
Abstract
Objectives
This study aimed to analyze the impact of glaucoma in ambulatory centers and hospitals in Spain over the past decade, in terms of incidence and medical costs.
Methods
Administrative data of glaucoma patients from ambulatory centers and hospitals in Spain and registered between 2011 and 2020 was obtained from a Spanish National discharge database. Medical costs obtained were based on the diagnosis-related group-based hospital payment systems, determined by the Spanish Ministry of Health.
Results
Data from 100,734 ambulatory care visits and 11,408 hospital admissions related to glaucoma were obtained from the database. Most of the cases were registered in patients over 65 years of age. The incidence of glaucoma in ambulatory centers was 2.2 per 10,000 persons over the study period; in hospitals, the incidence was 0.2 per 10,000 persons. The incidence of glaucoma in ambulatory settings increased significantly over the study period, while the incidence in hospitals decreased over the same period. Most ambulatory visits and hospital admissions were programmed or non-urgent. The mean cost per ambulatory visit was €954, €5.5 million in total annually; the mean cost per hospital admission was €3,727, €4.1 million in total annually. The annual cost of ambulatory care increased significantly over the study period, while the annual cost of hospital care decreased significantly.
Conclusions
The medical costs of glaucoma in Spanish hospitals decreased over the study period, while the costs of ambulatory care increased. This shift in the management of glaucoma should be considered in future resource allocation decisions.
Introduction
Glaucoma is the main cause of irreversible blindness globallyCitation1. Glaucoma comprises a group of disorders characterized by progressive degeneration of the optic nerve, with risk factors that comprise age, elevated intraocular pressure, non-white ethnicity and geneticsCitation2,Citation3. Preserving the patients’ quality of life is crucial in the management of glaucoma. Current guidelines include recommendations for initial testing, patient monitoring and methods to decrease intraocular pressure. For instance, the European Glaucoma Society recommends prostaglandin analogues, selective laser trabeculoplasty and trabeculectomy as initial treatments in patients with mild or moderate open angle glaucomaCitation2. In addition, certain patients may require an alternative approach, such as glaucoma drainage implant surgery, a frequent procedure to place an artificial filtering device to lower intraocular pressureCitation4,Citation5. Hence, the care of patients with glaucoma requires a combination of ambulatory surgery and follow-up and hospitalization for surgical treatmentCitation2,Citation6.
In 2013, the estimated prevalence of glaucoma in Europe among people aged 40–80 years was 2.9%, and long-term projections suggest that the number of people (aged 40–80 years) with glaucoma worldwide will increase over the next decadeCitation7. Few data is available describing the epidemiology of glaucoma in Spain and the associated medical costs have not been evaluated at the national level. One study from a private Spanish hospital, centered on the hospital management of glaucoma, estimated a mean cost of €2,502 (US$2,746) per patient with primary open-angle glaucoma between 2010 and 2013Citation8. This study and many others demonstrate the association between disease severity and costs, however, ambulatory data in Spain is limitedCitation8,Citation9. To update disease incidence and cost evaluations is crucial to develop accurate cost-effectiveness evaluations of glaucoma screening and care, and to design related public health strategies. Consequently, the objective of this study was to analyze the impact of glaucoma in ambulatory centers and hospitals in Spain over the past decade, in terms of incidence and medical costs.
Methods
Study design
A retrospective database study was set to evaluate the burden of glaucoma in Spain from a payer perspective. With this aim, administrative data corresponding to ambulatory visits and inpatient hospital admissions was analyzed, and obtained from a Spanish National discharge database. This database covers 90% of hospitals in Spain and includes data from all Spanish regions. Data is codified at the hospital level using the International Statistical Classification of Diseases and Related Health Problems, the 9th version (ICD-9) before 2016 and the 10th version (ICD-10) after the year 2016Citation10,Citation11. The Spanish Ministry of Health is responsible for data validation and elimination of errors and unreliable data.
Data extraction
The ICD-9 and ICD-10 codes corresponding to glaucoma (365 and H40) were used to claim records of ambulatory and hospital admissions in which glaucoma was registered as the admission motive (primary diagnosis). The inclusion period was from 1 January 2011 to 31 December 2020. There were no parameters identifying healthcare centers or medical history, all files were previously re-coded to maintain anonymity in accordance with the principles of Good Clinical Practice and the Declaration of Helsinki. No human participants were involved and there was no access to identifying information; in this context, patient consent and ethics committee approval are not requiredCitation12.
Study variables
The parameters obtained for hospital admissions included: patients’ age, date of admission, type of admission, date of discharge, type of discharge, primary diagnosis, up to 20 secondary diagnoses registered during the admission, medical procedures and cost. For ambulatory visits data obtained included: age groups, date of admission, type of admission, primary diagnosis and cost.
Data analysis
Patients diagnosed with glaucoma were identified by the primary diagnosis code. Patients’ were classified by sex and into four age groups. The first admission registered per patient was used to evaluate patient characteristics, whereas all files were used to analyze admission details and medical costs. Incidence was calculated as the admission/hospitalization rate based on the admissions registered in the database. This corresponded to the number of patients with glaucoma registered in Spanish ambulatory centers per population assigned, and the number of patients with glaucoma registered in Spanish hospitals per population assigned.
Direct medical costs were obtained from the database, where they are assigned according to the standardized average expenses of admissions and medical procedures determined by the Spanish Ministry of Health. These costs comprise all expenses related to the admission: medical examination and procedures, medication, surgery, diet, costs associated with personnel, medical equipment and resources. Costs were adjusted for inflation to 2020 values.
The Kolmogorov-Smirnov test was used to test for normality. Frequencies and percentages are presented for dichotomous variables and mean or median were calculated for continuous variables. Two-tailed non-parametric independent t-test (Mann-Whitney U test) or one-way analysis of variance (Kruskal-Wallis test) were used as appropriate and two-sample Z tests were used to test for differences in sample proportions. The Jonckheere–Terpstra trend test was used to assess trends in incidence and cost. A p < .05 was considered statistically significant.
Microsoft Excel© Professional Plus 2016 (Microsoft Corporation, Redmond, WA, USA) and StataSE 12 for Windows (StataCorp LP. 2011. Stata Statistical Software: Release 12. College Station, TX, USA) were used to perform statistical analyses.
Results
Over the study period, 100,734 ambulatory care visits were registered due to glaucoma (). During the same period, 11,408 hospital admissions were registered due to glaucoma. In both settings, most of the cases were registered in patients over 65 years of age, and there were significantly more males than females (p < .0001). The most frequent comorbid conditions registered in hospital centers were essential hypertension (21%), cataract (19%), diabetes mellitus (16%) and hyperlipidemia (11%).
Table 1. The number of ambulatory visits and hospital admissions registered between 2011 and 2020 by sex and age.
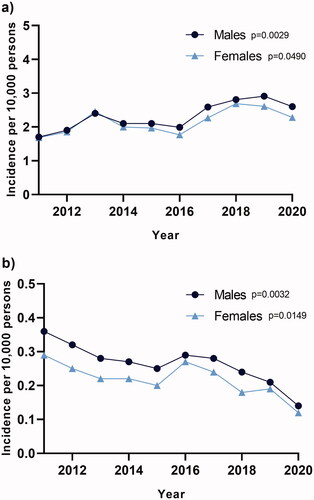
The incidence of glaucoma in ambulatory settings was 2.2 per 10,000 persons between 2011 and 2020; in hospitals, incidence was 0.2 per 10,000 persons. The incidence of glaucoma in ambulatory settings increased significantly over the study period (p = .0029 in males, p = .0490 in females), while the incidence in hospitals decreased over the same time period (p = .0032 in males, p = .0149 in females) ().
Figure 1. Incidence (admission/hospitalization rate) of glaucoma measured in ambulatory settings (a) and hospitals (b) per year in Spain. The Jonckheere–Terpstra trend test was used to assess temporal trends.
Most of the ambulatory visits (99%) were registered in ophthalmology departments and were programmed or non-urgent (96%). Most of the hospital admissions (96%) were registered in ophthalmology departments and were programmed or non-urgent (76%). The median length of hospital stay was 2 days, with no significant differences between males and females or by age (). The most frequent medical procedures registered at the hospital level were associated with surgical drainage procedures, while cataract-related surgeries were also registered.
Table 2. Characteristics of hospital admissions.
The mean cost per ambulatory visit was €954 over the study period, whereas the mean cost per hospital admission was €3,727 (). No significant differences were observed in the cost of ambulatory or hospital admissions by sex or age.
Table 3. Mean medical costs of ambulatory care and hospitalization by sex and age group.
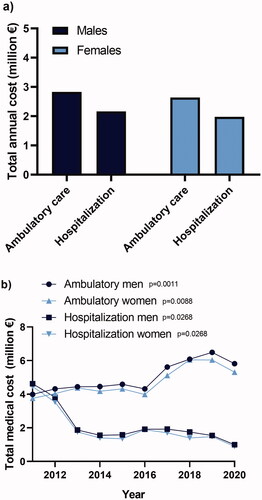
Ambulatory visits represented a total annual cost of €5.5 million, €2.8 for males and €2.6 for females (). The total annual cost of hospital care was €4.1 million, €2.2 for males and €2.0 for females. Similarly to what was observed in incidence rates, the annual cost of ambulatory care increased significantly over the study period (p = .0011 in males, p = .0088 in females), while the annual cost of hospital care decreased significantly (p = .0268 in males, p = .0268 in females) ().
Figure 2. Mean annual direct medical cost (a) and medical cost per year (b). Costs included medical examination and procedures, medication, surgery, diet, costs associated with personnel, medical equipment and resources; the Jonckheere–Terpstra trend test was used to assess temporal trends.
Discussion
Glaucoma is a chronic condition that can be associated with significant healthcare costs as the disease advancesCitation9. This study aimed to evaluate the incidence and costs of glaucoma in Spain both in ambulatory and hospital settings. The majority of patients included in the study were men over 45 years of age. Incidence in ambulatory settings was 2.2 per 10,000 persons, increasing significantly over the past decade, whereas the incidence registered in hospital settings was 0.2 per 10,000 persons, decreasing significantly during the same time period. Glaucoma requires multi-dimensional treatment, integrating pharmacological and surgical interventionsCitation2,Citation13. Data evaluated herein suggests a shift in disease management over the past decade. Further studies will be required to evaluate drug prescriptions and procedures that did not require hospitalization, not registered in this database. In hospital settings, the registered admissions were principally associated with invasive surgical procedures aimed at relieving elevated intraocular pressure, with a median length of stay of 2 days. In addition, a number of patients received cataract-related surgeries, which could be associated with a previous glaucoma surgeryCitation14.
In terms of medical costs, the mean cost per ambulatory visit in this study was €954, while the mean cost per hospital admission was €3,727. In this context, it could be argued that favoring outpatient/ambulatory procedures versus overnight surgical care could contribute to reducing the total burden of glaucoma; one option to advance in this direction would be the elimination of payments to hospitals for overnight glaucoma surgical care. Nevertheless, the lack of disease severity data in this study limits results in interpretation in this aspect. Additionally, another factor that could contribute to reducing the burden of glaucoma would be diminishing the costs linked to systemic comorbid conditions, such as hypertension, diabetes and hyperlipidemia.
The annual cost of glaucoma in this study summed at €9.6 million when considering ambulatory and hospital care. Earlier evaluations in the United States and several European countries estimated a cost per patient of €455–568 per year in the early stages of glaucoma, and €969–2,290 in end-stages, suggesting that an earlier diagnosis and treatment of glaucoma can reduce the burden of this disorder, however, evidence in this direction is limitedCitation15,Citation16. Overall, the cost-effectiveness of glaucoma screening has been repeatedly evaluated. Although screening for glaucoma was cost-effective in rural and urban Chinese regions in a 2019 study, a systematic meta-analysis deemed population screening not cost-effectiveCitation17,Citation18. Further studies will be required, with the introduction of new treatment options, to evaluate the cost-effectiveness of glaucoma screening and management.
Several limitations may have influenced the results of this study. Disease severity was not registered and prescription medication could not be evaluated. Similarly, ambulatory medical procedures were not registered in the database limiting the analysis of disease management. These restrictions hampered the analysis of cost drivers; however, mean and total costs were calculated independently, which ensures the reliability of economic data.
Conclusions
The medical costs of glaucoma registered in Spanish hospitals decreased over the study period, while the portion of costs associated with ambulatory care increased, reflecting a shift in the management of this disorder. The introduction of new therapeutic methodologies, favoring ambulatory care, should be considered in future resource allocation decisions.
Transparency
Declaration of funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of financial and other interest
The authors declare that they have no competing interests.
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Author contributions
JD contributed to the investigation by analyzing and interpreting the burden associated to glaucoma in Spain and was a major contribution in the intellectual content revision. AM analyzed the current situation of glaucoma in Spain, interpreted the statistical data and was a major contributor in writing the manuscript. All authors read and approved the final manuscript.
Data availability statement
Data sharing is restricted due to legal stipulations, yet the data that support the findings of this study is fully available from the Spanish Ministry of Health via the Unit of Health Care Information and Statistics (Spanish Institute of Health Information) for researchers who meet the criteria for access to confidential data at: https://www.mscbs.gob.es/estadEstudios/sanidadDatos/home.htm.
Ethics approval and consent to participate
Ethics committee approval and consent were not required for this study.
References
- Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990-2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221–e1234.
- European glaucoma society terminology and guidelines for glaucoma, 5th edition. Br J Ophthalmol. 2021;105(Suppl 1):769–169.
- Kang JM, Tanna AP. Glaucoma. Med Clin North Am. 2021;105(3):493–510.
- Aref AA, Gedde SJ, Budenz DL. Glaucoma drainage implant surgery. Dev Ophthalmol. 2017;59:43–52.
- Cohen LP, Pasquale LR. Clinical characteristics and current treatment of glaucoma. Cold Spring Harb Perspect Med. 2014;4(6):a017236–a017236.
- Kastner A, King AJ. Advanced glaucoma at diagnosis: current perspectives. Eye. 2020;34(1):116–128.
- Tham YC, Li X, Wong TY, et al. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090.
- Real JP, Lafuente MC, Palma SD, et al. Direct costs of glaucoma: relationship between cost and severity of the disease. Chronic Illn. 2020;16(4):266–274.
- Fiscella RG, Lee J, Davis EJ, et al. Cost of illness of glaucoma: a critical and systematic review. Pharmacoeconomics. 2009;27(3):189–198.
- Centers for Disease Control and Prevention (CDC). International classification of diseases, ninth revision, clinical modification (ICD-9-CM). CDC; 2015. [cited 2022 Feb 22]. https://www.cdc.gov/nchs/icd/icd9cm.htm.
- Centers for Disease Control and Prevention (CDC). International classification of diseases, tenth revision, clinical modification (ICD-10-CM). CDC; 2020. [cited 2022 Feb 22]. https://www.cdc.gov/nchs/icd/icd10cm.htm.
- Parliament of Spain. Law 14/2007, 3rd July, on biomedical research (BOE, 4 July 2007). Rev Derecho Genoma Hum. 2007;26:283–325.
- Schuster AK, Erb C, Hoffmann EM, et al. The diagnosis and treatment of glaucoma. Dtsch Arztebl Int. 2020;117(13):225–234.
- Patel HY, Danesh-Meyer HV. Incidence and management of cataract after glaucoma surgery. Curr Opin Ophthalmol. 2013;24(1):15–20.
- Lee PP, Walt JG, Doyle JJ, et al. A multicenter, retrospective pilot study of resource use and costs associated with severity of disease in glaucoma. Arch Ophthalmol. 2006;124(1):12–19.
- Traverso CE, Walt JG, Kelly SP, et al. Direct costs of glaucoma and severity of the disease: a multinational long term study of resource utilisation in Europe. Br J Ophthalmol. 2005;89(10):1245–1249.
- Tang J, Liang Y, O'Neill C, et al. Cost-effectiveness and cost-utility of population-based glaucoma screening in China: a decision-analytic Markov Model. Lancet Glob Health. 2019;7(7):e968–e978.
- Burr JM, Mowatt G, Hernández R, et al. The clinical effectiveness and cost-effectiveness of screening for open angle glaucoma: a systematic review and economic evaluation. Health Technol Assess. 2007;11(41):iii–iiv.