
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background
Following cardiovascular events, individuals often make choices about their working life that pose fiscal costs for the government in relation to lost tax revenue, increasing disability or early retirement. We evaluate the fiscal consequences for the Australian Government in atherosclerotic cardiovascular disease (ASCVD) patients with low-density lipoprotein >3.3 mmol/L after the maximum tolerated doses of a statin or when contraindicated or intolerant to statins, compared to evolocumab added to the standard of care.
Methods
The natural history of patients with ASCVD was evaluated using a multi-state Markov cohort model comparing evolocumab with current treatment practices. Published rates for the likelihood of being disabled and retiring prematurely in patients experiencing stroke or myocardial infarction were modeled. Reported government costs for annual disability payments and lost tax revenues from the nationally representative STINMOD + data set were used to estimate the fiscal consequences associated with attributable ASCVD events.
Results
The incremental tax gain associated with evolocumab in someone aged 40, 50 or 60 results in additional tax revenues of Aus$15,716, Aus$9,810 and Aus$4,217, respectively. Cost-savings attributed to disability payments of Aus$3,483, Aus$2,495 and Aus$4,619 were observed in those aged 40, 50 and 60, respectively. The ratio of evolocumab to fiscal benefits indicates that up to 52% of evolocumab costs are offset by future lifetime taxes paid and reduced social benefits payments in those treated aged 40. The ratio of fiscal benefits to costs in treating those aged 50 and 60 were 37% and 31%, respectively.
Conclusions
Applying a cross-sectorial government perspective budget impact assessment improves our understanding of fiscal changes attributed to ASCVD based on changes in premature mortality and work activity and how this influences lifetime tax contributions and public benefits. The main cost driver observed was associated with reduced ASCVD events that enabled people to remain productive and paying taxes.
Introduction
The consequences of severe health events such as heart attacks and strokes, often referred to as health shocks, can have far-reaching consequences as people establish different priorities and make important life choices following these eventsCitation1. The most significant choice that workers might make following a health shock is whether or not to continue working. Numerous studies have reported the likelihood of permanently discontinuing work following health shocks and chronic health conditions which include a range of conditions such as diabetes, heart disease, stroke, arthritis, skin diseases, and chronic painCitation2–5. It has been shown that individuals experiencing an acute hospitalization of more than three days, irrespective of the underlying health condition, have a 7% reduced likelihood of employment within 2 years following the event and the effect remained sustained up to 6 years post-hospitalizationCitation6. Furthermore, acute hospitalizations have also been shown to increase the probability of receiving disability payments and reduced earnings even in those that remained working, which suggests that some adjustments are made to their working conditionsCitation6. Prior studies indicate that the probability to continue working is dependent on the age and severity of the conditionCitation7. Additionally, it has been shown that an acute health event can influence the employment decisions of a spouseCitation2.
Previous studies have shown PCSK9 inhibitors to be a cost-effective option for those patients not responding to standard cholesterol-reducing therapyCitation8,Citation9. Whilst cost-effectiveness is useful for establishing value for money to health services, it fails to capture the broader economic consequences associated with preventing events that could lead to early retirement. In this analysis, we applied a public economic framework to evaluate consequences for the Australian Government following the introduction of a novel cardiovascular medicine proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor antibody therapy, evolocumab, for the prevention of myocardial infarction and stroke in adults with atherosclerotic cardiovascular disease (ASCVD). In Australia, evolocumab is indicated for the prevention of cardiovascular events, including primary hypercholesterolaemia and familial hypercholesterolaemia, in combination with optimally dosed statins or other lipid-lowering therapies. We constructed a disease state model that reflects different at-risk groups in Australia and estimated the likelihood of ASCVD events for those treated with evolocumab compared to the current standard of care. Factoring in the relationship between ASCVD events and future labour market choices made by these individuals, we estimated changes in fiscal outcomes for government using a public economic or “government perspective” comparative analytic frameworkCitation10.
The work described here builds on prior cost-effectiveness studies in high-risk atherosclerotic patients applying a public economic modeling framework to inform policy and funding decisions in AustraliaCitation11,Citation12. The modeling framework described here differs from a cost-effectiveness analysis as it considers a broader range of public economic costs and monetized benefits for the governmentCitation13. In this context, the present model evaluates how changes in morbidity and mortality attributed to ASCVD events following the introduction of evolocumab influence government tax revenue based on changes in work activity and social benefits, that is, disability payments in the cohort of treated subjects. By simultaneously looking at all government costs, we can better understand the impact that additional expenditure will have on government and potential cost offsets from disability payments, and the potential gains in tax revenue as people remain in the labour market.
Methodology
Model design
The natural history of patients with ASCVD, which includes coronary heart or cerebrovascular disease was evaluated using a multi-state Markov cohort model that compared evolocumab with the current standard of care (SoC) in Australia. The population considered are ASCVD patients reflecting the at-risk population in Australia with low-density lipoprotein (LDL) >3.3 mmol/L after maximum tolerated doses of a statin or contraindicated or intolerant to statins.
The model consisted of three alive states (ASCVD, MI and stroke) and two death states for those that die from ASCVD death or non-ASCVD death (Supplementary Materials). The transition between states was defined by treatment with evolocumab or the comparator resulting in a change in LDL where a mean percentage reduction in LDL of 59% (95% confidence interval, 58–60; p < .001) was observed in a randomized, double-blind multinational clinical trial at 48-weeksCitation14. Patients that discontinue treatment are assumed to achieve baseline level, with a 0% reduction in LDL attributable to evolocumab, and achieve the same level of LDL reduction as the SoC. The relationship between reductions in LDL and reductions in the proportional risks of ASCVD events rates have been described by the Cholesterol Treatment Trialists’ Collaborators (CTTC) whereby each 1 mmol/L reduction in LDL corresponds to a relative event rate of 0.78 for major vascular eventsCitation15. This relationship has been implemented by calculating the relative event rate corresponding to a reduction of x mmol/L as 0.78x. The ASCVD event rate was modelled as increasing in every year of the cycle which is consistent with the increased risk for events by ageCitation16. As previously reported the constant annual increases in cardiovascular events has a hazard ratio of 1.03 (95% CI 1.03–1.04) for a difference in age of 1 yearCitation16. Lipid-lowering therapy can translate into reductions in non-fatal ASCVD events, however, the effect can take up to 2 years for the effects to be observedCitation15. Non-fatal events are either MI or ischaemic stroke were split 59:41 in the base caseCitation17. Death rates from non-ASCVD causes have been estimated for Australian patients from all causes and cause-specific death rates using Australian life tables. Death rates for all causes and for diseases of the circulatory system (ICD10 I00-I99), by sex and 5-year age group, have been sourced from the General Record of Incidence of DeathCitation18. For each sex and 5-year age group, the proportion of all-cause deaths that were from diseases of the circulatory system was calculated as the death rate from diseases of the circulatory system divided by the all-cause death rate. Non-CV death rates have been calculated from the all-cause death rate and the proportion of deaths that are from diseases of the circulatory system. The sex and age-specific rates are used to infer the rates for each year in the model, given the baseline characteristics of the patient cohort.
Healthcare resource use
The model derived costs for each health state for treatment management and event costs. Acute costs for managing a fatal CHD event (Aus$3,423), of a non-fatal MI (Aus$9,969), and of a non-fatal stroke (Aus$24,476) have been derived from the Australian Statins ReviewCitation19. Cost for non-fatal events included the acute cost plus the estimated extra cost in the first 12 months after the event. Ongoing costs per month following an MI or stroke of Aus$160 and Aus$366, respectively were also includedCitation19. Patients who experienced multiple events accrued the acute cost for each event. The monthly treatment cost for evolocumab was derived from the approved PBS list price in Australia of Aus$488.95Citation20. As evolocumab was added to current therapy, no drug cost was applied for the current standard of care comparator.
Fiscal framework
Within each health state, patients can also be distributed to fiscal states. Fiscal states are determined by individuals’ labour market status and the subsequent fiscal relationship with the government based on their health status. Hence, for people with ASCVD who experience a CV event, labour market outcomes are likely to deteriorate while the probability of receiving disability and other Federal benefits increasesCitation13. As individuals experience CV events, they become increasingly likely to be permanently disabled or to die prematurely and thus, they incur more costs to the governmentCitation21.
In the current analysis, to quantify the public economic consequences of stroke and MI prevention that can be attributed to evolocumab compared to current treatment, patients in each health state were further distributed to fiscal states. There are three fiscal states that individuals from each CEA health state can be distributed: (1) Active (e.g. working, not working, not disabled); (2) Disabled as per the Australian social insurer Centrelink definition; and (3) death (an absorbing fiscal state). In contrast with CEA models, premature death in fiscal models reflects a loss of future tax revenue for the government, but simultaneously represents savings to the government as fewer people will receive public benefits in the future. The magnitude of the effect depends on the age at which death occurs in relation to lifetime taxes paid.
The distribution of people in the fiscal states changes following an ASCVD event as more people are likely to be disabled following the eventCitation10. Survivors of CV events have a higher likelihood of becoming disabled and thus, a higher probability of transitioning from the fiscal state “active” to the fiscal state “disabled”. During this transition between fiscal states, the model derives the public economic costs for the government. The likelihood of being out of work and disabled following a stroke or MI was based on Australian findings reported by Pit et al.Citation10 where significant differences in the odds of retiring were shown for females and males. As our fiscal model was not gender-specific, we applied a weighted odds ratio for the retirement of 2.7 and 1.6 following stroke or MI, respectively.
Public economic costs
The Australian Government provides a range of different transfer payments to citizens over the course of life depending on needs that are means-tested. Payment to individuals can include disability allowances, family allowances, pensions and a wide range of different payments depending on individual circumstances. We use a microsimulation model STINMOD + to estimate the average federal taxation and welfare payment for each combination of age cohort and disability status in 2018 in AustraliaCitation22. Specifically, STINMOD + uses nationally representative samples by age categories, therefore reflecting the age-specific employment income, tax payments and public benefits received over time. The model covers all major federal taxation and welfare schemes in Australia and it is often used for distributional analyses of income and welfare policiesCitation23,Citation24. In fiscal terms, citizens in Australia are classified as being active or disabled based on specified criteria. Within the STINMOD + data set, people meeting the criteria set by Centrelink as being disabled are included in the disability cohortCitation25. Within the fiscal analysis, we assume all subjects start in the active state. If they experience an ASCVD event, we apply the probability of transitioning from active to disabled.
Within the “active” fiscal state there is a heterogeneous range of profiles for those that are working and those not working and not disabled (e.g. early retirement, out of work, etc). Because the model is focused on public economic costs linked to CV events, it is not necessary to distinguish fiscally between those that are working or not working within the “active” fiscal state as those individuals retiring early and not disabled generally do not receive any public benefits. In contrast, transitioning to the “disabled” fiscal state attracts significant public benefits (). The STINMOD + output we use is in 5-year age bands, therefore the proportion of people retired increases over time and most dramatically at age 65 (a general retirement threshold in Australia, although not a mandatory retirement age). Pension costs per person were modified to reflect government policy objectives of transitioning people from state age pensions to self-funded pensions. We applied a value of 50% of people receiving state pension based on recent data for the proportion of recent retireesCitation26.
Table 1. Annual public benefit transfers for fiscal states Active and Disabled.
Direct and indirect taxes
The evolocumab fiscal model estimates age-specific direct and indirect tax payments for both treatment cohorts for active and disabled fiscal states. The direct taxes for each fiscal state were obtained from the STINMOD + tax-benefit microsimulation model containing 2018 tax reforms data (). STINMOD + was used to estimate annual direct tax contributions for the active and disabled fiscal states linked to the disease modeling for each treatment. The average reported Medicare levy paid by different cohorts is also reported as part of the STINMOD+. As the contribution varies by working status, this is an important component to include in the model estimations.
Table 2. Average annual net income taxes paid (direct taxes) and Medicare levy for active and disabled persons.
Annual indirect taxes paid to goods and service taxes (GST) were estimated based on applying household expenditure data for AustraliaCitation27 and applied to the proportion of annual salary that is spent on GST-liable items and estimated to be 67.9%. The rate for GST-liable items is comparable to previously published figures by the Australian Productivity CommissionCitation28. The percentage of GST-liable disposable income was then applied to the disposable income data generated in the STINMOD + to which the Australian GST rate was applied (Supplementary Materials).
Public economic costs calculations
The fiscal model generates average tax payments, average transfer payments received, and medical costs attributed to cardiovascular disease for both treatment options. For a cohort of patients treated with evolocumab and a cohort of patients receiving standard of care (SoC), the fiscal model estimates the sum of all taxes (direct and indirect) paid to the government and the present value of transfers received by the government of individuals throughout their lives and finally the total lifetime healthcare costs. The model counts costs over the remainder of life from the defined starting age. All costs in the model are for males and females combined and discounted at 5% as per Australia guidelinesCitation29. To estimate the benefit for the government, we assessed the incremental fiscal benefit–cost ratio (fBCR) using the following equation based on incremental public investment. The incremental fBCR estimates the ratio between changes in medical expenses (Δm), transfer payments from government (Δtr) and change in taxes (ΔTax) linked to the outcome and cost differences between SoC and evolocumab (Δdrug):
m: medical expensestr: transfer paymentsTax: taxes collecteddrug: drug therapy, evolocumab compared to standard of care
Sensitivity analysis
A univariate sensitivity analysis (SA) based on plausible variation in key model parameters was applied to explore the robustness of the findings. Model parameters inputs were explored individually in the SA applying a base case of age 50, baseline LDL 3.3 mmol/L and 5% discount rate. The variance applied for each parameter is described in .
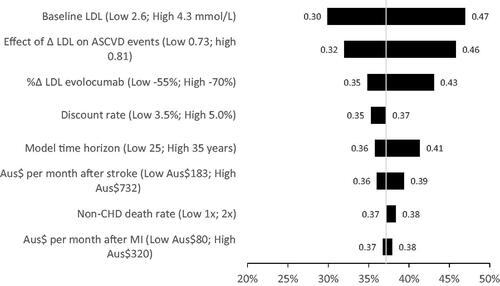
Figure 1. Univariate sensitivity analysis of key parameters on fiscal benefit cost ratio for persons aged 50-years-old in Australia.
Results
Changes in fiscal parameters for those treated with evolocumab + SoC compared to current treatment practices with treatment initiation at three different ages are described in . Government spending reported as a negative value indicates that reduced spending is observed on the program based on adopting the evolocumab strategy, that is, decreased expenditure. Increased government spending is shown as positive values based on adopting the evolocumab treatment program. In all instances, government costs increase for evolocumab, but reduce spending on other programs (e.g. medical costs and transfer payments). Incremental changes in government tax revenue are also reflected, based on adopting evolocumab where a positive value indicates increased taxes paid compared to current treatment practices.
Table 3. Incremental change in fiscal parameters based on treatment starting age (evolocumab – current treatment practice).
Treating a 40-year-old individual generates an additional Aus$15,716 in taxes with evolocumab compared to current treatment practices. The incremental tax associated with treating an individual aged 50 or 60 with evolocumab + SoC compared to SoC results in additional tax revenue for the Australian Government of Aus$9,810 and Aus$4,217, respectively. The absolute fiscal values for evolocumab and current treatments are provided in the Supplementary Materials.
For the age groups assessed, a reduction in medical spending of approximately Aus$4,300 per person treated was observed. There was little variation in savings based on age as costs were mostly attributed to acute events. Cost savings in government transfers were also observed for the three age cohorts assessed with reductions of Aus$3,483, Aus$2,495 and Aus$4,619 based on the age of treatment of 40, 50 and 60, respectively.
As observed from the fBCR analysis, the returns for the government are much greater when preventing events in younger individuals. For those treated with evolocumab, a fBCR of 0.52 is achieved in those aged 40. In contrast, the fBCR for evolocumab-treated subjects aged 50 and 60 a fBCR of 0.37 and 0.31 are observed.
Sensitivity analysis
The model was most sensitive to the baseline LDL score varying from fBCR of 0.30 to 0.47 when baseline LDL was 2.6 mmol/L and 4.3 mmol/L, respectively (). The effects of LDL on ASCVD events and the effect of evolocumab had the second and third greatest impact on the fBCR. The influence of monthly costs of stroke and MI management and non-CHD death had limited influence on the fBCR of evolocumab.
Discussion
Cardiovascular-related diseases are the leading cause of mortality worldwide with an estimated 17.9 million deaths annuallyCitation30. Australia is no exception to this trend, where approximately 4.8% of the population report one or more heart or vascular conditions including stroke, with an expenditure of more than Aus$7.8 billion annually accounting for approximately 12% of all healthcare expenditure in AustraliaCitation31,Citation32. In addition to direct health costs, previous studies in Australia report the impact of cardiovascular disease on the government in terms of reduced income and taxes paid compared to those fully employed without a chronic health conditionCitation21.
Following many health events, that is, health shocks and intensifying chronic health conditions, individuals will make life choices that influence their labour market condition. These choices are informed by many factors including the severity of their condition, age, time to retirement, social conditions and public support programs available that support people with disabilitiesCitation1,Citation7. These choices are important as they can influence an individual’s future earning capacity and their ability to save money for retirementCitation33,Citation34. For governments, these decisions are important as they can influence the size of the available workforce, social support payments and the amount of taxes collected over the lifetime of individualsCitation35. Furthermore, the number of people that become dependent on public programs when disabled creates deadweight losses in the economy as fewer numbers of people are working to support those dependent on public benefits.
Previous studies have reported on the cost-effectiveness of evolocumab based on changes in healthcare expenditureCitation8,Citation9. In this analysis we build on prior work describing the broader consequences of cardiovascular diseases and demonstrate how preventing attributable events can improve fiscal outcomes for government. In terms of improved tax revenue, we demonstrate that preventing an ASCVD event with evolocumab added to SoC for lipid-lowering in someone aged 40 in Australia can increase tax revenue by approximately Aus$15,716 over their remaining lifetime. Because fiscal events are influenced by the time at which they occur, preventing ASCVD events with evolocumab added to SoC in those aged 50 and 60 leads to future projected lifetime taxes paid of Aus$9,810 and Aus$4,217, respectively. The variation in incremental taxes paid illustrates the benefits of early identification and treatment that can lead to preventing or delaying the timing of events. A reduction in transfer payments was also observed for the three different age cohorts treated. The cost savings were likely attributed to changes in disability and other support payments, despite the countervailing fiscal costs of improved survival with evolocumab which leads to small increases in pension payments. The fiscal cost offsets described here are not captured in conventional cost-effectiveness analysis and help to offset the costs of introducing evolocumab.
Fiscal models in health offer a unique perspective compared to cost-effectiveness analysis. In CEA, healthcare resources are considered a cost and these costs discontinue when the person recovers or dies, in which circumstances there are no further costs. By comparison, in fiscal models, there can be associated losses even in death in those individuals that die prematurely and do not achieve their projected lifetime taxes paid. Similarly, premature mortality can give rise to some fiscal savings from reduced pension payments and future unrelated healthcare costs. The fiscal framework described here can be viewed as a cross-sectoral government perspective budget impact model. In this regard, we can explore how policy changes that influence health, or investments in healthcare that change morbidity and mortality, have future costs and tax revenue implications. This makes the fiscal modeling approach an enhanced budget impact model which takes a broader view regarding healthcare and expenditure for evaluating technologies.
Cardiovascular disease poses significant economic consequences for the Australian Government, largely attributed to changes in workforce participation in working-aged adults which influences government welfare payments and lifetime tax revenueCitation21. The cost consequences are profound beyond the health service and can also influence personal wealth accumulation which influences an individual’s ability to remain financially independentCitation36. Previous studies have illustrated that people experiencing strokes and myocardial infarctions in Australia have an increased likelihood of retiring early, increasing reliance on government social support programs, paying lower lifetime taxes and experiencing reduced wealth throughout their lifetimeCitation10,Citation21,Citation34. Furthermore, a study in Australia has reported that some individuals from non-impoverished families have an increased risk of falling into poverty after developing heart diseaseCitation37. The relationship between developing heart disease and poverty was age-dependent with increased risk in younger people compared to those aged 60, where the risks were much lower when older individuals have higher accumulated wealth compared to younger persons.
The analysis presented here describes fiscal benefits achieved from lowering cholesterol and the prevention of future cardiovascular events attributed to evolocumab that can have fiscal consequences for governments. The analytic approach described here is not unique to evolocumab and can be applied to evaluate current or future PCSK9 inhibitors or any other healthcare investmentCitation13,Citation38,Citation39. The magnitude of fiscal effects can be influenced by several factors including patient characteristics, the nature of events prevented and how events are likely to influence future lifetime trajectories and employment activity. Primary prevention of events will likely have greater fiscal benefit as they prevent people from initially withdrawing from work and in younger individuals, whereas preventing secondary events will only apply to those that remained working after the first event. In familial hypercholesterolemia which impacts people of younger ages, preventing cardiovascular events in early life should enable them to work longer which can offer considerable fiscal benefits.
To underscore the important relationship between investments in healthcare and their impact on government public accounts, we compare the impact of treating individuals with evolocumab + SoC between the ages of 40 and 60 and the remaining lifetime fiscal consequences. Due to improved survival in working-aged adults, we estimate improved productivity that generates future direct tax revenues for the Australian Government. Furthermore, increased survival leads to improved indirect tax revenue for the government attributed to consumption taxes. Moreover, several fiscal savings can be achieved for the government due to reduced disability and reduced healthcare cost savings.
The analysis described here monetizes changes in health-related productivity into future fiscal impact for the government. Because the analysis focuses solely on future financial transactions between citizens and state based on changes in lifetime work activity and taxes paid, this approach undervalues the health-related benefits for society that can be captured using preference-based utility approaches and the benefits that people experience from being healthy. Moreover, as the analysis captures only transactions between government and individuals, we fail to capture reduced lifetime earnings in those individuals experiencing non-fatal ASCVD events that can influence living conditions and exacerbate domestic social and economic factors. Furthermore, the approach described here undervalues the economic relationships that exist within society and economic multiplier effects that can be achieved from spending on health and improving outcomesCitation40. In this regard, we see this approach to supplement traditional CEA approaches for informing a broader range of interested parties involved in the allocation of resources.
A discount rate of 5% was applied in the base case analysis as recommended by the Australian PBAC guidelines for conducting cost-effectiveness analysis. The analysis described here is not a CEA, however, we applied the recommended discount rate for consistency with local practices and cost-effectiveness guidelines, although this approach is inconsistent with public economic analysis normally adopted by governments. By convention, the discount rate is meant to reflect the future value of money which varies and is influenced by prevailing economic conditions. The framework described here is based on the generational accounting framework where it is suggested to use the long-term bond rate for discounting as this more accurately reflects the future value of money in AustraliaCitation41.
Conclusions
Cardiovascular is one of the largest health and economic burdens for developed and developing countries in terms of morbidity, premature mortality and healthcare expenditure. We demonstrate that taking a broader public economic perspective can provide insights regarding a more comprehensive assessment of the public burden for governments, based on reduced lifetime taxes paid and public benefit support needs. In tandem, we apply this framework to evaluate new technologies providing governments the opportunity to take a broader public sector budget impact perspective to understand how investments within the health sector can have future fiscal consequences.
Transparency
Role of funding source
The funders of this work had no role in the interpretation and reporting of the findings. The authors retained full editorial control over the content described in this research.
Declaration of interest
The work conducted by NK and MPC was supported by a grant from Amgen. The authors hold no financial interests in the supporting organization. JL is an employee of the University of Canberra and received no compensation for academic contributions to this work. All authors have reviewed the final manuscript. This work has not been previously reported.
JME peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Author contributions
NK: conceptualization, investigation, resources, formal analysis, results interpretation, writing, review & editing manuscript; MC: conceptualization, investigation, resources, formal analysis, results interpretation, writing, review & editing manuscript; JL: conceptualization, data curation, application of results, formal analysis, review and editing manuscript
Supplemental Material
Download PDF (180.8 KB)Acknowledgements
We would like to thank Mendel Grobler for sharing his insights into the fiscal workings of Australia and providing valuable source documents.
Additional information
Funding
References
- Pond R, Stephens C, Alpass F. How health affects retirement decisions: three pathways taken by middle-older aged New Zealanders. Ageing & Society. 2010;30(3):527–545.
- McGeary KA. How do health shocks influence retirement decisions? Rev Econ Household. 2009;7(3):307–321.
- Saastamoinen P, Laaksonen M, Kääriä S-M, et al. Pain and disability retirement: a prospective cohort study. Pain. 2012;153(3):526–531.
- Zucchelli E, Jones AM, Rice N, et al. The effects of health shocks on labour market exits: evidence from the HILDA survey. Australian J Labour Econ. 2010;13:191–218.
- Meding B, Wrangsjö K, Burdorf A, et al. Disability pensions due to skin diseases: a cohort study in Swedish construction workers. Acta Derm Venereol. 2016;96(2):232–236.
- García-Gómez P, Van Kippersluis H, O’Donnell O, et al. Long term and spillover effects of health shocks on employment and income. J Hum Resour. 2013;48(4):873–909.
- Jiménez‐Martín S, Labeaga Vilaplana Prieto MJ, Vilaplana Prieto C. A sequential model of older workers’ labor force transitions after a health shock. Health Econ. 2006;15(9):1033–1054.
- Zomer E, Kumar R, Tonkin A. PCSK9 inhibitors in Australia: a cost-effectiveness analysis. Heart, Lung Circ. 2017;26:S348.
- Kazi DS, Penko J, Coxson PG, et al. Updated cost-effectiveness analysis of PCSK9 inhibitors based on the results of the FOURIER trial. JAMA. 2017;318(8):748–750.
- Pit SW, Shrestha R, Schofield D, et al. Partial and complete retirement due to ill-health among mature age Australians. Public Health. 2013;127(6):561–571.
- Fonarow GC, van Hout B, Villa G, et al. Updated cost-effectiveness analysis of evolocumab in patients with very high-risk atherosclerotic cardiovascular disease. JAMA Cardiol. 2019;4(7):691–695.
- Fonarow GC, Keech AC, Pedersen TR, et al. Cost-effectiveness of evolocumab therapy for reducing cardiovascular events in patients with atherosclerotic cardiovascular disease. JAMA Cardiol. 2017;2(10):1069–1078.
- Connolly MP, Kotsopoulos N, Postma MJ, et al. The fiscal consequences attributed to changes in morbidity and mortality linked to investments in health care: a government perspective analytic framework. Value Health. 2017;20(2):273–277.
- Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376(18):1713–1722.
- Flather M. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170 000 participants in 26 randomised trials. The Lancet. 2010;376:1670–1681.
- Wilson PW, D’Agostino R, Sr Bhatt DL, et al. An international model to predict recurrent cardiovascular disease. Am J Med. 2012;125(7):695–703.
- Lindh M, Banefelt J, Fox KM, et al. Cardiovascular event rates in a high atherosclerotic cardiovascular disease risk population: estimates from Swedish population-based register data. Eur Heart J Qual Care Clin Outcomes. 2019;5(3):225–232.
- AIHW. General record of incidence of mortality (GRIM). Canberra (Australia): Australian Government; 2011.
- PBS. Review of statin therapies. Canberra (Australia): Australian Government; 2012.
- PBS. Medicine list. Canberra (Australia): Australian Government; 2019.
- Schofield D, Shrestha R, Percival R, et al. The personal and national costs of CVD: impacts on income, taxes, government support payments and GDP due to lost labour force participation. Int J Cardiol. 2013;166(1):68–71.
- Li J. STINMOD + Overview. 2019. https://stinmod.canberra.edu.au/research/stinmodplus/model_doc/overview
- Australian Council of Social Services (ACOSS). The impact on households of tax cuts and lifting Newstart Allowance. 2019. https://www.acoss.org.au/wp-content/uploads/2019/04/Impact-of-tax-cuts-and-Newstart-increase-on-households_FINAL.pdf
- Li J, La HA, Sologon DM. Policy, demography, and market income volatility: what shaped income distribution and inequality in Australia between 2002 and 2016? Rev Income Wealth. 2020. DOI:https://doi.org/10.1111/roiw.12467
- CentreLink. Disability support pension. Canberra (Australia): Australian Government Services; 2020.
- Challenger. Super is delivering for people about to retire. Canberra (Australia): Challenger; 2019.
- ABoS. Household expenditure survey, Australia: summary of results, 2015-16. Canberra (Australia): Australian Bureau of Statistics ABS; 2017.
- PC. Goods and Services Tax. Economic Implications of an Ageing Australia: 2019.
- Pharmaceutical Benefits Advisory Committee. Guidelines for preparing a submission to the Pharmaceutical Benefits Advisory Committee. Canberra (Australia): PBAC; 2016. Available from: http://pbac.pbs.gov.au:8999/content/information/files/pbac-guidelines-version-5.pdf/
- WHO. Cardiovascular Diseases. 2017. Available from: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds)
- ABoS. National health survey: first results 2017-18. Canberra (Australia): Australian Bureau of Statistics ABS; 2018.
- AIHW. Health care expenditure on cardiovascular diseases 2008–09. Bruce (Australia): AIHW; 2014.
- Schofield DJ, Callander EJ, Shrestha RN, et al. Labour force participation and the influence of having CVD on income poverty of older workers. Int J Cardiol. 2012;156(1):80–83.
- Schofield D, Passey M, Percival R, et al. Retiring early with cardiovascular disease-impact on individual’s financial assets. Int J Cardiol. 2011;146(1):125–126.
- Black DC. Dame Carol Black’s review of the health of Britain’s working age population. Working for a healthier tomorrow. London (UK): London Crown; 2008.
- Schofield D, Kelly S, Shrestha R, et al. The long term financial impacts of CVD: living standards in retirement. Int J Cardiol. 2012;155(3):406–408.
- Callander EJ, Schofield DJ. The risk of falling into poverty after developing heart disease: a survival analysis. BMC Public Health. 2016;16:570.
- Sabatine MS. PCSK9 inhibitors: clinical evidence and implementation. Nat Rev Cardiol. 2019;16(3):155–165.
- Strilchuk L, Fogacci F, Cicero AF. Safety and tolerability of injectable lipid-lowering drugs: an update of clinical data. Expert Opin Drug Saf. 2019;18(7):611–621.
- Stuckler D, Reeves A, Mckee M. Social and economic multipliers: what they are and why they are important for health policy in Europe. Scand J Public Health. 2017;45(18):17–21.
- Auerbach AJ, Gokhale J, Kotlikoff LJ. Generational accounting: a meaningful way to evaluate fiscal policy. J Econ Persp. 1994;8(1):73–94.