
Abstract
Aim
The aim of this study was to capture and measure the impact of caregiving for an adult with uncontrolled drug-resistant focal-onset seizures (FOS) on the caregivers’ quality of life (QoL), and to quantify the costs of productivity losses associated with providing informal care in this patient population.
Methods
An online survey, which included the EQ-5D-5L, CarerQol-7D and the Work Productivity and Activity Impairment: Specific-Health Problem (WPAI:SHP) questionnaires, was administered to caregivers of individuals with uncontrolled drug-resistant FOS in the United Kingdom (UK), France, Spain, Germany, Italy, and Sweden.
Results
The study included 345 caregivers. Most were males, aged between 25 and 34 years old whose caring responsibilities took between 15 and 24 h per week. The caregivers’ mean EQ-5D-5L score was 0.6, with 95% confidence intervals (CI) of [0.58, 0.63], whilst the mean CarerQol-7D score was 72.61 [70.46, 74.76]. Caregivers’ mental health was the most substantially affected aspect of their QoL. In addition, most caregivers reported deriving some or a lot of fulfilment out of their caregiving tasks. The WPAI:SHP showed that the mean percentage of work impairment due to caregiving responsibilities was 63%, [59.75, 66.26]. The mean annualised costs of productivity losses per caregiver were estimated at €14,872 [€11,908; €17,888].
Limitations
One limitation consisted in the use of an online survey instead of a face-to-face interview. However, the medical terms were clearly explained, and examples were provided to help participants to give accurate responses. Another limitation was that the respondents self-reported as caregivers. Efforts were made to mitigate this weakness by using screener questions.
Conclusion
This study found that providing informal care for people with uncontrolled drug-resistant FOS had a negative impact on caregivers’ QoL, with mental health being affected the most. However, caregivers found their role fulfilling and had support with their caring tasks.
1. Introduction
Epilepsy is a serious chronic debilitating neurologic condition that affects more than 50 million people worldwide and which is characterised by recurrent unprovoked seizures caused by a disruption in the neuronal excitation-inhibition balance in the brainCitation1,Citation2. The most common type of seizures experienced by patients with epilepsy is focal-onset seizures (FOS). They begin on one side of the brain and are categorised into those with retained and impaired awarenessCitation3.
The standard treatment for FOS in adults consists of anti-seizure medication (ASM) which should be selected based on the patient’s seizure type, age, gender, comorbidities, and the drug’s adverse effectsCitation4,Citation5. Although long-term seizure remission is achieved in up to 70% of patients with epilepsy, the remaining 30% are failed by the initial ASM monotherapy or subsequent multiple ASM combinations and continue to experience seizuresCitation6,Citation7. These individuals are considered to have drug-resistant epilepsy (DRE)Citation8. Apart from polytherapy with various ASM, other treatment options for DRE patients include resective surgery, vagal nerve stimulation, and the ketogenic dietCitation9.
Focal epilepsy is commonly associated with comorbid health conditions such as psychiatric diseasesCitation10. Patients with FOS often experience stigma associated with seizures which leads to self-imposed isolation and deterioration of their interpersonal relationships and social lifeCitation11. In addition, they have a reduced quality of life (QoL)Citation12. Patients with DRE account for most of the burden of epilepsy due to increased stigma associated with experiencing uncontrolled seizures as well as suffering from comorbid health conditionsCitation13.
Many patients with epilepsy require support from a caregiver as they cannot manage without aid. A caregiver is someone from the patient’s social environment who provides care, but who does not usually receive financial compensation. Depending on the severity and frequency of their symptoms, the care needs of patients with epilepsy vary greatly from only requiring support during a seizure (i.e. calling for medical help, giving first aid or emergency medication) to needing full-time assistance, including help with everyday tasks, accompanying them to hospital appointments, providing transport, or helping them to maintain a safe environmentCitation14.
Acting as a caregiver can have both a positive and negative impact on the caregivers’ wellbeing. On the one hand, providing informal care requires a significant level of responsibility and commitment which can be psychologically and physically exhausting. In addition, caregivers invest time to take care of the patient, meaning that they have less time for leisure activities or for their work. This can become burdensome and lead to feelings of isolation and depressionCitation14. On the other hand, caregivers might find their caring role rewarding and fulfillingCitation15. In addition, providing informal care does not only have an effect on the caregivers’ well-being but also has an economic societal impact, as the time spent caregiving has an opportunity costCitation16.
It is widely recognised by health technology assessment (HTA) bodies that healthcare interventions can affect the QoL of both patients and caregivers. In England, the National Institute of Health and Care Excellence (NICE) states in its 2013 reference case that perspectives on outcomes should also include the health effects on carers, when relevantCitation17. In addition, NICE recommends health outcomes to be expressed as quality-adjusted life years (QALYs), which combine QoL and length of life, and yield a utility value anchored on a scale of 0 (equivalent to the dead) and 1 (full health) Citation17. The impact of a patient intervention on caregivers’ QoL can be significant and can occur for several reasons, including a change in the patient’s requirement for informal care, a change in emotional response to the patient’s condition or a change in the carer’s attitudeCitation18.
Hence, it is critical for economic evaluations to include health-related utility data for caregivers. The aim of this study was to measure the impact of caregiving for an adult with uncontrolled drug-resistant FOS on the caregivers’ health-related quality of life (HRQoL), and to quantify the costs of productivity losses associated with providing informal care in this patient population.
2. Methods
2.1. Study sample
Caregivers of adults with uncontrolled drug-resistant FOS from the UK, Germany, France, Italy, Spain, and Sweden were recruited via online panels by an online sampling agency, called Borderless Access. The selected individuals were contacted by the panel company and were provided with a link to take part in the survey. The link included information about the survey so that the individuals could make an informed decision about whether to participate or not. Upon completion of the survey, respondents were compensated with e-points that had a monetary value and could be used to make purchases. To be eligible to participate, respondents had to be adults (18 years or above) and identify as a caregiver for an adult who has a clinical diagnosis of focal epilepsy. In addition, the individuals the respondents cared for were required to have experienced at least three FOS and at least one seizure of disabling nature (i.e. with impaired awareness or focal to bilateral tonic-clonic seizure) in the past 28 days and to have previously been resistant to a minimum of two ASM. Data were collected in November 2020.
2.2. Study design
The survey consisted of background questions, caregiver burden questions, a generic preference-based QoL measure (EQ-5D-5L), a caregiver-specific measure (CarerQol-7D), and an economic burden measure, the Work Productivity and Activity Impairment Questionnaire: Specific Health Problem (WPAI:SHP). The survey was made available in English, German, French, Italian, Spanish, and Swedish. All respondents were requested to give consent before taking part in the survey and were asked to complete the survey only once. The survey was given a favourable ethical opinion from an independent reviewer working under the auspices of the Association of Research Managers and Administrators.
2.2.1. Background and caregiver burden questions
Respondents were asked about their socio-demographic details such as age, gender, occupational status, education, and geographical location. They were also asked about the age, disease history (i.e. type of FOS, frequency of seizures), and treatment experience (i.e. number of ASM prescribed over their lifetime and side effects) of the individual they cared for. In addition, respondents completed questions assessing their caregiver burden (i.e. type of care provided, average time spent caring per week).
2.2.2. Instruments
The EQ-5D-5L is a well-established generic, preference-based instrument that is commonly used to measure HRQoL across a variety of conditionsCitation19. The EQ-5D-5L evaluates patients’ HRQoL on five dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), each being characterised by five levels of severity (no problems, slight problems, moderate problems, severe problems, extreme problems). In the UK, each health profile described by the EQ-5D-5L yields a utility value anchored on a scale of 1 and −0.594, where 1 represents full health and −0.594 represents a state worse than death.
The CarerQol-7D is a validated instrument for measuring caregivers’ QoLCitation20. It measures two positive dimensions (fulfilment and support), and five negative dimensions (relational problems, mental health, physical health, financial problems, and problems combining daily activities with caring) of caregivingCitation21. Each dimension has three answering levels (no, some, a lot). The CarerQol-7D instrument generates caregiving utility values ranging between 0 and 100, where 0 indicates the worst informal care situation and 100 represents the best informal care situationCitation21. The CarerQol-7D was not administered to caregivers residing in France as a French version is not currently available.
The WPAI:SHP is a self-administered questionnaire used to assess the burden of caregiving on work productivityCitation22. The WPAI:SHP consists of six questions that establish employment status, hours missed from work due to caregiving, the number of hours worked, and the extent to which caregiving responsibilities affect both work productivity and non-work-related daily activities. Higher scores derived from the questionnaire suggest higher levels of impairmentCitation22.
2.3. Statistical analysis
2.3.1. Descriptive and caregiver burden statistics
Caregivers’ socio-demographic details, clinical data of the individuals cared for, and caregiver burden data were summarised using contingency tables.
2.3.2. Quality of life and economic burden
The EQ-5D-5L scores reported by respondents from all countries were pooled and were converted into utilities by applying the UK crosswalk value set which maps the EQ-5D-5L to the EQ-5D-3L, as per NICE recommendationCitation17. Similarly, the UK CarerQol tariff was used to obtain caregiving utilities from the CarerQol-7D scores reported by respondents from all countriesCitation23. WPAI:SHP data were used to derive four WPAI:SHP percentages which measure absenteeism, reduced productivity while at work, work impairment, and impairment in daily activities performed outside of work.
The EQ-5D-5L, CarerQol-7D and WPAI:SHP scores were summarised using mean, standard deviation, range, median and interquartile range. Summaries of dimensions for EQ-5D-5L and CarerQol-7D were also described (number and percentage reporting problems on each level for each dimension). Using a t-test, the mean EQ-5D-5L score found in our study sample was compared to the mean EQ-5D data for the average person (age/sex adjusted) within the UK general populationCitation24. We note that there are no CarerQol-7D or WPAI data available for the average person within the UK general population.
The cost of lost productivity due to providing informal care was determined using the Human Capital approach, which assumes that productivity losses are incurred up to a person’s retirementCitation25. The cost of lost productivity over a one-week period was calculated by multiplying the working hours lost by caregivers due to their caregiving responsibilities per week (derived from the WPAI:SHP) and the EU-27 average hourly labour cost in 2019, estimated at €27.70Citation26. Costs of productivity losses were summarised using mean, standard deviation, median and interquartile range. Assuming that the survey responses were typical of an average week, the average annualised costs per caregiver were then estimated.
2.3.3. Exploratory multivariable regression and subgroup analysis
An exploratory multivariable regression was performed to examine the impact of socio-demographic characteristics, clinical data, and caregiver burden onto the EQ-5D-5L and CarerQol-7D utility scores. Socio-demographic details (e.g. age, gender, degree, country), clinical data (e.g. length of diagnosis, FOS frequency, length of seizure-free period, seizure type, disabling seizures frequency, number of ASMs) and caregiver burden characteristics (e.g. time spent caring, type of care provided) were included as independent variables. Statistical significance was designated at p < .05.
In addition, an exploratory subgroup analysis was conducted to assess whether the frequency of FOS affects the EQ-5D-5L, CarerQoL-7D, WPAI:SHP scores, and costs of work productivity losses. All statistical analyses were conducted using Stata version 15.1 (StataCorp LP, College Station, TX, USA).
3. Results
3.1. Descriptive and caregiver burden statistics
shows the socio-demographic details of the caregivers included in the study. The sample consisted of 345 caregivers: 86 from the UK, 47 from Germany, 44 from France, 70 from Italy, 51 from Spain, and 47 from Sweden. The largest group of caregivers (38.55%) was aged between 25 and 34 years old. Most of them (59.48%) were male and had a university degree (80.41%). Caregivers were able to report multiple roles in terms of occupation. The results indicated that approximately 62.69% worked full-time, 16.62% worked part-time and 14.28% identified as full-time caregiver.
Table 1. Caregivers’ socio-demographic details.
summarises the background characteristics of the individuals cared for. The age range was fairly equally distributed; however, the largest group of individuals cared for (28.99%) was over 65 years old. Approximately 36.44% of the individuals receiving care were diagnosed with FOS between six and ten years ago. The longest continuous seizure-free period in the last 28 days for the largest group of individuals cared for (38.89%) was between 6 and 15 days. The largest group of individuals cared for (35.96%) had experienced three FOS, with focal impaired awareness being the most frequently experienced type of seizure (51.76%). In addition, 58.24% of the individuals cared for had experienced between two and five seizures of disabling nature in the last 28 days. In terms of ASM prescribed over their lifetime, 35% and 34.12% of individuals receiving care had been prescribed three and two ASM, respectively. The most prevalent side effects associated with ASM were fatigue (45%), dizziness (43%), headache (38%), drowsiness (36%), and nausea/vomiting (35%). Only 3% of caregivers indicated that the individual they cared for had suffered no side effects.
Table 2. Socio-demographic characteristics and clinical data of the individuals with FOS.
describes the caregiver burden characteristics. The time spent on caregiving varied within the sample, with the largest group of caregivers (27.94%) reporting between 15 and 24 h per week. Most caregivers (52.21%) accompanied the individual they cared for to a hospital or general practitioner (GP) appointment one to three times in the last 28 days. Moreover, 49.69% of hospital appointments were either with a neurologist or an epilepsy nurse specialist. The most frequently reported types of care provided by caregivers were offering psychological support (53%), staying with the individual after a seizure (43%), and aiding with everyday tasks (42%).
Table 3. Caregiver burden characteristics.
3.2. Quality of life and economic burden
Caregivers reported a mean EQ-5D-5L utility score of 0.6 (SD: 0.27), ranging from −0.24 to 1, and a mean EQ-VAS score of 64.23 (SD: 21.41), ranging from 0 to 100. The median EQ-5D-5L utility score was 0.62 [IQR: 0.44–0.8], while the median EQ-VAS score was 67.5 [IQR: 50–81]. In addition, the mean EQ-5D-5L utility score (0.6) for the caregivers included in our study was significantly lower (p < .01) than the average EQ-5D utility score (0.9) for the general UK population. Furthermore, caregivers reported a mean CarerQol-7D score of 72.61 (SD: 18.71), ranging from 20 to 100, and a mean CarerQol-VAS score of 6.64 (SD: 1.93), ranging from 1 to 10. The median CarerQol-7D score was 75.5 [IQR: 61.8–86.9], while the median CarerQol-VAS score was 7 [IQR: 5–8].
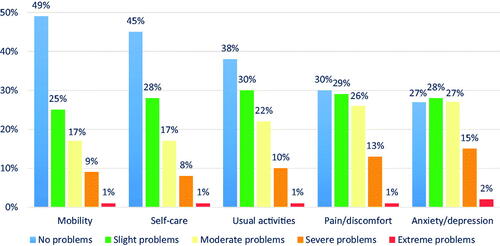
shows the proportions of the EQ-5D-5L dimensions. Most caregivers had no or slight problems in mobility (74%), self-care (73%), and usual activities (68%). Caregivers reported the greatest problems in mental health, with 44% reporting moderate, severe or extreme anxiety/depression. In addition, 40% of caregivers experienced moderate, severe, or extreme pain/discomfort.
Figure 1. Percentages reporting each level for the EQ-5D-5L dimensions.
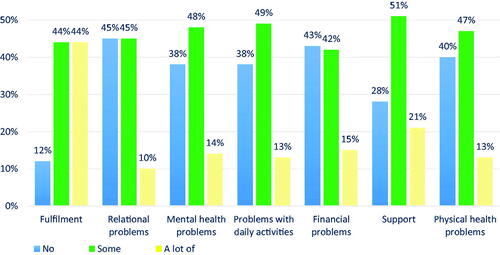
presents the proportions on the CarerQol-7D dimensions. Most caregivers (88%) derived some or a lot of fulfilment out of providing informal care, whereas 72% reported some or a lot of support with their caregiving responsibilities when needed. Caregivers reported the lowest scores in mental health and daily activities, with 62% of respondents having some or a lot of problems in each dimension.
Figure 2. Percentages reporting each level for the CarerQol-7D dimensions.
The WPAI:SHP indicated that the average percent of work time missed by respondents due to caregiving was 26.19% (SD: 23.91%), while the median was 18.18% [IQR: 6.38%–46.15%]. Caregivers reported an average percent impairment whilst working of 53.41% (SD: 25.13%), with a median of 60% [IQR: 40%–70%]. They also reported an average percent overall work impairment due to caregiving of 63% (SD: 25.92%), with a median of 69.76% [IQR: 50%–84.4%], and an average percent activity impairment due to caregiving of 56.34% (SD: 23.86%), with a median of 60% [IQR: 40%–70%]. All scores spanned from 0% to 100%. In addition, the mean cost of productivity losses per caregiver over a one-week period was €286 (SD: €461), ranging from €0 to €4,654. As it is usually found in the literature, the distribution of costs was skewed, with relatively low costs for most caregivers and high costs for a few caregivers. The median cost per caregiver over a one-week period was €139 [IQR: €55-€332]. The average and median annualised costs per caregiver were estimated at €14,872 and €7,228, respectively.
3.3. Exploratory multivariable regression and subgroup analysis
The findings of the exploratory multivariable regression analysis using the EQ-5D-5L utility score as the dependent variable are shown in . Caregivers in Sweden reported the lowest EQ-5D-5L utility score (β = −0.07, p = .23). There was a trend in lower EQ-5D-5L utility scores with increased age. Other socio-demographic details, such as gender and degree, were not correlated to the EQ-5D-5L utility score. In terms of the clinical characteristics of the individual cared for, the frequency of disabling seizures was negatively associated with the EQ-5D-5L utility score at a statistically significant level (β = −0.13, p = .006). There was no clear pattern between the remaining clinical data of the individual cared for, the time spent caring or the type of care provided, and the EQ-5D-5L utility score.
Table 4. Exploratory multivariate regression results for the EQ-5D-5L.
displays the findings of the exploratory multivariable regression analysis using the CarerQol-7D utility score as the dependent variable. Caregivers in Sweden reported the lowest CarerQol-7D utility score (β = −8.909, p = .02). Other socio-demographic details such as age, gender, and degree were not found to be associated with the CarerQol-7D utility score. In terms of the clinical characteristics of the individual cared for, there was a trend in lower CarerQol-7D score with increased FOS frequency. There was no clear relationship between other clinical data of the individual cared for, time spent caring, or the type of care provided, and the CarerQol-7D score.
Table 5. Exploratory multivariate regression results for the CarerQol-7D score.
presents the results of the subgroup analysis. Both EQ-5D-5L and CarerQol-7D utility scores were higher for the caregivers of individuals experiencing three FOS compared to the caregivers of individuals experiencing four or more FOS. However, the difference in EQ-5D-5L utility scores was not statistically significant (p = .08), whereas the difference in CarerQol-7D utility scores was (p < .001). Moreover, the costs of lost productivity per caregiver were lower for the caregivers of individuals experiencing three FOS than for the caregivers of individuals experiencing four or more FOS, but the difference was not statistically significant (p = .1). In addition, there was a trend in lower WPAI:SHP scores with increased FOS experienced by the individuals cared for. We note that the difference in percent work time missed between caregivers of individuals experiencing three FOS compared to caregivers of individuals experiencing four or more FOS was statistically significant (p = .01).
Table 6. EQ-5D-5L, CarerQol-7D, WPAI:SHP scores and cost per caregiver based on FOS frequency.
4. Discussion
To our knowledge, the current study was the largest multinational to date measuring the QoL of caregivers of adults with uncontrolled drug-resistant FOS which was conducted in real-world populations in the UK, Germany, France, Italy, Spain, and Sweden (n = 345). Our study captured the impact of providing informal care on the caregivers’ HRQoL and measured the costs of lost productivity associated with caregiving for this patient population.
This study found that caregivers of adults with uncontrolled drug-resistant FOS had a reduced QoL, as suggested by their EQ-5D-5L and CarerQol-7D utility scores: 0.6 (SD: 0.27) and 72.61 (SD:18.71), respectively. However, most caregivers reported to derive fulfilment out of their caring role (88%) and felt that they had support with their caring responsibilities (72%).
In addition, both EQ-5D-5L and CarerQol-7D showed that mental health was the most affected aspect of the caregivers’ QoL. We note that 27% and 38% of caregivers reported no problems in mental health when completing the EQ-5D-5L and the CarerQol-7D, respectively. This implies that when answering the EQ-5D-5L questionnaire, 11% of caregivers considered they had anxiety/depression problems, but they reported not having any problems when answering the mental health question of the CarerQol-7D questionnaire. This finding suggests that the mental health dimensions of the EQ-5D-5L and CarerQol-7D instruments were not interpreted in the same manner by caregivers. This could be due to the fact that EQ-5D-5L asks specifically about anxiety/depression, whereas CarerQol-7D asks about mental health in general, including examples such as stress, concerns about the future, fear.
Additionally, our study indicated that caregiving for this patient population placed a significant burden on the caregivers’ work productivity. This was further translated to substantial costs of productivity losses incurred by employers. We estimated the mean annualised cost of lost productivity per caregiver at €14,872. There are approximately 600,000 people with epilepsy in the UKCitation27. FOS constitutes the most common seizure type, with over 60% of patients with epilepsy experiencing FOSCitation28. In addition, approximately 40% of people with epilepsy have DRE, deriving no benefit from two ASMCitation6. Considering these statistics, approximately 144,000 people in the UK experience uncontrolled drug-resistant FOS seizures. There are no robust estimates of how many people from this patient population require a caregiver in the UK. However, assuming that approximately 20% need support from a caregiver, the average annualised cost of productivity losses to the UK would be €428 million.
The multivariate regression analysis was intended to be exploratory to assess the direction and significance of potential background details, clinical data, or caregiver burden characteristics on the caregivers’ HRQoL. It is worth highlighting that few consistent patterns were seen, whereas high standard errors and p values were observed. This was likely due to variation between patients, and interactions between some of the variables, but the sample size was not large enough to formally test for interactions. However, we found that there was a statistically significant negative association between the caregivers’ EQ-5D-5L utility scores and the frequency of disabling seizures experienced by the individuals cared for. We mention that seizures of disabling nature are more severe than FOS, and have a significant negative effect on the individuals’ HRQoLCitation29. These findings suggests that a poor QoL of the individual cared for has a detrimental impact on the caregivers’ QoL. In addition, it is worth noting that there might be other factors that negatively affect caregivers’ QoL, including caregivers’ health issues. This suggestion is based on the finding that 40% of caregivers reported moderate, severe or extremely severe pain when completing the EQ-5D, while 60% of caregivers reported some or a lot of problems in their physical health when completing the CarerQol-7D. However, we did not collect data on whether caregivers suffered from chronic conditions, and thus we were not able to include this covariate in the regression analysis and evaluate its impact on the caregivers’ quality of life.
The literature on caregiver burden from epilepsy and its associated effect on caregivers’ HRQoL is limited. Most studies have mainly focused on the paediatric population. Hussain et al.Citation30 assessed the health and caregiver burden of caregivers of patients with epilepsy in the US using an online survey. They also estimated the economic costs to the US using the WPAI. The study found that many caregivers had mental health problems, with 47.85% and 38.65% of caregivers reporting anxiety and depression, respectively. This is consistent with our results. In addition, similarly to our findings, the authors also showed that work productivity losses were higher for the caregivers of individuals with higher seizure frequency. Moreover, the economic burden to the US was found to be substantial. Another study by Lai et alCitation31 studied the factors associated with caregiver burden in those caring for patients with epilepsy in Asia. The authors found that caregiver burden has a negative impact on the caregivers’ mental well-being, as shown by caregivers reporting high scores of depression, anxiety, stress and overall poor quality of life. The study also showed that the frequency of seizures experienced by the care receiver was positively associated with caregiver burden. Van Andel et al.Citation32 investigated the HRQoL of caregivers who provide informal care to adults with partial epilepsy in the Netherlands. The caregivers completed the EQ-5D and the RAND-36. The EQ-5D utility score and EQ-VAS reported by caregivers were 0.88 (0.17) and 81, respectively. These health-related utilities are substantially higher than the utility values obtained in our study (EQ-5D utility: 0.6 and EQ-VAS: 61). In addition, the authors found that the mental health score obtained from the RAND-36 questionnaire was significantly reduced, which is consistent with our findings. A potential rationale for the differences in EQ-5D utilities between our study and the study of Van Andel et al.Citation32 consists in the fact that the caregivers from our study had a greater caregiver burden and provided care for individuals with more severe clinical characteristics.
We note some strengths of the study. One strength consisted in using two different HRQoL instruments for measuring caregivers’ HRQoL. Both instruments indicated that caregivers reported the greatest problems in their mental health, which further strengthened this finding. A further strength was the inclusion of the validated economic burden measure (WPAI:SHP) that assesses the caregiving impact on productivity. This provided employers and policy experts an estimate of lost productivity costs incurred by employers.
We acknowledge some limitations of the study. One weakness was the use of an online survey instead of a face-to-face interviewCitation33–36. In the absence of an interviewer, participants may not engage or understand the questions properly and thus, may give inaccurate responses. However, we phrased the questions as simply as possible and offered examples to minimise any uncertainty in the results. Clear definitions of the medical terms, which used plain language and were reviewed by a clinician, were also included in the survey to help participants understand the questions and give accurate responses. Another limitation is that the respondents self-reported that they are caregivers providing informal care for an adult with a clinical diagnosis of FOS and with the corresponding clinical data. Efforts were made to mitigate this weakness by recruiting through an experienced and highly reputable caregiver panel. In addition, screener questions were used to exclude individuals who did not meet the eligibility criteria. However, this limitation is commonly seen in other similar studiesCitation16.
Further research of the HRQoL of caregivers of people with uncontrolled drug-resistant FOS would be beneficial to strengthen our findings. In addition, further work could include measuring caregivers’ HRQoL using the CarerQol-7D along with other HRQoL measures which provides utilities accepted by HTA bodies, such as the SF-36. Other caregiver burden or background characteristics, such as the relationship between the caregiver and the individual cared for or the caregivers’ chronic conditions, should also be collected in the survey as these could have an impact on the caregivers’ HRQoL.
5. Conclusion
Caring for an adult with uncontrolled drug-resistant FOS negatively impacted caregivers’ HRQoL, with mental health being affected the most. However, caregivers derived fulfilment out of their caring tasks and felt supported with their caring responsibilities. In addition, the costs of productivity losses associated with caregiving for this patient population were substantial as demonstrated by a mean percent overall work impairment due to caregiving of 63%. The mean annualised costs of productivity losses per caregiver were estimated at €14,872. The findings of this study can be incorporated into future economic models and HTA submissions.
Transparency
Declaration of funding
This study was sponsored by Arvelle Therapeutics, a company of Angelini Pharma. SK Pharmaceuticals is the licensor of cenobamate. PHMR received financial support for conducting this study, including the development, administration, and data collection of the online survey, data analysis and preparation of the manuscript.
Declaration of financial/other interests
IAS, IF and LL are full-time employees of PHMR. NS, JM, EDO’F and SJ are former employees of Arvelle Therapeutics GmbH. FP is a full-time employee of Angelini Pharma. Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Author contributions
IAS: Led the analysis and drafting of the manuscript, contributed to the study design and interpretation. IF: Contributed to the study design, analysis, interpretation, and drafting of the manuscript. NS: Contributed to the study design, analysis, interpretation, and drafting of the manuscript. FP: Contributed to the study design, analysis, interpretation, and drafting of the manuscript. JM: Contributed to the study design, analysis, interpretation, and drafting of the manuscript. EDO’F: Contributed to the study design, analysis, interpretation, and drafting of the manuscript. LL: Led the study design, contributed to the analysis, interpretation, and drafting of the manuscript. Oversight of the project.
Acknowledgements
No assistance in the preparation of this article is to be declared.
References
- Organisation WH. Epilepsy fact sheet. New York World Health Organization; 2018. Available from: http://www.who.int/mediacentre/factsheets/fs999/en/
- Scharfman HE. The neurobiology of epilepsy. Curr Neurol Neurosci Rep. 2007;7(4):348–354.
- Fisher RS. The new classification of seizures by the international league against epilepsy 2017. Curr Neurol Neurosci Rep. 2017;17(6):48.
- Nevitt SJ, Sudell M, Weston J, et al. Antiepileptic drug monotherapy for epilepsy: a network Meta‐analysis of individual participant data. Cochrane Database Syst Rev. 2017;6:CD011412.
- Boon P, Ferrao Santos S, Jansen AC, et al. Recommendations for the treatment of epilepsy in adult and pediatric patients in Belgium: 2020 update. Acta Neurol Belg. 2021;121(1):241–257.
- Chen Z, Brodie MJ, Liew D, et al. Treatment outcomes in patients with newly diagnosed epilepsy treated with established and new antiepileptic drugs: a 30-year longitudinal cohort study. JAMA Neurol. 2018;75(3):279–286.
- Schiller Y. Seizure relapse and development of drug resistance following long-term seizure remission. Arch Neurol. 2009;66(10):1233–1239.
- Kwan P, et al. Definition of drug resistant epilepsy: consensus proposal by the ad hoc task force of the ILAE commission on therapeutic strategies; 2010. Wiley Online Library.
- Laxer KD, Trinka E, Hirsch LJ, et al. The consequences of refractory epilepsy and its treatment. Epilepsy Behav. 2014;37:59–70.
- Jansen C, Francomme L, Vignal J-P, et al. Interictal psychiatric comorbidities of drug-resistant focal epilepsy: prevalence and influence of the localization of the epilepsy. Epilepsy Behav. 2019;94:288–296.
- Jacoby A, Snape D, Baker GA. Epilepsy and social identity: the stigma of a chronic neurological disorder. Lancet Neurol. 2005;4(3):171–178.
- Jacoby A, Baker G. Quality of life issues in intractable focal epilepsy. In: Intractable focal epilepsy. London: WB Saunders; 2000. p. 419–436.
- W.H.O. The Global Burden of Disease: 2004 Update. Available at: http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf; 2018.
- Society E. Caring for someone with epilepsy; 2019. Available from: https://wwwepilepsysocietyorguk/caring-someone-epilepsy.
- Brouwer WBF, van Exel NJA, van den Berg B, et al. Process utility from providing informal care: the benefit of caring. Health Policy. 2005;74(1):85–99.
- Kanters TA, Brugts JJ, Manintveld OC, et al. Burden of providing informal care for patients with atrial fibrillation. Value Health. 2021;24(2):236–243.
- NICE, Guide to the methods of technology appraisal; 2013. Available from: https://wwwniceorguk/process/pmg9/chapter/the-reference-case#measuring-and-valuing-health-effects.
- Al-Janabi H, Nicholls J, Oyebode J. The need to “carer proof” healthcare decisions. 2016. British Medical Journal Publishing Group.
- Devlin NJ, Brooks R. EQ-5D and the EuroQol group: past, present and future. Appl Health Econ Health Policy. 2017;15(2):127–137.
- Hoefman RJ, van Exel NJA, Foets M, et al. Sustained informal care: the feasibility, construct validity and test-retest reliability of the CarerQol-instrument to measure the impact of informal care in long-term care. Aging Ment Health. 2011;15(8):1018–1027.
- Brouwer WBF, van Exel NJA, van Gorp B, et al. The CarerQol instrument: a new instrument to measure care-related quality of life of informal caregivers for use in economic evaluations. Qual Life Res. 2006;15(6):1005–1021.
- Reilly MC, Gooch KL, Wong RL, et al. Validity, reliability and responsiveness of the work productivity and activity impairment questionnaire in ankylosing spondylitis. Rheumatology. 2010;49(4):812–819.
- Hoefman RJ, van Exel J, Brouwer WB. Measuring care-related quality of life of caregivers for use in economic evaluations: CarerQol tariffs for Australia, Germany, Sweden, UK, and US. Pharmacoeconomics. 2017;35(4):469–478.
- Szende A, Janssen B, Cabases J. Self-reported population health: an international perspective based on EQ-5D. 2014. Springer Nature.
- Van den Hout W. The value of productivity: human-capital versus friction-cost method. Ann Rheumatic Dis. 2010;69(Suppl 1):i89–i91.
- Explained ES. Wages and labour costs; 2019. Available from: https://ec.europa.eu/eurostat/statistics-explained/index.php/Wages_and_labour_costs#Net_earnings_and_tax_burden
- Action E. Epilepsy facts and terminology; 2018. Available from: https://www.epilepsy.org.uk/press/facts
- Schmitz B, Montouris G, Schäuble B, et al. Assessing the unmet treatment need in partial-onset epilepsy: looking beyond seizure control. Epilepsia. 2010;51(11):2231–2240.
- Harden CL, Maroof DA, Nikolov B, et al. The effect of seizure severity on quality of life in epilepsy. Epilepsy Behav. 2007;11(2):208–211.
- Hussain SA, Ortendahl JD, Bentley TGK, et al. The economic burden of caregiving in epilepsy: an estimate based on a survey of US caregivers. Epilepsia. 2020;61(2):319–329.
- Lai S-T, Tan W-Y, Wo MC-M, et al. Burden in caregivers of adults with epilepsy in Asian families. Seizure. 2019;71:132–139.
- Andel J, Westerhuis W, Zijlmans M, et al. Coping style and health-related quality of life in caregivers of epilepsy patients. J Neurol. 2011;258(10):1788–1794.
- Jiang R, Shaw J, Mühlbacher A, et al. Comparison of online and face-to-face valuation of the EQ-5D-5L using composite time trade-off. Qual Life Res. 2021;30(5):1433–1444.
- Rowen D, Brazier J, Keetharuth A, et al. Comparison of modes of administration and alternative formats for eliciting societal preferences for burden of illness. Appl Health Econ Health Policy. 2016;14(1):89–104.
- Norman R, King MT, Clarke D, et al. Does mode of administration matter? Comparison of online and face-to-face administration of a time trade-off task. Qual Life Res. 2010;19(4):499–508.
- Dillman DA. Why choice of survey mode makes a difference. Public Health Rep. 2006;121(1):11–13.