
Abstract
Objective
Jewish suicides increased heavily under Nazi-rule. This research investigated risk factors for dying from suicide according to sociodemographic characteristics, local context, and time periods.
Methods
Nazi-registration of Amsterdam residents of Jewish origin in 1941 linked to death and suicide lists. The added suicides after the Nazi-invasion (1940, n = 115) and the suicides when deportation trains ran (1942/1943, n = 182) were each matched to 25 controls using sex and age. Suicide was compared across migrant, occupational, marital, and religious status and neighborhood religiosity. Conditional logistic regression was applied, stratified by time period.
Results
In 1940, immigrant (cf. native born, odds ratio (OR) 1.89, 95%CI 1.21–2.96, p = .005) and married Jews (cf. previously married) showed higher suicide risk; members of Israelite Congregations (cf. nonmembers, OR 0.35, 95%CI 0.22–0.56, p < .001) showed reduced risk. Jews living in low synagogue rate neighborhoods showed higher risk compared to those living in neighborhoods without any synagogues (OR 2.48, 95%CI 1.65–3.72, p < .001) while those living in high synagogue rate neighborhoods showed no increased risk (OR 0.58, 95%CI 0.30–1.11, p = .10). In 1942/1943, the association between religious status (OR 1.07, 95%CI 0.67, 1.72, p = .77), synagogue rate (OR 1.27, 95%CI 0.91–1.77, p = .16), immigrant status (OR 1.30, 95%CI 0.92–1.84, p = .14) and suicide attenuated; Jews in managerial/professional occupations (cf. workers) or unmarried (cf. married) showed higher risk.
Conclusions
In 1940, immigrants’ higher suicide risk likely indicates greater fear of Nazis while religious affiliation’s lower risk might indicate a protective effect of religious belief. In 1942/1943, risk differences markedly attenuated likely indicating increased fear of Nazis among all Jews.
Religiously affiliated Jews showed reduced risk of dying from suicide after the Nazi-invasion
Jewish immigrants showed higher risk of dying from suicide after the Nazi-invasion
By 1942/1943, these risks attenuated indicating fear of the Nazis spread and nullified religion’s protection
Highlights
INTRODUCTION
Epidemiological studies on suicide among Jews during the Nazi-persecution are uncommon within Holocaust and suicide literature (Levav & Klomek, Citation2018). The main reason for this is an absence of reliable data. We can read about Jewish suicides in diaries (Mechanicus, Citation1964), postwar memories (Hemelrijk, Citation2003), historical studies (De Jong, Citation1970; Hartig, Citation2007; Presser, Citation1968), and on websites such as the Digital Jewish Monument (Faro, Citation2015). A few studies used records from offices for national statistics to quantify Jewish suicide in Nazi-Germany (Kwiet, Citation1984) or during the Nazi-occupation of the Netherlands (Ultee, Luijkx, & van Tubergen, Citation2009). Our study examines the association of sociodemographic characteristics with the risk of dying from suicide for Jews living in Amsterdam during the Nazi-occupation using an epidemiological approach.
The overall suicide rate in the Netherlands during the Second World War remained about the same as before the war (Lester, Citation1994); however, the rate for men declined while that for women increased (Kruijt, Citation1960). The overall rate conceals an increase in suicides within some sociodemographic groups such as the Jewish population. The number of Jewish suicides increased heavily after the Nazi-German invasion in May 1940 and rose again in the summer of 1942 when deportation trains to Nazi-camps left the Netherlands (Herzberg, Citation1978). Some used the term “suicide epidemic” to describe these peaks in suicides (Presser, Citation1968) as the rate of Jewish suicides per 100,000 increased more than eight-fold compared to suicides in pre-WWII years (Ultee et al., Citation2009). Ultee et al. (Citation2009) showed fluctuations during the Nazi-occupation in crude suicide rate per 100,000 in the Jewish community according to nationality, sex, and marital status.
The present study contributes to the research on Jewish suicides during the Nazi-regime by applying an individual-level approach to investigate suicide among Jews living in Amsterdam using a retrieved German Nazi-registration list of Jewish inhabitants matched to postwar lists of victims and linked to data on Jewish suicides from different sources. About 75% of these Jews did not survive the Nazi-occupation (Tammes, Citation2007b, Citation2017). Such an approach results in a more accurate examination of sociodemographic factors on the risk of Jewish suicide and the impact of time and local context (Neeleman, Citation2002).
Our study has three objectives. Firstly, to explore sociodemographic differences in risk of dying from suicide. Is there an increased risk to die from suicide among (i) Jewish immigrants, since most of them fled Nazi-German territory in the 1930s (Moore, Citation1984; Rijksinspectie van de Bevolkingsregisters, Citation1942) and feared living (again) under Nazi-rule (Herzberg, Citation1978; Ligtenberg, Citation2017), and (ii) among Jews who had abandoned Judaism as they were less restricted by Jewish law prohibiting suicide (Kaplan & Schoeneberg, Citation1988). Furthermore, based on impression-based evidence and descriptive statistics, we examine whether there is an increased risk to die from suicide among (iii) married Jews, since many suicides were carried out in couples or groups, particularly after the Nazi-invasion, probably fearing separation or lost hope in the future (Kruijt, Citation1960; Presser, Citation1968) and (iv) among Jews in higher occupational jobs, since many suicide victims were doctors, bankers, academics, and politicians, believed living under Nazi-regime would be unbearable as they were likely better informed and were more likely to have access to the means to kill themselves (De Jong, Citation1970; Kruijt, Citation1960; Presser, Citation1968; Van den Ende, Citation2015). Secondly, to examine whether the risk of dying from suicide among these four groups changed over time during the Nazi-occupation by comparing suicides after the Nazi-invasion of the Netherlands in May 1940 to suicides after the start of the deportation of Jews to Nazi-camps abroad from July 1942 onwards. When trains left the Netherlands to Nazi-camps abroad regularly from July 1942 onwards basically all Jews ran the risk of deportation which might have resulted in an increase of suicides among all groups of Jews and not only among migrant and non-religious Jews anymore. However, we still expected married Jews to have a higher risk fearing separation and for Jews with highest occupation status fearing life in Nazi-camps abroad as they lacked (manual) skills. Thirdly, to examine whether the risk of dying from suicide differed according to local context either as a marker of individual risk or as a measure of community norms around the permissibility of suicide; we explored whether living in a more religious neighborhood would reduce this risk (Bailey & Stein, Citation1995).
MATERIALS AND METHODS
Study Design and Population
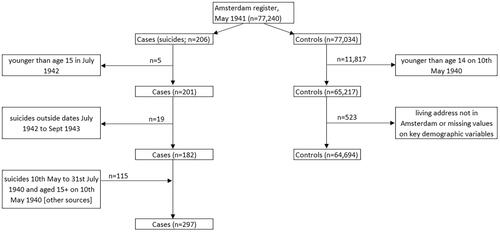
This study used a nested case-control design. To identified eligible cases and controls we used the Amsterdam registration list containing over 77,000 persons with three or four Jewish grandparents made up in May 1941 (Tammes, Citation2017) and sources mentioning Jewish suicides such as recently digitized police reports(Amsterdam City Archives), war documentation on Jewish suicides (The NIOD Institute for War Holocaust and Genocide Studies; The NIOD Institute for War Holocaust and Genocide Studies), Digital Jewish Monument (Faro, Citation2015), and Ligtenberg’s listing (Ligtenberg, Citation2017). Cases were persons aged 15 or older whose living address was in Amsterdam and who died from suicide in the Netherlands. The study selected two groups of cases to examine whether risk factors for suicide may have differed over time periods. The first group of cases (n = 115) were those who died from suicide within three months of the Nazi-Germany invasion of the Netherlands on May 10, 1940. The second group of cases (n = 182) were those who were on the Amsterdam list and died from suicide between July 1, 1942 and October 1, 1943; in July 1942, regular deportations to Nazi-camps were announced and the first train left mid-July. In September 1943, the last razzia (round-up) took place and after that only a limited number of Jews exempted from deportations could stay in Amsterdam.
To select controls, we applied incidence-density sampling which required individual matching for time. In this study, the potential controls were alive for at least another 30 days after the case died from suicide. We included in the control group victims who died at a later period of time during the Holocaust since they could have carried out suicide at an earlier time, and increasing the group size improves the precision of the analyses. A threshold of a 30-day period was chosen to consider potential deportation of the control—most Jews deported between July 1942 and September 1943 were killed soon after arrival and dates of deaths of Jewish victims of the Nazi-persecution are sometimes approximations and set at the beginning, halfway or end of the month the deportation train left the Netherlands. To determine date of death of those killed by the Nazis and those assumed to have died of natural causes in the Netherlands, the Amsterdam list was linked to several victimization and death lists (Tammes, Citation2017); survivors of the Nazi-occupation could also be potential controls. Furthermore, potential controls were matched to cases on sex and on age (±1 year); a person’s age was calculated using the date of birth on the Amsterdam list while a person’s sex was determined by using first name and maiden name of married women. Potential controls were excluded if date of death was unclear or they had missing values on key sociodemographic variables, leaving 64,694 potential controls and 297 suicide cases (). We applied matching without replacement to find 25 controls for each case so each control can only be used once.
FIGURE 1. Flow chart of the nested case-control approach.
Covariates
The Nazis ordered all persons living in the Netherlands who had one or more Jewish grandparents to be registered. These persons had to complete a form including questions about the personal religious denomination of themselves, their spouses and their grandparents. Supplementary legislation to the Nuremberg Laws defined persons who had three or four Jewish grandparents, or who had two Jewish grandparents and belonged themselves to an Israelite Congregation—that is being a member of an Israelite religious community, or were married to a Jew as so-called “full” Jew. In this study they are referred to as “Jews”, regardless of whether they are a practicing Jew or are not religious as they ran the risk of being persecuted by the Nazis based on the Nazi definition of who is a Jew. Dutch historians generally believe that practically all Jews complied with the order to register (De Jong, Citation1972; Herzberg, Citation1978). The list of Amsterdam Jews was based on these registrations and therefore includes persons who did not belong to an Israelite Congregation but were of Jewish descent. Based on the religion on this registration list we dichotomized religious affiliation into those belonging and those not belonging to an Israelite Congregation (as the number of Jews converted to Christianity was very small).
Based on the place of birth on the Amsterdam list we determined who was born in the Netherlands and who was born abroad allowing us to test the immigrant hypothesis.
Marital status on the Amsterdam list was used to determine who was unmarried, married, or had been married.
In accordance with the Historical International Standard Classification of Occupations (Van Leeuwen & Maas, Citation2011), occupations were categorized into seven social classes (Tammes, Citation2012). Given small numbers in some classes among the suicide cases, the two highest classes were combined into “managers and professionals” and the other five classes into “workers”; those without a job were categorized in a separate group.
To determine the contextual effect of religious neighborhoods, we calculated the number of synagogues per 1,000 religious Jews in each neighborhood. This is because orthodox Jews must walk to the synagogue on Shabbat (the Jewish sabbath) so long distances need to be avoided though liberal Jews could use some form of transportation and travel further. This resulted in multiple or clustering of synagogues in several Amsterdam areas, most were small and modest buildings apart from one or two grand synagogues, such as the Portuguese synagogue of Amsterdam. We defined practicing Jews as those who belonged to an Israelite Congregation and aged 13 or older when Jewish boys can have their Bar Mitzvah (ritual for coming of age). We linked the addresses on the Amsterdam list to neighborhoods (Tammes, Citation2011) and the synagogue addresses in 1940 to neighborhoods using several historical sources (Joods Amsterdam, Citation2020; Reijnders, Citation1969, Citation1987–1988). After this linkage, we derived the number of synagogues per 1,000 religious Jews in a neighborhood, and split this into three ordinal categories (no synagogues, 0–1 synagogues and more than 1 synagogue per 1,000 religious Jews).
Statistical Methods
Suicide (i.e., case-control status) is treated as a binary outcome and is modeled using conditional logistic regression taking account of the case-control groups created through matching controls to each case. Robust standard errors were used to account for clustering by household.
Each of the five sociodemographic or contextual-level factors (religion, immigrant, occupation, marital status, religious area) are tested separately in 1940 and again in 1942/1943, i.e., stratified by time. To test change over time in risk to die from suicide we used an interaction model for each of the five main factors, in order to formally test whether change over time was statistically significant. Finally, in each time period (1940 and 1942/1943) we present a multivariable model, including each of these five factors together, while adjusting for age as a continuous matching variable (Pearce, Citation2016). We included both belonging to an Israelite Congregation (individual-level covariate) as well as an ecological marker of religiosity at a contextual level as there may be additive effects.
We report odds ratios (OR), and 95% confidence intervals (95%CI) to provide evidence as to whether our sample results are likely to infer population associations. We use a strength of evidence approach (Sterne & Smith, Citation2001), whereby smaller p values suggest stronger evidence for a population effect, though this in itself does not demonstrate causality.
RESULTS
Sociodemographics of Jewish suicides are shown in . Men, persons not affiliated with an Israelite Congregation and managers/professionals were overrepresented among suicides in 1940 while those living in areas with higher numbers of synagogues were underrepresented when compared with potential controls (May 1941). Women and previously married persons were overrepresented among suicides in 1942/1943 while these later suicides were on average older. Immigrants and those not in work were overrepresented while workers were underrepresented among suicides both in 1940 and in 1942/1943.
TABLE 1. Descriptive statistics of Jews who died from suicide between May–July 1940 or July 1942–September 1943 and potential controls aged 15+ living in Amsterdam.
All cases except one matched to 25 controls, one case only had 20 controls, resulting in 2,875 controls for the suicides in 1940 and 4,545 control for the suicides in 1942/1943. shows all unadjusted and adjusted findings stratified by time, while shows the interaction effects relating to our change over time models.
TABLE 2. Association between sociodemographic factors and neighborhood composition and the odds ratios of dying from suicide for Amsterdam Jews aged 15+ between May 10 and July 31, 1940 and July 1, 1942 and September 30, 1943 in nested case-control analyses.
The odds of suicide were doubled among immigrant Jews, compared to native Jews during 1940 (OR 2.10, 95%CI 1.38–3.19; p = .001). This association was similar when adjusting for marital, work and religious status (OR 1.89, 95%CI 1.21–2.96; p = .005). During the later period, in 1942/1943, the association was weaker in both the univariate (OR 1.37, 95%CI 0.98–1.92; p = .070) and adjusted models (OR 1.30, 95%CI 0.92–1.84; p = .139). These results suggest that over time there was some attenuation of the association between immigrant status and suicide among Jews. However, this was not a statistically significant change (OR 0.65, 95%CI 0.38–1.12; p = .120).
In 1940, there was evidence that “workers” were less likely to die from suicide compared to “managers and professionals” (OR 0.44, 95%CI 0.34–0.79; p = .006), though this association was attenuated when adjusting for other factors (OR 0.57, 95%CI 0.31–1.03; p = .061). This association was consistent into the later war period of 1942/1943 in both the univariate (OR 0.40, 95%CI 0.21–0.75; p = .005) and adjusted models (OR 0.42, 95%CI 0.22–0.80; p = .008). There was no evidence in either time period for a difference in suicide risk between “managers and professionals” and unemployed Jews. The results from our interaction models suggest there was no strong time effect (p = .846 for workers, p = .765 for those not in work) on the association of occupational status on suicide among Jews.
Jews belonging to an Israelite Congregation were less likely to die from suicide in 1940 (OR 0.29, 95%CI 0.19–0.46; p < .001) and this association was also observed when adjusting for all factors (OR 0.35, 95%CI 0.22–0.56; p < .001). However, in 1942/1943, there was no evidence for an association between religious status and suicide in either the univariate (OR 0.91, 95%CI 0.57–1.45; p = .698) or adjusted models (OR 1.07, 95%CI 0.67–1.72; p = .768). The results from our interaction model suggest there was a time effect (OR 3.10, 95% CI 1.63–5.91; p = .001). This OR of 3.10 suggests that the protective association estimated in 1940 (OR 0.29) attenuated by over three times toward the null (3.10 × 0.29 = 0.90).
During the 1940 period, previously married Jews were less likely to die from suicide compared to married Jews (OR 0.31, 95%CI 0.11–0.87; p = .025), and this association was consistent after adjusting for all other factors (OR 0.23, 95%CI 0.09–0.63; p = .004). However, in the 1942/1943 period, this association was not observed in either the univariate (OR 1.16, 95%CI 0.74–1.83; p = .508) or adjusted models (OR 1.14, 95%CI 0.73–1.80; p = .561). Unmarried Jews were more likely to die from suicide compared to married Jews, but this result cannot be inferred to the population in either the univariate (OR 1.43, 95%CI 0.88–2.34; p = .153) or adjusted models (OR 1.44, 95%CI 0.85–2.47; p = .179). However, in the 1942/1943 period there was evidence for an increased risk among unmarried Jews compared to married Jews (OR 1.64, 95%CI 1.10–2.46; p = .015), and this was consistent after adjusting for all other factors (OR 1.78, 95%CI 1.18, 2.69; p = .006). The results from our interaction model suggest there was a time effect, with changes in the association of marital status on suicide among Jews over time, with an attenuation in the association for those previously married, compared to married (OR 3.70, 95%CI 1.22–11.18; p = .020). This suggests the protective effect found in 1940 (OR 0.31) is attenuated completely beyond the null over time (3.70 × 0.31 = 1.15). There was no evidence for a change over time in the comparison between unmarried and married Jews (OR 1.15, 95%CI 0.61–2.17; p = .667).
Jews living in neighborhoods with a low number of synagogues were more likely to die from suicide compared to those living in neighborhoods without any synagogues in 1940 (OR 2.48, 95%CI 1.65–3.72, p < .001), and this was robust to adjustment for other sociodemographic variables (OR 2.41, 95%CI 1.60–3.63, p < .001). Conversely, those living in neighborhoods with higher numbers of synagogues experienced a protective effect OR 0.50 (95% CI 0.26–0.95, p = .034) compared to those living in neighborhoods without any synagogues, though this association was attenuated when adjusting for other factors (OR 0.58, 95%CI 0.30–1.11, p = .102). The harmful effect of living in low synagogue areas attenuated significantly during the war, with an interaction OR of 0.54 (95%CI 0.32–0.90; p = .02), completely beyond the null over time (0.54 × 2.48 = 1.33).
DISCUSSION
Main Findings
Jews who belonged to an Israelite Congregation and to a lesser extent Jews who lived in neighborhoods with higher synagogue rates had a reduced risk to die from suicide in 1940 indicating a reduced possibly protective effect of religion, in line with most research on this topic (Koenig, Citation2016; Lawrence, Oquendo, & Stanley, Citation2016). Interestingly, those living in areas with no synagogue also had a reduced risk of dying from suicide compared to those who lived in an area with a low synagogue rate. We speculate that Jews living in these areas might have been more assimilated and hence may have felt protected as they were less obviously “Jewish”; for example, four areas in Amsterdam showed a higher concentration of Jews married to a non-Jew (Tammes, Citation2011) and three of these areas had no synagogues. Similarly, those in the most religious areas felt that they could not use suicide as a way out due to the prohibition of suicide in the Jewish religion, leaving the middle group—those living in areas with low synagogue rate in-between and showing highest relative suicide rate. However, in 1942/1943 religion no longer had a “protective effect” for either method of measuring religiosity. We speculate that a hostile environment, such as an increased perceived threat of the Nazi-occupier, or an indirect awareness of the fate that awaited Jews who were shipped out to concentration camps, could have nullified the protective effect of religious belief and most Jews regardless of their religiosity feared death (Lawrence et al., Citation2016).
Immigrant Jews showed an increased risk to die from suicide in 1940 likely indicating greater perceived threat of the Nazi-regime and may reflect their past experience and treatment by the Nazi-authorities in the home population or messages from relatives who did not migrate describing the murder and deportation of the Jewish community that they came from. The reduced suicide risk among immigrant Jews in 1942/1943 (compared to 1940) most likely reflects the increasing realization of this real threat among the native Jews so that such differences were diminished.
Jews in managerial and professional employment were more likely to die from suicide compared to Jews in other employment in 1940 and also in 1942/1943, likely indicating greater perceived fear of the Nazi-regime in 1940 and greater fear in 1942/1943 for working in Nazi-camps abroad or easier access to some methods of suicide such as medications. No difference was found between managerial and professional employment and not employed; though, this latter group is a mixture of youngsters, elderly, spouses, and unemployed persons. Although in 1940 many suicides were done together or in groups (Kruijt, Citation1960), the similar risk to die from suicide for married and unmarried Jews indicates that these group suicides involved married and unmarried persons but less often previously married as they showed a reduced risk; this latter group were mainly widow(er)s and more likely to live alone. In 1942/1943, unmarried Jews had a higher risk than married Jews to die from suicide possibly greater perceived fear for deportations. It was announced that initially only those aged between 20 and 45 would be deported while families would not be split up—which turned out to be untrue (Presser, Citation1968) but might have prevented married couples from suicide.
Although historical studies pointed at the increase in Jewish suicides, not much is known about sociodemographic differences in risk of dying from suicide. For the occupation years, Herzberg showed total numbers of suicide with peaks in 1940, 1942, and 1943 while for the year 1940 suicides were split into age groups with highest numbers among those aged between 30 and 70, however these numbers are not separated between Jews and non-Jews (Herzberg, Citation1978). Kruijt categorized suicides in 1940 and in 1941–1944 into different sociodemographic and economic groups but showed no separate tables for Jews (Kruijt, Citation1960). Ultee et al. (Citation2009) calculated and compared yearly Jewish suicide rates per 100,000 Jews in the Netherlands between 1940 and 1943 as they lacked information for comparable persons who had not died from suicide. They found that non-Dutch Jews were more likely to die from suicide than Dutch Jews in 1940 but not in 1942; this finding is in line with our result. However, they found that non-Dutch Jews had again a higher likelihood in 1943. Furthermore, they found that widow(er)s were more likely to die from suicide in all years than married persons. Our finding on previously married persons might deviate from their finding as it includes also divorced persons. Differences in findings could also be the result of our study design as we matched comparable non-suicide persons to those who died from suicide, though our collected data might underestimate suicide cases.
Strengths and Limitations
Although we are aware of the Nazis’ initial intentions for the registration of Jews, the Amsterdam list comprises the whole Jewish community in spring 1941 and makes it a unique source to study the Nazi-persecution of Jews; we therefore matched controls from this list to suicide cases both in 1940 and in 1942/1943.
Whereas Jews were still able to move from Amsterdam in 1940, this became more difficult thereafter as anti-Jewish rules restricted moving and traveling (Presser, Citation1968). These and other anti-Jewish regulation and the deportations from the summer of 1942 onwards threatened all members of the Jewish community listed in 1941. Our study is therefore less prone to confounding and hence is more likely to reflect causality.
While we combined data on suicide from different sources, the number of persons on the Amsterdam list identified as dying from suicide might still be an underestimation; sources might have been incomplete or had limited access due to privacy regulations. We have no direct measure of individual piety, though we also used an area-based measure to help better classify individuals. This was rather crude as we do not know the number of seats and size of each synagogue, which varied greatly between synagogues. Nevertheless, the number of synagogues per 1,000 religious Jews we feel is still a reasonable proxy for religiosity in a neighborhood.
Another limitation to our findings involves the assumptions regarding suicide. We have examined religiosity and immigrant status because such data were available. However, we acknowledge that alternative explanations for increased suicide ideation and attempt are possible. However, in depth data on other possible factors such as disrupted community supports among immigrants, multiple traumas, and tragic losses, or abandoning Judaism as a marker for a more generalized nihilism, were not available. Furthermore, we are conscious that suicide in the face of profound adversity such as persecution is likely very different from suicide in the context of mental illness.
We came across failed suicide attempts in several sources. Since these attempts were not systematically recorded, we did not include these in our analyses. Likewise, we have not investigated method of suicide. Although this is known for many suicides in 1940, it is less clear for the later suicides. Studying the method of suicide might give us better insight about motivations. This study focused on Jewish suicides in Nazi-occupied Netherlands – other data are needed to study factors and processes influencing the risk of suicide in Nazi-camps abroad (López-Muñoz & Cuerda-Galindo, Citation2016) or postwar (Lipsicas, Levav, & Levine, Citation2017; Lurie, Goldberger, Gur Orr, Haklai, & Mendlovic, Citation2021; Nakash, Liphshitz, Keinan-Boker, & Levav, Citation2013).
CONCLUSIONS
While Jewish suicides under Nazi-regime has been a sensitive subject (Herzberg, Citation1978; Ligtenberg, Citation2017; Ultee et al., Citation2009), the lack of available data (Levav & Klomek, Citation2018) and methodological issues has hindered studying this subject in the past. This case-control study focused on two decisive moments, the Nazi-invasion in May 1940 and the start of deportations in the summer of 1942. It showed differences in risk of dying from suicide in 1940 according to sociodemographic and local characteristics. However, the difference in risk diminished over time between some groups. Jews belonging to an Israelite Congregation showed reduced risk in 1940 but not in 1942/1943 indicating religion was no longer protective as hostility or perceived threat of the Nazi-regime increased. Immigrants showed an increased risk in 1940 but this was weakened in 1942/1943 as suicide among native-born Jews rose indicating increased awareness of the Nazi-intentions. The increased perceived Nazi-threat overruled social, cultural or religious protection against suicide resulting in an increased risk to die from suicide in 1942/1943 among religious and native Jews. Some Jews might have feared even a greater threat later in the war, such as unmarried Jews (fear of early deportation) and Jews in managerial and professional occupations (fearful of camp life abroad), resulting in higher risk to die from suicides in these groups in 1942/1943.
The finding of an increased risk to die from suicide for immigrants is contrary to their higher survival rate compared to native-born Jews found in other studies (Tammes, Citation2007a, Citation2017, Citation2019). Both findings, however, suggest immigrants were more aware of the Nazi-intensions and acted differently to escape persecution, some decided to hide or flee and others to die by suicide. Goeschel stressed that Jews who died from suicide in Berlin were not simply passive victims; suicide became the last means of maintaining their dignity and agency (Goeschel, Citation2015). Whether Jewish suicides were often carefully planned as Goeschel (Citation2015) suggested, could not be tested with our data. However, the notion of suicide as an act of agency fits in the concept that Jews had choices in deciding on strategies to deal with extreme threatening situations such as the Nazi-persecution (Finkel, Citation2017). Besides cooperation, coping, evasion, and resistance, suicide might be regarded as another option; for some a preferred first option, for some others a last resort after other strategies had failed.
ETHICS APPROVAL
Ethical approval was not required since the material used in this study are historical data available for public consultation (after signing an archive declaration) at the archive of the NIOD Institute for War Holocaust and Genocide Studies in Amsterdam or are publicly available on websites of the NIOD Institute for War Holocaust and Genocide Studies and The Digital Monument to the Jewish Community in the Netherlands and in published materials.
ACKNOWLEDGEMENTS
We would like to thank Prof. Bart Wallet for his assistance in compiling a list of synagogues with their addresses in Amsterdam in 1940 and Prof. David Gunnell for his suggestions.
DISCLOSURE STATEMENT
Yoav Ben-Shlomo’s father was a holocaust survivor born in Poland. No other conflicts were declared.
DATA AVAILABILITY STATEMENT
Data underlying this article cannot be shared publicly as some of the data were obtained after signing an archive declaration. Data will be shared upon reasonable request to the corresponding author.
Additional information
Funding
Notes on contributors
Peter Tammes
Peter Tammes, PhD, Bristol Medical School: Population Health Sciences, University of Bristol, Bristol, UK.
Tim Jones
Tim Jones, PhD, and Yoav Ben-Shlomo, PhD, Bristol Medical School: Population Health Sciences, University of Bristol, Bristol, UK; The National Institute for Health Research Applied Research Collaboration West (NIHR ARC West), University Hospitals Bristol and Weston NHS Foundation Trust, Bristol, UK.
Yoav Ben-Shlomo
Tim Jones, PhD, and Yoav Ben-Shlomo, PhD, Bristol Medical School: Population Health Sciences, University of Bristol, Bristol, UK; The National Institute for Health Research Applied Research Collaboration West (NIHR ARC West), University Hospitals Bristol and Weston NHS Foundation Trust, Bristol, UK.
Andrew J. Simpkin
Andrew J. Simpkin, PhD, School of Mathematics, Statistics and Applied Mathematics, National University of Ireland, Galway, Ireland.
REFERENCES
- Amsterdam City Archives. Police reports 1940-1945 archive no. 5225.
- Bailey, W. T., & Stein, L. B. (1995). Jewish affiliation in relation to suicide rates. Psychological Reports, 76(2), 561–562.
- De Jong, L. (1970). Het Koninkrijk der Nederlanden in de Tweede Wereldoorlog 1939-1945. Deel 3. Mei 1940. Translated title: The Kingdom of the Netherlands During World War II. The Hague: Martinus Nijhoff.
- De Jong, L. (1972). Het Koninkrijk der Nederlanden in de Tweede Wereldoorlog, deel 4, mei 1940-maart 1941, twee helften. Translated title:The Kingdom of the Netherlands During World War II. The Hague: Martinus Nijhoff.
- Faro, L. M. (2015). The Digital Monument to the Jewish Community in the Netherlands: A meaningful, ritual place for commemoration. New Review of Hypermedia and Multimedia, 21(1-2), 165–184. doi:10.1080/13614568.2014.983556
- Finkel, E. (2017). Ordinary Jews: Choice and survival during the Holocaust. Oxford: Princeton University Press.
- Goeschel, C. (2015). Suicide in Nazi Germany. Oxford: Oxford University Press.
- Hartig, C. (2007). Conversations about taking our own lives—Oh, a poor expression for a forced deed in hopeless circumstances!” Suicide among German Jews 1933–1943. The Leo Baeck Institute Yearbook, 52(1), 247–265. doi:10.3167/lbyb.2007.5213
- Hemelrijk, J. (2003). There is a way to freedom. Seven months of concentration camp. Amsterdam: Hemelrijk & Groeneveld.
- Herzberg, A. J. (1978). Kroniek der jodenvervolging, 1940-1945. Translated title: Chronicle of the persecution of the Jew, 1940–1945. Amsterdam: Meulenhoff.
- Joods Amsterdam. (2020, May). Retrieved from https://www.joodsamsterdam.nl/synagoge-index-2/
- Kaplan, S. J., & Schoeneberg, L. A. (1988). Defining suicide: Importance and implications for Judaism. Journal of Religion and Health, 27(2), 154–156.
- Koenig, H. G. (2016). Association of religious involvement and suicide. JAMA Psychiatry, 73(8), 775–776.
- Kruijt, C. S. (1960). Zelfmoord: Statistisch-sociologische verkenningen. Translated title: Suicide: Statistical-sociological explorations. Assen: Van Gorcum en Prakke.
- Kwiet, K. (1984). The ultimate refuge: Suicide in the Jewish community under the Nazis. Year Book, 29(1), 135–167.
- Lawrence, R. E., Oquendo, M. A., & Stanley, B. (2016). Religion and suicide risk: A systematic review. Archives of Suicide Research: Official Journal of the International Academy for Suicide Research, 20(1), 1–21.
- Lester, D. (1994). Suicide rates before, during and after the world wars. European Psychiatry, 9(5), 262–264. doi:10.1017/S092493380000362X
- Levav, I., & Klomek, A. B. (2018). A review of epidemiologic studies on suicide before, during, and after the Holocaust. Psychiatry Research, 261, 35–39.
- Ligtenberg, L. (2017). Mij krijgen ze niet levend: De zelfmoorden van mei 1940. Translated title: Suicide: Statistical-sociological explorations. Amsterdam: Uitgeverij Balans.
- Lipsicas, C. B., Levav, I., & Levine, S. Z. (2017). Holocaust exposure and subsequent suicide risk: A population-based study. Social Psychiatry and Psychiatric Epidemiology, 52(3), 311–317. doi:10.1007/s00127-016-1323-3
- López-Muñoz, F., & Cuerda-Galindo, E. (2016). Suicide in inmates in Nazis and Soviet concentration camps: Historical overview and critique. Frontiers in Psychiatry, 7, 88.
- Lurie, I., Goldberger, N., Gur Orr, A., Haklai, Z., & Mendlovic, S. (2021). Suicide among Holocaust survivors: A national registry study. Archives of Suicide Research, 1–12. doi:10.1080/13811118.2020.1868366
- Mechanicus, P. (1964). In dépôt. Dagboek uit Westerbork. Translated title: In dépôt. Diary from Westerbork. Amsterdam: Polak & Van Gennep.
- Moore, B. (1984). Jewish Refugees in the Netherlands 1933–1940: The Structure and Pattern of Immigration from Nazi Germany. The Leo Baeck Institute Yearbook, 29(1), 73–101. doi:10.1093/leobaeck/29.1.73
- Nakash, O., Liphshitz, I., Keinan-Boker, L., & Levav, I. (2013). The effect of cancer on suicide among elderly Holocaust survivors. Suicide & Life-Threatening Behavior, 43(3), 290–295.
- Neeleman, J. (2002). Beyond risk theory: Suicidal behavior in its social and epidemiological context. Crisis, 23(3), 114–120.
- Pearce, N. (2016). Analysis of matched case-control studies. BMJ, 352:i969. doi:10.1136/bmj.i969
- Presser, J. (1968). Ashes in the wind: The destruction of Dutch Jewry. London: Souvenir Press.
- Reijnders, C. (1969). Van “Joodsche Natiën” tot Joodse Nederlanders: Een onderzoek naar getto-en assimilatieverschijnselen tussen 1600 en 1942. Translated title: From "Jewish Nation" to Jewish Dutch. A research on ghetto and assimilation phenomena between 1600 and 1942. Amsterdam: Joko.
- Reijnders, C. (1987–1988). Op zoek naar oude chewre-sjoeltjes in Amsterdam. Hakehilla, 33,34.
- Rijksinspectie van de Bevolkingsregisters. (1942). Statistiek der bevolking van joodschen bloede in Nederland samengesteld door de Rijksinspectie van de bevolkingsregisters aan de hand van de formulieren van aanmelding ingevolge verordening no. 6/1941. Translated title: Statistics of the population of Jewish blood in the Netherlands compiled by the State Inspectorate of the Population Registers based on the registration forms concerning regulation No. 6/1941. The Hague: Algemeene Landsdrukkerij.
- Sterne, J. A., & Smith, G. D. (2001). Sifting the evidence—What’s wrong with significance tests? Physical Therapy, 81(8), 1464–1469.
- Tammes, P. (2007a). Jewish immigrants in the Netherlands during the Nazi occupation. The Journal of Interdisciplinary History, 37(4), 543–562. doi:10.1162/jinh.2007.37.4.543
- Tammes, P. (2007b). Survival of Jews during the Holocaust: The importance of different types of social resources. International Journal of Epidemiology, 36(2), 330–335.
- Tammes, P. (2011). Residential segregation of Jews in Amsterdam on the eve of the Shoah. Continuity and Change, 26(2), 243–270. doi:10.1017/S0268416011000129
- Tammes, P. (2012). “Hack, pack, sack”: Occupational structure, status, and mobility of Jews in Amsterdam 1851–1941. The Journal of Interdisciplinary History, 43(1), 1–26. doi:10.1162/JINH_a_00336
- Tammes, P. (2017). Surviving the Holocaust: Socio-demographic differences among Amsterdam Jews. European Journal of Population = Revue Europeenne de Demographie, 33(3), 293–318.
- Tammes, P. (2019). Associating locality-level characteristics with surviving the holocaust: A multilevel approach to the odds of being deported and to risk of death among Jews living in Dutch municipalities. American Journal of Epidemiology, 188(5), 896–906.
- The NIOD Institute for War Holocaust and Genocide Studies. Amsterdamsch Joodsch Psychiatrisch Gezelschap archive no. 249-0030B/a6.
- The NIOD Institute for War Holocaust and Genocide Studies. Joodsche Raad voor Amsterdam archive no. 182/203.
- Ultee, W., Luijkx, R., & van Tubergen, F. (2009). The Netherlands and World War II, Jews and suicide. In L. Sher & A. Vilens (Eds.), War and suicide (pp. 73–92). New York: Nova Science Publishers.
- Van den Ende, H. (2015). ‘Vergeet niet dat je arts bent’: Joodse artsen in Nederland 1940-1945. Translated title: 'Don't forget you are a doctor': Jewish doctors in the Netherlands, 1940-1945. Amsterdam: Uitgeverij Boom.
- Van Leeuwen, M. H., & Maas, I. (2011). HISCLASS: A historical international social class scheme. Leuven: Universitaire Pers Leuven.