
Abstract
Background
Prior economic analyses demonstrate that legacy tissue valves are associated with substantial financial savings over the long run after a surgical aortic valve replacement (SAVR). Bioprostheses with RESILIA tissue reduce calcification, the primary cause of structural valve deterioration (SVD), and have demonstrated promising pre-clinical and 5-year clinical results. This economic evaluation quantifies the expected long-run savings of bioprosthetic valves with RESILIA tissue relative to mechanical valves given 5-year clinical results and expected performance through year 15.
Methods
Simulation models estimated disease progression across two hypothetical SAVR cohorts (tissue vs. mechanical) of 10,000 patients in the US over 15 years. One comparison evaluated RESILIA tissue valves relative to mechanical valves. The other compared legacy SAVR tissue and mechanical valves. Health outcome probabilities and costs were based on literature and expert opinion. Incidence rates of health outcomes associated with mechanical valve were calculated using relative risks of expected outcomes in tissue valve versus mechanical valve patients. The comparisons also accounted for anti-coagulation monitoring in both cohorts. Savings estimates are based on US healthcare costs and do not yet account for the premium associated use of RESILIA relative to a standard tissue valve.
Results
Relative to mechanical SAVR, the median net discounted savings for a patient receiving SAVR with a RESILIA tissue valve is $20,744 ($US, 2020; 95% CI = $15,835–$26,655) over a 15-year horizon. While 30-day and 1-year savings were not significant, expected savings after 5 years are $9,110 (95% CI = $6,634–$11,969). Net savings for RESILIA SAVR valves were approximately 30–50% larger than savings anticipated using legacy tissue SAVR valves.
Conclusion
RESILIA tissue valves are associated with lower health expenditures relative to mechanical valves.
Introduction
Surgical aortic valve replacement (SAVR) is a frequently provided treatment for moderate-to-severe aortic stenosis (AS) – a common diagnosis in the US populationCitation1,Citation2. Two general types of valve replacements for SAVR are mechanical and tissue (bioprosthetic) valves. Valve choice has frequently depended on factors such as expected durability, the potential for reoperation, whether patients may experience bleeding or thrombosis, the patient’s expected lifespan after the SAVR operation, and factors related to diet, exercise, and other lifestyle preferencesCitation1. Typically, a key tradeoff between tissue and mechanical valve SAVR is whether the expected higher risk of reoperation associated with tissue valves is offset by the burden of lifelong anticoagulation monitoring (ACM) necessitated by the use of a mechanical valves and the attendant risks of ACM such as bleeding or stroke. Prior meta-analyses and comparative studies have identified health outcomes associated with tissue and mechanical SAVR, only recently has an economic evaluation explicitly examined the expected trajectory of US health system costs over periods of up to 25 years associated with tissue relative to mechanical valves for SAVRCitation3–16. While the initial economic analysis supported use of tissue valves, costs associated with reoperation were generally larger in the tissue valve cohorts which used “legacy” technologyCitation8. However, subsequent innovations in material science have improved the durability of tissue valvesCitation17–19. One of the key differentiating features in “legacy” tissue valves and current tissue valve technology is the addition of RESILIA, a preservation technology that permanently blocks residual aldehyde groups that bind to calcium and reduces calcificationCitation20. Five-year clinical data from the COMMENCE trial indicate lower reoperation rates and structural valve deterioration (SVD) for aortic valves that have the RESILIA anti-calcification platform, a technology engineered for extended durabilityCitation17–19,Citation21,Citation22. Using the published COMMENCE data, this study quantifies the expected long-term discounted per-surgery savings when using a RESILIA valve relative to a mechanical valve for SAVR.
Methods
This financial model follows published guidance for economic evaluations in healthcare (CHEERS methodology)Citation23–26. The study adopts a health system perspective for the US and focuses on expenditures for sequalae subsequent to an initial SAVR procedures. The structure of the model is similar to the previously published approach: first we assumed equally-sized synthetic cohorts for (A) “mechanical SAVR” and (B) “tissue SAVR” patients (n = 10,000 each)Citation8. The model estimates sequelae for 15 years after the initial SAVR procedure and accounts for mortality and five other clinical events associated with SAVR within each period (conditional on survival) – the same events used in the prior economic analysis of tissue vs. mechanical SAVRCitation27. These events are (1) endocarditis, (2) bleeding or hemorrhagic event, (3) thrombosis, (4) reoperation, and (5) anti-coagulant monitoring (ACM; required for life in the case of mechanical SAVR or assumed to last 6 months in the case of tissue SAVR). This study excluded stroke, as both bleeding/hemorrhage and thrombosis could potentially “double counted” as both a stroke and either a bleeding event (hemorrhagic stroke) or thrombotic event (ischemic stroke caused by thromboembolism). Within each time period, we estimated the total SAVR-related expenditures by multiplying the expected number of events occurring in a hypothetical cohort of patients by the cost per event (after accounting for discounting and medical inflation).
Incidence Rates with Novel Tissue Valves (RESILIA)
The model estimated the probability of each clinical event after implantation of a novel tissue valve occurring in the first 30 days after the initial SAVR surgery and every year thereafter over a 15-year horizon (Figure A3, Supplementary Material). During the first 5 years, also referred to as the “clinical data period”, data on incidence of events reflect the clinical results of the COMMENCE trialCitation21. Event definitions applied in the COMMENCE trial have been previously publishedCitation28. For each period in the “clinical data period”, the probability of events accounted for survival and relied on initial sample size, number of events and life-years recorded in the COMMENCE trial (Table A1, Supplementary Material). After year 5, the period that will be referred to as the “projection period”, clinical data are not yet available for RESILIA valves, so the model relies on weighted data from the three primary legacy long-term tissue valve cohort studies to conservatively approximate the incidence of events in years 5–15 for tissue valves (Table A5, Supplementary Material)Citation15,Citation29,Citation30. While the 5-year results are likely the most reliable, we felt it important to include the projection period of 10 years since “reoperation” and “ACM costs” are the most important sources of savings (or costs) estimated in prior models and probabilities of reoperation (across all patient types) increase as a function of time after surgery. Incorporating the longer time horizon allows for a more conservative “long run” estimate of savings relative to simple linear extrapolation based on 5-year savings.
The model assumes tissue SAVR patients undergo ACM for 6 months after surgery, but mechanical SAVR patients require ACM for lifeCitation1. The base case version of the model also conservatively assumes that mortality rates for tissue valves are equal to those of mechanical valves (from a pure cost perspective this assumption likely results in relatively larger costs associated with the tissue valve cohort).
Incidence rates with mechanical valves
The event rates for each health outcome in the mechanical valve cohort are calculated by multiplying event-specific relative risks by the incidence rates for each of the clinical events in the tissue valve cohort. Since the COMMENCE trial was a single-arm study (no mechanical valve comparator was evaluated in the trial), we estimate the relative risk for each event type by dividing an annual incidence rate from a comparable mechanical valve study by the rate estimated for tissue valves in the COMMENCE trial (Table A2, Supplementary Material). In select scenario analyses, the relative risks for each outcome are adjusted to more conservative or more aggressive estimates (Table A3, Supplementary Material). The base case values were generally the median of the three estimates reported in Table A3.A (lower three rows) (Supplementary Material), except in the case of thromboembolism where a relatively conservative (high) estimate was kept for RESILIA tissue valves (relative to mechanical valves). In the conservative scenario the largest of the three relative risk estimates are used (which increase the expected costs associated with RESILIA valve use). The only exception was the reoperation relative risk (maintained at 1.11) since we evaluate the highest relative risk (2.19) separately in a sensitivity analysis. In the most aggressive scenario, the lowest of the three estimated relative risks are used with the exception of the slightly higher thromboembolism estimate.
Events and costs
For each cohort, the total annual events for each event type are estimated by multiplying the cohort size at the beginning of the period by the incidence rate for that period. These events are then multiplied by the cost of each event to estimate overall costs across the entire cohort in each period. The model purely focuses on costs and does not include quality-of-life (QoL) nor does it calculate incremental cost-effectiveness ratios (ICERS). Costs per event (Table A4, Supplementary Material) were derived from the literature and were updated to 2020 US dollars based on historic medical inflation estimates for inpatient careCitation31–34. The estimates are most appropriate for the US health care system and may differ substantially in the health systems of other countries. The “base case” model assumed a medical inflation rate of 3% and discounted future costs by 3% (so effectively each of these factor offset each otherCitation24,Citation25. The simulation model included both the mean estimate of cost inputs and standard deviation (or similar measures of variation) for each cost input. If standard deviations of a particular cost input were not available from the literature, estimates of the coefficient of variation (CoV or the standard deviation divided by mean) from prior US hospital inpatient cost analyses were applied to calculate standard deviationsCitation35. Costs for tissue and mechanical SAVR hospitalizations were based on Medicare reimbursement. The historical experience in Medicare payment slightly favored tissue SAVR (by $244 or ∼0.5% of $51,864). These costs may include a DRG payment from the payer to the hospital, which incorporates the cost of the device. Hence, this analysis offers perspective on the savings capacity over time associated with tissue SAVR. To the extent that financial stakeholders (payers, hospitals, or patients) absorb any addition costs for novel devices, those can be deducted from the savings estimate in the relevant period, but such marginal costs may vary across and within markets (and typically are confidential) so they are not estimated in our model. Thromboembolism and endocarditis costs were derived from the literature. In addition, the cost of a bleeding event ($22,085) was based on analysis of an internal database (Truven MarketScan). Thromboembolism costs also accounted for subsequent related complications. Costs for bleeding and endocarditis included both the initial hospitalization and readmission costs. The base case for a bleeding event was similar to the literature-based cost of a hospitalized stroke ($25,394)Citation36.
The model relied on a prior time-dependent activity-based costing (TDABC) analysis to account for anticoagulation medication and monitoring (ACM) costs. TDABC accounts for labor time and fixed and variable unit costs related to both (A) medical prescriptions that address coagulation and (B) services and diagnostics that ensure medication adherenceCitation37. On a yearly basis the model estimates ACM costs at $1,694. This weighted estimate includes stable (48%, $1,057), average (33%, $1,605) and unstable (19%, $3,461) patients based on INR measurements. These costs were based on the experience of patients from the Mayo Clinic who were on warfarin and visiting an ACM clinic. In the model, stable patients were assumed to receive ACM services once per month.
Model types
The base case “deterministic” model estimates the total discounted SAVR-related costs in both tissue SAVR and mechanical SAVR patient groups in every time period (first 30 days, annually for 15 years thereafter). Overall period costs are the product of expected clinical events in the period and the associated cost for each clinical event type. We then aggregate these expenditures over time across different durations (from any period between 30 days and 15 years) for both our tissue SAVR and mechanical SAVR cohort. The deterministic model helps calculate the “average” expected effect, but the Monte Carlo simulations incorporated both the mean and distribution of key inputs. In the simulation model health event probabilities are assumed to follow a “beta” distribution and the standard deviations are calculated on the basis of the absolute numbers of “cases” relative to the “number at risk” from the relevant studies. Cost inputs are assumed to have a “gamma” distribution and, as these are US hospital costs, we use previously reported “coefficient of variation” data for US hospitals to estimate standard deviationCitation35. When we apply hazard rates or relative risks, these are assumed to have a “normal” distribution with standard deviations reported from the source studies.
The simulation approach may result it slightly different averages than the deterministic model and simulations also provide confidence intervals. Each simulation ran 10,000 trials based on the random draws of each input. The mean and median (5,000th) output value were estimated, and the 250th and 9,750th supplied our 95% confidence interval (CI) and, if this interval did not include $0, it was statistically significant. Sensitivity and scenario analyses were also conducted to highlight the key determinants that drive our central outcome – the difference in cumulative SAVR-related healthcare costs per person comparing tissue and mechanical patient groups. Models were programmed using @Risk v8.2 within Microsoft Excel.
Results
Novel tissue vs. mechanical valves: base case results
The results generally demonstrate that valves employing RESILIA are expected to reduce future health system expenditures relative to mechanical valves used for SAVR. These savings accrue both in the first 5 years of the model and during the “projection period” (years 5–15) when the incidence rates for the tissue valve cohort revert to the weighted estimates from older tissue devices long-run registries due to lack of data availability beyond 5 years for the novel tissue valve with anti-calcific properties (, ). Specifically, by year 5 the discounted cumulative savings in the deterministic (simulation) model are $8,872 (Median = $9,093; 95% CI = $6,589–$12,048). Projecting to year 15, associated net savings increase to $20,498 (Median = $20,755; 95% CI = $15,780–$26,636). Given the distributions and input estimates and distributional assumptions for the base case model, RESILIA valves are associated with statistically significant cost savings (the 95% CI exceeds $0) by the end of year 2 and statistical significance is maintained through year 15.
Figure 1. Cumulative net discounted savings over time per initial SAVR surgery. Associated with novel tissue vs. mechanical valves ($US 2020). Base case model.
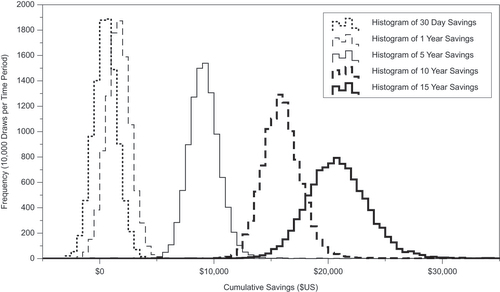
Figure 2. Cumulative net dicounted savings over time per initial SAVR surgery associated with novel tissue vs. mechanical valves ($US 2020), by reoperation relative risk estimate (projection period).
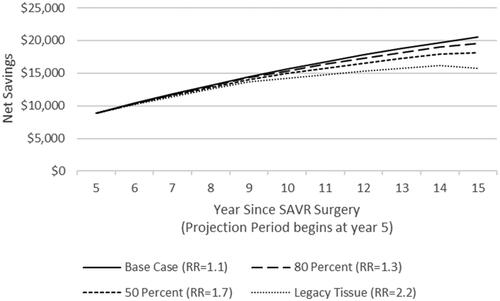
Table 1. Cumulative net discounted savings per initial SAVR surgery associated with the novel tissue vs. mechanical valves ($US 2020) base case model.
Select sensitivity analyses
Probabilistic sensitivity analyses (PSAs) for the 5-year and 15-year models help identify which stochastic inputs influence the savings outcome the most (Figures A1 and A2, Supplementary Material). In both the 5- and 15-year models which compare the RESILIA tissue and mechanical valves, inputs related to the cost or probability of operation or reoperation for the SAVR procedure are ranked the most important. After reoperation SAVR inputs associated with endocarditis, bleeding, mortality, and thromboembolism (in that order) are the next most important in the 5-year analysis. In the 15-year analysis the order of the secondary factors is similar, but mortality estimates appear to be slightly more influential than bleeding inputs.
While the PSA helps identify reoperation as a central driver that influences savings, the omission of non-stochastic inputs, specifically anti-coagulant monitoring costs (which are not estimated with a distribution and variance in the simulation) prompted an alternative analysis to help draw out the relative importance of each of the clinical sequelae and ACM costs. disaggregates the contribution of each of the sequelae and ACM costs from the deterministic model. This analysis also has the benefit of jointly accounting for multiple factors (including relative risk, probability of health outcome occurring in tissue valve cohort, cost per occurrence of each health outcome) that impact overall savings related to each health outcome.
Table 2. Disaggregated cumulative net discounted savings per initial SAVR surgery associated with the novel tissue vs. mechanical valves ($US 2020) base case deterministic model.
Across almost all time periods assessed in the model, savings associated with ACM cost reduction in novel tissue valve patients are a substantial share of overall savings. After 5 years, approximately 81% ($7,145 of $8,872) of the net savings are accounted for by ACM cost savings. By year 15, 93% of the net savings are derived from ACM cost reductions. If the ACM costs were excluded from the analysis (final column of ), savings would still accrue in patients receiving RESILIA valves rather than mechanical valves, but the levels would naturally be substantially lower ($1,727 in the 5-year analysis and $1,481 in the 15-year model).
Given the potential importance of reoperation on costs, we also conducted a set of sensitivity analyses in which alternative reoperation relative risks are applied during the “projection period” between years 5 and 15 (the base case model assumes a reoperation rate relative risk of 1.1 which translates to 10% higher probability of reoperation in the RESILIA group relative to the mechanical valve group). If the relative risk increases to 2.2 for reoperation immediately upon year 5 (the assumption that was previously applied to legacy tissue valves), the net savings by year 15 drop to $15,697 (). Less conservative assumptions (lower relative risk values for the reoperation rate) naturally yield larger savings estimates compared to the most conservative approach. Net savings are $19,538 at 15 years if the relative risk is 1.3 (80% of the “benefit” level from year 0 to 5) and $18,098 if the relative risk is 1.65 (50% of the “benefit”).
Relative risk scenario analyses
Given the frequent use of “single arm” studies to estimate incidence rates of important sequelae across different types of medical devices, our study applied three primary approaches to estimate relative risks between tissue and mechanical valves. First, clinical trial estimates from RESILIA valves were compared to mechanical valve studies with similar durations and endpoints. Second, existing literature including single one-off studies of legacy tissue valves and mechanical valves were evaluated. Lastly, robust and frequently cited meta-analyses were consulted. Each approach generally yielded different but generally comparable estimates. Table A3 (Supplementary Material) accounts for the dispersion in these relative risks and, in addition to the “base case” scenario discussed above, includes a “conservative” and “aggressive” scenario. Across all scenarios, the mortality relative risk is fixed at 1.0 (a conservative assumption for tissue valves). In the conservative scenario where both the bleeding and endocarditis relative risks increase to favor mechanical valves the 5-year savings drops to $7,266 and the 15-year savings is $18,208 in the deterministic model. In the more aggressive model 5-year and 15-year savings associated with novel tissue valves increase to $11,640 and $25,899 respectively ().
Table 3. Cumulative net discounted savings per initial SAVR surgery associated with novel tissue vs. mechanical valves ($US 2020). Scenario analyses for relative risk (deterministic models).
Legacy tissue valve savings
In the comparable model for legacy tissue valves (which have higher re-operation rates than novel tissue valves) the savings relative to mechanical valves are $6,585 at year 5, $2,287 less than the 5-year savings in the base case model for a novel tissue valve (Table A6, Supplementary Material). After including the “projection window” (years 5–15) the savings are $13,456 at year 15, $7,042 less than the savings anticipated in the “base case” model for the novel tissue valve. A large share of the differential between the legacy tissue valve and the novel tissue valve is due to the substantially larger reoperation costs (and the balance of the difference primarily stems from event probabilities in the first 5 years). At 5-years reoperation costs are $1,182 more than mechanical valves in the legacy model, but just $63 in the novel tissue valve model. Similarly, at 15 years the differential increases to $5,289 ($5,833 in additional reoperation costs for legacy tissue valves and $544 additional costs with novel tissue valves). In the case of the legacy tissue valves the savings generated from reduced ACM are substantially offset by the larger reoperation costs. This countervailing cost is substantially lower in the case of novel tissue valves.
Conclusion
The deterministic and simulation models both demonstrate that novel tissue valves are associated with long-run savings relative to mechanical valves. While prior economic analyses indicated that even legacy tissue valves yield savings relative to mechanical valves, this analysis updates expectations given the 5-year clinical data for novel tissue valvesCitation8. The anticipated improvement is derived mainly from lower expected reoperation rates while the savings associated with lower ACM costs are retained.
It is important to consider the limitations to place the results in context. One limitation of the study is the restricted duration (15 years). While the prior economic analysis for legacy tissue valves covered a 25-year period, it was supported by data from a series of long-run cohort studies. Given that there was just 5 years of clinical data (along with substantial promising laboratory analyses), we felt it reasonable to restrict the model to 15 years with relatively conservative incidence and relative risk assumptions for the “projection period” between years 5 and 15. But reoperations do occur over extended periods – it is not uncommon for reoperations to occur beyond 15 years (and likely at a higher rate as time proceeds). As additional years of clinical follow-up occur, additional data will more precisely inform the benefit associated with more advanced tissue valves.
A second limitation is the lack of randomized controlled trials to directly compare outcomes for SAVR valve options. As such, our findings should be interpreted as associations rather than causal evidence. Going forward, comparative cohort studies that follow similar patients receiving either tissue or mechanical SAVR may help bridge the “causation gap” and improve the robustness and validity of evidence for making clinical and economic evaluations. In selecting studies to help populate the model inputs, we generally included large trials or cohort studies with long follow-up periods, but the samples across studies likely were not perfectly matched. In addition, as this analysis relies on large, historical studies which represent multiple mechanical valve technologies; the savings estimates for tissue valves in this analysis are perhaps best interpreted as a comparison based on the historical performance of mechanical valves as a class rather than a particular model. If select mechanical valves, in practice, perform better than the historical “average”, cost savings may differ and could be reduced. Both the lack of an RCT design and the use of a general mechanical SAVR data are key reasons why we conducted sensitivity and scenario analyses.
Third, as a pure economic evaluation, these analyses exclude value related to quality-of-life (QoL) improvements. Stakeholders such as health insurers and payers should ideally pair this analysis with their expectations for the implicit value of improving QoL via stronger health outcomes. Clinical events may naturally be a more important factor in clinician decision-making and patient preference than pure financial savings (which do not necessarily accrue to the patient). In addition, the model assumed parity in mortality rates. If one believes the relative risk of mortality is greater (less) than one in tissue valves relative to mechanical valves, the model underestimates (overestimates) savings associated with tissue valves.
Fourth, the model uses data on reoperation, irrespective of whether the reoperation was due to SVD. Given that there were no cases of SVD detected in the first 5 years of the COMMENCE trial, the model may be overestimating the number of reoperations associated with the RESILIA valves. Conditional on the expectation there are no reoperations tied to SVD, net savings linked with the RESILIA tissue valves may be too small. Savings would be larger if fewer reoperations were associated with novel tissue valves than in the current base case model. While the definition used for SVD in the COMMENCE trial was more stringent than the VARC-2 definition that accounts for hemodynamic compromise, it is reoperations, not SVD, that impacts associated savings in the model. However, both SVD and reoperation data on novel tissue valves do not yet extend beyond 5 years.
Fifth, the results are best construed as the expected savings, in aggregate, for a sample of patients with a mean age of 67 (some younger, some older). While the COMMENCE trial did not have sufficient sample size to make inferences about subgroups defined by age it enrolled patients from 32 centers and had relatively broad inclusion/exclusion criteria. Future economic research with larger samples in either younger or older cohorts will illuminate the linkage between age, health outcomes and expected savings. Moreover, as guidelines have historically called for use of mechanical valves in younger (<50) patients and tissue valves in older patients (>65), to the degree our clinical comparisons do not fully account for selection issues, the estimates of clinical events and their attendant costs may impart bias. If it is the case the older, sicker patients are more likely to historically have received tissue valves; the direction of such a bias may overestimate events and underestimate cost savings for tissue valve patients relative to mechanical valves. However, lacking full information on the patients across studies, only causal studies in the future can more precisely identify the clinical and economic value associated with tissue valves.
Sixth, to the extent that strokes are not accounted for in either the “bleeding” or “thromboembolism” health outcomes, the result may be biased. It is likely that this omission would bias the savings estimate downward if strokes (like bleeding and thromboembolism) are more common with mechanical valves. The costs associated with bleeding and thromboembolism event may not also include some of the longer term costs related to stroke such as rehabilitation expenditures.
Lastly, while our analysis suggests there is an additional savings premium associated with the use of RESILIA valves, relative to legacy tissue valves, the comparison is indirect. Future clinical comparisons of different tissue valve technologies could help refine the improvement in relative value associated with improved medical technology.
Payers, patients, physicians and other stakeholders weigh several factors as they seek to optimize clinical and economic outcomes linked to AS treatments. While finance and costs are just one “pillar” to consider in the decision-making process, this evaluation suggests that it is very likely that tissue valves confer long-run economic benefit relative to mechanical valves at the payer, insurer, and patient level. Moreover, recent improvements in tissue SAVR technology have potentially expanded the economic benefit relative to mechanical valves beyond what they were with legacy tissue valves.
Transparency
Declaration of funding
This research was supported by Edwards Lifesciences.
Role of the Funder/Sponsor: Two authors are employees of the funder, Edwards Lifesciences, and two authors are paid consultants to Edwards Lifesciences.
Declaration of financial/other relationships
EK and TN receive consulting fees from Edwards Lifesciences. TN also receives fees as a speaker for Edwards Lifesciences. MR and GM are both employees of Edwards Lifesciences. TN did not receive any fees as a consequence of this project.
Author contributions
Concept and design: EK, MR, MG, TN.
Acquisition of data: EK.
Analysis and interpretation of data: EK, MR, MG, TN.
Drafting of Manuscript: EK.
Critical revision of paper for important intellectual content: EK, MR, MG, TN.
Obtaining Funding: EK, MR, MG.
Administrative, technical, and logistical support: EK, MR, MG.
Statistical Analysis: EK, MR, MG, TN.
Supervision: EK, MR, MG, TN.
Reviewer disclosures
A reviewer on this manuscript has disclosed that they have received institutional grants, research support, speaker honoraria, and travel compensation from Edwards Lifesciences, Symetis SA, Jena Valve, Boston Scientific, Medtronic, Abbott, and Novartis. The other peer reviewers on this manuscript have received an honorarium from JME for their review work but have no other relevant financial relationships to disclose.
Supplemental Material
Download MS Word (324.5 KB)Acknowledgements
None.
References
- Nishimura RA, Otto CM, Bonow RO, et al. 2017 AHA/ACC focused update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. J Am Coll Cardiol. 2017;70(2):252–289.
- Nkomo VT, Gardin JM, Skelton TN, et al. Burden of valvular heart diseases: a population-based study. The Lancet. 2006;368(9540):1005–1011.
- Etnel JR, Huygens SA, Grashuis P, et al. Bioprosthetic aortic valve replacement in nonelderly adults: a systematic review, meta-analysis, and microsimulation. Circ Cardiovasc Qual Outcomes. 2019;12(2):e005481.
- Glaser N, Jackson V, Holzmann MJ, et al. Aortic valve replacement with mechanical vs. biological prostheses in patients aged 50–69 years. Eur Heart J. 2016;37(34):2658–2667.
- Hirji SA, Kolkailah AA, Ramirez-Del Val F, et al. Mechanical versus bioprosthetic aortic valve replacement in patients aged 50 years and younger. Ann Thorac Surg. 2018;106(4):1113–1120.
- Isaacs AJ, Shuhaiber J, Salemi A, et al. National trends in utilization and in-hospital outcomes of mechanical versus bioprosthetic aortic valve replacements. J Thorac Cardiovasc Surg. 2015;149(5):1262–1269.e3.
- Kilic A, Bianco V, Gleason TG, et al. Hospital readmission rates are similar between patients with mechanical versus bioprosthetic aortic valves. J Card Surg. 2018;33(9):497–505.
- Nguyen TC, Walker T, Gunnarsson C, et al. Long-term healthcare expenditures over time for tissue and mechanical aortic valve replacement. Ann Thorac Surg. 2021;112(2):526–531.
- Son J, Cho YH, Jeong DS, et al. Mechanical versus tissue aortic prosthesis in sexagenarians: comparison of hemodynamic and clinical outcomes. Korean J Thorac Cardiovasc Surg. 2018;51(2):100–108.
- Tong X, George MG, Gillespie C, et al. Trends in hospitalizations and cost associated with stroke by age, United States 2003–2012. Int J Stroke. 2016;11(8):874–881.
- Webb JG, Mack MJ, White JM, et al. Transcatheter aortic valve implantation within degenerated aortic surgical bioprostheses: PARTNER 2 valve-in-valve registry. J Am Coll Cardiol. 2017;69(18):2253–2262.
- Zhao DF, Seco M, Wu JJ, et al. Mechanical versus bioprosthetic aortic valve replacement in middle-aged adults: a systematic review and meta-analysis. Ann Thorac Surg. 2016;102(1):315–327.
- Badhwar V, Ofenloch JC, Rovin JD, et al. Noninferiority of closely monitored mechanical valves to bioprostheses overshadowed by early mortality benefit in younger patients. Ann Thorac Surg. 2012;93(3):748–753.
- Bourguignon F, Rogers FH. Distributional effects of educational improvements: are we using the wrong model? Econom Educ Rev. 2007;26(6):735–746.
- Bourguignon T, Bouquiaux-Stablo A-L, Candolfi P, et al. Very long-term outcomes of the Carpentier-Edwards perimount valve in aortic position. Ann Thorac Surg. 2015;99(3):831–837.
- Dangas GD, Weitz JI, Giustino G, et al. Prosthetic heart valve thrombosis. J Am Coll Cardiol. 2016;68(24):2670–2689.
- Flameng W, Hermans H, Verbeken E, et al. A randomized assessment of an advanced tissue preservation technology in the juvenile sheep model. J Thorac Cardiovasc Surg. 2015;149(1):340–345.
- Sadri V, Trusty PM, Madukauwa-David ID, et al. Long-term durability of a new surgical aortic valve: a 1 billion cycle in vitro study. JTCVS Open. 2022;9:59–69.
- Tod TJ, Gohres RA, Torky M, et al. Influence of tissue technology on pannus formation on bioprosthetic heart valves. Cardiovasc Eng Tech. 2021;12(4):418–425.
- Puskas JD, Bavaria JE, Svensson LG, et al. The Commence trial: 2-year outcomes with an aortic bioprosthesis with RESILIA tissue. Eur J Cardiothorac Surg. 2017;52(3):432–439.
- Bavaria JE, Griffith B, Heimansohn DA, et al. Five-year outcomes of the COMMENCE trial investigating aortic valve replacement with RESILIA tissue. Ann Thoracic Surg. 2022;2022:58.
- Bartus K, Litwinowicz R, Bilewska A, et al. Final 5-year outcomes following aortic valve replacement with a RESILIA™ tissue bioprosthesis. Eur J Cardiothorac Surg. 2021;59(2):434–441.
- Drummond M, Barbieri M, Cook J, et al. Transferability of economic evaluations across jurisdictions: ISPOR good research practices task force report. Value Health. 2009;12(4):409–418.
- Husereau D, Drummond M, Petrou S, et al. Consolidated health economic evaluation reporting standards (CHEERS)—explanation and elaboration: a report of the ISPOR health economic evaluation publication guidelines good reporting practices task force. Value Health. 2013;16(2):231–250.
- Neumann PJ, Sanders GD, Russell LB, et al. Cost-effectiveness in health and medicine. Oxford: Oxford University Press; 2016.
- Husereau D, Drummond M, Augustovski F, et al. Consolidated health economic evaluation reporting standards 2022 (CHEERS 2022) statement: updated reporting guidance for health economic evaluations. Int J Technol Assess Health Care. 2022;38(1):32.
- Nguyen T, Walker T, Moore M, et al. Long-term healthcare expenditures over time for tissue and mechanical aortic valve replacement. Ann Thoracic Surg. 2021;112(2):526–531.
- Akins CW, Miller DC, Turina MI, et al. Guidelines for reporting mortality and morbidity after cardiac valve interventions. Eur J Cardiothorac Surg. 2008;33(4):523–528.
- Bourguignon T, El Khoury R, Candolfi P, et al. Very long-term outcomes of the Carpentier-Edwards perimount aortic valve in patients aged 60 or younger. Ann Thorac Surg. 2015;100(3):853–859.
- Bourguignon T, Lhommet P, El Khoury R, et al. Very long-term outcomes of the Carpentier-Edwards perimount aortic valve in patients aged 50–65 years. Eur J Cardiothorac Surg. 2016;49(5):1462–1468.
- Dunn A, Grosse SD, Zuvekas SH. Adjusting health expenditures for inflation: a review of measures for health services research in the United States. Health Serv Res. 2018;53(1):175–196.
- Grosse SD, Nelson RE, Nyarko KA, et al. The economic burden of incident venous thromboembolism in the United States: a review of estimated attributable healthcare costs. Thromb Res. 2016;137:3–10.
- Morita Y, Haruna T, Haruna Y, et al. Thirty‐day readmission after infective endocarditis: analysis from a nationwide readmission database. J Am Heart Assoc. 2019;8(9):e011598.
- Simon Ak A, Brown P, Reynolds M, et al. 90-Day cost and clinical outcomes comparing TAVR to SAVR: do the economics work? Presented at: American college of cardiology. Orlando, FL. Session Aortic Valve Disease: optimizing TAVR; 2018.
- Cooper Z, Craig SV, Gaynor M, et al. The price ain’t right? Hospital prices and health spending on the privately insured. Q J Econ. 2019;134(1):51–107.
- Wang G, Zhang Z, Ayala C, et al. Costs of hospitalization for stroke patients aged 18–64 years in the United States. J Stroke Cerebrovasc Dis. 2014;23(5):861–868.
- Bobade RA, Helmers RA, Jaeger TM, et al. Time-driven activity-based cost analysis for outpatient anticoagulation therapy: direct costs in a primary care setting with optimal performance. J Med Econ. 2019;22(5):471–477.