
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Aim
To quantify the economic burden associated with tobacco smoking among smokers aged 30-69 years, and second-hand smokers (SHS) aged 15-69 years in Jordan.
Materials and methods
A prevalence-based analysis was conducted in alignment with the Economics of Tobacco Toolkit developed by the WHO. The time-horizon of the analysis was one year (2019). Direct and indirect costs were estimated using data from the 2019 Global Burden of Diseases study. The analysis targeted the Jordanian population of smokers aged 30–69 years, and SHS aged 15-69 years. Adjustments were applied for age, gender, and smoking-related diseases. Direct costs were estimated using the smoking-attributable fraction (SAF) and national health expenditures. Indirect costs were divided into morbidity and mortality components. A discount rate of 3.0% and an annual productivity growth rate of 1.0% were assumed in modelling future economic losses. A sensitivity analysis was conducted on the lower and upper estimates of data used in this study.
Results
The cost of tobacco smoking and SHS exposure was estimated at US$2,108 million (95% confidence interval [CI] = US$2,003 million-US$2,245 million). This represents 4.7% (95%CI = 4.5%–5.0%) of national gross domestic product (GDP). Direct costs accounted for 3.1% of national GDP. Tobacco smoking accounted for 85.0% of total cost and SHS exposure accounted for 15.0% of total cost. Direct costs accounted for 67.0% of total cost, while indirect morbidity and mortality costs accounted for 9.0% and 24.0% of total cost, respectively. Non-communicable diseases accounted for 96.0% of total direct costs compared to communicable diseases (4.0% of total direct costs).
Conclusions
Smoking cessation interventions such as raising taxes on cigarettes, protecting people from tobacco smoke, warning labels, plain packaging, and bans on advertising, are crucial for controlling national expenditures for treating smoking-related diseases and for averting future economic losses.
PLAIN LANGUAGE SUMMARY
In this work, we aimed to calculate the annual economic impact of tobacco smoking in Jordan in 2019. We used the World Health Organization toolkit methodology to estimate both the direct and indirect costs associated with smoking nationally. Our focus was on Jordanian smokers aged 30-69 years and people exposed to second-hand smoke aged 15–69 years. Direct costs were calculated using epidemiological data on the proportion of health expenditures attributable to smoking and the national health expenditures. Indirect costs were divided into two components: morbidity and mortality. We also projected future economic losses, assuming a 3.0% discount rate and a 1.0% annual growth rate of productivity. Our study estimated that the cost of smoking and exposure to second-hand smoke was US$2,108 million (US$2,003 million-US$2,245 million), which accounted for 4.7% (4.5%-5.0) of Jordan’s gross domestic product. The majority of the cost (85.0%) was due to direct smoking, while 15.0% was due to exposure to second-hand smoke. Direct costs made up 67.0% of the total cost, while the costs related to morbidity and mortality accounted for 9.0% and 24.0% of the total cost, respectively. In conclusion, our study emphasized that tobacco smoking has a significant economic impact on Jordan. Therefore, it is crucial to implement effective smoking cessation programs, such as enforcing existing anti-tobacco policies and raising taxes. These measures can help control national expenditures for treating smoking-related diseases and prevent future economic losses.
Introduction
The causal relationship between smoking and negative health consequences has been established since 1960Citation1–3. Beyond its impact on health, the detrimental effects of smoking on economies and societies have received considerable research focus, particularly in developed countriesCitation1. However, few studies from developing countries have been conducted to investigate this issueCitation4. These studies underscore that tobacco smoking stands as one of the main causes of preventable deaths not only in most high-income nations but also increasingly in low- and middle-income countries. Furthermore, the research highlights additional ramifications linked to smoking, including disability and productivity losses due to premature deathsCitation5.
Since the adoption of the United Nations (UN) Agenda for Sustainable Development in 2015, comprising 17 Sustainable Development Goals (SDGs), member states have committed to achieving these objectives by 2030Citation6. Within this framework, tobacco control was identified as a strategic imperative to realize goals aimed at promoting healthy lives and well-being for populationsCitation6. Despite being a UN member and endorsing the SDGs, Jordan struggles with an ongoing smoking epidemic, even as the nation progresses in implementing tobacco control policies designed to align with the SDGs.
According to the World Bank, Jordan is categorized as an upper-middle-income country and contends with one of the highest smoking rates in the Middle East and North Africa (MENA) regionCitation7. The Global Burden of Disease Study in 2019 revealed that the prevalence of smoking among the population of Jordan is notably high, estimated at 55.0% among males and 12.0% among femalesCitation8. The reported figures surpass those of other Middle Eastern countriesCitation7.
This elevated smoking rate in Jordan is associated with heightened morbidity and mortality rates. According to the United Nations Development Programme (UNDP), smoking and second-hand smoke (SHS) exposure contribute to approximately 9,000 deaths annually in JordanCitation9, with an additional 38,809 years of healthy life lost due to disability (YLDs)Citation9.
Moreover, the societal and economic impact of smoking in Jordan is substantial. A survey by the World Health Organization (WHO) indicates that Jordanian smokers spend approximately JOD73.0 (US$103.0) per month on tobacco-related products, constituting 18.0%-30.0% of the average monthly income in Jordan. In comparison, the average monthly spending on fruits is JOD 27.0 (US$38.0)Citation10.
Expanding the economic context to a national level, a 2015 study estimated the economic losses from smoking in Jordan at US$2.2 billion were in 2015 alone, representing 6.0% of Jordan’s gross domestic product (GDP) for that yearCitation11.
While studies assessing the economic cost of smoking in Jordan have been conducted, they were mostly limited to survey data or focused on direct costs only. The Economics of Tobacco Toolkit developed by the World Health Organization (WHO) provides a standardized approach to capture the direct and indirect costs of smoking in societies with limited data sourcesCitation12. This toolkit is considered a universal tool in measuring the adverse economic effects of smokingCitation13,Citation14.
The objective of this study is to assess the economic burden of diseases and deaths attributable to smoking and SHS exposure on society in Jordan. The results of this study can be instrumental in justifying the needs for stronger tobacco control policies and guiding health policy and planning in Jordan.
Methods
Model overview
A prevalence-based model, over a 1-year time horizon (2019), was constructed in accordance with the guidelines provided by the WHO toolkitCitation12. This toolkit offers several different methodologies for estimating two key components: direct smoking-attributable costs and indirect costs arising from productivity losses due to smoking-attributable disability and mortalityCitation12. These different approaches were provided to meet different levels of data availability for estimating specific smoking-related costs in countries with limited dataCitation12. In the WHO toolkit, direct costs encompass expenses resulting from healthcare services provided to treat diseases related to smoking. This category includes the costs associated with hospitalization, outpatient visits, treatments, diagnostics, and related medical servicesCitation12. Indirect costs in the toolkit are subdivided into morbidity costs and mortality costs stemming from smoking-related diseases. In this analysis, two populations were included for estimating direct and indirect costs: the smoking population aged 30-69 years and the SHS-exposed population aged 15-69 years. The inclusion of these two groups aligns with common practiceCitation13,Citation14. Further, the diseases associated with smoking attributable mortality and morbidity were sourced from the 2019 Global Burden of Diseases (GBD)Citation8. shows the smoking-attributable diseases included in this study. The risks associated with these smoking-attributable diseases, adjusted by gender, age, smoking versus SHS, and country, were obtained from IHMECitation8. Specific to Jordan, smoking attributable risks of mortality and morbidity estimates resulting from these diseases are detailed in the supplemental material, Tables S1–S8, clustered by gender and age for both smoking and SHS exposure. All costs presented in this study are denominated in US 2019 dollars (US$), as equivalent to JOD 1.41.
Table 1. Smoking-attributable diseases.
Direct costs
According to the WHO toolkit, the formula used to calculate the direct costs is:
where SHE denotes smoking-attributable health expenditures, SAF denotes smoking-attributable fraction, and THEs represents the total national annual health expenditure. The SAF signifies the proportion of health services utilization, healthcare costs, deaths, or other health outcome measures attributable to smoking and SHS. The THEs represents the total national annual expenditure in Jordan for treating diseases, encompassing government health spending, out-of-pocket health expenditure, and prepaid private spending. The main data sources for these two important parameters are the 2019 GBD studyCitation8 (Supplemental Tables S1–S4); and a published dataset on global health expenditures that estimated health expenditure per capita in Jordan for 2019Citation8. lists the necessary inputs for estimating total health expenditures, including the total population in Jordan and total health expenditures per capita per yearCitation15,Citation16.
Table 2. Model inputs.
Indirect costs
The smoking attributable indirect morbidity cost (SAI) arising from both active smoking and SHS was estimated using the human capital approachCitation8. This approach takes into consideration the SAF, duration of disability due to smoking and SHS related-diseases adjusted by age and gender, the employment-population ratio, and the productivity of the employed population. Prior studies considered the age of 30 years as the minimum age of latency, representing the time lag between exposure to smoking and the manifestation of associated health outcomesCitation13,Citation14. The smoking attributable indirect morbidity cost was calculated as:
Where SAI denotes smoking attributable indirect morbidity cost, SAFdga denotes smoking-attributable fraction of morbidity cost caused by disease d, within a population characterized by gender g and age a; YLDdga represents the number of years lost to disability; EMPga is the employment-to population ratio applicable to the population with gender g and age a; PROD stands for the GDP per worker, calculated by dividing the national GDP by total employment.
The values of YLDs are populated in the online supplemental material (S5-S8), based on data from the IHMECitation8. The EMP, national GDP, GDP per capita, and productivity data were obtained from published materials and the International Monetary Fund (IMF) for 2019Citation17.
Smoking Attributable Indirect Mortality Cost (SAMC) arising from smoking and diseases attributable to SHS within a population characterized by gender g and age a is expressed by the following formula:
Where SAMC denotes smoking attributable indirect mortality cost; d is a disease; g is gender; a is age; SAF is the smoking-attributable fraction of deaths; TDEATH is the total number of deaths; PVLE is the total discounted present value of lifetime earnings per person; MINs represents the minimum age which is 30; MAXs represents the minimum age which is 69.
The calculated PVLE was based on the approach developed by Max and colleaguesCitation18, which was adopted by othersCitation13,Citation14. The equation used for the calculation is:
Where a is age; g is gender; PVLE represents the present discounted value of lifetime earnings; SURV is the probability that a specific person will survive; MAX is maximum age group; Y is the mean annual earnings of an employed person; E represents the proportion of the population that are employed in the labor market; YH represents the average annual imputed value of household production; EH represents the proportion of the population that are doing housekeeping; V represents the growth rate of labor productivity; r refers to discount rate.
Data on number of deaths resulted from smoking-attributable diseases and life expectancy were obtained from the IHMECitation8. Data on life expectancy for the Jordanian population was sourced from the IHMECitation8. For the calculation of PVLE, we used GDP per worker as earnings, excluding the value of housekeeping services. Further, an annual productivity growth rate of 1% and discounting rate of 3% were assumed in the calculation. These assumptions were made by prior studiesCitation13,Citation14.
Sensitivity analysis
A sensitivity analysis was conducted using the ranges reported in the data sources for the total health care expenditure per year per capita and the rate of smoking among men and womenCitation8,Citation15. The lower and the upper estimates of these parameters were used to report the upper and the lower estimates for the cost of tobacco smoking and SHS exposure in Jordan.
Results
In our data analysis for Jordan, smoking and SHS accounted for 33% of deaths in 2019. Smoking-Attributable Fractions (SAFs) for various groups revealed that, on average, smoking men had a SAF of 27.0% (95% CI = 9.9%-35.0%), smoking women had an SAF of 7.0% (95% CI = 2.5%-11.0%), SHS-exposed men had a mean SAF of 4.0% (95% CI = 2.4%-5.0%), and SHS-exposed women had a mean SAF of 5.0% (95% CI = 0.8%-5.0%). The number of YLDs resulting from smoking in this study was 38,809, representing 26.0% of the total YLDs in Jordan for 2019 (147,050 YLDs). That is, smoking and SHS exposure accounted for 26.0% of the total YLDs in 2019, with a notable concentration of YLD among men aged 50-54 years, accounting for 12.0% of total YLDs (4,282 YLD).
and show detailed costs associated with smoking and SHS in Jordan. The overall economic burden of smoking in Jordan was estimated at US$2,108 million (US$2,003 million-US$2,245 million), equivalent to approximately US$197 per capita (US$187-US$209). The direct costs primarily attributable to smoking and SHS accounted for the largest share, representing 66.0% of the total cost. Among these, smoking men had the highest direct cost at US$909 million, contributing 43.0% to the total cost. Further breaking down the costs showed that smoking men and women together accounted for a direct cost of US$1,144 million (54% of the total cost). The direct cost of SHS exposure among men and women was estimated at US$267 million, constituting 12.6% of the total cost.
Figure 1. Costs of smokers and SHS estimated as per capita per year.
Abbreviations: SHS, second-hand smoker
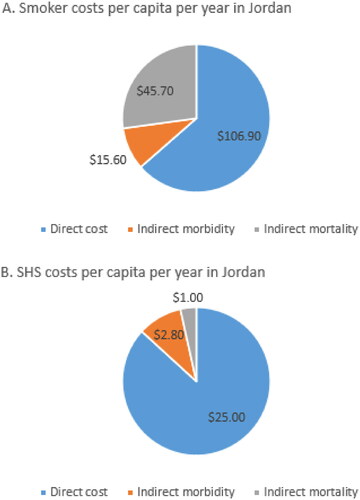
Table 3. Direct cost and indirect cost of smoking and secondhand smoke exposure (SHS).
The indirect cost of smoking amounted to US$696 million, which is 33% of the total smoking-related costs. Within the indirect costs, morbidity cost was US$196.7 million, representing 31.0% of the overall indirect cost. The mortality cost of smoking was estimated at US$499 million, contributing to 69% of the total indirect cost and 23.0% of the total smoking-related costs in Jordan. The substantial smoking-attributable mortality cost, estimated at almost US$500 million, constituted 24.0% of the total smoking-related cost. Smoking-attributable morbidity costs accounted for a relatively lower share at 9.30% of the total smoking and SHS costs.
The disaggregation of direct costs associated with Non-Communicable Diseases (NCDs) disclosed that 96.0% of the total direct costs were expended on NCDs, with ischemic heart diseases being the leading cause at 45.0%, followed by tracheal, bronchus, and lung cancer at 14.0%. The highest cost associated with communicable diseases was due to tuberculosis, which accounts for 4.0% of total direct costs.
The direct cost of smoking accounted for 4.7% (95%CI = 4.5%-5.0%) of the national GDP, most of which is due to direct costs incurred by smoking men and women, constituting 2.5% of the GDP, followed by the direct costs of SHS for both genders which was estimated at 0.6% of the GDP.
Discussion
This study highlights the substantial economic impact of smoking and SHS-related diseases in Jordan, emphasizing the urgency for comprehensive tobacco control measures aligned with SDGs. The total cost attributed to smoking and SHS amounted to 4.7% of the national GDP, accounting for a significant percentage of GDP in a country with limited economic resourcesCitation19–21.
The substantial smoking-attributable mortality cost, estimated at almost US$500 million, constituted 24.0% of the total smoking-related cost. Smoking emerged in this study as the predominant cause of mortality in Jordan, with 33.0% of all deaths in 2019 (a total of 2,837 deaths) attributed to smoking. This avoidable loss of lives underscores the imperative for healthcare policymakers to enforce evidence-based smoking cessation programs. Conversely, smoking-attributable morbidity costs accounted for a relatively lower share at 9.3% of the total smoking and SHS costs. This lower proportion can be attributed to the modest productivity per capita and low employment-to-population ratio in Jordan. The average GDP per worker in 2019 was US$12,891Citation17, while the employment-to-ratio stood at 32.0% in the same year. These factors might have influenced the diminished cost of morbidity. It is imperative for decision-makers to recognize that, without considering these variables, the number of YLDs resulting from smoking in this study was 38,809, representing 26.0% of the total YLDs in Jordan for 2019 (147,050 YLDs). This proportion poses a substantial concern about the national productivity in future developmental plansCitation22.
A cross-country study inclusive of six Gulf Cooperation Council (GCC) countries and Greece suggested that Jordan had a higher economic cost of smoking than any other middle-income country in the MENA regionCitation13. Kuwait led among the GCC countries, with the total cost of smoking accounting for 1.5% of national GDP, while cost in Greece was around 2.2% of its national GDPCitation13,Citation14.
Furthermore, a global study involving 152 countries estimated the economic cost of smoking at US$467 billion in 2016, which is equivalent to 5.7% of global health expenditures and 1.8% of global GDP, clearly indicating that Jordan’s share of smoking cost to national GDP surpasses the global averageCitation4,Citation23.
While caution is warranted in cross-country comparisons due to variations in income levels, Jordan’s smoking-attributable share of GDP remains higher than other middle-income countries in the MENA region. For instance, Bahrain’s economic cost of smoking in 2019 was US$952 million, representing 1.4% of their national GDP, and Lebanon, despite a high smoking rate of 32.0%, had an economic cost of smoking of 1.1% of their national GDP in 2008Citation24,Citation25.
Jordan has joined the WHO Framework Convention on Tobacco Control (WHO FCTC)Citation26. In this role, Jordan is committed to implementing evidence-based tobacco control initiatives to reduce the demand and supply of tobacco. In a prior study that assessed the impact of WHO FCTC tobacco control investment programs in 21 member countries, Jordan was the country most affected by smokingCitation27. In this study conducted by Mann et al. the annual socioeconomic costs of tobacco use in Jordan was estimated at US$2,500 million which represents 6% of the Jordanian GDP.
Our findings are consistent with a prior study conducted by Mann et al. Although Mann et al. used the same WHO toolkit with different model parameters, the socioeconomic losses of 4.7% of Jordanian GPD in our study is still consistent with the Mann et al.’s estimate for Jordan which averaged 6% of national GDPCitation27. In the Mann et al. study, the rate of smoking among men and women was aggregated to 42% compared to our study that used disaggregated estimates at 22% among men and 4% among womenCitation8. Also, Mann et al. considered the age of 15 years as the minimum age of latency between exposure to smoking and the health outcomes. Our study, as prior studiesCitation13,Citation14, considered age of 30 years as the minimum age of latency, representing the time lag between exposure to smoking and the manifestation of associated health outcomesCitation13,Citation14. Such differences in model inputs explain the discrepancies between the two studies.
If Jordan implemented the packages of the WHO FCTC, the return on investment would be substantial. In Jordan, a package of six measures were recommended to reduce tobacco demand and supply: raising taxes on cigarettes, protecting people from tobacco smoke, warning labels, plain packaging; bans on advertising, and mass media campaignsCitation27.
We acknowledge some limitations of our study, such as the absence of detailed data on healthcare utilization and adjustments per smoking status, reliance on previously published studies for smoking-attributable fractions and healthcare expenditures, the exclusion of household productivity in present discounted value of lifetime earnings calculations, and omitting SHS costs for those under age 15 and all costs for those over age 69. Some diseases like asthma that may affect younger women and children were not included in this study due to lack of data. Further, the cost to purchase tobacco was not included in this study because the prices of tobacco in Jordan are associated with sales taxes that are varied between products and categorized into tiersCitation28,Citation29. This was difficult to capture without a public survey.
Smoking exacts a high toll not only on high income countries, but also on lower- and middle-income countries such as Jordan. It is critical that attention be paid to the economic burden of smoking on all nations. This study has utilized updated Global Burden of Disease estimates to assess smoking-related costs in Jordan according to the WHO toolkit. The findings highlight the urgency for Jordanian policymakers to implement effective tobacco control measures, aligning with the SDGs to which Jordan has committed.
Author contributions
All authors contributed to the study design and concept, analysis and review, and manuscript writing and review.
Reviewer disclosures
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose. Two members of the editorial board helped adjudicate the final decision on this paper.
Supplemental Material
Download MS Word (68.6 KB)Transparency
Declaration of financial/other relationships
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Goodchild M, Nargis N, Tursan d‘Espaignet E. Global economic cost of smoking-attributable diseases [published correction appears in Tob Control. 2018 Jul;27(4):478]. Tob Control. 2018;27(1):58–64. doi: 10.1136/tobaccocontrol-2016-053305.
- USDHHS. The health consequences of smoking: a report to the Surgeon General. Washington, DC: US Department of Health and Human Services, Centers for Disease Control and Prevention. National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2004.
- Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990-2020: global burden of disease study. Lancet. 1997;349(9064):1498–1504. doi: 10.1016/S0140-6736(96)07492-2.
- GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet (London, England). 2018;392(10159):1923–1994.
- The W. Curbing the epidemic: governments and the economics of tobacco control. The World Bank. Tob Control. 1999;8(2):196–201. doi: 10.1136/tc.8.2.196.
- UN. Transforming our world: the 2030 agenda for sustainable development. New York: United National General Assembly; 2015.
- World Bank. Breaking the habit: tobacco control & behavioral solutions can save lives in Jordan; 2023. [accessed 2023 Dec 6]. Available from: https://blogs.worldbank.org/arabvoices/breaking-habit-tobacco-control-behavioral-solutions-can-save-lives-jordan.
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 (GBD 2019) results. Seattle: Institute for Health Metrics and Evaluation (IHME); 2020. [cited 2023 Dec 6]. Available from: https://vizhub.healthdata.org/gbd-results/.
- United Nations Development Programmme (UNDP). Investment case for tobacco control in Jordan; 2023. [cited 2023 Dec 6]. Available from: https://www.undp.org/sites/g/files/zskgke326/files/migration/jo/JordanTobaccoControlInvestmentCase.pdf.
- The Jordan Times. High mortality rates prompt experts to renew calls to curb smoking across Kingdom; 2023. [cited 2023 Dec 6]. Available from: https://jordantimes.com/news/local/high-mortality-rates-prompt-experts-renew-calls-curb-smoking-across-kingdom#:∼:text=According%20to%20recent%20studies%2C%20the,related%20products%20than%20food%20items.
- World Health Organization. Making the economic case for tobacco control action in Jordan; 2023. [cited 2023 Dec 6]. Available from: https://www.emro.who.int/jor/jordan-news/making-the-economic-case-for-tobacco-control-action-in-jordan.html.
- WHO. Economics of tobacco toolkit: assessment of the economic costs of smoking. Geneva: World Health Organization; 2011.
- Koronaiou K, Al-Lawati JA, Sayed M, et al. Economic cost of smoking and secondhand smoke exposure in the Gulf Cooperation Council countries. Tob Control. 2021;30(6):680–686. doi: 10.1136/tobaccocontrol-2020-055715.
- Koronaiou K, Delipalla S. The economic cost of tobacco smoking and secondhand smoke in Greece: musculoskeletal disorders the leading contributor to smoking-related morbidity. Tob Prev Cessat. 2019;5:39. doi: 10.18332/tpc/113091.
- Global Burden of Disease 2021 Health Financing Collaborator Network. Global investments in pandemic preparedness and COVID-19: development assistance and domestic spending on health between 1990 and 2026. The Lancet. Global Health. 2023;11(3):e385–e413.
- Worldmeters. Jordan population; 2023. [cited 2023 Dec 6]. Available from: https://www.worldometers.info/world-population/jordan-population/.
- International Monetary Fund. World economic and financial surveys: world economic outlook database; 2023. [cited 2023 Dec 6]. Available from: https://www.imf.org/external/pubs/ft/weo/2018/02/weodata/index.aspx.
- Max W, Rice DP, Sung H, et al. Valuing human life: estimating the present value of lifetime earnings; 2000. [cited 2023 Dec 6]. Available from: https://escholarship.org/uc/item/82d0550k.
- Al-Hajaya S KM. The optimal size of government expenditure in Jordan for the period (1985–2014). Jordan J Econ Sci. 2017;4(2):171–183. doi: 10.12816/0040710.
- Alkhatib SM. The contribution of manufactured exports and R&D to industrial growth in Jordan. Jordan J Econ Sci. 2022;9(1):71–84.
- Oberg M, Jaakkola MS, Woodward A, et al. Worldwide burden of disease from exposure to second-hand smoke: a retrospective analysis of data from 192 countries. Lancet. 2011;377(9760):139–146. doi: 10.1016/S0140-6736(10)61388-8.
- Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2224–2260. [published correction appears in Lancet. 2013 Apr 13;381(9874):1276] [published correction appears in Lancet. 2013 Feb 23;381(9867):628. AlMazroa, Mohammad A [added]; Memish, Ziad A [added]] doi: 10.1016/S0140-6736(12)61766-8.
- Ng M, Freeman MK, Fleming TD, et al. Smoking prevalence and cigarette consumption in 187 countries, 1980-2012. JAMA. 2014;311(2):183–192. doi: 10.1001/jama.2013.284692.
- Omotowo I, Ndibuagu E, Ezeoke U. Cigarette smoking and attitudes concerning its control among healthcare workers in Enugu, South-East, Nigeria. Health. 2016;8(11):1049–1058. doi: 10.4236/health.2016.811108.
- Karanikolos M, Mladovsky P, Cylus J, et al. Financial crisis, austerity, and health in Europe. Lancet. 2013;381(9874):1323–1331. doi: 10.1016/S0140-6736(13)60102-6.
- WHO. 2021 global progress report on implementation of the WHO Framework Convention on Tobacco Control; 2023. [cited 2023 Dec 6]. Available from: https://fctc.who.int/publications/i/item/9789240041769.
- Mann N, Spencer G, Hutchinson B, et al. Interpreting results, impacts and implications from WHO FCTC tobacco control investment cases in 21 low-income and middle-income countries. Tob Control. 2024;33(Suppl 1):s17–s26. doi: 10.1136/tc-2023-058337.
- Tax Gap of Heated Tobacco Products in Jordan. Available from: https://www.tobaccofreekids.org/what-we-do/global/taxation-price/tax-gap-jordan#:∼:text=Since%202014%2C%20the%20Kingdom%20of,0.545%20per%20pack%20of%2020.
- Marquez PV, Krasovsky K, Andreeva T. Jordan - overview of tobacco use, tobacco control legislation and taxation (English). WBG global tobacco control program. Washington, DC: World Bank Group; 2019. Available from: http://documents.worldbank.org/curated/en/809891561045747696/Jordan-Overview-of-Tobacco-Use-Tobacco-Control-Legislation-and-Taxation.