. Instead, we scored the prevalence of osteoporosis in the female population aged ≥50 years which was presented as an unscored element in the SCOPE projectCitation9. We categorized the prevalence values from the SCOPE project into tertiles to generate scoring thresholdsCitation9.
Policy framework
We determined the availability and quality of literature sources for hip fracture incidence from our systematic review. We consulted with osteoporosis experts to confirm the presence of national fracture registries, to determine whether osteoporosis is a national health priority (NHP) in Saudi Arabia, to understand whether osteoporosis is typically managed in primary care or by another medical specialty, and to find out if osteoporosis is a recognized medical specialty in and of itself or a component of specialty training. We referred to the IOF’s website for the listing of national osteoporosis societies operating in Saudi ArabiaCitation20.
Service provision
We queried the osteoporosis experts to understand the reimbursement environment for osteoporosis treatments and Dual-energy X-ray Absorptiometry (DXA) scans in Saudi Arabia. We obtained the number of DXA machines available per million persons from the IOF Middle East & Africa Regional AuditCitation21. In the SCOPE project, this information came from the combined sales information of major DXA providersCitation9. We referred to the FRAX website to determine if Saudi Arabia had a country-specific FRAX toolCitation22. We collected additional information on the availability and use of risk assessment tools from our discussions with osteoporosis experts. We identified osteoporosis guidelines in our systematic review and evaluated the guidelines using the Appraisal of Guidelines for Research & Evaluation (AGREE) criteriaCitation23. We confirmed the appraisal and selection of guidelines with the osteoporosis experts to ensure accuracy. We reported the number of fracture liaison service (FLS) centres in Saudi Arabia as per the IOF Capture the Fracture Map of Best PracticeCitation24. We also asked the osteoporosis experts if data on the quality of care provided to osteoporosis patients is systematically collected at a national level in Saudi Arabia.
Service uptake
We used a Kanis et al. publication to assess the uptake of FRAX algorithmsCitation25. We characterized the pharmacological treatment gap among hip fracture patients using a publication by Sadat-Ali et al.Citation26 This publication was provided by one of the osteoporosis experts because we anticipated difficulties in replicating the SCOPE methodology which used FRAX model simulationsCitation9,Citation26. We surveyed the osteoporosis experts on average wait times for surgery following hip fracture.
Economic model
We parameterized an existing, peer-reviewed model with inputs specific to Saudi ArabiaCitation13. The model estimates economic burden at the cohort-level and has inputs related to fractures (incidence, population demography) and costs (hospitalization, testing, hip fracture surgery, and drugs). The osteoporosis experts assisted in verifying the proposed inputs, ensuring face validity of our economic model.
We designed the model to calculate the total economic burden over one year, the annual burden per 1,000 persons at risk aged 50–89 years, and the total economic burden over five cumulative years. To present the burden of osteoporosis as a proportion of gross domestic product (GDP), we divided the annual burden in 2019 from the model by the International Monetary Fund’s 2019 nominal GDP estimate for Saudi ArabiaCitation27.
As recommended by the Evidence for Policy and Practice Information and Coordinating Centre costing tool, we inflated costs before converting using year over year inflation data from the Organization for Economic Co-operation and Development (OECD); we used a fixed rate to convert between currencies ($1.00 United States dollar [USD] equals 3.75 Saudi Riyal [SR])Citation28–30. We also reported the costs in terms of purchasing power parity (PPP) by converting the results of the model into international dollars. We used the 2019 PPP exchange rate from the International Monetary Fund (1.539 SR = $1.00 PPP) to perform this conversionCitation31. Similar to a budget impact analysis, our burden of illness model estimates costs over the short-term. Therefore, we did not apply discountingCitation32.
In our systematic review, we identified hip fracture incidence rates that were specific to Saudi ArabiaCitation8. However, we did not find fracture incidence rates at skeletal sites other than the hip that were specific to Saudi Arabia. Consequently, we assumed that the ratio of hip fracture incidence to fracture incidence at additional skeletal sites was similar in Saudi Arabia and Sweden (where more granular data were available). We then used the Swedish fracture ratios to impute fracture incidence at the spine, forearm, and other skeletal sites, including the ribs, pelvis, humeral shaft, proximal humerus, clavicle, sternum, other femoral, tibia, and fibulaCitation33. The Swedish fracture ratios are often used as a proxy when populating models with partial data and have even been used in the development of country-specific FRAX modelsCitation34,Citation35. To calculate the total number of fractures, we multiplied the fracture incidence rates by the corresponding age- and sex-specific population estimates for Saudi Arabian adults aged 50–89 years. We used the medium variant reported by the United Nations to inform our population projectionsCitation19. The medium variant was derived from census data and included both Saudi Arabia nationals and foreign residents in the total estimateCitation19. We varied population demography year over year in accordance with the United Nations’ projections but kept the incidence rates fixed. As a result, changes in the number of fractures predicted by the model are explained by underlying shifts in age- and sex- distributions.
We assumed all fracture patients were hospitalized because our incidence rates were derived from hospital admissions data. We also assumed all patients incurred testing costs which included the cost of blood and urine investigations as well as radiographsCitation10. Due to data limitations, we only considered surgery costs for hip fractures, which included the cost of the operating rooms, surgeon fees, and implantsCitation10. We assumed all hip fracture patients incurred surgery costs. We used a published study to inform the proportion of all fracture patients in the model receiving prescription drugs as 74%Citation26. This study included patients receiving a regimen of (1) an anabolic agent, calcium and vitamin D3, or (2) a bisphosphonate, calcium, and vitamin D3Citation26.
We obtained the hospital length of stay for hip and spine fractures from the published literatureCitation8,Citation36. We relied on estimates from the osteoporosis experts to inform the length of stay for forearm fractures and fractures at other sites. We applied the World Health Organization’s primary hospital bed cost for Saudi Arabia as our per diem cost to capture the daily expenditures related to personnel, capital, and food throughout the hospital stayCitation37. We extracted unit costs for testing, hip fracture surgery, and prescription drugs from a previous BOI investigationCitation10. We present the values of each of these inputs in Supplementary Appendix S3.
We did not account for patient productivity losses because the economic participation rate for our population of interest was thought to be low. According to Saudi Arabia’s General Authority for Statistics 2018, only 0.4% of females aged ≥65 years participated in the labour forceCitation38. We also did not account for informal caregiver costs, rehabilitation, and long-term care costs because of insufficient data. In accordance with previously established methodology, we did not account for mortality in the model and, thus, we did not capture costs related to premature deathsCitation39.
We conducted bidirectional, one-way sensitivity analyses to address uncertainty in our estimates. We varied several inputs, including hospital length of stay, fracture incidence ratios, the proportion of fracture patients hospitalized, prescription drug cost, and hip fracture surgery cost. Where possible, we tested values that were higher and lower than the base-case value. We informed the range of tested values using the literature and in the absence of data from the literature, we relied on expert opinion. Results are reported in tabular format combined with a tornado diagram.
Results
Systematic review
The database search strategy identified 2,630 unique records for title and abstract screening of which 149 were included in the full-text review. An additional 13 records were identified by hand-searching, grey literature searches, or provided by the osteoporosis experts for full-text review. After completing the two-level screening, 31 records met the eligibility criteria and were included for data extraction. A PRISMA flow diagram of study selection is presented in Supplementary Appendix S2.
Scorecard
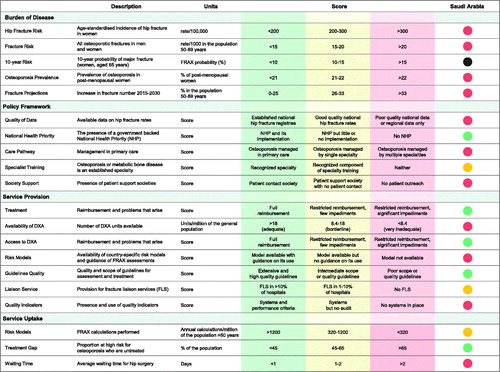
The scorecard for Saudi Arabia is presented in .
Figure 1. Scorecard for osteoporosis in Saudi Arabia. Abbreviations. DXA, dual-energy x-ray absorptiometry; FLS, fracture liaison service; FRAX, fracture risk assessment model; NHP, national health priority.
Burden of disease
The age-standardized incidence of hip fracture in women, crude rate of fragility fractures in men and women aged 50–89 years, osteoporosis prevalence in post-menopausal women, and the projected growth in fractures from 2015 to 2030 were all categorized as high risk (). There was no information available for the 10-year probability of major osteoporotic fracture.
Table 1. Epidemiological measures of osteoporosis burden in Saudi Arabia.
Policy framework
At the time when this study was conducted, there were no national hip fracture registries in Saudi Arabia and the available estimates of hip fracture incidence were based on regional samplesCitation8. The lack of national fracture data represented an area of high risk. However in 2018, a National Plan for Osteoporosis Prevention and Management in the Kingdom of Saudi Arabia was published by the Ministry of Health in consultation with the Saudi Osteoporosis Society and an expert panel in Saudi ArabiaCitation41. This action plan laid out several recommendations and key areas of focus to improve osteoporosis prevention and management. As such, osteoporosis was considered an NHP in Saudi Arabia (low risk). Despite increased government attention, there were several shortcomings identified in the care pathway for osteoporosis patients. First, primary care physicians did not oversee the principal care of patients with osteoporosis (high risk), and osteoporosis was not considered a medical specialty (moderate risk). Instead, orthopaedic surgeons, endocrinologists, and rheumatologist were the lead specialists and received osteoporosis training as a component of their residencies. Society support was also an area of high risk because the role of national patient societies is to improve care and increase awareness of osteoporosis among the general public. In Saudi Arabia, there were only two scientific societies geared specifically towards physicians: (1) Saudi Osteoporosis Society and (2) Pan Arab Osteoporosis Society. There were no societies engaged in patient outreach.
Service provision
Treatment access was an area of low risk in Saudi Arabia. Common osteoporosis treatments, like oral bisphosphonates, vitamin D, and calcium supplements, were reimbursed in full by the National Health System. More costly treatments, such as denosumab and teriparatide, were also available with justification and were fully covered. From a diagnosis perspective, the number of DXA machines in Saudi Arabia was determined to be inadequate (high risk). As of the 2011 Middle East and Africa IOF Audit, there were five DXA machines per million of the general population in Saudi ArabiaCitation21. Although the availability of DXA machines was an issue, access to reimbursement coverage was not. Annual DXA exams were found to be reimbursed without restriction (low risk). There was no country-specific FRAX model for Saudi Arabia (high risk). High quality treatment guidelines were available with recommendations for post-menopausal women, men, and patients with glucocorticoid-induced osteoporosis (low risk)Citation42. As of June 2019, there was only one FLS in Saudi Arabia listed on the IOF Capture the Fracture Map of Best Practice (moderate risk). This FLS was located at the King Fahd Hospital of the University, AlKhobar and its rating was in progressCitation24. As a corollary to the lack of FLS sites, there were no national systems in place to systematically collect data on the quality of care provided to patients (high risk).
Service uptake
Even though Saudi Arabia does not have a country-specific FRAX model, it still showed relatively frequent uptake of the FRAX algorithm. A Google Analytics study that tracked the source of the originating country was able to determine that on an annual basis, approximately 504 FRAX calculations were performed per million of the population ≥50 years of age in Saudi Arabia (moderate risk)Citation25. Treatment uptake was scored as low risk based on a recent study that found three out of four patients with a prior hip fracture received optimal pharmacologic treatment at one yearCitation26. This level of treatment uptake (75%) was considerably higher than what has been reported for other countriesCitation9,Citation14. However, given the estimate was derived from a single centre, retrospective study with a small number of hip fracture cases, the result should be interpreted with caution. The wait time for surgery following hip fracture was scored as high risk because it averaged more than two days.
BOI model
In 2019, the model estimated a total of 174,225 osteoporotic fractures would occur in Saudi Arabia, 17,467 of which would be hip fractures (). As shown in , the corresponding one-year economic burden of illness for all fractures was SR2.38 billion ($636 million USD; $1.55 billion PPP). This value constituted roughly 0.08% of Saudi Arabia’s nominal GDP in 2019. For every 1,000 men and women aged 50–89 years at risk of osteoporosis in Saudi Arabia, the annual cost was SR453,325 ($120,887 USD; $2,94,558 PPP). From 2019 to 2023, the number of fractures was projected to grow by 27.7%. The 5-year cumulative burden during this period attributable to 988,029 total fractures was SR13.5 billion ($3.60 billion USD; $8.77 billion PPP). The largest expenditure was the hospitalization costs (42%), followed by testing costs (24%), and drug costs (21%). Surgical costs comprised the remaining 14% of the burden.
Table 2. Estimated number of fractures among adults aged 50–89 years in Saudi Arabia.
Table 3. Estimated economic burden of osteoporosis in Saudi Arabia for 2019.
Sensitivity analyses
In the sensitivity analyses, change in hospital length of stay had the greatest impact on the 1-year estimate of economic burden (±24% of base case value), followed closely by changes in the fracture ratios (±21%), and the proportion of patients hospitalized (−21%) (). The impact of varying the prescription drug cost and hip fracture surgery cost was less pronounced, with model estimates changing by ±14% and ±7%, respectively.
Figure 2. One-way sensitivity analyses for the estimated economic burden of osteoporosis in Saudi Arabia (2019). Abbreviation. SR, Saudi Riyal. 3.75 Saudi Riyal = 1 United States dollar. The tornado diagram displays the difference in one-year burden when comparing the results of the sensitivity analyses to the results of the base case analysis. a ± 13.08 days of base case value. Based on standard deviation in Sadat-Ali et al.Citation8 The hospital lengths of stay for vertebral, wrist, and other fractures were varied in proportion to the change in hip fracture. b ± 33% (proportion of base case value). Range informed by Siggeirsdottir et al.Citation43 cAssumption informed by expert opinion. d ± 67% (proportion of base case value). Range informed by expert opinion. e ± 50% (proportion of base case value). Upper bound informed by Sadat-Ali et al.Citation8 Note, additional details of cost breakdown were supplied by the authors.

Discussion
The study showed there are areas for improvement in osteoporosis care (through the scorecard analysis) and that osteoporosis will likely become more common as Saudi Arabia’s population ages, leading to increased osteoporotic fractures and associated expenditures. A total of 174,225 osteoporotic fractures are expected to occur in Saudi Arabia during 2019. The annual direct medical costs attributable to these fractures are estimated to be SR2.38 billion ($636 million USD; $1.55 billion PPP). By 2023, the number of fractures in Saudi Arabia is projected to grow to 222,454. The cumulative economic burden from 2019 to 2023 is estimated as SR13.5 billion ($3.60 billion USD; $8.77 billion PPP). The model was most sensitive to changes in hospital length of stay, the ratios used to impute fracture incidence, and the proportion of patients hospitalized.
Although osteoporosis is an NHP in Saudi Arabia, current policy frameworks and service provision do not fully reflect the human and financial burden of the disease. There is a paucity of high-quality data in Saudi Arabia to evaluate fracture patterns. Care pathways for the disease are also underdeveloped. Specialists, rather than general physicians, are responsible for the bulk of patient care and there are no societies in Saudi Arabia that focus on patient outreach. Furthermore, there is no country-specific FRAX model and the number of DXA machines is inadequate. At the time of the 2011 Middle East and Africa IOF Audit, the number of DXA machines per million persons in Saudi Arabia (5 DXA/million) was substantially lower than other countries in the region, including the United Arab Emirates (12 DXA/million), Turkey (13 DXA/million), and Lebanon (27 DXA/million)Citation21. Finally, auditing systems to monitor quality of care are lacking, and the mean wait time for hip surgery following fracture does not meet best practice standards.
Saudi Arabia is performing well in a few key areas of osteoporosis care. Notably, the country has well-established clinical practice guidelines. The reimbursement policies are also favourable and allow patients who are aware of their osteoporosis to access treatment. However, the high burden of disease observed in Saudi Arabia (4/5 elements red) makes it imperative that Saudi Arabia perform well across all areas of disease management. When comparing the scorecard for Saudi Arabia with the scorecard for Europe, it is evident that several European countries have a similarly high burden of disease, including Austria (5/5 elements red), Denmark (4/5 elements red), and Sweden (4/5 elements red)Citation9. Sweden, in particular, may serve as a benchmark for Saudi Arabia. Sweden scored as low or moderate risk on all but one element of policy framework, service provision, and service uptakeCitation9. Thus, Sweden may have existing models of care for Saudi Arabia to learn from as the country works to improve its service offerings.
The burden estimates found in this study align closely with a previous Saudi Arabia investigation from 2007Citation10. This is to be expected given that several unit costs in our model were derived from this investigation (Supplementary Appendix S3)Citation10. The 2007 investigation estimated a cost of SR48,712 ($12,990 USD) per hip fractureCitation10. In our model, when only hip fractures were considered, the per fracture cost was SR48,254 ($12,868 USD). However, both the 2007 estimate and our estimate are conservative relative to a 2015 investigation wherein the cost per hip fracture patient was roughly SR75,000 ($20,000 USD)Citation8,Citation10. This discrepancy is likely attributable to physical therapy costs which were included in the 2015 investigation, but not in our BOI modelCitation8. Of note, the 2015 investigation also estimated the indirect costs of hip fracture to be SR1.69 billion ($452 million USD), or three times the direct cost of SR565 million ($151 million USD)Citation8.
Our study is strengthened by the combination of tools we developed to communicate our findings, namely, the scorecard and BOI model. Both these tools were informed by a rigorous evidence base (systematic review, expert surveys, and grey literature search). Together they provide complementary data and speak to the current state of osteoporosis care in Saudi Arabia. They also serve as actionable tools that healthcare policy makers and providers can point to as incentives for improving care. The inclusion of all osteoporotic fractures in our BOI model, as opposed to just hip fractures, is another strength of our study. Furthermore, we report the results of the BOI model in international dollars to account for PPP, which more accurately reflects domestic spending on non-tradable goods and facilitates cross-country comparisonsCitation44.
There are limitations associated with our analysis. Recent epidemiologic and costing information on osteoporosis in Saudi Arabia is scarce. As a result, there is considerable uncertainty in the fracture extrapolations. We assumed regional hip fracture rates were representative of the national population and Swedish fracture ratios were a valid surrogate to calculate the incidence of fractures at other sitesCitation8,Citation33. Primary fracture data at the population level are required to test these assumptions. Furthermore, informal caregiver costs and long-term rehabilitation costs were not included given the paucity of data. The burden estimates are likely understated because of these omissionsCitation8. Quantification of these additional cost categories should be a priority of future research.
Conclusion
The results of this study confirm the significant and growing economic impact of osteoporotic fractures. Barring intervention, an estimated 988,029 fragility fractures will occur in Saudi Arabia between 2019 and 2023 with an associated burden of SR13.5 billion ($3.60 billion USD; $8.77 billion PPP). This estimate does not reflect informal caregiver costs or long-term rehabilitation costs which likely carry a substantial societal burden. Based on the scorecard, the development of a national fracture registry is warranted, as are efforts to establish greater osteoporosis awareness among the general population and increase primary fracture prevention.
Transparency
Declaration of funding
This study was funded by Amgen Inc.
Declaration of financial/other relationships
MS and AE received consulting fees from Amgen. EVERSANA received financial support from Amgen for the conduct of this study. RA, JGP, and NS are employees of Amgen. RKM and CD are employees of EVERSANA. CC is an employee and shareholder of EVERSANA. EVERSANA consults for various pharmaceutical, medical device, and biotech companies.
The peer reviewers on this manuscript have received an honorarium from JME for their review work. In addition, a reviewer on this manuscript has disclosed that they have collaborated extensively with Saudi Arabian government agencies and universities since 2012 (and the Middle East more broadly). They have several Middle Eastern researchers in their group. They have also conducted studies on osteoporosis and bone disease in Europe, in addition to their work in the US. The reviewers have no other relevant financial relationships or otherwise to disclose.
Author contributions
RA, JGP, NS, RKM, and CC were involved in the conception and design of the study. RKM, CD, and CC were involved in the analysis of data and all authors contributed to the interpretation of data. All authors participated in drafting of the paper and critical revisions for intellectual content. All authors approved the final version. All authors agree to be accountable for all aspects of the work.
Supplemental Material
Download PDF (233.2 KB)Acknowledgements
The authors thank the information specialists who conducted their searches for the systematic review. The authors also thank Ana Lüdke for helping to coordinate the early stages of their study and Kirk Szafranski and Tim Disher for their work in building the economic model.
Notes
Notes
i U.S. National Library of Medicine, Bethesda, US.
References
- Akkawi I, Zmerly H. Osteoporosis: current concepts. Joints. 2018;6:122–127.
- Jackuliak P, Payer J. Osteoporosis, fractures, and diabetes. Int J Endocrinol. 2014;2014:1–10.
- Alotaibi A, Perry L, Gholizadeh L, et al. Incidence and prevalence rates of diabetes mellitus in Saudi Arabia: an overview. J Epidemiol Glob Health. 2017;7:211–218.
- Alqarni S. A review of prevalence of obesity in Saudi Arabia. J Obes Eat Disord. 2016;2:25.
- Johansson H, Siggeirsdóttir K, Harvey NC, et al. Imminent risk of fracture after fracture. Osteoporos Int. 2017;28:775–780.
- Sadat-Ali M, Alfaraidy M, AlHawas A, et al. Morbidity and mortality after fragility hip fracture in a Saudi Arabian population: report from a single center. J Int Med Res. 2017;45:1175–1180.
- Downey C, Kelly M, Quinlan JF. Changing trends in the mortality rate at 1-year post hip fracture – a systematic review. World J Orthop. 2019;10:166–175.
- Sadat-Ali M, Al-Dakheel DA, Azam MQ, et al. Reassessment of osteoporosis-related femoral fractures and economic burden in Saudi Arabia. Arch Osteoporos. 2015;10:37.
- Kanis JA, Borgström F, Compston J, et al. SCOPE: a scorecard for osteoporosis in Europe. Arch Osteoporos. 2013;8:144.
- Bubshait D, Sadat-Ali M. Economic implications of osteoporosis-related femoral fractures in Saudi Arabian society. Calcif Tissue Int. 2007;81:455–458.
- Moher D, Liberati A, Tetzlaff J; for the PRISMA Group, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535–b2535.
- McGowan J, Sampson M, Salzwedel DM, et al. PRESS peer review of electronic search strategies: 2015 Guideline Statement. J Clin Epidemiol. 2016;75:40–46.
- Aziziyeh R, Amin M, Habib M, et al. The burden of osteoporosis in four Latin American countries: Brazil, Mexico, Colombia, and Argentina. J Med Econ. 2019;22:638–644.
- Aziziyeh R, Amin M, Habib M, et al. A scorecard for osteoporosis in four Latin American countries: Brazil, Mexico, Colombia, and Argentina. Arch Osteoporos. 2019;14:69.
- Grey Matters: a practical tool for searching health-related grey literature [Internet]. Canadian Agency for Drugs and Technologies in Health (CADTH); [updated 2015; cited 2019 Mar 13]. Available from: https://www.cadth.ca/resources/finding-evidence/grey-matters
- SCORECARD Questionnaire [Internet]. International Osteoporosis Foundation; 2012 [cited 2018 Aug 24]. Available from: https://www.iofbonehealth.org/sites/default/files/PDFs/SCOPE/SCOPE_questionnaire_template.pdf
- Kanis JA, Odén A, McCloskey EV, et al.; on behalf of the IOF Working Group on Epidemiology and Quality of Life. A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos Int. 2012;23:2239–2256.
- Al-Nuaim AR, Kremli M, Al-Nuaim M, et al. Incidence of proximal femur fracture in an urbanized community in Saudi Arabia. Calcif Tissue Int. 1995;56:536–538.
- World Population Prospects: The 2017 Revision [Internet]. United Nations (UN) Population Division of the Department of Economic and Social Affairs; [updated 2017 Jun; cited 2019 Mar 13]. Available from: https://esa.un.org/unpd/wpp/
- National Societies [Internet]. International Osteoporosis Foundation; [updated 2017; cited 2019 Mar 13]. Available from: https://www.iofbonehealth.org/societies-country-index-view/all
- El-Hajj Fuleihan G, Adib G, Nauroy L. The Middle East & Africa regional audit: epidemiology, costs & burden of osteoporosis in 2011. Nyon: International Osteoporosis Foundation; 2011.
- FRAX: Fracture Risk Assessment Tool [Internet]. Centre for Metabolic Bone Diseases University of Sheffield; [updated 2018; cited 2018 Mar 13]. Available from: https://www.sheffield.ac.uk/FRAX/
- Brouwers M, Browman G, Burgers J, et al. Appraisal of guidelines for research & evaluation II. Update: September 2013. Hamilton (ON): The AGREE Next Steps Consortium; 2009.
- Capture the Fracture: Map of Best Practice [Internet]. International Osteoporosis Foundation; [updated 2019; cited 2019 Jul 30]. Available from: https://www.capturethefracture.org/map-of-best-practice
- Kanis JA, Johansson H, Oden A, et al.; Epidemiology and Quality of Life Working Group of IOF. Worldwide uptake of FRAX. Arch Osteoporos. 2014;9:166.
- Sadat-Ali M, AlShammari SM, Uddin FZ, et al. Are we closing the gaps in the management of osteoporosis following fragility fractures of the femur? J Int Med Res. 2019;47:1843–1847.
- GDP, current prices [Internet]. International Monetary Fund; 2020 [cited 2020 Feb 20] Available from: https://www.imf.org/external/datamapper/datasets/WEO/1
- Inflation (CPI) [Internet]. Organisation for Economic Co-operation and Development (OECD); 2018 [cited 2018 Mar 29]. Available from: https://data.oecd.org/price/inflation-cpi.htm
- Currency exchange rates [Internet]. Organisation for Economic Co-operation and Development (OECD); 2019 [cited 2019 May 10]. Available from: https://stats.oecd.org/
- CCEMG – EPPI-Centre Cost Converter [Internet]. The Campbell and Cochrane Economics Methods Group (CCEMG) and the Evidence for Policy and Practice Information and Coordinating Centre (EPPI-Centre); [updated 2016; cited 2018 Mar 15]. Available from: http://eppi.ioe.ac.uk/costconversion/default.aspx
- Implied PPP conversion rate [Internet]. International Monetary Fund; 2020 [cited 2020 Feb 20] Available from: https://www.imf.org/external/datamapper/PPPEX@WEO/OEMDC/ADVEC/WEOWORLD/SAU
- Sullivan SD, Mauskopf JA, Augustovski F, et al. Budget impact analysis-principles of good practice: report of the ISPOR 2012 Budget Impact Analysis Good Practice II Task Force. Value Health. 2014;17:5–14.
- Kanis JA, Oden A, Johnell O, et al. The burden of osteoporotic fractures: a method for setting intervention thresholds. Osteoporos Int. 2001;12:417–427.
- Zerbini CA, Szejnfeld VL, Abergaria BH, et al. Incidence of hip fracture in Brazil and the development of a FRAX model. Arch Osteoporos. 2015;10:224.
- Jaller-Raad JJ, Jaller-Char JJ, Lechuga-Ortiz JA, et al. Incidence of hip fracture in Barranquilla, Colombia, and the development of a Colombian FRAX model. Calcif Tissue Int. 2013;93:15–22.
- Joestl J, Lang N, Bukaty A, et al. Osteoporosis associated vertebral fractures – Health economic implications. PLoS One. 2017;12:e0178209.
- Country-specific unit costs [Internet]. World Health Organization; 2008 [cited 2018 Mar 29]. Available from: http://www.who.int/choice/country/country_specific/en/
- Labour Market: Fourth Quarter 2018 [Internet]. General Authority for Statistics; 2018 [cited 2019 Apr 15]. Available at https://www.stats.gov.sa/sites/default/files/lm_2018_q4_en.pdf
- Tarride JE, Hopkins RB, Leslie WD, et al. The burden of illness of osteoporosis in Canada. Osteoporos Int. 2012;23:2591–2600.
- Sadat-Ali M, Al-Habdan IM, Al-Turki HA, et al. An epidemiological analysis of the incidence of osteoporosis and osteoporosis-related fractures among the Saudi Arabian population. Ann Saudi Med. 2012;32:637–641.
- National Plan for Osteoporosis Prevention and Management in the Kingdom of Saudi Arabia [Internet]. National Action Plan Working Group; 2018 [cited 2019 Mar 6]. Available from: https://www.moh.gov.sa/en/Ministry/MediaCenter/Publications/Documents/NPOPM-2018.pdf
- Al-Saleh Y, Sulimani R, Sabico S, et al. 2015 Guidelines for Osteoporosis in Saudi Arabia: recommendations from the Saudi Osteoporosis Society. Ann Saudi Med. 2015;35:1–12.
- Siggeirsdottir K, Aspelund T, Johansson H, et al. The incidence of a first major osteoporotic fracture in Iceland and implications for FRAX. Osteoporos Int. 2014;25:2445–2451.
- Global Burden of Disease Health Financing Collaborator Network. Past, present, and future of global health financing: a review of development assistance, government, out-of-pocket, and other private spending on health for 195 countries, 1995–2050. Lancet (London, England). 2019;393:2233–2260.