
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Aims
To obtain appropriate health state utility values for cost-effectiveness analyses of new Mycobacterium avium complex pulmonary disease (MAC-PD) treatments. The impact of MAC-PD severity and symptoms on quality of life (QoL) also were quantified.
Methods
A questionnaire describing four health states, MAC-positive severe, MAC-positive moderate, MAC-positive mild, and MAC-negative, was developed based on St. George’s Respiratory Questionnaire (SGRQ) Symptom and Activity scores from the CONVERT trial. The time trade-off (TTO) method with ping-pong titration procedure was used to estimate health state utilities. Regression analyses assessed the impacts of covariates.
Results
Of 319 Japanese adults (49.8% female, mean age 44.8 years), mean (95% CI) health state utility scores (MAC-positive severe, MAC-positive moderate, MAC-positive mild, and MAC-negative) were 0.252 (0.194–0.310), 0.535 (0.488–0.582), 0.816 (0.793–0.839), and 0.881 (0.866–0.896), respectively. MAC-negative state utility scores were significantly higher than MAC-positive severe (mean difference [95% CI], 0.629 [0.574–0.684]), MAC-positive moderate (0.346 [0.304–0.389]), and MAC-positive mild (0.065 [0.048–0.082]) scores (p < .001 each). Most participants would trade survival duration to avoid MAC-positive states (97.5% to avoid MAC-positive severe; 88.7% MAC-positive moderate; 61.4% MAC-positive mild). Regression analyses to investigate the impact of background characteristics showed similar utility differences between health states when not adjusted for covariates.
Limitations
Some participant demographics differed from the general population; however, this did not impact utility differences among health states as regression analyses adjusting for demographics did not affect these differences. Similar investigations are needed among patients with MAC-PD and in other countries.
Conclusions
This study evaluating the impact of MAC-PD on utilities using the TTO method demonstrates that differences in utilities are dependent on the severity of respiratory symptoms and their impacts on daily activities and QoL. These results could contribute to a better quantification of the value of MAC-PD treatments and improve assessments of cost-effectiveness.
Introduction
Nontuberculous mycobacterial pulmonary disease (NTM-PD) is a rare, progressive, and sometimes life-threatening pulmonary disorder that is increasing in prevalence and incidence worldwide.Citation1–4 In Japan, NTM-PD incidence increased 2.6 fold from 2007 (5.7 cases/100,000 person-years) to 2014 (14.7 cases/100,000 person-years).Citation5 The prevalence of NTM-PD in Japan has been estimated to be up to 10 times the incidence, as a consequence of the intractable nature of the disease.Citation6 Mycobacterium avium complex pulmonary disease (MAC-PD), typically the result of infection with either Mycobacterium avium or Mycobacterium intracellulare, is the most common form of NTM-PD, accounting for 80–90% of NTM-PD cases in Japan.Citation2,Citation7,Citation8
MAC-PD diagnosis is based on the synthesis of clinical, radiographic, and microbiological data, as there is a lack of specific radiological findings or pulmonary symptoms.Citation9 Patients with MAC-PD may present with respiratory symptoms, such as refractory cough, excess sputum production, hemoptysis, and dyspnea, and/or systemic symptoms, such as fatigue, fever, and weight loss. However, these symptoms may vary between patients and are not specific for MAC-PD.Citation10 Consequently, patients with MAC-PD may experience delays in obtaining a definitive diagnosis.
Guideline-based treatment for patients with noncavitary nodular-bronchiectatic MAC-PD is long-term triple therapy (macrolide, ethambutol, and rifampicin), with add-on injectable aminoglycoside for severe/advanced nodular bronchiectatic, cavitary, or macrolide-resistant disease.Citation9 Between 20% and 40% of patients with MAC-PD are refractory to guideline-based treatmentCitation11–13 and for these patients (those without serum conversion) long-term triple therapy with an add-on amikacin liposome inhalation suspension (ALIS) is recommended.Citation9 Guideline-based treatment may be ineffective due to failure to induce culture conversion (an indicator of treatment success) or severe adverse side effects, which together contribute to poor treatment compliance, disease chronicity, relapse, and/or development of treatment-resistant NTM strains.Citation14–18
Despite the limitations associated with these treatment options, there were few advancements in treatment options for patients with MAC-PD until the recent approval of ALIS (in 2018 in the United States, and 2021 in Japan) as add-on therapy for the management of treatment-refractory MAC-PD. ALIS enables the non-intravenous administration of amikacin in the lungs via inhalation, which has been shown to increase drug concentration at the infected area while minimizing systemic exposure.Citation19,Citation20 The efficacy and safety of ALIS were assessed in the CONVERT phase III trial (NCT02344004) and open-label extension study (NCT02628600).Citation19,Citation21 In the phase III trial, significantly (p < .0001) more patients with refractory MAC-PD experienced culture conversion when treated with a multidrug background regimen together with ALIS (29.0%; 65/224) than when treated with background regimen alone (8.9%; 10/112).Citation19
Lung function and QoL are closely associated in patients with MAC-PD,Citation17 and the CONVERT trial also sought to assess changes in QoL via health state utility assessment using the EQ-5D-3L questionnaire. Health state utility measures can quantify the relative value of a patient’s QoL on a scale between 0 (equal to death) and 1 (equal to perfect health) which can then be used to calculate quality-adjusted life years in cost-effectiveness analyses.Citation22 These measures are useful in decision-making because they enable comparisons between various healthcare interventions.Citation23 However, in the CONVERT trial, EQ-5D-3L index score did not discriminate well between patients who did and patients who did not have clinically meaningful changes on four anchor variables (conversion status, percent predicted forced expiratory volume in 1 s, SGRQ scores, and 6-Minute Walk Test).Citation24 This lack of discriminatory ability was evidenced by a large degree of overlap in cumulative distribution function curves, similar changes in EQ-5D-3L VAS scores for all anchors, and a median change of 0 in EQ-5D-3L index scores for both the responder and non-responder groups.Citation24 Poor responsiveness to clinically meaningful changes indicates that the EQ-5D-3L instrument may not be appropriate for evaluating changes in health-related QoL over time in patients with refractory MAC-PD.Citation24 As such, there is a need for alternative tools to assess QoL changes in this patient population.
The time trade-off (TTO) method is a direct method of analysis which obtains the value of health states from a general population, rather than from patients with the disease of interest. This method is recommended by Japanese guidelines for cost-effectiveness evaluations as an accepted methodology for estimating health state utilities.Citation25 Specifically, Japanese guidelines for cost-effectiveness evaluations accept the TTO method when it is difficult to directly obtain utility values from patients.Citation25 In many aspects, the TTO method is considered more sensitive to specific disease and health states than the EQ-5D-3L.Citation26 This is partly because, unlike the EQ-5D-3L which measures health status “today”, the TTO method can assess intermittent and discontinuous symptoms, as are many of those experienced by patients with MAC-PD, through the use of vignettes.Citation26 Vignettes (also known as scenarios or health state descriptions) have been widely used in health economic models to elicit individuals’ preferences on QoL measures.Citation27–29 It is useful to incorporate vignettes into TTO methodology to describe disease conditions, treatments, and their impacts on various domains of health-related QoL. The EQ-5D-5L and other preference-based measures which obtain data from patients directly could solve the limitation of the EQ-5D-3L, but MAC-PD is a rare disease and it is difficult to collect an adequate number of samples. Therefore, we have used the TTO method in a general population sample for the present study.
This study aimed to obtain more appropriate QoL values for conducting cost-effectiveness analyses than those estimated by the EQ-5D-3L. In addition, the impact on QoL of MAC-PD disease severity and symptom changes associated with culture conversion were estimated, and those QoL impacts which may have value in health economic analyses were quantified.
Methods
Overview of study design
In this study, an interview questionnaire was administered to participants from the general public in Japan using a TTO method based on vignettes describing MAC-PD patients’ symptoms and daily lives. Questionnaire development and data collection were based on the methodology recommended by Matza et al.Citation26 Multiple health state descriptions for patients with MAC-PD, defined by disease severity and sputum culture status, were developed based on SGRQ symptom scores (assessing the impact of respiratory symptoms) and activity scores (assessing the impact of disease on mobility and physical activity) using data from the CONVERT trial post-hoc analysis for the present study.Citation30–32 Pilot interviews were conducted online in 20 participants to confirm comprehension prior to finalizing the questionnaire. After finalizing the questionnaire to reflect feedback from pilot interview respondents, the main survey was conducted face-to-face. Interviewers who had been pretrained with an interview guide conducted in person, one-on-one interviews with study participants using a standard script to collect health state utility scores and brief demographic and clinical background information. Participants answered the interview questions while looking at a computer screen and paper materials illustrating each question. All health states were presented to all participants and utility scores were assessed. It was explained to participants that the disease presented in the questionnaire was: a chronic, slowly progressive respiratory infection; a bacterial infection and not a viral infection like COVID-19 or influenza; and not an infectious disease that can be transmitted from person to person. Before the survey was administered, informed consent was obtained from all participants (both pilot survey respondents and final interview participants). Prior to undertaking the main TTO tasks, participants were asked the following questions to ensure they sufficiently understood the disease and TTO concept: (1) impression of the study attributes of the health state description (i.e. duration of survival, symptom and impact on daily activity) in advance; (2) trade-off task between duration of survival and symptoms; (3) TTO training for living in a wheelchair. The TTO method with a ping-pong titration procedure (in which a survival time of up to 10 years is increased or decreased in increments of 1 year) was used to estimate health state utilities.Citation33 If living 10 years in the health state was evaluated to be worse than living 0 years in full health (i.e. dying now), then the lead-time TTO method was used to evaluate the health state. In the lead-time TTO method, respondents compared living 10 years in a health state to be evaluated after 10 years in full health with living 0–10 years in full health. The TTO method, rather than the standard gamble method, was used to enhance the comparability of results from the present study with the EQ-5D, and a survival length of 10 years was adopted as it is similar to the time horizons used to derive scoring tariffs for the EQ-5D as recommended by Matza et al.Citation26
Health state development and validation
Scenarios were developed as health state descriptions of patients with MAC-PD to be presented in the TTO tasks. To reduce the survey participation burden and increase participant engagement, we included 4 clinically meaningful scenarios based on the distribution of SGRQ data from the CONVERT trial.Citation30 Of the 4 scenarios based on SGRQ data, three (corresponding to Symptom and Activity score terciles at baseline) were defined: a MAC-positive severe state, a MAC-positive moderate state, and a MAC-positive mild state. A MAC-negative state then was defined using the median Symptom and Activity score of the 80% of patients who had achieved culture conversion (i.e. were MAC-negative) at 12 months after treatment initiation. The health state descriptions were developed by selecting SGRQ wording that corresponded to the Symptom and Activity scores excluding the Impact score because Impact score items are considered sensitive to the patient’s individual condition. Activity and Symptom scores for each scenario are shown in and the health state descriptions for each are shown in Supplementary Tables 1–4. The SGRQ was developed as a disease-specific, health-related QoL measure in asthma and chronic obstructive pulmonary disease (COPD), and is capable of evaluating changes over time in disease symptoms and the social and psychological impacts of such symptoms. This questionnaire consists of 50 items, which are divided into three components (Symptom, Activity, and Impact) and calculates a score for each and a total sum of the 3 scores.Citation34,Citation35 The SGRQ has also been validated as a QoL measure in other chronic respiratory diseases in addition to asthma and COPD and has been validated as a measure of respiratory manifestations in MAC-PD.Citation10,Citation36 Furthermore, the Japanese version of the SGRQ has also been validated.Citation37
Table 1. Assumed SGRQ scores for each health state.
Table 2. Social and demographic background characteristics.
Table 3. Clinical background of participants and comparison with the general population.
Table 4. Comparison of health state utilities.
Survey procedure
A pilot survey of 20 participants was conducted prior to the main survey to ascertain whether the health state descriptions were clear and understandable to the general public, to identify and address potential problems that may arise in the data collection process, and to estimate the number of valid responses that could be expected from the main survey. The procedure for conducting the pilot survey was as follows:
Pilot survey participants were selected from all survey candidates based on eligibility criteria.
Pilot surveys were conducted via an online interview.
Upon completing the pilot survey, participants provided feedback on their understanding of the health state descriptions and survey procedures.
The main survey was conducted in face-to-face interviews with 16 trained interviewers and two supervisors who provided quality checks over the four days of data collection. Both the pilot survey and the main survey were conducted in Tokyo, Japan, during the daytime between November 26 and 30, 2021 and took about one hour per respondent to complete. These surveys were conducted by Intage Healthcare Inc, a company with expertise in market research and data collection. After the interviews, cash vouchers worth 5,000 JPY (Japanese yen) were provided to respondents in compensation for research cooperation expenses.
Survey participants
As utilities used in health economic evaluations should reflect the values of the general population,Citation23 this survey was conducted in the general Japanese population rather than in patients with MAC-PD. Participants were adults aged ≥20 years who were living in Japan at the time of screening. Those who had difficulty granting consent or completing the questionnaire due to low Japanese language skills were excluded. The target sample size was 150–300 participants, which was considered sufficient for utility estimation based on previous studies using the TTO method.Citation38–40 Snowball sampling from a list of potential collaborators maintained by the survey company was used to identify candidates who then were contacted by e-mail to request their participation in the main survey. Sampling was adjusted to evenly distribute respondents by gender and age. We used an equal recruitment method for each age group rather than recruiting subjects according to the composition of the Japanese population to avoid introducing bias. As Japan currently has a highly aged population, a sample reflecting the age distribution of the general population would likely skew the results by giving greater weight to the values of particular groups.
Statistical procedure
All statistical analyses were performed using SAS Version 9.4 (SAS Institute, Cary, NC). A p-value of <.05 on both sides was considered statistically significant. Missing values were not imputed. Participants’ social and clinical background data were summarized by means and standard deviations (SDs) for continuous variables, and frequencies and percentages for categorical variables.
In the TTO survey, health state utility scores for health states that were not evaluated as “worse than death” were calculated using the following formula, with death (0) to full health (1) as the anchor:
Where x and y are the respective survival durations at which the combinations of the two health conditions and survival durations were judged by the participants to be equivalent by the ping-pong titration method, or the average survival durations for each health state at two points when the superiority of the two combinations was reversed. The utility scores for health states evaluated as “worse than death” were calculated based on the following formula. In this case, utility could range from 0 to −1:
Where x′ is the survival duration only in full health when the combinations of the two health conditions and survival durations were judged by the participants to be equivalent, or the average survival duration only in full health at two points when the superiority of the two combinations was reversed (Supplemental Figure 1).
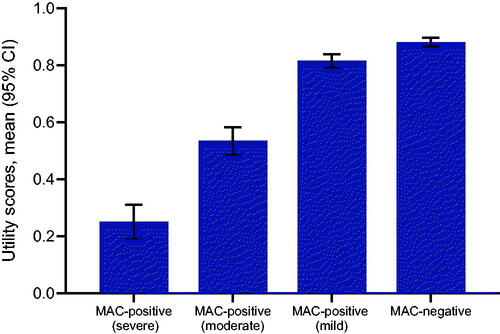
Figure 1. Utility scores were calculated for each health state. Abbreviations. CI, confidence interval; MAC, Mycobacterium avium complex; SD, standard deviation; SGRQ, St. George’s Respiratory Questionnaire.
Means, SDs, medians, and 95% confidence intervals (CIs) were calculated for the estimated health state utilities and differences in utilities between health conditions. Utilities were compared by paired t-test. Subgroup analyses by median age (46 years), sex, median educational background (college graduate), or employment status (full-time and part-time employees were defined as employed) also were performed for health state utilities and compared by t-test. The order of utility, willingness to trade time, and rates of positive/negative utilities also were calculated to characterize the health state utilities.
To confirm the robustness of estimated utility differences between health states, the impacts of covariates such as social and clinical background data were estimated by regression analyses. As in previous studies, ordinary least squares and Tobit models were used to generate estimates using disutility (calculated as 1 − utility) as the dependent variable and health states as the explanatory variable with the MAC-negative state set as the reference.Citation38 All social and clinical background data were entered as covariates and selected using the stepwise forward selection method. R-square and mean absolute error were used to check the goodness of fit of each model. Regarding the validity of the models, the ordinary least squares model has the advantage of not having to assume a distribution while utility scores had heteroscedasticity due to their being in the −1 to 1 range, with larger residuals when the utility was near the lower or upper limit. On the other hand, while the Tobit model can handle truncated data, utility values were generally normal in the range above 0 but the distribution was skewed to values close to −1 in the range below 0.
Evaluation of TTO validity for estimating utility values in previous studies
In November 2022, we performed a Medline literature review of studies including both the SGRQ and utilities obtained from EQ-5D to investigate issues regarding EQ-5D data and to identify evidence regarding the validity of TTO utility estimates. The clinical questions of this literature search were: population = patients with pulmonary diseases, intervention = not applicable, comparator = not applicable, outcome = SGRQ score and utilities measured by EQ-5D, study type = any clinical trials, observational studies and mapping analysis research studies which reported SGRQ score and QoL as measured by preference-based methods. This literature review included patients with pulmonary diseases but was not limited to MAC-PD in order to evaluate the association between SGRQ score and QoL as measured by EQ-5D. The search formula used in this literature review is shown in Supplemental Table 5.
Table 5. Rates of utility differences between select pairs of health states.
Ethical approval and informed consent
This study was conducted in accordance with the Ethical Guidelines for Medical and Biological Research Involving Human SubjectsCitation41 and was reviewed and approved by the nonprofit organization MINS Research Ethics Committee (20-9-401, 5-Chome, Mita, Minato-ku, Tokyo).
Results
Background information of sample group
A total of 319 participants were screened and completed the survey. The participants were 49.8% female with a mean age of 44.8 years old (). Over half (54.2%) of the survey population had graduated from university as their highest educational qualification which is a greater proportion than in the Japanese general population (22.1%).Citation42 Consequently, the number whose highest qualification was senior or junior high school graduate was lower than in the general population. In terms of employment, 63.5% of participants were employed (50.2% fulltime; 13.2% part-time) which is higher than in the Japanese general population (31.6% and 9.4%, respectively) (). Almost all participants (n = 311, 97.5%) had never been diagnosed with MAC-PD, COVID-19, or any other chronic respiratory disease, while one participant (0.3%) had previously been diagnosed with MAC-PD. The most frequently reported health conditions were hypertension (6.6%), allergic rhinitis (4.4%), and stiff shoulders (3.1%) ().
Health state utilities
Mean (95% CI) utility scores for health states based on SGRQ data (MAC-positive severe state, MAC-positive moderate state, MAC-positive mild state, and MAC-negative state) were 0.252 (0.194–0.310), 0.535 (0.488–0.582), 0.816 (0.793–0.839), and 0.881 (0.866–0.896), respectively (). Utility scores were significantly higher in the MAC-negative state compared with the MAC-positive severe (mean difference [95% CI], 0.629 [0.574–0.684]), MAC-positive moderate (0.346 [0.304–0.389]), and MAC-positive mild (0.065 [0.048–0.082]) states with p < .001 for each (). The distribution of utility scores for each health state are shown in Supplemental Figure 4.
With a few exceptions (0.6%–4.4% of participants), most participants gave the MAC-negative state a utility score that was higher than or equivalent to the MAC-positive state (). The majority of participants were willing to trade survival duration to avoid the MAC-positive states (97.5% to avoid MAC-positive severe; 88.7% to avoid MAC-positive moderate; 61.4% to avoid MAC-positive mild). All participants judged the MAC-negative state to be preferable or equivalent to death. The MAC-positive severe state and MAC-positive moderate state were judged to be worse than death by 14.7% and 4.4% of participants, respectively (). Regarding the one participant who valued the MAC-negative state as equal to death, we considered this response in the context of other valuation studies that we have conducted in which some respondents expressed the desire to die as soon as possible should their sense of well-being become poor.
Table 6. Willingness to trade time and rates of positive and negative utilities.
Subgroup comparison
Utility scores tended to be lower among older participants (aged ≥46 years) in all health states, although this was significant only for the MAC-positive severe health state (). There were no statistically significant differences between subgroups by sex, educational background, or employment status.
Table 7. Health state utilities based on SGRQ data by subgroups.
Regression analysis
Results of regression analyses using the ordinary least squares and Tobit models are shown in . Among the covariates, age, hospital visits for ocular diseases, and hospital visits for hypertension were selected. There were almost no differences in terms of the impacts of health states on utility scores in either model, and scores for health states were similar to differences in utility scores between health states as shown in with almost no impact of any covariate.
Table 8. Estimation of utilities by regression analyses.
Evaluation of TTO validity for estimating utility values in previous studies
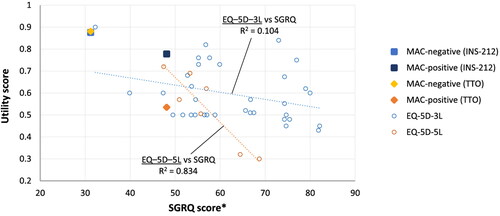
The PRISMA flowchart is shown in Supplemental Figure 3. The Medline search identified 18 publications which reported SGRQ Symptom scores, Activity scores, and EQ-5D scores and clearly distinguished whether the EQ-5D-3L or EQ-5D-5L was used (Supplemental Table 6). Scatter plots for the association of utility with mean Symptom and Activity scores reported in these publications and plots of TTO estimates for MAC negativity and MAC positivity (moderate) as estimated in the current study are shown in . If measured multiple times within the same publication, the respective data were plotted. COPD accounted for 87.8% of cases and interstitial lung diseases, emphysema, acute respiratory distress syndrome, and pulmonary tuberculosis also were reported. Scatter plots demonstrated that QoL values of EQ-5D-3L were highly variable even if the SGRQ score was the same (e.g. SGRQ ranged from 70 to 80 for EQ-5D-3L's QoL of 0.4–0.8). The coefficients of determination (R2) for EQ-5D-3L and SGRQ were 0.104.
Figure 2. SGRQ scores and QoL values of EQ-5D delivered from selected literatures in literature review, CONVERT trial, and QOL values from MAC-negative and MAC-positive with moderate grade in TTO method. Abbreviations. MAC, Mycobacterium avium complex; SGRQ, St. George’s Respiratory Questionnaire. *Mean value of the Activity and Symptom scores of SGRQ.
Discussion
Many patients with NTM-PD have poor QoL, which is closely associated with the severity of their pulmonary and physical functioning and radiological scores.Citation10,Citation17,Citation43–45 Effective use of guideline-based therapy with triple therapy can improve NTM-PD symptoms and help to achieve treatment goals.Citation9,Citation46 While the ultimate goal of therapy is to achieve and maintain negative culture conversion (i.e. microbiological cure), this is challenging for the many patients with refractory disease.Citation44 In these patients, treatment goals focus on relieving symptoms, radiological findings, and QoL.Citation44 Given the importance of QoL, for patients and as an indicator of the response to treatment, QoL measures used for patients with NTM-PD should assess domains that adequately reflect those conditions specific to this population. As prior studies have suggested that the EQ-5D-3L may not accurately capture changes in QoL over time in patients with MAC- or NTM-PD, who often experience cycles of improvement/exacerbation, there is a need for new utilities to assess QoL in this population.Citation24,Citation47 Hong et al. compared the results of measuring QoL using EQ-5D in patients with NTM-PD including MAC-PD using the general population as a control.Citation47 In this report, there were no significant differences between patients with NTM-PD and controls in EQ-5D index score while, on the other hand, there were significant differences in VAS score. In addition, the EQ-5D index and VAS scores were largely discrepant in patients with severe NTM-PD with FEV1 of 50 or less. From these findings, Hong et al. conclude that EQ-5D is not a useful measure for assessing QoL in patients with NTM-PD.Citation47 Efthymiadou et al. also reported that the EQ-5D did not capture key aspects of QoL among patients with various chronic illnesses, including pulmonary diseases, and had particular difficulty capturing fatigue which is one of the most common symptoms impacting patient QoL.Citation48
Scatter plots from the Medline literature review showed that QoL values measured by the EQ-5D-3L were highly variable (SGRQ ranged from 70 to 80 for EQ-5D-3L's QoL of 0.4–0.8). Furthermore, the coefficients of determination for EQ-5D-3L and SGRQ were low (0.104), suggesting that EQ-5D-3L may not properly assess respiratory diseases when compared to measures obtained by the SGRQ. It is unlikely that our utilities as estimated by TTO methodology (the blue square and orange diamond in ) have unduly overestimated clinically relevant changes in MAC-PD for the following reasons: (1) the recall interval of the TTO was sufficient to evaluate symptoms of chronic respiratory diseases, and (2) the plot of utility as estimated by the TTO method did not deviate significantly from the plot of data in previous studies.
Utility scores for patients with MAC-PD estimated in this study decreased with increasing disease severity, with all MAC-positive states having significantly lower utilities than the MAC-negative state. In addition, regression analyses using the ordinary least squares and Tobit models with demographic and clinical background data as covariates showed that the regression coefficients for health states were comparable to the differences in utility scores between health states. These findings are consistent with other studies assessing QoL in patients with NTM-PD. Kawahara et al. found that worse lung function, radiological findings, and exercise tolerance all were significantly associated with lower SGRQ scores.Citation44 Mehta et al. found that QoL among patients with NTM-PD (N = 51) was significantly impaired compared with a general population and that low QoL scores were more closely associated with poor lung function than with age, sex, or other comorbid pulmonary conditions.Citation17
The results of the current study may be relevant both to physicians making treatment decisions and public health agencies allocating resources in light of the fact that significantly worse pulmonary outcomes, higher hospitalization rates, and higher healthcare costs are observed among patients with NTM-PD who receive non-guideline-based therapy regimens compared with those receiving guideline-based therapy as recommended.Citation14,Citation16,Citation46,Citation49
While this is the first study to use the TTO method for estimating utilities in patients with MAC-PD, the results are consistent with a prior TTO analysis by Cho et al. that estimated utilities in COPD.Citation22 This study included a survey of the general population using COPD health state descriptions of different severities defined by six dimensions: (i) extent of dyspnea; (ii) impact on nonstrenuous activities; (iii) impact on strenuous activities; (iv) ability to work; (v) anxiety and depression; and (vi) energy and tiredness.Citation22 The estimated utilities were 0.824, 0.646, and 0.305 for moderate, severe, and very severe disease, respectivelyCitation22; these utility values are close (less than or equal to about 0.1 differences) to those estimated in this study for mild, moderate, and severe MAC-positive states based on SGRQ data. The SGRQ can be used for QoL evaluation in chronic respiratory diseases other than COPD, including MAC-PD.Citation10,Citation36,Citation44,Citation45 Although some of the SGRQ questions are specific to COPD, most of the questions in the Activity and Impact components are related to dyspnea and associated activity limitations and are not disease specific. This indicates that COPD and MAC-PD have similar symptoms, functional impairments, and burdens. In addition, MAC-PD patients frequently have comorbid COPD].Citation50,Citation51 Therefore, the utility values of both diseases are likely to be close.
Limitations
There were differences in the demographic characteristics of the survey population and the general population of Japan, with higher proportions of study participants having university-level education and being employed fulltime. However, any effect of these demographic differences on the generalizability is assumed to be small, because there is no inconsistency of utility estimates among participants with different educational levels and employment status. Furthermore, demographic characteristics did not affect differences in utilities among health states as shown by the regression analysis. This study was conducted in the general population, so it is unclear if similar utility differences between disease severity states exist among patients with MAC-PD.Citation23 In addition, health state utilities are influenced by culture and can vary between countries.Citation50 Thus, similar investigations are needed in populations of patients with MAC-PD and in other countries. In addition to the above, we recognize that this study includes other potential limitations including the possibility of interviewer effects (e.g. it is preferable to use fewer interviewers) and uncertainty regarding participants’ understanding of the TTO tasks as we did not use the EuroQol Valuation Technology (EQ-VT) or another similar data control tool.Citation52,Citation53 We did not exclude outlier responses (i.e. those answering that a MAC positive status was equal to or higher than a MAC negative status) because we have not obtained other definitive evidence to conclude that these data are inappropriate, and the total amount of such data was small.
Conclusions
This is the first study to evaluate the impact of MAC-PD on utilities using the TTO method. We believe that the study solves several limitations of previous estimates obtained using the EQ-5D-3L because that instrument does not sufficiently capture changes in QoL over time as experienced by patients with MAC-PD. Although there are still potential limitations to using the TTO method, the results of this study could nevertheless contribute to a better quantification of the value of treatments for MAC-PD and facilitate more thorough cost-effectiveness assessments.
Transparency
Author contributions
TM, KM, and MY: Conceptualization, methodology, and design; TM: Data acquisition; TM, FM, MH, and JF: Data analysis and interpretation; TM: Drafting publication.
Reviewer disclosures
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Previous presentations
The contents of this article have not been previously presented.
Supplemental Material
Download MS Word (259.8 KB)Acknowledgements
Andrew Jackson, medical writer of MIMS Japan Co., Ltd., conducted a language quality check of the draft manuscript. Medical writing support was provided by Kat Hendrix, PhD of Curo Consulting, a division of Envision Pharma Group, and funded by Insmed Incorporated.
Declaration of funding
This study was sponsored by Insmed GK.
Disclosure statement of financial/other interests
TM is a fulltime employee of CRECON Medical Assessment Inc, paid consultants for Insmed Godo Kaisha. KM has received consulting fees from Insmed, and honoraria for educational lectures from Insmed Godo Kaisha. FM is a fulltime employee of CRECON Medical Assessment Inc, paid consultants for Insmed Godo Kaisha. MY is a full-time employee of Insmed Godo Kaisha and a shareholder of Insmed Incorporated. JF and MH are full-time employees and shareholders of Insmed Incorporated.
References
- Diel R, Lipman M, Hoefsloot W. High mortality in patients with Mycobacterium avium complex lung disease: a systematic review. BMC Infect Dis. 2018;18(1):206.
- Furuuchi K, Morimoto K, Yoshiyama T, et al. Interrelational changes in the epidemiology and clinical features of nontuberculous mycobacterial pulmonary disease and tuberculosis in a referral hospital in Japan. Respir Med. 2019;152:74–80.
- Izumi K, Morimoto K, Hasegawa N, et al. Epidemiology of adults and children treated for nontuberculous mycobacterial pulmonary disease in Japan. Ann Am Thorac Soc. 2018;16:341–347.
- Marras TK, Mendelson D, Marchand-Austin A, et al. Pulmonary nontuberculous mycobacterial disease, Ontario, Canada, 1998–2010. Emerg Infect Dis. 2013;19:1889–1891.
- Namkoong H, Kurashima A, Morimoto K, et al. Epidemiology of pulmonary nontuberculous mycobacterial disease, Japan. Emerg Infect Dis. 2016;22(6):1116–1117.
- Morimoto K, Iwai K, Uchimura K, et al. A steady increase in nontuberculous mycobacteriosis mortality and estimated prevalence in Japan. Ann Am Thorac Soc. 2014;11(1):1–8.
- Ito Y, Hirai T, Fujita K, et al. Increasing patients with pulmonary Mycobacterium avium complex disease and associated underlying diseases in Japan. J Infect Chemother. 2015;21(5):352–356.
- Morimoto K, Hasegawa N, Izumi K, et al. A laboratory-based analysis of nontuberculous mycobacterial lung disease in Japan from 2012 to 2013. Ann Am Thorac Soc. 2017;14(1):49–56.
- Daley CL, Iaccarino JM, Lange C, et al. Treatment of nontuberculous mycobacterial pulmonary disease: an official ATS/ERS/ESCMID/IDSA clinical practice guideline. Eur Respir J. 2020;56:2000535.
- Maekawa K, Ito Y, Oga T, et al. High-resolution computed tomography and health-related quality of life in Mycobacterium avium complex disease. Int J Tuberc Lung Dis. 2013;17(6):829–835.
- Diel R, Nienhaus A, Ringshausen FC, et al. Microbiologic outcome of interventions against mycobacterium avium complex pulmonary disease: a systematic review. Chest. 2018;153(4):888–921.
- Lee BY, Kim S, Hong Y, et al. Risk factors for recurrence after successful treatment of Mycobacterium avium complex lung disease. Antimicrob Agents Chemother. 2015;59(6):2972–2977.
- van Ingen J, Obradovic M, Hassan M, et al. Nontuberculous mycobacterial lung disease caused by Mycobacterium avium complex – disease burden, unmet needs, and advances in treatment developments. Expert Rev Respir Med. 2021;15(11):1387–1401.
- Aliberti S, Sotgiu G, Castellotti P, et al. Real-life evaluation of clinical outcomes in patients undergoing treatment for non-tuberculous mycobacteria lung disease: a ten-year cohort study. Respir Med. 2020;164:105899.
- Boyle DP, Zembower TR, Qi C. Relapse versus reinfection of Mycobacterium avium complex pulmonary disease. Patient characteristics and macrolide susceptibility. Ann Am Thorac Soc. 2016;13(11):1956–1961.
- Kumar K, Daley CL, Griffith DE, et al. Management of Mycobacterium avium complex and Mycobacterium abscessus pulmonary disease: therapeutic advances and emerging treatments. Eur Respir Rev. 2022;31:210212.
- Mehta M, Marras TK. Impaired health-related quality of life in pulmonary nontuberculous mycobacterial disease. Respir Med. 2011;105:1718–1725.
- van Ingen J, Wagner D, Gallagher J, et al. Poor adherence to management guidelines in nontuberculous mycobacterial pulmonary diseases. Eur Respir J. 2017;49:1601855.
- Griffith DE, Eagle G, Thomson R, CONVERT Study Group, et al. Amikacin liposome inhalation suspension for treatment-refractory lung disease caused by Mycobacterium avium complex (CONVERT). a prospective, open-label, randomized study. Am J Respir Crit Care Med. 2018;198(12):1559–1569.
- Insmed Incorporated. ARIKAYCE® (amikacin liposome inhalation suspension) for oral inhalation use [prescribing information]. Bridgewater (NJ): Insmed Incorporated; 2018. [cited 2022 Oct 26]. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/207356s000lbl.pdf
- Winthrop KL, Flume PA, Thomson R, et al. Amikacin liposome inhalation suspension for Mycobacterium avium complex lung disease: a 12-month open-label extension clinical trial. Ann Am Thorac Soc. 2021;18(7):1147–1157.
- Cho S, Kim H, Kim SH, et al. Utility estimation of hypothetical chronic obstructive pulmonary disease health states by the general population and health professionals. Health Qual Life Outcomes. 2015;13:34.
- Rowen D, Mulhern B, Banerjee S, et al. Comparison of general population, patient, and carer utility values for dementia health states. Med Decis Making. 2015;35(1):68–80.
- Shah A, Ng X, Shah R, et al. Psychometric validation of the EQ-5D-3L in patients with nontuberculous mycobacterial (NTM) lung disease caused by Mycobacterium avium complex (MAC). Patient Relat Outcome Meas. 2021;12:45–54.
- Center for Outcomes Research and Economic Evaluation for Health National Institutes of Public Health C2H. Guideline for preparing cost-effectiveness evaluations to the central social insurance medical council. Tokyo, Japan: National Institute of Public Health (C2H); 2022. Available from: https://c2h.niph.go.jp/tools/guideline/guideline_en.pdf
- Matza LS, Stewart KD, Lloyd AJ, et al. Vignette-based utilities: usefulness, limitations, and methodological recommendations. Value Health. 2021;24(6):812–821.
- Hall F, de Freitas HM, Kerr C, et al. Estimating utilities/disutilities for high-risk metastatic hormone-sensitive prostate cancer (mHSPC) and treatment-related adverse events. Qual Life Res. 2019;28(5):1191–1199.
- Lloyd A, Piglowska N, Ciulla T, et al. Estimation of impact of RPE65-mediated inherited retinal disease on quality of life and the potential benefits of gene therapy. Br J Ophthalmol. 2019;103(11):1610–1614.
- Matza LS, Deger KA, Vo P, et al. Health state utilities associated with attributes of migraine preventive treatments based on patient and general population preferences. Qual Life Res. 2019;28(9):2359–2372.
- Insmed Incorporated. CONVERT trial: data on file. Bridgewater (NJ): Insmed Incorporated; 2021.
- Leitman A. NTM lung disease: patient experiences and preferences. FDA public workshop: development of antibacterial drugs for treatment of nontuberculous mycobacterial disease. Silver Spring (MD): U. S. Food and Drug; 2019. [cited 2022 Sept 1]. Available from: https://www.fda.gov/media/124058/download
- Pravosud V, Mannino DM, Prieto D, et al. Symptom burden and medication use among patients with nontuberculous mycobacterial lung disease. Chronic Obstr Pulm Dis. 2021;8(2):243–254.
- Devlin NJ, Tsuchiya A, Buckingham K, et al. A uniform time trade off method for states better and worse than dead: feasibility study of the ‘lead time’ approach. Health Econ. 2011;20:348–361.
- Jones PW, Quirk FH, Baveystock CM, et al. A self-complete measure of health status for chronic airflow limitation. The St. George’s Respiratory Questionnaire. Am Rev Respir Dis. 1992;145:1321–1327.
- Saint George’s University of London. St. George’s Respiratory Questionnaire. 2022 [cited 2022 Dec 11]. Available from: https://www.sgul.ac.uk/research/research-operations/research-administration/st-georges-respiratory-questionnaire/sgrq
- Ogawa T, Asakura T, Suzuki S, et al. Longitudinal validity and prognostic significance of the St George’s Respiratory Questionnaire in Mycobacterium avium complex pulmonary disease. Respir Med. 2021;185:106515.
- Hajiro T, Nishimura K, Tsukino M, et al. Comparison of discriminative properties among disease-specific questionnaires for measuring health-related quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157:785–790.
- Mukuria C, Rowen D, Brazier JE, et al. Deriving a preference-based measure for myelofibrosis from the EORTC QLQ-C30 and the MF-SAF. Value Health. 2015;18:846–855.
- Mulhern B, Rowen D, Jacoby A, et al. The development of a QALY measure for epilepsy: NEWQOL-6D. Epilepsy Behav. 2012;24:36–43.
- Rowen D, Mulhern B, Banerjee S, et al. Estimating preference-based single index measures for dementia using DEMQOL and DEMQOL-Proxy. Value Health. 2012;15:346–356.
- Ministry of Education Culture, Sports, Science and Technology, Ministry of Health, Labour and Welfare, and Ministry of Economy, Trade and Industry. Ethical guidelines for medical and biological research involving human subjects (in Japanese). Tokyo: Ministry of Education, Culture, Sports, Science and Technology, Ministry of Health, Labour and Welfare; 2022. [cited 2022 Jan 4]. Available from: https://www.mhlw.go.jp/content/000757566.pdf
- Japan Statistics Bureau of the Ministry of Internal Affairs and Communications. Table 2–1. Population by male and female, age/education, employment status/jobs (15 years old and over) – Japan. e-Stat Japan in statistics. Tokyo: National Statistics Center; 2017. [cited 2022 Sept 28]. Available from: https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00200532&tstat=000001107875&cycle=0&tclass1=000001107876&tclass2=000001107877&tclass3val=0
- Asakura T, Funatsu Y, Ishii M, et al. Health-related quality of life is inversely correlated with C-reactive protein and age in Mycobacterium avium complex lung disease: a cross-sectional analysis of 235 patients. Respir Res. 2015;16:145.
- Kawahara K, Tabusadani M, Yamane K, et al. Health-related quality of life associates with clinical parameters in patients with NTM pulmonary disease. Int J Tuberc Lung Dis. 2021;25:299–304.
- Yagi K, Asakura T, Namkoong H, et al. Association between six-minute walk test parameters and the health-related quality of life in patients with pulmonary Mycobacterium avium complex disease. BMC Pulm Med. 2018;18:114.
- Fukushima K, Kitada S, Komukai S, et al. First line treatment selection modifies disease course and long-term clinical outcomes in Mycobacterium avium complex pulmonary disease. Sci Rep. 2021;11:1178.
- Hong JY, Lee SA, Kim SY, et al. Factors associated with quality of life measured by EQ-5D in patients with nontuberculous mycobacterial pulmonary disease. Qual Life Res. 2014;23:2735–2741.
- Efthymiadou O, Mossman J, Kanavos P. Health related quality of life aspects not captured by EQ-5D-5L: results from an international survey of patients. Health Policy. 2019;123(2):159–165.
- Marras TK, Mirsaeidi M, Vinnard C, et al. Guidelines-based treatment associated with improved economic outcomes in nontuberculous mycobacterial lung disease. J Med Econ. 2019;22:1126–1133.
- Ringshausen FC, Wagner D, de Roux A, et al. Prevalence of nontuberculous mycobacterial pulmonary disease, Germany, 2009–2014. Emerg Infect Dis. 2016;22:1102–1105.
- Mahlich J, Dilokthornsakul P, Sruamsiri R, et al. Cultural beliefs, utility values, and health technology assessment. Cost Eff Resour Alloc. 2018;16:19.
- Purba FD, Hunfeld JAM, Iskandarsyah A, et al. Employing quality control and feedback to the EQ-5D-5L valuation protocol to improve the quality of data collection. Qual Life Res. 2017;26:1197–1208.
- Ramos-Goñi JM, Oppe M, Slaap B, et al. Quality control process for EQ-5D-5L valuation studies. Value Health. 2017;20:466–473.
- Insmed I. CONVERT trial: data on file. Bridgewater (NJ): Insmed Incorporated; 2021.
- Japan MoHLaW. [Comprehensive Survey of Living Conditions 2019] (Japanese). Tokyo: Director General for Statistics and Information Policy; 2020 [cited 26 Oct 2022]. Available from: https://www.mhlw.go.jp/toukei/saikin/hw/k-tyosa/k-tyosa19/index.html
- Ministry oIAaC. Final report of the 2015 population and households of Japan. Tokyo: Director General Statistics Bureau; 2018 [cited 26 Oct 2022]. Available from: https://www.stat.go.jp/english/data/kokusei/2015/final_en/final_en.html#Summary
- Ministry oIAaC. Annual report on the labour force survey 2017. Tokyo; 2017 [cited 26 Oct 2022]. Available from: https://www.stat.go.jp/english/data/roudou/report/2017/index.html
- Organisation fEC-oaDO. OECD. OECD Reviews of public health: Japan: a healthier tomorrow. Paris: OECD Publishing; 2019 [cited 26 Oct 2022]. Available from: https://doi.org/10.1787/9789264311602-en