
Abstract
Aim
Peristomal skin complications (PSCs) and leakages are major issues for people living with a stoma. The purpose of this study is to understand how these stoma-linked complications impact health-related quality of life (HRQoL) in a UK population.
Materials and methods
The study used time trade-off (TTO) methodology to quantify health state utilities associated with two stoma-related complications: PSC and leakages. Respondents assessed 10 different health states with different PSC severity levels (no, mild, moderate or severe PSC) and frequencies of leakage events (2, 12 or 48 leakages onto clothes per year, and no leakage due to a digital solution). The average disutility value for each health state was also assessed. The study was conducted via a web-based survey in the UK adult general population.
Results and limitations
The analysis included 758 respondents. Respondents considered living with a stoma with no PSC to be more favorable than the other health states. Severe pain, itching and/or burning (PIB) was associated with the largest disutility compared to no PSC. The disutility (0–1 scale) compared to no PSC was 0.287 (p < .0001), 0.106 (p < .0001) and 0.025 (p=.0005) for PIB scores of 8, 5 and 2, respectively, on a 1–10 scale. More frequent leakage events were associated with lower utility. The utility decreases compared to no PSC were 0.114 (p < .0001), 0.057 (p < .0001) and 0.022 (p < .0001) for 48, 12 and 2 leakage events per year, respectively. The health state with a digital notification solution that notifies the user before a leakage event happens was considered as good as no PSC.
Conclusions
Experiencing mild, moderate, and severe levels of PSC or leakage onto clothes is associated with a significant reduction in HRQoL compared to no PSC and/or no leakage. Stoma appliances that reduce the skin complications or keep leakage from reaching the clothes are likely to improve HRQoL.
Introduction
In the UK, more than 170,000 people (or approximately one in every 500) live with a stoma, and an estimated 13,500-plus people each year experience a stoma surgeryCitation1. Stoma is a surgically created diversion, either permanent or temporary, of feces or urine through an opening in the abdominal wall and into an ostomy bagCitation2. Although there are different types of stomas, most people living with a stoma have either a colostomy (opening from the colon), an ileostomy (opening from the ileum) or a urostomy (diversion of urine from the bladder)Citation3.
A stoma surgery can be a life-saving procedureCitation4–6, but having a stoma negatively influences – socially, mentally and physically – the everyday life of the person living with itCitation7–10. Physical complications include skin excoriation, parastomal hernia, retraction, necrosis, infection, prolapse, stenosis, fistula, small bowel obstruction, appliance leakage, stomal bleeding and high outputCitation1,Citation2,Citation11. Social and psychological complications include stigma as well as reduced social life and social life satisfaction, primarily due to the risk of gas emission or leakage from the stomaCitation12,Citation13. “Leakage,” a broad term that covers several different types of events, is commonly used to describe stoma effluent that reaches beyond the baseplate (leading to, e.g. the soiling of clothes or bedsheets) or spreads underneath the baseplateCitation14.
Leakage and fear of leakage are major concerns for people living with a stoma, and generate emotional impact, impact on usual and social activities, and impact on coping and control, especially when leakage happens in a public spaceCitation15. The social and emotional discomfort from leakage also seems to impact labor market participationCitation16. People living with a stoma report that they constantly worry about leakage (>90%), have problems sleeping (54%), stay at home (47%), avoid close physical contact with other people (36%) or even avoid people in general (33%)Citation16. Furthermore, 66% of people with a stoma experience some degree of impact on their ability to work because of leakage or worry about leakage from their stomaCitation16.
Although some studies have investigated the impact of leakage on people’s lives, the utility impact on health-related quality of life (HRQoL) remains uncertain, partly because no widely accepted standardized way of measuring leakages exists. A validated tool that indirectly quantifies the impact of leakage on stoma-related quality of life (QoL) does existCitation15, but there is also a need for a direct measurement of HRQoL. This study will contribute new knowledge, qualify and reinforce the findings of the indirect approach, and reveal how people think differently about what constitutes leakageCitation14.
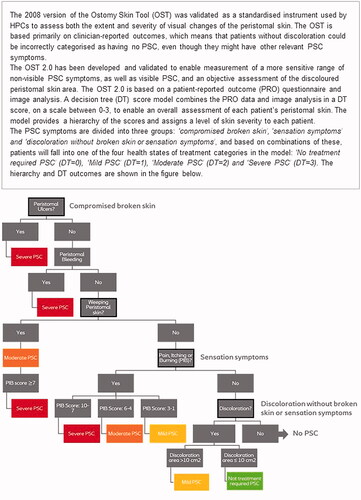
Leakage under the baseplate may cause irritant contact dermatitis, the most common reason behind peristomal skin complications (PSCs)Citation17,Citation18. The incidence of PSC is influenced by uncertainty; however, different investigations have estimated a rate of 18–88%Citation19. PSC can include visual signs (such as weeping or bleeding skin or ulcers) or nonvisual signs (such as pain, itching and/or burning sensations, or PIB)Citation19. A recently updated skin tool has been developed to capture a wider range of sensation symptoms and thereby assess the severity of PSC with more precision than previously. The new tool categorizes PSC as either no treatment required, mild, moderate or severe, based on the visual and nonvisual signs, including the experienced PIB sensations ()Citation16.
Figure 1. Ostomy Skin Tool 2.0. Source: The Ostomy Skin Tool 2.0: a new instrument for assessing peristomal skin changes, Martins et al.Citation16
A recent study shows that PSCs have a negative impact on QoL for most peopleCitation19. However, the most common tools for measuring HRQoL, such as EQ-5D-5L, may not be sufficient for capturing the impact of changes in PSC category or in the number of leakage events. Likewise, the general HRQoL metrics may create challenges in evaluating the discomfort related to worrying about events such as potential leakage from a stoma.
A study showed the minimally important difference (MID) of the EQ-5D-5L tool was between 0.037 and 0.069, indicating the tool’s suitability to capture only larger changes in utilityCitation20. The current study aims to estimate the disutility associated with different frequencies of leakage and different levels of PSC using the time trade-off (TTO) methodology, which is preferred for capturing small changes in utility.
Methods
Time trade-off methodology
The TTO method is used to calculate utility values ranging from 0 to 1 by asking respondents to “trade off” a part of their remaining lifespan to live in an improved health state. The TTO method is thoroughly described in the literatureCitation21–29.
Each respondent is presented with one health state at a time and a description of the key characteristics of this state. Respondents are repeatedly asked to choose between living in the presented health state for a lifetime, t, and alternatively living in full health for a shorter lifetime, x. For each repetition, the shorter lifetime, x, is varied until the point of indifference, x*, is found. The individual’s preference score for the specific health state, known as the utility, is then calculated based on the indifference point x* and the expected lifespan t, as x*/t. The time horizon used in the questionnaire was based on each respondent’s individual life expectancy, calculated from the most recent lifespan tables from the World Health OrganizationCitation30 and from the respondent’s age and gender.
Each respondent was presented with either a set of five leakage-related health states (1, 7–10) or a set of six PSC-related health states (1–6) (). The procedure of identifying the utility for each respondent for each health state followed a standard bisection methodology, using a utility of 0.6 as a starting point and then narrowing that measurement until an interval around the respondent’s point of indifference was reached. The distribution tails were given particular attention.
Definition of health states
Health states were defined based on a validated skin tool outlining different categories of PSC severityCitation16, current knowledge regarding patient experiences with leakage eventsCitation16, and workshop discussions with health economic and medical experts. Ten different health states, including a base case with no PSC and no leakage, were developed based on different levels of PSC and different frequencies of leakage onto clothes. The “no PSC” base case includes the “no treatment required” outcome in the skin tool. The five different PSC health states included mild PSC, two versions of moderate PSC and two versions of severe PSC. The four different leakage frequency health states include two leakages onto clothes per year, one leakage per month and four leakages per month, as well as no leakage due to a digital solution, integrated into the stoma bag, that warns the user to change the appliance before a leakage event happens (Figure S2).
Each health state was described based on the key characteristics of living with a stoma, the skin tool and patient experience with leakage. Figure S1 shows how the key characteristics of living with a stoma were described to the respondents. All health states were described as permanent situations that the respondents should imagine living with for their remaining lifespan ().
Table 1. Health states.
Questionnaire design
To familiarize respondents with the subject, the TTO method and the type of questions, all respondents were first presented with a health state scenario designed as a “warm-up” exercise. Afterwards, the respondents were randomized to either the PSC block (with six health states, including the base case) or the leakage block (with five health states, including the base case). shows an example: the leakage health state, in which the respondents experience leakage two times a year. The remaining health states were described in similar ways.
Figure 2. Example of TTO survey question.
Survey description
Data were collected via an internet-based survey, using an existing representative email panel of respondents from the general population who had previously agreed to participate in such surveys. The respondents were anonymous, and no sensitive information was revealed to the authors. Inclusion criteria were (1) consent to participate in the survey and (2) age above 17 years. The survey was conducted in the UK general population from April to May 2021. The respondents received remuneration (points corresponding to £1–£2) for participating in the survey.
The questionnaire was programmed in a commercial survey software package, SurveyXact (Aarhus N, Denmark). Its functionality was tested in a pilot study of 200 respondents. The survey was then completed among the general population, because health technology assessment (HTA) authorities such as the National Institute for Health and Care Excellence (NICE)Citation31 recommend using utilities generated by the general public for health economic evaluation. The survey was carried out within the codes of conduct of the Market Research Society and following the applicable ESOMAR guidelines.
Exclusion criteria
Respondents who chose to trade a very large proportion of their remaining lifespan or chose not to trade any lifetime at all were carefully screened. Respondents were excluded if they refused to trade on ethical or religious grounds, or if they stated that they did not understand the question. On the other hand, if respondents believed the health state was manageable or if they expressed a desire to live as long as possible due to obligations (such as being a caregiver), their answers were kept in the further analyses.
Statistical analysis
Data were analyzed with the statistical software SAS version 9.4 (Cary, NC). A utility value was calculated for each of the 10 health states based on the individual trade-offs. The utility value represents the midpoint of the chosen range of indifference. For example, a respondent who indicated an indifference point between 0.80 and 0.85 was assigned a utility value of 0.825. After calculating the individual utility for all respondents for all health states, the outliers (top and bottom 2.5%) were excluded, and the utility value for each individual health state and for differences between health states was estimated. The average disutility difference between two health states was calculated as the mean of their individual differences. An objective cut-off of 5% increased the stability of results that are otherwise sensitive to outliers. Nonparametric bootstrapping with 10,000 iterations was used to simulate standard errors and confidence intervals (CIs) for the mean TTO values, as the distribution of utility values was non-normal. This method estimates the parameter’s distribution by repeatedly resampling the original dataset with replacementsCitation32–35.
Results
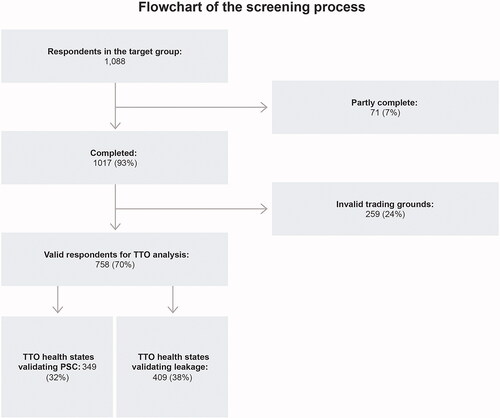
In all, 1,017 respondents (93% of the target population) from the UK general population completed the questionnaire between April and May 2021, with a mean completion time of 9.2 min. A total of 758 respondents (70%) with an average age of 45 years (female 52%, male 48%) were eligible for the final analysis, with 259 respondents (24%) excluded because they indicated individual reasons for trading too much or too little (such as religious or ethical reasons) or because they did not understand the questions. Furthermore, 71 (7%) did not complete the survey. Of the 758 respondents, 349 were presented with the PSC health states, and the remaining 409 were presented with the leakage health states. All respondents got the base case health state, as shown in the flowchart ().
Figure 3. Respondent flowchart.
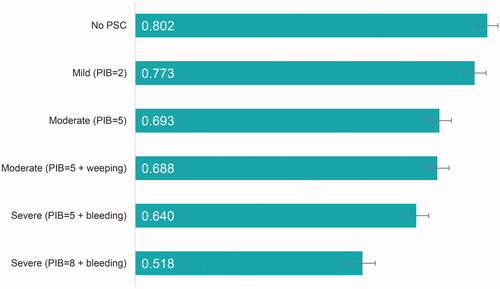
Respondents considered living with a stoma with no PSC and no weeping or bleeding skin to be more favorable than the remaining health states with higher levels of PIB sensations and some weeping or bleeding skin. On a 0–1 scale, the utility value was 0.802 (CI: 0.778–0.826) for no PSC, 0.773 (CI: 0.747–0.799) for mild PSC with PIB = 2, 0.693 (CI: 0.665–0.720) for moderate PSC with PIB = 5, 0.688 (CI: 0.661–0.715) for moderate PSC with PIB = 5 and weeping skin, 0.640 (CI: 0.611–0.669) for severe PSC with PIB = 5 and bleeding skin, and 0.518 (CI: 0.487–0.547) for severe PSC with PIB = 8 and bleeding skin ().
Figure 4. Utilities associated with different levels of PSC. Error bars show 95% CI.
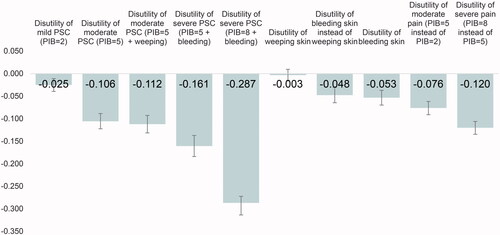
There is an increasing disutility for increasing severity of PSC and for bleeding skin compared to no PSC (). Severe PIB is associated with the largest utility decrease. Having a PIB of 8 (on a 1–10 scale) decreased the utility by 0.287 (p < .0001) compared to having no PSC and decreased the utility by 0.120 (p < .0001) compared to having a PIB of 5 (on a 1–10 scale). In comparison, experiencing an increase in PIB from 2 to 5 decreased the utility by 0.076 (p < .0001). Having severe PSC from bleeding skin and a PIB score of 5 decreased the utility by 0.161 (p < .0001) compared to experiencing no PSC, while the disutility of having moderate PSC with a PIB score of 5 with or without weeping skin was 0.112 (p < .0001) and 0.106 (p < .0001), respectively. The disutility associated with having mild PSC with a PIB score of 2 was 0.025 (p=.0005) compared to experiencing no PSC. There was a disutility of 0.053 (p < .0001) related to having bleeding skin compared to having skin with no weeping or bleeding. The utility associated with weeping skin alone was not significant (p=.2978).
Figure 5. Utility differences associated with different levels of PSC. Error bars show 95% CI.
Time trade-off results for leakage onto clothes
Respondents considered living with a stoma with no PSC to be more favorable than the health states with two to 48 leakage events per year. Respondents considered having no leakage events due to a digital notification solution to be as good as a health state without PSC.
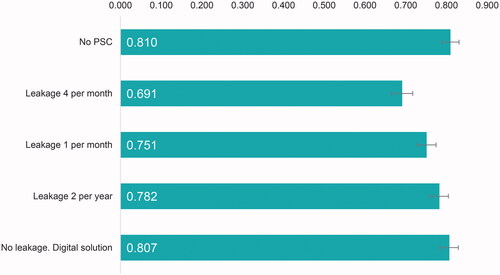
The utility value was 0.810 (CI: 0.788–0.831) for no PSC, 0.691 (CI: 0.666–0.717) for a health state with four leakage events per month, 0.751 (CI: 0.728–0.774) for one leakage event per month, 0.782 (CI: 0.759–0.805) for two leakage events per year, and 0.807 (CI: 0.784–0.829) for a health state with no leakage events due to a digital notification solution ().
Figure 6. Utilities associated with different frequencies of leakage. Error bars show 95% CI.
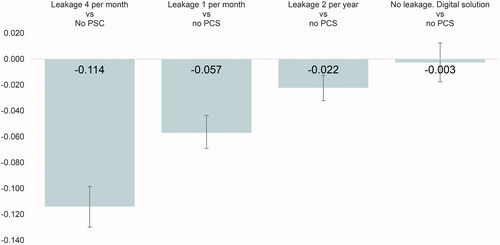
The health states with more frequent leakage events were associated with greater disutility. Experiencing four leakage events per month resulted in a disutility of 0.114 (p < .0001) compared to the health state without PSC, whereas one leakage event per month gave a disutility of 0.057 (p < .0001) and two per year led to a disutility of 0.022 (p < .0001). The health state with a digital notification solution was considered as good as a health state with no PSC ().
Figure 7. Leakage utility differences for health states with leakage compared to no PSC. Error bars show 95% CI.
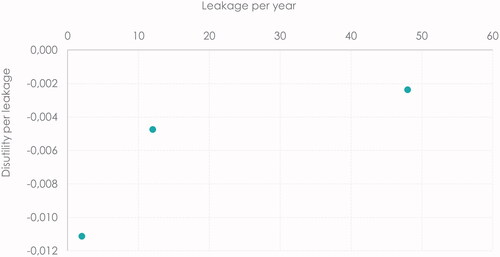
Each leakage event was associated with a smaller disutility of 0.002 if the respondents expected to experience 48 events per year, whereas the disutility per event was 0.011 when the respondents expected two events per year. The disutility per leakage event was 0.005 for one expected leakage event per month ().
Figure 8. Marginal disutility per leakage event, based on expected number of events.
Discussion
This study shows how some of the most common stoma complications impact patients’ QoL. The utility values for the health states range between 0.518 and 0.810 on a 0–1 scale. These findings are in line with other studies that have investigated the QoL of people with chronic conditions. The derived utility values for mild, moderate and severe PSC are similar to the utility values found for mild, moderate and severe levels of hand eczemaCitation36 as well as psoriatic arthritis and plaque psoriasisCitation37, and are within the range of several other chronic diseasesCitation38. Other studies have reported utility values for first recurrence after breast cancer and for disability after hip fracture that are similar to the leakage health states and the mild to moderate PSC levelsCitation39. Severe PSC health states are comparable to hospital kidney dialysis or severe congestive heart failureCitation39. The results for no leakage due to digital solution and for no treatment required for PSC or no PSC show that living in these health states is similar to the utility of people from the UK living with one long-term condition and is around 0.1 lower on a 0–1 scale than people with no long-term conditionsCitation40,Citation41.
The results presented here show that the respondents were willing to trade remaining life years to avoid stoma complications, which indicates that various levels of PSC and frequencies of leakage have a significant impact on HRQoL. The results further indicate the societal value of avoiding these stoma-related complications, which should be taken into account when evaluating stoma innovations.
Particularly, the study found a larger disutility related to experiencing PSC with severe levels (7–10 on a scale of 1–10) of PIB sensations compared to other PSC health states: a moderate level of PIB (4–6) is associated with a smaller disutility, and a mild PIB (1–3) has an even smaller disutility. The importance of PIB, which is a nonvisual sign of PSC, supports the dimensions of the updated skin tool 2.0, which now explicitly includes nonvisual signs of PSC, compared to the tool’s first version, which mainly included visual signs. Our findings therefore support the classification from the skin tool 2.0, where a PIB score of 7–10 is classified as severe PSC, a PIB of 4–6 indicates moderate PSC, and a PIB of 1–3 represents mild PSC.
Bleeding skin (a visual sign) also has a relatively large impact on HRQoL, which further supports the findings from the skin tool 2.0, which immediately classifies PSC with bleeding skin as severe PSC. Our findings also indicate that weeping skin (without pain) does not in itself lead to significant disutility. However, it can be argued that weeping skin does come with some level of PIB, which makes it very hard to distinguish one effect from the other.
The study also finds that leakage events have an impact on HRQoL: experiencing more frequent events is associated with a larger disutility, while a digital solution that notifies the user of an impending leakage can restore HRQoL to a level similar to that of a patient who has no PSC. This indicates that the uncertainty surrounding when a leakage could happen imposes a significant disutility.
Furthermore, the study shows that the more leakage events patients expect to experience per year, the smaller a disutility they tend to associate with each event. This points to a coping mechanism where the disutility of each event is perceived as smaller if the person is accustomed to the event happening. This tendency is in line with economic theoryCitation42 and reflects the fact that people adapt to the circumstances of their life. A similar tendency exists when people seem to value the same health state more after living with a condition for a while compared to when they were newly diagnosed.
In the study, we find a small (but not statistically significant) numerical difference in the evaluation of the “no PSC” health state between the PSC and leakage evaluation groups. This is acceptable and due to a variation in sample between the two groups.
The study excluded respondents who reported not understanding the questions or who refused to trade time on ethical or religious grounds, as well as the outliers (top and bottom 2.5%). In general, this approach does not impact the outcome since the results for the included and the full group are comparable.
The TTO method, a standard tool for health economic evaluation, may be used by HTA bodies to valuate different health states. This study shows that the TTO vignette method can be a useful alternative, as standard methods such as EQ-5D-5L are more suitable for measuring larger differences in HRQoL. The utilities derived from the study give a numeric value measured in quality-adjusted life-year (QALY) for a reduction in PSC or frequency of leakage and may be used as input parameters in future cost–utility analyses. When including impact on HRQoL in an evaluation of different stoma attributes, using a method that captures even small changes over time in a systematic and standardized manner is very important.
Limitations
Conducting an online TTO survey is associated with methodological strengths and limitations. A clear advantage of the approach is the larger sample sizes, and thus more robust results, compared to an interview-based approach. When recruiting online, it is also possible to secure a study population that is representative of the population of interest. However, the internet-based approach includes only internet users, which creates a potential bias if the internet users tend to value the different health states differently from internet nonusers. Nevertheless, since the study was conducted in the UK, which has a 98% internet penetration rateCitation43, this poses a minor challenge. Another limitation of the online survey is the lack of opportunities to further explain the content of a health state if the description does not fully reflect all disadvantages and benefits of the key characteristics. To limit this type of bias, the health states were based on the validated toolCitation16 and features were described objectively. All results should be interpreted with these limitations in mind.
This study uses utility values calculated from the views of the general population without personal experience with the condition in question, as this approach is recommended by most HTA authoritiesCitation31. Additionally, several studies find the utility differences for specific health states tend to be similar for the general population and a population of people who have experience with the investigated health states. Still, it would be valuable to compare these utilities with utility values based on views among people living with a stoma to further investigate the similarities and differences among these populations.
Conclusions
This study suggests that for a person living with a stoma, both experiencing mild, moderate and severe levels of PSC and experiencing leakage onto clothes are associated with a significant reduction in HRQoL compared to a situation with no PSC and/or no leakage.
Stoma appliances that reduce the skin complications or keep leakage from reaching the clothes are likely to improve HRQoL. The utility values from this study express the relative health benefits for the specific health states and could be used in a cost–utility analysis of different types of stoma appliances or stoma management options.
Transparency
Declaration of funding
This research was funded by Coloplast A/S, Humlebaek, Denmark.
Declaration of financial/other relationships
Authors JHB and LFJ were employed by Coloplast A/S during the study period and the preparation of this manuscript. NR was a member of the Coloplast Ostomy Forum Advisory board and has been compensated for her contribution according to fair market value. CY and MB are employed at Incentive Denmark, which is a paid vendor of Coloplast A/S, Denmark.
Author contributions
JHB and LFJ conceived the original idea that was discussed and further developed by all authors. CY and MB performed the data collection and statistical analysis. All authors contributed to the interpretation of results and critically reviewed and approved the final manuscript. All authors are accountable for all aspects of the work.
Reviewer disclosures
A reviewer on this manuscript has disclosed that they have received research, speaking and/or consulting support from Eli Lilly and Company, GlaxoSmithKline/Stiefel, AbbVie, Janssen, Alovtech, vTv Therapeutics, Bristol-Myers Squibb, Samsung, Pfizer, Boehringer Ingelheim, Amgen, Dermavant, Arcutis, Novartis, Novan, UCB, Helsinn, Sun Pharma, Almirall, Galderma, Leo Pharma, Mylan, Celgene, Ortho Dermatology, Menlo, Merck & Co, Qurient, Forte, Arena, Biocon, Accordant, Argenx, Sanofi, Regeneron, the National Biological Corporation, Caremark, Teladoc, Eurofins, Informa, UpToDate and the National Psoriasis Foundation. He is founder and part owner of Causa Research and holds stock in Sensal Health. The other peer reviewers on this manuscript have no other relevant financial relationships or otherwise to disclose.
Supplemental Material
Download MS Word (771.8 KB)Acknowledgements
The authors thank Brian Devin for his valuable input toward the accuracy of the health state descriptions and Professor John Brazier for his contribution to both the health state definitions and the interpretation of results.
References
- Kettle J. StoMap programme baseline report; 2019. p. 29. https://www.eoecph.nhs.uk/Files/Integrated%20Care/StoMap%20Baseline%20Report%20FINAL.pdf
- Pandiaraja J, Chakkarapani R, Arumugam S. A study on patterns, indications, and complications of an enteric stoma. J Family Med Prim Care. 2021;10(9):3277–3282.
- Perrin A. Exploring individuals’ perceptions of living with a stoma. Br J Nurs. 2019;28(16):S18–S22.
- Ananthan M, Gomathi V, Praveen P. Colostomy – a life saving procedure? Int J Adv Res. 2018;6(5):1007–1010.
- Bladder & Bowel UK. Are British public attitudes towards people with stomas improving? [Internet]; 2020 [cited 2022 Jan 6]. Available from: https://www.bbuk.org.uk/blog/are-british-public-attitudes-towards-people-with-stomas-improving/
- United Ostomy Associations of America. What is an ostomy? United Ostomy Associations of America [Internet]; 2022 [cited 2022 Jan 6]. Available from: https://www.ostomy.org/what-is-an-ostomy/
- Mols F, Lemmens V, Bosscha K, et al. Living with the physical and mental consequences of an ostomy: a study among 1–10-year rectal cancer survivors from the population-based PROFILES registry. Psychooncology. 2014;23(9):998–1004.
- Nichols TR. Quality of life in persons living with an ostomy assessed using the SF36v2: mental component summary: vitality, social function, role-emotional, and mental health. J Wound Ostomy Cont Nurs. 2016;43(6):616–622.
- Carlsson E, Fingren J, Hallén A-M, et al. The prevalence of ostomy-related complications 1 year after ostomy surgery: a prospective, descriptive, clinical study. Ostomy Wound Manage. 2016;62:34–48.
- Ayik C, Özden D, Cenan D. Ostomy complications, risk factors, and applied nursing care: a retrospective, descriptive study. Wound Manag Prev. 2020;66(9):20–30.
- Krishnamurty D, Blatnik J, Mutch M. Stoma complications. Clin Colon Rectal Surg. 2017;30(3):193–200.
- Abdalla MI, Sandler RS, Kappelman MD, et al. The impact of ostomy on quality of life and functional status of Crohn’s disease patients. Inflamm Bowel Dis. 2016;22(11):2658–2664.
- Dabirian A, Yaghmaei F, Rassouli M, et al. Quality of life in ostomy patients: a qualitative study. Patient Prefer Adherence. 2010;5:1–5.
- Down G, Vestergaard M, Ajslev TA, et al. Perception of leakage: data from the ostomy life study 2019. Br J Nurs. 2021;30(22):S4–S12.
- Nafees B, Størling ZM, Hindsberger C, et al. The ostomy leak impact tool: development and validation of a new patient-reported tool to measure the burden of leakage in ostomy device users. Health Qual Life Outcomes. 2018;16(1):231.
- Martins L, Down G, Andersen BD, et al. The ostomy skin tool 2.0: a new instrument for assessing peristomal skin changes. Br J Nurs. 2022;31(8).
- Herlufsen P, Olsen AG, Carlsen B, et al. Study of peristomal skin disorders in patients with permanent stomas. Br J Nurs. 2006;15(16):854–862.
- Martins L, Samai O, Fernández A, et al. Maintaining healthy skin around an ostomy: peristomal skin disorders and self-assessment. Gastrointest Nurs. 2011;9(Suppl. 2):9–13.
- Fellows J, Voegeli D, Håkan-Bloch J, et al. Multinational survey on living with an ostomy: prevalence and impact of peristomal skin complications. Br J Nurs. 2021;30(16):S22–S30.
- McClure NS, Sayah FA, Xie F, et al. Instrument-defined estimates of the minimally important difference for EQ-5D-5L index scores. Value Health. 2017;20(4):644–650.
- Dolan P, Gudex C, Kind P, et al. The time trade-off method: results from a general population study. Health Econ. 1996;5(2):141–154.
- Dolan P. Modeling valuations for EuroQol health states. Med Care. 1997;35:1095–1108.
- Dolan P. The measurement of individual utility and social welfare. J Health Econ. 1998;17(1):39–52.
- Dolan P. Aggregating health state valuations. J Health Serv Res Policy. 1997;2(3):160–165.
- Dolan P, Jones-Lee M. The time trade-off: a note on the effect of lifetime reallocation of consumption and discounting. J Health Econ. 1997;16(6):731–739.
- Torrance G. Preferences for health outcomes and cost–utility analysis. J Manag Care. 1997;3:8–20.
- Torrance GW, Furlong W, Feeny D. Health utility estimation. Expert Rev Pharmacoecon Outcomes Res. 2002;2(2):99–108.
- Robinson A, Dolan P, Williams A. Valuing health status using VAS and TTO: what lies behind the numbers? Soc Sci Med. 1997;45(8):1289–1297.
- Torrance GW, Feeny D. Utilities and quality-adjusted life years. Int J Technol Assess Health Care. 1989;5(4):559–575.
- WHO. Life tables for WHO member states; [Internet]; 2019. Available from: http://apps.who.int/gho/data/node.main.687?lang=en
- National Institute for Health and Care Excellence (NICE). Guide to the methods of technology appraisal 2013. Process and methods [Internet]; 2013 [cited 2021 Jul 8]. Available from: https://www.nice.org.uk/process/pmg9/resources/guide-to-the-methods-of-technology-appraisal-2013-pdf-2007975843781
- Atkinson SE, Wilson PW. Comparing mean efficiency and productivity scores from small samples: a bootstrap methodology. J Prod Anal. 1995;6(2):137–152.
- Efron B. Nonparametric estimates of standard error: the jackknife, the bootstrap and other methods. Biometrika. 1981;68(3):589–599.
- Briggs AH, Wonderling DE, Mooney CZ. Pulling cost-effectiveness up by its bootstraps: a non-parametric approach to confidence interval estimation. Health Econ. 1997;6(4):327–340.
- Chang W, Collins E, Kerrigan C. An internet-based utility assessment of breast hypertrophy. Plast Reconstr Surg. 2001;108(2):370–377.
- National Institute for Health and Care Excellence. Single technology appraisal (STA): specification for manufacturer/sponsor submission of evidence. NICE [Internet]. NICE; 2012. Available from: https://www.nice.org.uk/media/default/about/what-we-do/nice-guidance/nice-technology-appraisals/specification-formanufacturer-sponsor-submission-of-evidence-june-2012.doc
- Yang Y, Brazier J, Longworth L. EQ-5D in skin conditions: an assessment of validity and responsiveness. Eur J Health Econ. 2015;16(9):927–939.
- Capucci S, Hahn-Pedersen J, Vilsbøll A, et al. Impact of atopic dermatitis and chronic hand eczema on quality of life compared with other chronic diseases. Dermatitis. 2020;31(3):178–184.
- Bell CM, Chapman RH, Stone PW, et al. An off-the-Shelf help list: a comprehensive catalog of preference scores from published cost–utility analyses. Med Decis Making. 2001;21(4):288–294.
- 2 Health-related quality of life for people with long-term conditions [Internet]. NHS Digit; 2022 [cited 2022 Mar 30]. Available from: https://digital.nhs.uk/data-and-information/publications/statistical/nhs-outcomes-framework/march-2022/domain-2---enhancing-quality-of-life-for-people-with-long-term-conditions-nof/2-health-related-quality-of-life-for-people-with-long-term-conditions
- NHS Digital. Health related quality of life for people with long-term conditions; 2019.
- Menzel P, Dolan P, Richardson J, et al. The role of adaptation to disability and disease in health state valuation: a preliminary normative analysis. Soc Sci Med. 2002;55(12):2149–2158.
- Statista. Countries with the highest internet penetration rate 2021; [Internet]; 2022 [cited 2022 Jan 6]. Available from: https://www.statista.com/statistics/227082/countries-with-the-highest-internet-penetration-rate/