
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background
Breast cancer (BC) poses a public health challenge as the most commonly diagnosed cancer among women globally. While BC mortality has declined across Europe in the past three decades, an opposite trend has been reported in some transitional European countries. This analysis estimates the mortality burden and the cost of lost productivity due to BC deaths in nine Central and Eastern Europe (CEE) countries: Bulgaria, Croatia, Czech Republic, Hungary, Poland, Romania, Serbia, Slovakia, and Slovenia, that have defied the favorable cancer mortality trends. These estimates may provide relevant evidence to aid decision-makers in the prioritization of BC-targeted policies.
Methods
The human capital approach (HCA) was used to estimate years of life lost (YLL) and productivity losses due to premature death from BC (ICD-10 code: C50 Malignant neoplasm of breast). YLL and present value of future lost productivity (PVFLP) were calculated using age and gender-specific mortality, wages, and employment rates. Data were sourced from the World Health Organization (WHO), Eurostat, and the World Bank.
Results
In 2019, there were 19,726 BC deaths in the nine CEE countries. This study estimated BC deaths resulted in 267,184 YLL. Annual PVFLP was estimated to be €85 M in Poland, €46 M in Romania, €39 M in Hungary, €21 M in Slovakia, €18 M in Serbia, €16 M in Czech Republic, €15 M in Bulgaria, €13 M in Croatia, and €7 M in Slovenia.
Conclusion
Premature death from BC leads to substantial YLL and productivity losses. Lost productivity costs due to premature BC-related mortality exceeded €259 million in 2019 alone. The data modeled provide important evidence toward resource allocation priorities for BC prevention, screening, and treatment that could potentially decrease productivity losses. Careful consideration should be given to BC-specific policies, such as surveillance programs and the availability of new treatments in CEE countries to decrease the medical and financial burden of the disease.
1. Introduction
Breast cancer (BC) is a pathological condition that develops in the breast tissue. In most cases, emergence occurs predominantly within milk ducts but is also known to develop within breast lobulesCitation1. The 2020 GLOBOCAN database reported around 2.3 million new cases of BC globally, making BC the most common tumor among women worldwideCitation2. The prevalence of BC is widely recognized with over 7.8 million women in 2020 diagnosed with BC in the past five yearsCitation3.
There are four main molecular subtypes of BC with distinct features requiring different treatment modalities. BC subtypes are primarily defined based on the presence or absence of the following receptors: human epidermal growth factor receptor-2 (HER2) and the hormone receptors (HR): estrogen receptors (ER), and progesterone receptors (PR). The most common subtype, luminal A (HR+/HER2–), is positive for hormone receptors and typically has a slower growth rate compared to the other subtypes. The second subtype, luminal B (mainly HR+/HER2+), is also positive for hormone receptors but grows faster than the luminal A subtype. Triple-negative breast cancer (TNBC) is an aggressive type of BC that lacks the expression of ER, PR, HER2 and is referred to as HR−/HER2–Citation4. The aggressive nature of this cancer stems from its complex molecular characteristics which does not respond to systemic therapy, resulting in poor overall prognosis compared to HR-positive patientsCitation5. TNBC comprises approximately 15-20% of all BC cases and women with TNBC are more prone to recur or relapse given its rare immunohistochemical characteristicsCitation6. The fourth subtype is HER2-positive BC which is ER- and PR-negative and HER2-positiveCitation7.
There are striking variations in cancer epidemiology between European countries, including significant differences in the cancer incidence and mortalityCitation8. Central and Eastern Europe (CEE) generally have higher incidence of cancers than other areasCitation9. Excess mortality can be seen in CEE versus western European countries, with a study estimating that over 55,000 cancer deaths could be avoided by closing the mortality gapCitation10. A number of attributable factors could be associated with these regional variations, including: different prevalence of underlying risk factors, inadequacies in screening and early diagnosis, the distribution of cancer types, and different treatment options and follow-up careCitation11. Furthermore, it has been reported that CEE countries spend less per person on pharmaceuticals, and fewer EMA-approved drugs are reimbursed in CEE countries than in other European countries, which could add to the burden of mortality due to later diagnosis and limited treatment options. Although there is a growing body of evidence that recognizes the importance of the clinical and humanistic burden of BC in CEE countriesCitation12, few studies have investigated the economic burden of this disease in these regionsCitation13.
In order to develop long-term evidence-based policy decisions, a greater understanding of the epidemiology, healthcare resource utilization, and productivity losses associated with BC is needed. It is recognized that cancer poses a considerable economic burden, not only to healthcare systems, but also to other areas of the economy, including productivity losses through early mortality and absenteeismCitation13. Out of all cancers, BC is associated with the highest healthcare costs, at €6.7 billion every year, and accounts for approximately 13% of the total cancer healthcare costs in the European Union (EU)Citation13. Recent evidence investigating the societal and economic burden of premature death due to BC using years of life lost (YLL), years of productive life lost (YPLL), and present value of future lost productivity (PVFLP) metrics suggested that the expenditure for patients with BC in Hungary amounted to €167.51 million and the average cost per patient was around €2,585Citation14. Due to the higher incidence and mortality rates of BC in CEE compared to other European areas, there may be higher overall higher lost productivity, and an increased proportion of mortality in younger age groups would lead to a higher productivity loss per cancer death in the modelCitation15. However, at the time of writing, no published literature on productivity loss due to BC in CEE has been identified.
The current BC policy landscape in CEE sees various stakeholders united with the common goal of reducing cancer mortality and improving its prognosisCitation16. Over the past decade, member states in the EU have formulated and/or updated their National Cancer Control Programme to tackle the growing burden of BCCitation16. As oncology care is not independent of the other segments of the healthcare system, an efficient allocation of resources dedicated toward cancer care needs to be carefully balanced with other healthcare needs to mitigate the significant costs associated with BC.
This analysis was conducted to estimate the societal and economic burden of premature death due to BC in nine CEE countries (Bulgaria, Croatia, Czech Republic, Hungary, Poland, Romania, Serbia, Slovakia, and Slovenia) over a one-year period (2019). More specifically, the study calculated YLL, YPLL, and PVFLP to illustrate, using quantitative evidence, the impact that premature mortality due to BC has on societal costs, and provide support for shaping cancer control policies.
2. Methods
2.1. Model structure
The human capital approach (HCA) was used to estimate productivity losses due to premature death from BC (ICD-10 code: C50 Malignant neoplasm of breast) in the nine CEE countries investigated. The methodology used is consistent with the study by Bencina et al. on the lost productivity due to head and neck cancer mortality in Hungary, Poland, and RomaniaCitation17.
The model used a lifetime horizon with a societal perspective to calculate the three primary outcomes of interest: YLL, YPLL, and PVFLP. As patients entered the model at death, any costs incurred whilst alive, such as direct costs to the healthcare system including treatment costs, were not considered in the model. BC patients who died in 2019 were incorporated into the model population, and in order to reflect varying mortality different ages, the population was stratified into age groups. Deaths across all age categories were considered in YLL calculations, however, years of life lost after retirement age were not included in the YPLL and PVFLP calculations as productivity losses are not incurred after retirement. The default model retirement ages were country- and gender-specific.
2.2. Model calculations
To calculate YLL, YPLL, and PVFLP, the model first estimated expected life years remaining and expected productive life years remaining using the following formulae:
where i = 1,2,3…I are population age groups used in the model.
2.2.1. Years of life lost
YLL is a measure of premature mortality that considers both the frequency of deaths and the age at which death occurs. In the model, YLL for the population is calculated by multiplying the number of deaths by the expected life years remaining for an individual using the following formula:
where i = 1,2,3…I are population age groups used in the model.
YPLL is an estimate of the average years a person would have been in productive employment (defined in this model as earning a wage) had they not died prematurely of BC, aggregated for the whole population who died of BC in 2019. It was assumed that the population would be in employment until the retirement age (unemployment is also taken into account throughout life), after which all labor participation ceases. In the model, YPLL is calculated using the following formula:
where i = 1,2,3…I are population age groups (see section on epidemiological inputs for more detail).
2.2.2. Present value of future lost productivity
In the model, PVFLP was calculated in two steps. The model first calculated the PVFLP (per person) by multiplying the productive life years remaining by country-, age-, and gender-specific annual wages (productive life years refer to those in employment i.e. before the retirement age). The model then calculated the PVFLP (per country) by multiplying the PVFLP (per person) by the age-specific mortality data.
PVFLP was corrected for country-level unemployment rates (using labor force participation as a measure of unemployment in the base case) to reflect the actual labor force characteristics. Annual earnings were discounted at a rate of 3% annually to obtain the present value of future earnings.
PVFLP per person was estimated using the following formula:
where i = 1,2,3…I are population age groups.
Secondly, PVFLP per person was multiplied by the age-specific mortality data to obtain an estimate of the PVFLP per country.
where i = 1,2,3…I are population age groups.
2.3. Inputs and assumptions
The model included epidemiological data to estimate YLL and YPLL and economic data to estimate PVFLP (Supplement 1)Citation18–23.
2.3.1. Epidemiological inputs
Epidemiological inputs included mortality data and life expectancies. Mortality data were derived from Eurostat (Supplement 2) which stratifies mortality by country, age group and cancer indication. Due to a lack of data on the distribution of mortality within each age group, it was assumed to be uniformly distributed. YLL was calculated using life expectancy data. Country and sex-specific life expectancy estimates were sourced from the World Bank (Supplement 3). The estimation of the mortality ratio of molecular subtypes of BC utilized incidence and five-year survival data from a population-based study conducted in Belgium due to a lack of published data from CEE countriesCitation24.
2.3.2. Economic inputs
The model used country-specific economic inputs including mean annual earnings and labor force participation rates to estimate the PVFLP. The most recent available data before 2020 were used to avoid modeling the impact that COVID-19 has had on the labor market and annual earnings. Mean annual earnings were reported in Euros (Supplement 4, Supplement 5) and labor force participation rates were reported as percentages (Supplement 6). Costs that could have been incurred (e.g. future medical costs) were not considered as these are not associated with productivity losses.
Data regarding annual earnings, minimum wage, and labor force participation rates were sourced from the Eurostat databaseCitation25–27. In instances where age groups in the Eurostat database did not align with the age groups used in the model, a weighted average was used to populate those in the model. For instance, for the 15–39 years age category, a weighted average of the “less than 30” and the “30–49 years” age categories from Eurostat were taken. Although minimum wage provides a lower estimation of PVFLP than annual average earnings, annual average earnings were used in the base case as it is a more realistic assumption to expect the majority of the population to be on the average wage as opposed to the minimum wage. In the model, individuals in the 0–14 age category were assumed to have a wage of zero.
Country-level labor force participation rates were included in the PVFLP calculations in the base case as this provides a more conservative estimate of productivity losses. Labor force participation was assumed to remain constant until the retirement age, as the data source used to populate the model assumes a constant labor force participation rate across the population. These rates were only applied to the working-age population, assumed to be 15+ in this model.
2.4. Sensitivity analysis and scenario analysis
A deterministic sensitivity analysis (DSA) was used to investigate the robustness of results, by varying epidemiological and economic inputs, namely mortality, life expectancy, retirement age, measures of income and measures of unemployment. The univariate DSA varied parameters by a default range of ±10%. As both epidemiological and economic inputs were made up of population-specific data (e.g. mortality rates were stratified by age group and sex), all related inputs were varied simultaneously to model the impact in overall changes to every type of input. This was sufficient to observe a difference in outcomes and record the impact on the PVFLP/death in a single year’s mortality from BC.
Scenario analyses included the use of minimum wage (Supplement 7) in place of annual earnings. It was assumed that minimum wage was equal across age groups and genders and only varied per country.
3. Results
There was a total of 19,726 deaths, 267,184 YLL and 49,057 YPLL, and approximately 259 M€PVFLP in 2019 from BC in the nine CEE countries of interest ().
Table 1. Total number of deaths, YLL, YPLL, PVFLP and PVFLP/deaths by country in 2019.
Although Poland had the highest overall absolute number of deaths (), it had a crude mortality rate of 0.0185% (seventh lowest of the nine countries included in the analysis). Of the nine countries investigated, Serbia had the highest BC mortality rate, followed by Hungary and Slovenia (). The population size and mortality rates are reflected in the YLL and YPLL in , e.g. Slovenia has a considerably lower YPLL than other larger countries, such as Poland.
Table 2. Population size and crude mortality rates by country in 2019.
In the nine CEE countries of interest, the highest YLL in 2019 was observed in Poland with 101,288 years (40% of the total YLL across the nine countries included in this analysis), reflective of its larger population size. Romania reported the second highest YLL with 46,516 years and Czech Republic reported the third highest YLL with 23,612 years. These three countries accounted for 64% of the total years lost.
Overall, the highest YPLL was estimated to be in Poland, with a total of 15,507 years (32% of all YPLL). Similarly to the number of deaths, the countries that reported the second and third highest YPLL were Romania and Hungary, with 8,826 years and 6,926 years respectively. These findings were reflective of the large population sizes for Poland and Romania. As expected, the country with the smallest population size, (Slovenia), reported the lowest YPLL of the nine countries investigated.
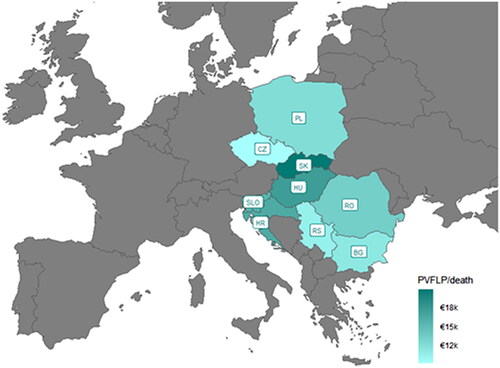
The model estimated that the PVFLP associated with premature mortality due to BC in the nine countries in 2019 exceeded €259 million. Of the nine countries included in the analysis, Poland had the highest absolute PVFLP exceeding €85 million (33% of all PVFLP), reflective of the larger population. PVFLP in Romania and Hungary were approximately €46 million and €39 million respectively. PVFLP results stratified by BC subtype are shown in (Supplements 8–12 for detailed results stratified by country and subtype). According to these results, the highest PVFLP was associated with the HR+/HER2− BC subtype.
Table 3. PVFLP results stratified by BC subtype.
Considering the total number of deaths across the nine countries in 2019, the average premature mortality cost per BC-related death was €13,152. Slovakia reported the highest PVFLP per BC-death followed by Hungary and Croatia (). Czech Republic had the lowest PVFLP per BC-death (€9,121); less than half the PVFLP per BC-death reported in Slovakia. The is primarily driven by the low retirement age in Czech Republic, particularly in females.
Figure 1. Total present value of future lost productivity (PVFLP) in 2019. Abbreviations. PL, Poland; CZ, Czech Republic; SK, Slovakia; HU, Hungary; SLO, Slovenia; HR, Croatia; RO, Romania; RS, Serbia; BG, Bulgaria.
The DSA () showed that the PVFLP per BC-death (average for countries included in the analysis) was most sensitive to changes in the retirement age, followed by the measure of productivity used (annual earnings in the base case). Consistent with the study by Bencina et al.Citation17, no change in results was observed when mortality or life expectancy were varied in the DSA. PVFLP per BC-death estimates at the lower and upper values of the input parameters are shown in .
Figure 2. Deterministic sensitivity analysis (DSA) results for annual present value of future lost productivity PVFLP) per death varied using lower and higher input parameter values.
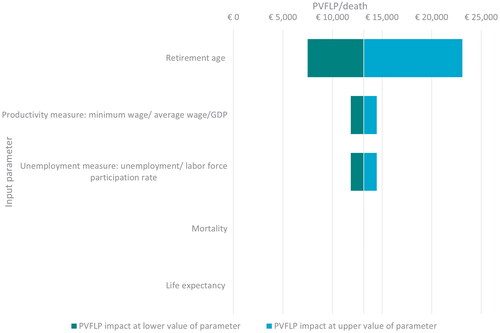
Table 4. PVFLP (€) results at the lower and upper values of the input parameters.
A scenario analysis using minimum wage in place of mean annual earnings resulted in a lower PVFLP compared to the base case model settings which used annual earnings to calculate PVFLP. In 2019, PVFLP across the nine countries exceeded €87 million when using minimum wage as an input, as opposed to €259 million in the base case. Results by country in the base case compared to scenario analysis are presented in .
Table 5. PVFLP (€) results using minimum wage.
4. Discussion
Based on this analysis, there was a total of 19,726 deaths due to BC in 2019 in the nine countries in CEE. Of the countries included in this analysis, the absolute number of deaths were highest in Poland, Romania and Hungary respectively. The number of deaths align with the population size of the countries, as Poland has a population of 38 million, Romania 19 million, Hungary 10 million, Czech Republic 11 million, Bulgaria and Serbia 7 million, Slovakia 5 million, Croatia 4 million, and Slovenia 2 million (2019 data)Citation28. When accounting for the crude death rate due to BC, Poland, which reported the highest number of deaths, also reported one of the lowest mortality rates. Based on these mortality data, 267,184 years of life were lost in 2019 due to BC in the countries investigated.
A 2018 study on the cost of cancers in Europe estimated a total productivity loss of €70 billion (€50 billion due to premature mortality and €20 billion due to morbidity)Citation29. In the current analysis, YLL due to BC were estimated to cause a loss in productivity of approximately €259 million. Despite the conversative approach used in this model to estimate PVFLP, significant losses of productivity have been estimated. Costs accrued due to premature BC mortality are estimated to exceed €85 million annually in Poland, €45.7 million in Romania, and €38.8 million in Hungary. Total PVFLP was considerably lower in the scenario analysis where minimum wage was used as a measure of productivity. Despite the lower PVFLP resulting from the use of conservative estimates of population income, the lost productivity losses were still substantial and amounted to approximately €87.3 million across the nine countries.
Other published studies have also illustrated that premature BC mortality can lead to substantial economic burden from absenteeism and loss of productive life years, which will affect the patient’s family and the government in terms of national production and tax incomeCitation30,Citation31. It is recognized that the disease stage has a direct impact on the extent of the productivity losses as cancer symptoms typically worsen as the disease progresses. Moreover, the market value of the YPLL was reported to be highest amongst mid-life women, who are estimated to have reached their most productive time of life. These findings support the rationale to implement strategies targeting age-specific improvements in productivityCitation31.
Given the substantial losses estimated in this model, BC consolidates its position as a significant contributor to the overall lost productivity costs due to cancer mortality in Europe, particularly in Poland, Romania, Hungary, and Slovenia. A multidisciplinary approach that considers all factors contributing to the premature mortality of working-age patients affected by BC is therefore needed to alleviate European countries from this pressing burden.
BC represents a public health concern requiring a multifaceted approach to improve patient outcomes. Research suggests that BC screening is crucial in improving survival as early diagnosis results in timely treatment which is strongly correlated with improved prognosis and reduced mortalityCitation32. In the UK alone, it is estimated that screening programs prevent one death due to BC for every 200 women who participate, corresponding to 1,300 fewer deaths annuallyCitation33,Citation34. Additionally, in recent years, improvements in the treatment landscape have played a pivotal role in improving survival rates in BC patients with a decreasing mortality trend observed in many European countries in the last three decadesCitation35,Citation36. Standard radiotherapy and chemotherapy treatments, novel endocrine, and targeted therapies have significantly increased survival ratesCitation37,Citation38. Particularly in TNBC where there is no standardized treatment options and chemotherapy responses are short-lived, targeted therapies are a promising treatment approach to improving overall survivalCitation38,Citation39. For this reason, a synergistic approach which combines early detection and innovative treatments should be prioritized by policymakers to alleviate the burden of BC in the population.
This model provides quantifiable evidence of the societal impact of BC using reliable data sources. The model was based on publicly available datasets from reputable organizations including the WHO, Eurostat, and World Bank. Another strength of this model was the use of country-specific input values which are reflective of the local setting e.g. local retirement ages. Moreover, the study uses gender-specific annual earnings, retirement ages and life expectancies. This is particularly important when estimating productivity losses in BC where the incidence is less than 1% in males. If sex differences were not accounted for, the model would have overestimated the productivity losses as, on average, men are in employment for longer and earn higher wagesCitation40. Although differences in population characteristics (i.e. gender and age) were incorporated where possible, simplifying assumptions were used to reflect the available data, e.g. the uniform distribution of mortality within age groups. In particular, the use of data from Belgium for the TNBC subtype calculations might not reflect the epidemiology of disease in CEE, however data for CEE were not available. Additionally, the differences in the healthcare systems across the range of countries considered in the analysis may introduce further variations between the countries and the data collection to inform the mortality estimations, in particularly the proportion of GDP utilized for healthcare expenditure within each country may impact the access to treatment and the ability to diagnose conditions between the countries modeled.
There are a number of other factors not included in this model that could impact the societal costs of BC. Firstly, this study does not account for direct costs of BC to the healthcare system, such as drug or surgery costs and therefore it does not calculate the overall economic burden of BC or its various subtypes. A study on the direct medical costs of advanced BC in the Netherlands estimated lifetime hospital costs of patients to exceed €52,000Citation41. Incorporating costs to the healthcare system in the model calculations would have therefore resulted in higher societal costs. Given the high costs associated with the treatment of BC, preventative measures such as educational strategies should also be considered to decrease the burden on the healthcare system and allow for more efficient policy prioritization.
Secondly, this analysis does not include productivity losses due to reduced work hours. Metastatic BC has been shown to severely impact productivity as working hours are reduced due to absenteeism resulting directly from the illness or as a side effect of the treatmentCitation42–44. A population-based study on work absence following BC diagnosis showed that patients, on average, took six months off following their diagnosisCitation45. As absenteeism was not accounted for in this current study design, the calculated productivity losses are in fact a conservative estimate of the economic losses due to BC. The current analysis, which only considers productivity losses resulting from premature mortality, estimated productivity losses in Poland to be approximately €85 million in 2019. A study on public finance burden attributable to BC in Poland estimated productivity losses at €583.7 million in 2010 and €699.7 million in 2014. Although the methodology was similar to the one utilized in this analysis, the productivity losses estimated were considerably higher as productivity losses were not limited to premature mortality but also accounted for absenteeism and disabilityCitation46. Additionally, the study considered the wider impact on the caregivers of patients with BC which is often overlookedCitation47. As such, if BC morbidity and caregiver burden were modeled, total productivity losses reported here would have been considerably higher for all countries. Although the current model illustrates the productivity losses resulting from premature BC mortality, the wider economic burden of this indication is not fully captured in the current analysis.
Although measures such as incidence and mortality are often used to prioritize disease areas for new policy, the measures used in this report expand on these commonly reported outcomes. For example, YLL as measure of mortality takes into account age of death, so it gives wider overview on mortality burden. Cancer polices should focus where the burden is the highest (in terms of number of deaths, and age at death) and therefore it is important that the measures used to inform these policies reflect these nuances. By further incorporating the YPLL and the associated cost, the model adds depth to these measures and provides a quantifiable societal view.
5. Conclusion
Major efforts are still required to reduce the gap in BC burden in Eastern Europe. This model estimated that BC resulted in a total of 247,373 years of potential life lost in 2019 in the countries included in the analysis: Bulgaria, Croatia, Czech Republic, Hungary, Poland, Romania, Serbia, Slovakia, and Slovenia. Across the nine countries, lost productivity costs due to premature BC-related mortality were substantial, exceeding €259 million in 2019 alone.
These estimates therefore illustrate the economic burden resulting from BC in this region and provides relevant insights that can be used to support the development of future evidence-based health policies to reduce this burden and to inform future decision-making in CEE countries. Identifying the burden caused by potentially preventable mortality in breast cancer further supports the need for investment in the prevention and treatment of this disease, and adds to the evidence base to show why the prevention of premature mortality in breast cancer should be prioritized.
Transparency
Declaration of funding
This work was funded by Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA.
Declaration of financial/other relationships
GB, CB, EK and SS are employees of MSD subsidiaries of Merck & Co., Inc., Rahway, NJ, USA and may own stocks and/or stock options in Merck & Co., Inc., Rahway, NJ, USA.
NC, RH and GW are employees of Adelphi Values (PROVE), paid consultants to MSD.
AM has no conflict of interest.
Reviewer disclosures
Peer reviewers on this manuscript have received an honorarium from JME for their review work but have no other relevant financial relationships to disclose.
Supplemental Material
Download MS Word (236 KB)Acknowledgements
None stated.
References
- Akram M, Iqbal M, Daniyal M, et al. Awareness and current knowledge of breast cancer. Biol Res. 2017;50(1):1–23.
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249.
- DeSantis CE, Bray F, Ferlay J, et al. International variation in female breast cancer incidence and mortality rates. Cancer Epidemiol Biomarkers Prev. 2015;24(10):1495–1506.
- Dass SA, Tan KL, Selva Rajan R, et al. Triple negative breast cancer: a review of present and future diagnostic modalities. Medicina. 2021;57(1):62.
- Gonzalez L, Mortimer J, Kruper L. De-escalation of systemic therapy for Early-Stage, Node-Negative Her2+ and Triple-Negative breast cancer. Curr Breast Cancer Rep. 2021;13(3):151–156.
- Yao H, He G, Yan S, et al. Triple-negative breast cancer: is there a treatment on the horizon? Oncotarget. 2017;8(1):1913–1924.
- Cancer Treatment Centers of America. Breast cancer molecular types; 2022 [accessed 2022 Oct]. Available from: https://www.cancercenter.com/cancer-types/breast-cancer/types/breast-cancer-molecular-types
- European Commission. Cancer in Europe: 5 things the data tells us; 2022 [accessed 2022 Jan]. Available from: https://joint-research-centre.ec.europa.eu/jrc-news/cancer-europe-5-things-data-tells-us-2022-01-13_en
- Dyba T, Randi G, Bray F, et al. The European cancer burden in 2020: incidence and mortality estimates for 40 countries and 25 major cancers. Eur J Cancer. 2021;157:308–347.
- Santucci C, Patel L, Malvezzi M, et al. Persisting cancer mortality gap between Western and Eastern Europe. Eur J Cancer. 2022;165:1–12.
- La Vecchia C, Conte P. Cancer control in Central and Eastern Europe. Oncologist. 2016;21(10):1161–1162.
- Vrdoljak E, Wojtukiewicz MZ, Pienkowski T, et al. Cancer epidemiology in Central, South and Eastern European countries. Croat Med J. 2011;52(4):478–487.
- Luengo-Fernandez R, Leal J, Gray A, et al. Economic burden of cancer across the European Union: a population-based cost analysis. Lancet Oncol. 2013;14(12):1165–1174.
- Inotai A, Abonyi-Tóth Z, Rokszin G, et al. Prognosis, cost, and occurrence of colorectal, lung, breast, and prostate cancer in Hungary. Value Health Reg Issues. 2015;7:1–8.
- Hanly P, Soerjomataram I, Sharp L. Measuring the societal burden of cancer: the cost of lost productivity due to premature cancer‐related mortality in Europe. Int J Cancer. 2015;136(4):E136–E145.
- European Commission. Europe’s Beating cancer plan. Brussels: European Commission; 2021.
- Bencina G, Chami N, Hughes R, et al. Lost productivity due to head and neck cancer mortality in Hungary, Poland, and Romania. J Cancer Policy. 2022;34:100366.
- Eurostat. Causes of death - deaths by country of residence and occurrence mortality estimates (2010, 2015 and 2019). 2021 [accessed 2021 Oct] Available from: https://ec.europa.eu/eurostat/web/health/data/database
- The World Bank. Life expectancy at birth, female (years). 2021 [accessed 2021 Oct] Available from: https://data.worldbank.org/indicator/SP.DYN.LE00.FE.IN
- The World Bank. Life expectancy at birth, male (years). 2021 [accessed 2021 Oct] Available from: https://data.worldbank.org/indicator/SP.DYN.LE00.MA.IN
- Eurostat. Mean annual earnings by sex, age and economic activity; 2018. Available from: https://ec.europa.eu/eurostat/databrowser/view/EARN_SES18_27__custom_1501377/default/table?lang=en
- Eurostat. Minimum wages. 2015 [accessed 2021 Oct]. Available from: https://ec.europa.eu/eurostat/databrowser/view/tps00155/default/table?lang=en
- The World Bank. Labor force participation rate, national estimate. 2019 [accessed 2021 Oct]. Available from: https://data.worldbank.org/indicator/SL.TLF.CACT.NE.ZS
- van Walle L, Vandeven J, Colpaert C, et al. Incidence of breast cancer subtypes in Belgium: a population-based study. Belg J Med Oncol. 2020;14(6):263–273.
- Eurostat. Unemployment rate; 2021 [accessed 2021 Oct]. Available from: https://ec.europa.eu/eurostat/databrowser/view/tepsr_wc170/default/table?lang=en
- Eurostat. Gross domestic product at market prices; 2017 [accessed 2021 Oct]. Available from: https://ec.europa.eu/eurostat/web/products-datasets/-/tec00001
- Eurostat. Mean annual earnings by sex, age and economic activity; 2018 [accessed 2021 Oct]. Available from: https://ec.europa.eu/eurostat/databrowser/view/EARN_SES18_27__custom_1501377/default/table?lang=en
- World Bank. Population, total; 2019 [accessed 2022 Jul]. Available from: https://data.worldbank.org/indicator/SP.POP.TOTL
- Hofmarcher T, Lindgren P, Wilking N, et al. The cost of cancer in Europe 2018. Eur J Cancer. 2020;129:41–49.
- Tripathy D, Curteis T, Hurvitz S, et al. Correlation between work productivity loss and EORTC QLQ-C30 and -BR23 domains from the MONALEESA-7 trial of premenopausal women with HR+/HER2− advanced breast cancer. Ther Adv Med Oncol. 2022;14:17588359221081203. 17588359221081203.
- Trogdon JG, Liu X, Reeder-Hayes KE, et al. Productivity costs associated with metastatic breast cancer in younger, midlife, and older women. Cancer. 2020;126(18):4118–4125.
- Shah TA, Guraya SS. Breast cancer screening programs: review of merits, demerits, and recent recommendations practiced across the world. J Microsc Ultrastruct. 2017;5(2):59–69.
- Blanks RG, Moss SM, McGahan CE, et al. Effect of NHS breast screening programme on mortality from breast cancer in England and Wales, 1990-8: comparison of observed with predicted mortality. BMJ. 2000;321(7262):665–669.
- Thornton J. Targeted breast screening could reduce overdiagnosis and be more cost effective, study finds. BMJ. 2018;362:k3009.
- Tong CW, Wu M, Cho WC, et al. Recent advances in the treatment of breast cancer. Front Oncol. 2018;8:227.
- Wojtyla C, Bertuccio P, Wojtyla A, et al. European trends in breast cancer mortality, 1980–2017 and predictions to 2025. Eur J Cancer. 2021;152:4–17.
- Trimboli RM, Giorgi Rossi P, Battisti NML, et al. Do we still need breast cancer screening in the era of targeted therapies and precision medicine? Insights Imaging. 2020;11(1):1–10.
- Breastcancer.org Adding Keytruda to chemotherapy improves overall survival in metastatic, strongly PD-L1-positive triple-negative breast cancer. 2021.
- Burguin A, Diorio C, Durocher F. Breast Cancer treatments: updates and new challenges. JPM. 2021;11(8):808.
- Anderson WF, Jatoi I, Tse J, et al. Male breast cancer: a population-based comparison with female breast cancer. J Clin Oncol. 2010;28(2):232–239.
- Schneider PP, Ramaekers BL, Pouwels X, et al. Direct medical costs of advanced breast cancer treatment: a real-world study in the southeast of the Netherlands. Value Health. 2021;24(5):668–675.
- Blinder V, Eberle C, Patil S, et al. Women with breast cancer who work for accommodating employers more likely to retain jobs after treatment. Health Aff. 2017;36(2):274–281.
- Bradley CJ. Economic recovery: a measure of the quality of cancer treatment and survivorship? Cancer Am Cancer Soc. 2015;121(24):4282–4285.
- Bradley CJ, Neumark D, Luo Z, et al. Employment-contingent health insurance, illness, and labor supply of women: evidence from married women with breast cancer. Health Econ. 2007;16(7):719–737.
- Drolet M, Maunsell E, Mondor M, et al. Work absence after breast cancer diagnosis: a population-based study. CMAJ. 2005;173(7):765–771.
- Łyszczarz B, Nojszewska E. Productivity losses and public finance burden attributable to breast cancer in Poland, 2010–2014. BMC Cancer. 2017;17(1):1–13.
- Wan Y, Gao X, Mehta S, et al. Indirect costs associated with metastatic breast cancer. J Med Econ. 2013;16(10):1169–1178.