
Abstract
Objectives
Identify interventions offered for children bereaved by parental suicide, investigate reported effectiveness and explore the acceptability of identified interventions.
Method
Six electronic databases were systematically searched for primary studies investigating intervention effectiveness and acceptability, (August 2011 to June 2023). Eligibility required inclusion of participants bereaved by parental suicide during childhood among sample populations. Methodological quality was evaluated applying JBI critical appraisal tools. Narrative synthesis was conducted using parallel-results convergent design.
Results
Of the 22 eligible reports, 19 articles reported on 12 manual-based supports provided during childhood; three papers described users’ experiences of various specified intervention types offered following childhood loss. Twenty-one studies reported on interventions offered for heterogeneous participant groups that included children bereaved by parental suicide. Time from loss to intervention generally included both recent (1 < 30mths) and more distant loss, with just one intervention described as solely for recently bereaved children. Eight interventions (n = 12 studies) demonstrated significant positive effects (p < 0.05), for maladaptive grief, mental health, quality of life. Only one study investigated suicide-related outcomes. Qualitative findings (n = 8 studies) facilitated development of four acceptability themes: Perceived utility, Relationships, Components and Delivery.
Conclusions
Heterogeneity in causes of loss/trauma and relationships with the deceased limit specific conclusions regarding effectiveness/acceptability of reviewed interventions for children bereaved by parental suicide. Few sub-group analyses of effects were reported, and qualitative evidence specifically from children bereaved by parental suicide was limited. Further research is recommended regarding mixed-user interventions, specifically for children bereaved by parental suicide.
HIGHLIGHTS
Significant effects: improved grief responses, mental health, quality of life
Acceptability themes: Perceived utility, Relationships, Components, Delivery
Findings derive from research involving heterogenous user groups
INTRODUCTION
Globally, over 700,000 people are lost to suicide each year (World Health Organization, Citation2022a). People of reproductive age (15-49yrs), potentially those with responsibilities for children, comprise approximately 65% of recorded suicides (WHO, Citation2021, Citation2022b). Thus, children bereaved by parental suicide can be recognized as a sizeable population; however few studies have investigated numbers of such children. Berman (Citation2011) reported six close family members, including children, as exposed to every suicide. Burrell et al. (Citation2021) and Kuramoto et al. (Citation2010) found, on average, two children impacted by each parental suicide.
Many grievers accommodate their loss over time (Bonanno, Citation2004; Castelli Dransart, Citation2017; Harris et al., Citation2021). For bereaved children, supportive early parental care, family stability, strong social networks, and higher socioeconomic status may promote resilience to distress following parental loss (Burrell et al., Citation2017; Guldin et al., Citation2015; Hua et al., Citation2020). However, subgroups of bereaved children, including those bereaved by parental suicide, may experience significant challenges (Burrell et al., Citation2018; Jakobsen & Christiansen, Citation2011; Kuramoto et al., Citation2009).
These challenges include psychological disorders, for example, maladaptive grief (MG), depression, posttraumatic stress (PTSD), behavioral and emotional problems (Berg et al., Citation2016; Hamdan et al., Citation2012; Pham et al., Citation2018). Those bereaved may exhibit elevated risks of self-harm/suicide (Hua et al., Citation2019; Rostila et al., Citation2016). Kuramoto et al. (Citation2013) reported age at loss may influence levels/duration of suicide risk for children bereaved by parental suicide, with young children (≤ 5yrs) experiencing the highest risk levels and for the greatest duration, approximately 20yrs post-loss. For children (6-12yrs), suicide risk was found to peak after five years, whilst teenagers’ suicide risk was highest during the initial 1-2yrs following parental suicide. Moreover, family history of suicide and strong attachment to the deceased may increase suicide risk and psychological distress for children bereaved by parental suicide (Tidemalm et al., Citation2011; Cerel et al., Citation2014; Meyer-Lee et al., Citation2020). Social problems can also arise (Doka, Citation1989; Mortell, Citation2015), with others minimizing, denying or deriding such children’s experiences (Cain & Lafreniere, Citation2015; Degroot & Carmack, Citation2022; Oexle et al., Citation2020). Perceived suicide stigma may increase anxiety and shame (Doka, Citation1999), prompting the bereaved to conceal details of their loss to avoid public humiliation (Hanschmidt et al., Citation2016). Grievers’ quality of life can consequently diminish (Azorina et al., Citation2019; Burrell et al., Citation2020; Pitman et al., Citation2018). Therefore, interventions may be needed to assist children bereaved by parental suicide as they mature through childhood and into adulthood, to ameliorate functional and psychological problems that may arise following their loss (Cerel et al., Citation2014).
Interventions that consider individual experiences, can lead to better health and functioning for service-users (Sturmberg et al., Citation2012). Moreover, users’ compliance with healthcare recommendations may increase for supports perceived as acceptable (e.g., Sidani et al., Citation2009; Tarrier et al., Citation2006). Thus, intervention acceptability may improve likelihood of uptake, adherence and completion, potentially contributing to overall effectiveness for a greater number of users.
There is a lack of published research regarding effects of interventions offered for children bereaved by parental suicide (Maple et al., Citation2018), and studies of intervention acceptability are limited (Sekhon et al., Citation2017). Recent reviews of interventions for suicide-bereaved people, including children (Andriessen et al., Citation2019; Journot-Reverbel et al., Citation2017) reported only one study published before the present review’s proposed coverage commencement (refer Method section) that examined intervention involving children bereaved by parental suicide (Pfeffer et al., Citation2002). Other reviews of interventions for bereaved children (Bergman et al., Citation2017; Clute & Kobayashi, Citation2013) located just two earlier studies regarding interventions offered to participant groups that included children bereaved by parental suicide (Camp Magik: McClatchey et al., Citation2009; Family Bereavement Program (FBP): (Sandler et al., Citation1992). Later research regarding these two interventions is discussed in the Results section, below.
To date, no published systematic review has focused on both effectiveness and acceptability of interventions offered for children bereaved by parental suicide, either exclusively or as part of heterogenous groups of bereaved/trauma survivors. This review therefore proposes to investigate quantitative research to identify outcomes, for which researched intervention demonstrated statistically significant effects (p < 0.05) for participants comprising or including children bereaved by parental suicide. Contemporaneously, the review will examine qualitative and quantitative research, which includes children bereaved by parental suicide among participants, for attributes that may contribute to intervention acceptability, broadly interpreted as encompassing satisfaction, suitability, perceived utility and face validity of interventions (Kaltenthaler et al., Citation2008; Sekhon et al., Citation2017).
This study poses the question: Do children bereaved by parental loss to suicide have access to effective and acceptable intervention? Three objectives are emphasized:
identify interventions offered for children bereaved by parental suicide,
investigate effectiveness of identified interventions,
explore acceptability of identified interventions.
METHOD
The review was conducted in compliance with PRISMA 2020 (Page et al., Citation2021) using recommendations from JBI Manual for Evidence Synthesis (JBI, 2020) concerning data presentation and synthesis. Mixed methods review methodology was followed (Grant & Booth, Citation2009); namely, the bringing together of quantitative effectiveness review and qualitative review on attitudes to interventions and their implementation. The review protocol was shared through ResearchGate (Graham et al., Citation2021). It was not published in any systematic-review-specific registry.
Inclusion/Exclusion Criteria
Inclusion criteria:
primary empirical research published in peer-reviewed journals: 1 August 2011 – 30 June 2023,
studies whose participants included a proportion (>0%) of people (any age), bereaved by parental suicide in childhood (<19 years), and
studies which measured intervention effects and/or reported on acceptability for interventions offered following such bereavement.
Exclusion criteria: case studies, books, grey literature, reviews; research centered on informal support, e.g., from family, friends, peers, or medication as interventions; studies that explain current/proposed intervention without appraising effectiveness/acceptability, (Supplementary file 1).
Search Strategy and Study Selection
In May/June 2021, in consultation with IT specialists, FG tested draft search strategies, and performed scoping searches for selected databases: CINAHL-Complete, PubMed, ProQuest Central-Psychology, Sociology-Collection, PsycInfo, PsycArticles. Potential terms from titles, abstracts, key words of ten eligible studies identified from scoping searches, were examined and highlighted. FG then conferred with UNE School of Health librarian, WB, SW, and MM to refine/confirm robustness of final strategies. (Supplementary 2).
Between September 2021 and March 2022 database searches were conducted, limiting retrieval coverage to August 2011–December 2021 (Supplementary 3). This coverage period was selected so that review learnings might still be relevant to interventions under development or currently available for children bereaved by parental suicide. Using Covidence systematic review software (Veritas Health Innovation, Citation2021), FG and AC independently screened titles/abstracts of retrieved studies, then independently reviewed full-text articles. Search coverage was subsequently extended to 30 June 2023, and titles/abstracts of retrieved studies from the extended search independently screened by FG and WB in December 2023. Two additional articles were selected for independent full-text review by FG/WB, but excluded for not meeting inclusion criteria. FG performed manual searches examining reference lists of articles selected for full-text review to identify/screen studies citing selected research. Consensus on study selection was reached, following 90% initial inter-rater agreement during screening, through regular discussion between FG and AC/WB, with adjudication on any unresolved disagreement by MM.
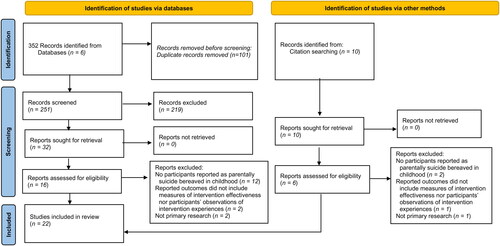
Database searches identified 352 records. Removal of duplicates (n = 101) left 251 records for title/abstract review. Thereafter, a further 219 were excluded as not satisfying inclusion criteria, generating retrieval of 32 reports for full text screening. Following full-text screening, 22 records were selected for critical appraisal, comprising sixteen records from database searches and six from citation searching ().
FIGURE 1. PRISMA flow diagram.
Data extraction and critical appraisal
Using JBI data extraction and critical appraisal tools (JBI, 2020) FG, in consultation with WB, SW and MM, developed data collection spreadsheets, completed data extraction, and appraised each study for possible bias in research design, analysis, reporting, for example, recording relevant reasoning for risk of bias as low, medium, high. (Supplementary 4).
Synthesis Methods
Effect Measures
Due to diversity of outcome measures, standardized mean difference effect size (Cohen’s d) was selected as universal effect measure. Odds ratios (OR; p<.05), where reported, were converted to Cohen’s d to facilitate comparability (Chinn, Citation2000). As this review concerned an under-examined population, appraisal of effect sizes by referring to earlier research was not considered possible (Vacha-Haase & Thompson, Citation2004). Accordingly, ranges of small (.2), medium (.5), large (.8), were used to interpret effect size (Cohen, Citation1988).
Design
Narrative synthesis was selected to accommodate the breadth of the research question and dissimilarity of data, help organize studies into more analogous groups to address review objectives, and generate an end-product relevant for researchers/intervention providers (Barnett-Page & Thomas, Citation2009; Lucas et al., Citation2007). Acknowledging the diversity of findings from this review, differing perspectives were adopted for analysis of quantitative findings – post-positivist, and qualitative evidence – constructivist. Thus, parallel-results convergent design was nominated as synthesis strategy. Quantitative and qualitative evidence were separately analyzed and reported in the review Results. Integration of evidence was then presented during interpretation of results in the Discussion. (Hong et al., Citation2017; Popay et al., Citation2006; Stern et al., Citation2021).
Quantitative evidence
Effectiveness
FG conducted preliminary synthesis of significant effects to help illuminate patterns regarding the nature of outcomes and effect sizes, iteratively examining extracted data, compiling detailed textual descriptions of intervention attributes, participant characteristics, study contexts. Tables/charts were developed to analyze how effectiveness may have been moderated by study variables, including methodological quality, design, participant particulars, intervention details. A collaborative process between FG, WB, SW and MM shared tabulated data of potential moderator variables, intervention descriptions, and analyses of relationships discerned for reported significant effects (Popay et al., Citation2006).
Acceptability
Quantitative evidence of acceptability was limited to completion rates; it was not possible for this review to make meaningful inferences regarding contributors to variations in intervention completion.
Qualitative evidence
Acceptability
Reflexive thematic analysis, embracing the value of the subjective dimension of qualitative analysis, was used for synthesis of qualitative findings (Braun & Clarke, Citation2006; Braun & Clarke, Citation2021; Gough & Madill, Citation2012; Zimmer, Citation2006). Using NVivo 12 software (QSR International Pty Ltd, Citation2020), FG interpreted evidence reflexively to inductively code data and reduce findings into fewer key meaning-units to respond to the research question, iteratively reexamining assumptions and purposefully making decisions around the wording of participants’ perceptions (Braun & Clarke, Citation2019). Regularly conferring with WB, SA and MM, FG explored and refined relationships within meaning-units using vote-counting of numbers of studies/participants reporting observations as descriptive technique, to rationalize ideas, review evidence strengths/limitations, conceptualize themes (Braun & Clarke, Citation2021; Langley et al., Citation1995; Light & Smith, Citation1971; Popay et al., Citation2006). Independently, WB examined extracted qualitative information and coding choices to assess credibility of proposed themes. Lastly, FG and WB conferenced to deliberate upon and distill those themes to the ones presented in this review.
Certainty Assessment
See Supplementary 5.
RESULTS
Of the 22 included papers, 19 studies evaluated 12 manual-based interventions and three studies reported findings regarding a number of specified intervention types. Twenty-one studies (96%) involved heterogenous participant groups, which included a mix of participants bereaved by parental suicide in childhood and other participants with experience of bereavement/trauma from different causes and/or loss of non-parental loved ones. One study examined support provided exclusively for children bereaved by parental suicide (Daigle & Labelle, Citation2012); significant effects were not reported in this study, assessed low-quality.
Twelve studies (55%) reported significant effects (p < 0.05) from eight interventions, for grief responses, mental health, quality of life. Only one included study investigated suicide-related outcomes (Sandler et al., Citation2016). Qualitative findings from eight reports (36%) supported the development of four acceptability themes: Perceived utility, Relationships, Components, Delivery.
Included studies
Reviewed studies comprised three randomized controlled trials (RCTs), five pseudo-RCTs, four quasi-experimental, one descriptive observational, three mixed method (MMR) and six qualitative studies. ().
TABLE 1. Summary of included studies and interventions (sorted by study design, and alphabetically by intervention).
Critical appraisal revealed studies of medium-high (n = 1), medium (n = 13), and low (n = 8) quality (Supplementary 6).
Study participants
Participant heterogeneity across included studies encompassed diverse childhood bereavements, e.g., sudden medical events, including heart attacks; long-term medical conditions, such as cancer; violence, including accidents, homicide, suicide; and loss of loved ones with differing relationships to the bereaved, e.g., friends, parents, other relatives. Three quantitative studies and one MMR involved children with experience of non-loss trauma within participant cohorts, e.g., abuse, domestic violence. Percentages of participants bereaved by parental suicide during childhood are presented in , and discussed in the Quantitative and Qualitative findings sections, below.
Identified interventions
Of the 12 identified manual-based interventions, six were designed as selective interventions targeted to children from specific subgroups of the population with above average risk of developing psychological disorder, such as parentally- or suicide-bereaved children. Four group interventions and two bereavement camps were classified as selective. The remaining six identified interventions were designed as indicated interventions for high-risk individuals already demonstrating measurable signs of psychological disorder, for example elevated MG or PTSD symptoms (Institute of Medicine, Citation1994). These indicated interventions comprised three groups, two individual interventions and one bereavement camp.
Ten interventions reported time from loss to intervention. Only one support was offered solely for recently bereaved children (FBP: <30mths post loss) and nine were provided for participants, with experience of both recent (<30mths) and longer-term bereavement/trauma.
The supports investigated alongside other intervention types included grief therapists, psychologists, camps and support groups.
A broad range of intervention components were identified including psychoeducation, grief therapy, cognitive behavioral therapy (CBT). All indicated interventions used trauma-focused approaches incorporating loss narrative construction.
Quantitative findings
Participant heterogeneity
All eight interventions that demonstrated significant effects involved heterogeneous user groups, including children bereaved by parental suicide and other participants with experience of childhood trauma/loss from diverse causes, with variously-related deceased. Notwithstanding heterogeneity, significant effects were mostly reported for study participants as one combined group, i.e., intermixing findings for children bereaved by parental suicide and findings for other participants. Eleven studies reported percentages of children bereaved by parental suicide as between <2% to <21% (). Only one study, assessed low quality, reported a majority of suicide-bereaved participants (60%: Spuij et al., Citation2015). Thus, whilst sub-group findings specific to childhood parental suicide might provide useful information, they could have questionable statistical power.
Significant effects
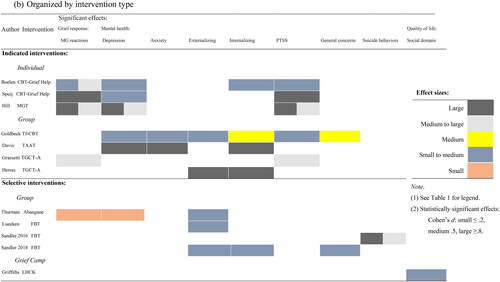
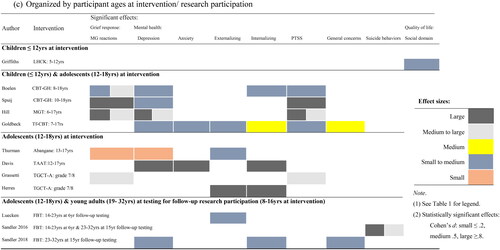
Significant intervention effects were reported for grief responses, mental health, quality of life. These effects were visually analyzed by reference to study design, intervention type, participant ages (). Key results are discussed below, ( provides details of interventions, related studies and participant).
FIGURE 2. Quantitative evidence: Significant intervention effects. Organized by: (a) study design; (b) intervention type; and (c) participant ages at intervention/ research participation.

Grief responses
Two individual and two group interventions (n = 5 studies) reported significant MG reductions: CBT Grief-Help, (n = 2 studies), (i) small-medium effects post & -3mths, medium-large −6 & -12mths, (ii) large; MGT, large–Phase I, medium-large–Phase II; Abangane: small; TGCT-A: medium-large.
Mental health
Five indicated interventions demonstrated significant mental health effects (n = 7 studies). Both individual interventions ameliorated participants’ depression and posttraumatic stress (PTSD) – CBT Grief-Help, (n = 2 studies), (i) small-medium, both concerns, (ii) small-medium and large, respectively; MGT, large – Phase I, medium-large –Phase II, for both concerns. Three indicated group supports alleviated a broader range of psychological difficulties:
Anxiety & depression – TAAT: large; Tf-CBT: small-medium
Externalizing & internalizing – TAAT: large; Tf-CBT: small-medium & medium, respectively; TGCT-A: large
PTSD – Tf-CBT: small-medium; TGCT-A: medium-large
General psychological concerns – Tf-CBT: medium
Two selective group interventions demonstrated significant beneficial effects (n = 4 studies): Abangane, depression: small, externalizing: small-medium; and FBP, (n = 3 studies), (i) externalizing −6yrs: small-medium; (ii) suicide behaviors, -15yrs: large, −6 & -15yrs combined: medium-large; (iii) internalizing, externalizing, general psychological concerns, -15yrs: small-medium.
Quality of Life
One MMR (camp intervention) reported significant positive effects (small-medium) on quality of life for children (5-12yrs).
Moderating Variables
Only one intervention (CBT Grief-Help) was investigated for moderating effects. Boelen et al. (Citation2021), RCT, reported greater MG improvements for parentally-bereaved participants vis-a-vis other relatives, and more pronounced short-term MG effects for older participants. Spuij et al. (Citation2015), uncontrolled exploratory study, reported less sizeable ameliorating effects on externalizing for suicide-bereaved participants, and on depression for children with more distant loss; neither variable demonstrated moderating effects in the 2021 study.
In summary, most effectiveness evidence was demonstrated for grief responses and psychological concerns in studies that involved adolescent intervention participants (12-18yrs) either exclusively or together with younger children (<12yrs). More sizeable beneficial effects were reported in uncontrolled studies, with controlled studies evidencing a greater number of smaller effects. Indicated interventions demonstrated a greater number and increased size of effects ().
Qualitative findings
Participant heterogeneity
The eight studies that evidenced acceptability reported findings developed from majority consensus of heterogeneous users, including participants bereaved by parental suicide in childhood, and generally did not refer to variations among users’ perceptions, notwithstanding heterogeneity. Six studies reported 8-25% participants as bereaved by parental suicide in childhood; two studies reported higher percentages (Andriessen et al., Citation2022: 61%; Brewer & Sparkes, Citation2011: 38%). One study reported overall similarity in responses for suicide-bereaved children and other participants, (Andriessen et al., Citation2019); another involved only suicide-bereaved participants (Andriessen et al., Citation2022); neither alluded to differences arising from reported varying relationships.
All studies however emphasized that, as qualitative research, findings were unique to their particular participants, providing illuminative, not definitive, answers to research questions. Hence, evidence presented supportive of qualitative findings in this review includes quotations from participants bereaved by parental suicide in childhood, where reported; other participants’ perceptions have also been quoted as illustrative of developed themes.
Acceptability
Four acceptability themes were developed:
Perceived utility
This theme, derived from eight studies, incorporated four subthemes – grief responses, mental health, quality of life, personal growth ( provides supporting evidence).
FIGURE 3. Perceived utility: Qualitative evidence. *Number of research studies that provided evidence for each theme.
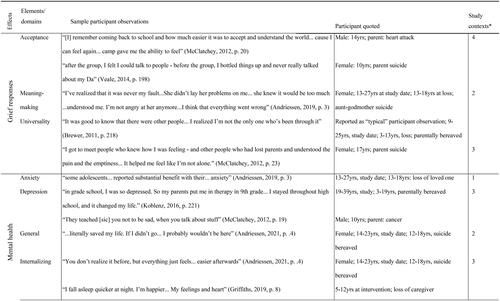
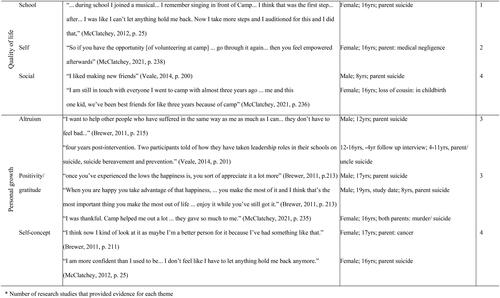
Firstly, “Grief responses”, was evidenced for two camps (n = 3 studies), one group intervention (n = 1 study), and several specified intervention types (n = 3 studies), and encompassed positive, adaptive response changes: acceptance, meaning-making, universality.
Secondly, participants perceived improvements for four “Mental health” concerns (n = 6 studies) – anxiety, depression, general mental health, internalizing. Most mental health evidence was provided retrospectively by teenage/adult participants (13-39yrs; n = 3 studies) for individual interventions offered following childhood bereavement.
Thirdly, two camps (n = 3 studies) and one group intervention (n = 1 study) evidenced benefits to “Quality of life”: school, personal, social domains.
Finally, three “Personal growth” attributes emerged: altruism; positivity/gratitude; improved self-concept, across three camps (n = 4 studies), one group (n = 1 study), and several specified supports (n = 1 study). Two camp studies reported most personal growth evidence (9-25yrs, 16-18 + yrs).
Relationships
Six studies evidenced three underlying sub-themes.
Firstly, participants welcomed “Connection,” with facilitators and with interventions (n = 5 studies):
…importance of feeling… connected through… personal relationship, (Andriessen et al., Citation2022, p. 3; 14-23yrs: interview: 12-18yrs: suicide-bereavement).
[camp is] part of my personality… ‘I am a student… waitress… I volunteer at camp …it became part of me, (McClatchey et al., Citation2021, p. 236; female; 16yrs; both parents, murder/suicide).
…bonding …with …other people …brings …people together, to feel wanted, to feel… their lives are not over, (McClatchey & Wimmer, Citation2012, p. 25; female; 16yrs; parental suicide).
…all shared that bond… able to understand… all had something similar happen, (McClatchey et al., Citation2021, p. 235; female; 18yrs: interview; 16yrs: loss; parent: medical negligence).
what helps… most was having someone… I… feel comfortable talking to… no judgement… understands where I’m coming from… (Andriessen et al., Citation2019, p. 4; female; 13-27yrs: interview: 13-18yrs: suicide-bereaved)
I felt… she was listening to me… felt respected and heard, (Andriessen et al., Citation2022, p. 4; female; 14-23yrs: interview; 12-18yrs: suicide-bereaved)
Components
Five intervention components contributed to acceptability (n = 7 studies).
“Commemorative activities” helped (n = 3 studies). For example, older parentally-bereaved participants (19-39yrs: interview; 3-19yrs: loss) appreciated ceremony, and positive memories, “Rituals were comforting,” … “I love looking at pictures of him…” (Koblenz, Citation2016, pp. 211, 214). Camp participants (8-17yrs) valued communicating with the deceased, e.g., “…they let all their feelings in a balloon… let it go… ‘That helped’,” (McClatchey & Wimmer, Citation2012, p. 22; male; 8yrs; parent heart attack).
“Creative/play-based activities” were also important (n = 4 studies). Talent show performances, for example, had “profound impact” (McClatchey & Wimmer, Citation2012, p. 25; female; 16yrs; parent suicide). Younger children (≤12yrs) liked hands-on activities, including “making things” … “Shaking the glass… with colors mixing,” (Griffiths et al., Citation2022, p. 8; campers; 5-12yrs; caregiver loss); “play with toys… drawing,” (Veale, Citation2014, p. 200; male; 8yrs; parent suicide).
Thirdly, participants valued creating “Loss narratives” (4 studies), e.g.,
When… written… you get… better glimpses of what happened… better realization… helps you cope… (McClatchey & Wimmer, Citation2012, p. 22; teenage boy; parent suicide).
As… young people tell their stories… the more they… restructure events favorably the more… enhanced their sense of personal well-being, (Brewer & Sparkes, Citation2011, p. 211; 19-39yrs: interview; 3-19yrs: parental loss).
It helped you… get over it because you talk about it more. (Veale, Citation2014, p. 198; male; 9yrs; parent suicide).
“Counselling” also rated highly (n = 3 studies). For example, individual counseling was “so much relief,” (Andriessen et al., Citation2022, pp. 3-4; female, 14-23yrs; 12-18yrs: suicide-bereaved). Group counseling was “really helpful” (McClatchey & Wimmer, Citation2012, p. 19; female; 17yrs; parent suicide).
Finally, “Learning activities” were useful (n = 2 studies), e.g.,
She taught me a lot of strategies to deal with things, (Andriessen et al., Citation2022, p. 4; female, 14-23yrs; 12-18yrs: suicide-bereaved).
…when I left camp… I realized… subliminally I was using things… I learned at camp, (McClatchey et al., Citation2021, p. 235; female; 17yrs; parent: cancer).
Delivery
Two contributors to acceptability emerged (n = 4 studies),
Firstly, “Agency,” was highly rated (n = 2 studies), e.g., “He’d just talk to me and I’d completely guide the conversation… made me feel better,” (Andriessen et al., Citation2022, p. 5; female, 14-23yrs; 12-18yrs: suicide-bereaved). Another participant observed, “We wouldn’t just have to sit down and listen, could play… having a laugh,” (Veale, Citation2014, p. 200; male: 8yrs; parent suicide).
Secondly, users appreciated “Skills and commitment” (n = 4 studies). Suicide expertise was important, “He was a child’s counsellor… tailored to suicides …knew what I was going through,” (Andriessen et al., Citation2022, p. 6; female, 14-23yrs; 12-18yrs – suicide-bereaved). Dedicated professionals were acknowledged, “If you lose someone… that’s the place to go… really got into people’s lives… They are there for you,” (McClatchey & Wimmer, Citation2012, p. 25; female; 16yrs; parent suicide). Caregivers also found intervention “beneficial to… my children… excellent… from committed caring people,” (Griffiths et al., Citation2022, p. 7: children, 5-12yrs; caregiver loss).
In conclusion, a clear set of acceptability themes were formed, which may be useful for intervention developers/facilitators to consider for loss/trauma survivors including children bereaved by parental suicide. Notably, the themes encompass perspectives of younger children (<12yrs), adolescents (12-18yrs) and adult study participants (19-39yrs; 3-19yrs: loss).
DISCUSSION
This study presents the first mixed method systematic review of the effectiveness and acceptability of interventions offered for children bereaved by parental suicide.
Identified interventions
Some parallels emerged with recent reviews concerning suicide-bereaved children (Journot-Reverbel et al., Citation2017); suicide-bereaved people (Andriessen et al., Citation2019); parentally-bereaved children (Bergman et al., Citation2017). These earlier reviews covered research from 1975-2018, and reported on only three interventions offered to participants that included children bereaved by parental suicide from research published prior to this review’s coverage period (2011-2023). In contrast, the current review provided new information regarding twelve manual-based interventions and various specified intervention types.
Effectiveness
Significant effects from this review correspond with earlier research. Bergman et al. (Citation2017) reported significant effects ameliorating MG and PTSD for one indicated intervention offered to participants including children bereaved by parental suicide. The present study revealed additional effects for anxiety, depression, externalizing, internalizing, and general psychological difficulties across five indicated interventions. Secondly, for selective interventions offered for participants including children bereaved by parental suicide, Andriessen et al. (Citation2019), reported significant effects for anxiety, depression; Bergman et al. (Citation2017) described small effects for grief, anxiety, depression, externalizing, internalizing, social difficulties. The present study evidenced more sizeable effects for these outcomes, and revealed new selective intervention effects on suicide behaviors and quality of life. Notably, inclusion of more wide-ranging study designs, heterogenous participant groups, and recency of research explains new information uncovered by the present review.
Acceptability
This review’s acceptability themes are consistent with previous research findings. Perceived utility aligns with emphasis from Dyregrov (Citation2011) that professional support for suicide-bereaved people, including children, must be developed and offered for users’ specific needs, e.g., grief concerns, psychosocial distress. Highlighted as new learning is the value bereaved participants placed on acquiring adaptive grief responses and personal growth.
The Relationships theme has some correspondence with earlier youth-friendly intervention research regarding the importance of connection and trust, (Ambresin et al., Citation2013; Hawke et al., Citation2019). Reflecting Clute and Kobayashi (Citation2013), this theme also included campers’ appreciation of peer-bonding with other bereaved children.
The Components theme aligns with appreciation for creative/play-based and learning activities from Clute and Kobayashi (Citation2013). New findings emphasize the benefits of commemorative activities, loss narratives and counseling.
Finally, participants’ appreciation of skilled providers, corresponds with conclusions in Ambresin et al. (Citation2013) and Hawke et al. (Citation2019). New information regarding Delivery concerns the value of user agency embedded in intervention delivery.
Strengths and Limitations
Strengths of this review included rigorous study selection, with all title/abstract screenings and full-text reviews conducted independently by two researchers. The inclusion of qualitative acceptability data was also a strength, enhancing understandings of a greater range of interventions offered for children bereaved by parental suicide.
Attention is drawn to several limitations. Firstly, the restricted number of eligible studies and methodological concerns, including small sample sizes, moderated review findings. Also, diversity of outcome measures used may limit comparability of effects (Wilson et al., Citation2021). Furthermore, most included research reported findings for heterogenous participant groups with experience of childhood loss/trauma from diverse causes including suicide, encompassing various relationships including parents, without explicit subgroup analyses. Caution is therefore recommended in applying findings of intervention effectiveness for children bereaved by parental suicide.
Research Implications
High-quality research is recommended to investigate effect variations for participant subgroups, particularly children bereaved by parental suicide, from interventions offered to heterogenous groups of bereaved/trauma survivors. Research aimed at increasing understanding of acceptability of mixed group interventions for children bereaved by parental suicide is also recommended.
Conclusions
This review provides a contemporary inventory of evidence-based interventions offered for mixed groups of children exposed to loss/trauma from diverse causes and relationships. Heterogeneity however limits specific conclusions regarding effectiveness for children bereaved by parental suicide. Further, applicability of acceptability findings for children bereaved by parental suicide was implicit rather than explicit in most qualitative studies. Nonetheless, this review presents evidence illuminative of intervention attributes that may improve acceptability for children impacted by loss/trauma, including bereavement by parental suicide.
Supplemental-file-6.docx
Download MS Word (40.3 KB)Supplemental-file-5.docx
Download MS Word (32.7 KB)Supplemental-file-3.docx
Download MS Word (29.8 KB)Supplemental-file-2.docx
Download MS Word (35.9 KB)Supplemental-file-1.docx
Download MS Word (30.9 KB)Supplemental-file-4.docx
Download MS Word (31.6 KB)ACKNOWLEDGMENTS
The authors would like to acknowledge Ms. Alanya Carrandi who contributed to the study selection process for the present review, conducting independent screenings of titles, abstracts, and full texts of retrieved articles and conferencing on conflicts regarding inclusion of studies.
DISCLOSURE STATEMENT
No potential conflict of interest was reported by the author(s).
DATA AVAILABILITY STATEMENT
The authors confirm that the data supporting the findings of this study are available within the article and/or its supplementary files.
Additional information
Funding
Notes on contributors
Frances Graham
Frances Graham, Warren Bartik, School of Psychology, Faculty of Medicine and Health, University of New England, Armidale, NSW, Australia.
Warren Bartik
Frances Graham, Warren Bartik, School of Psychology, Faculty of Medicine and Health, University of New England, Armidale, NSW, Australia.
Sarah Wayland
Sarah Wayland, Myfanwy Maple, School of Health, Faculty of Medicine and Health, University of New England, Armidale, NSW, Australia.
Myfanwy Maple
Sarah Wayland, Myfanwy Maple, School of Health, Faculty of Medicine and Health, University of New England, Armidale, NSW, Australia.
REFERENCES
- Aromataris, E., & Munn, Z., Eds. JBI manual for evidence synthesis. (2020). JBI. https://doi.org/10.46658/JBIMES-20-01
- Achenbach, T., McConaughy, S., Ivanova, M., & Rescorla, L. (2011). Manual for the ASEBA brief problem monitor (BPM). University of Vermont, Research Center for Children, Youth, & Families.
- Achenbach, T. M. (1991a). Manual for the Child Behavior Checklist/4-18 and 1991 profile. University of Vermont, Department of Psychiatry.
- Achenbach, T. M. (1991b). Manual for the youth self-report and 1991 profile. Department of Psychiatry, University of Vermont Burlington.
- Achenbach, T. M., & Rescorla, L. (2003). Manual for the ASEBA adult forms & profiles. University of Vermont, Research Center for Children, Youth, & Families.
- Achenbach, T. M., & Rescorla, L. A. (2004). The Achenbach System of Empirically Based Assessment (ASEBA) for Ages 1.5 to 18 Years. APA PsycNet. https://psycnet.apa.org/record/2004-14949-007
- Ambresin, A.-E., Bennett, K., Patton, G. C., Sanci, L. A., & Sawyer, S. M. (2013). Assessment of youth-friendly health care: A systematic review of indicators drawn from young people’s perspectives. The Journal of Adolescent Health: Official Publication of the Society for Adolescent Medicine, 52(6), 670–681. https://doi.org/10.1016/j.jadohealth.2012.12.014
- Andriessen, K., Krysinska, K., Hill, N. T. M., Reifels, L., Robinson, J., Reavley, N., & Pirkis, J. (2019). Effectiveness of interventions for people bereaved through suicide: A systematic review of controlled studies of grief, psychosocial and suicide-related outcomes. BMC Psychiatry, 19(1), 1-15. https://doi.org/10.1186/s12888-019-2020-z
- Andriessen, K., Krysinska, K., Rickwood, D., & Pirkis, J. (2022). “Finding a safe space”: A qualitative study of what makes help helpful for adolescents bereaved by suicide. Death Studies, 46(10), 2456–2466. https://doi.org/10.1080/07481187.2021.1970049
- Andriessen, K., Lobb, E., Mowll, J., Dudley, M., Draper, B., & Mitchell, P. B. (2019). Help-seeking experiences of bereaved adolescents: A qualitative study. Death Studies, 43(1), 1–8. https://doi.org/10.1080/07481187.2018.1426657
- Angold, A., Costello, E. J., Messer, S. C., & Pickles, A. (1995). Development of a short questionnaire for use in epidemiological studies of depression in children and adolescents. International Journal of Methods in Psychiatric Research, 5, 237–249.
- Azorina, V., Morant, N., Nesse, H., Stevenson, F., Osborn, D., King, M., & Pitman, A. (2019). The perceived impact of suicide bereavement on specific interpersonal relationships: A qualitative study of survey data. International Journal of Environmental Research and Public Health, 16(10), 1801. https://doi.org/10.3390/ijerph16101801
- Bar-On, R., & Parker, J. D. A. (2000). BarOn emotional quotient inventory: Youth version. Multi-Health system, Incorporated.
- Barnett-Page, E., & Thomas, J. (2009). Methods for the synthesis of qualitative research: A critical review. BMC Medical Research Methodology, 9(1), 59. https://doi.org/10.1186/1471-2288-9-59
- Beck, J. S., Beck, A. T., & Jolly, J. B. (2001). Beck youth inventories of emotional & social impairment: Depression inventory for youth, anxiety inventory for youth, anger inventory for youth, disruptive behavior inventory for youth, self-concept inventory for youth: Manual. Psychological Corporation.
- Berg, L., Rostila, M., & Hjern, A. (2016). Parental death during childhood and depression in young adults – A national cohort study. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 57(9), 1092–1098. https://doi.org/10.1111/jcpp.12560
- Bergman, A.-S., Axberg, U., & Hanson, E. (2017). When a parent dies - a systematic review of the effects of support programs for parentally bereaved children and their caregivers. BMC Palliative Care, 16(1), 39. https://doi.org/10.1186/s12904-017-0223-y
- Berman, A. L. (2011). Estimating the population of survivors of suicide: Seeking an evidence base. Suicide & Life-Threatening Behavior, 41(1), 110–116. https://doi.org/10.1111/j.1943-278x.2010.00009.x
- Birmaher, B., Brent, D. A., Chiappetta, L., Bridge, J., Monga, S., & Baugher, M. (1999). Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED): A replication study. Journal of the American Academy of Child and Adolescent Psychiatry, 38(10), 1230–1236. https://doi.org/10.1097/00004583-199910000-00011
- Boelen, P. A., Lenferink, L. I. M., & Spuij, M. (2021). CBT for prolonged grief in children and adolescents: A randomized clinical trial. The American Journal of Psychiatry, 178(4), 294–304. https://doi.org/10.1176/appi.ajp.2020.20050548
- Bolton, P., & Tang, A. M. (2002). An alternative approach to cross-cultural function assessment. Social Psychiatry and Psychiatric Epidemiology, 37(11), 537–543. https://doi.org/10.1007/s00127-002-0580-5
- Bonanno, G. A. (2004). Loss, trauma, and human resilience: Have we underestimated the human capacity to thrive after extremely aversive events? The American Psychologist, 59(1), 20–28. https://doi.org/10.1037/0003-066X.59.1.20
- Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. https://doi.org/10.1191/1478088706qp063oa
- Braun, V., & Clarke, V. (2019). Reflecting on reflexive thematic analysis. Qualitative Research in Sport, Exercise and Health, 11(4), 589–597. https://doi.org/10.1080/2159676X.2019.1628806
- Braun, V., & Clarke, V. (2021). One size fits all? What counts as quality practice in (reflexive) thematic analysis? Qualitative Research in Psychology, 18(3), 328–352. https://doi.org/10.1080/14780887.2020.1769238
- Brewer, J., & Sparkes, A. C. (2011). Parentally bereaved children and posttraumatic growth: Insights from an ethnographic study of a UK childhood bereavement service. Mortality, 16(3), 204–222. https://doi.org/10.1080/13576275.2011.586164
- Burnett, P., Middleton, W., Raphael, B., & Martinek, N. (1997). Measuring core bereavement phenomena. Psychological Medicine, 27(1), 49–57. https://doi.org/10.1017/s0033291796004151
- Burrell, L. V., Mehlum, L., & Qin, P. (2017). Risk factors for suicide in offspring bereaved by sudden parental death from external causes. Journal of Affective Disorders, 222, 71–78. https://doi.org/10.1016/j.jad.2017.06.064
- Burrell, L. V., Mehlum, L., & Qin, P. (2018). Sudden parental death from external causes and risk of suicide in the bereaved offspring: A national study. Journal of Psychiatric Research, 96, 49–56. https://doi.org/10.1016/j.jpsychires.2017.09.023
- Burrell, L. V., Mehlum, L., & Qin, P. (2020). Educational attainment in offspring bereaved by sudden parental death from external causes: A national cohort study from birth and throughout adulthood. Social Psychiatry and Psychiatric Epidemiology, 55(6), 779–788. https://doi.org/10.1007/s00127-020-01846-4
- Burrell, L. V., Mehlum, L., & Qin, P. (2021). Co-occurrence of psychosocial sequelae in bereaved offspring. Journal of Affective Disorders, 283, 325–328. https://doi.org/10.1016/j.jad.2021.01.044
- Cain, A. C., & Lafreniere, L. S. (2015). The taunting of parentally bereaved children: An exploratory study. Death Studies, 39(1-5), 219–225. https://doi.org/10.1080/07481187.2014.975870
- Castelli Dransart, D. A. (2017). Reclaiming and reshaping life: Patterns of reconstruction after the suicide of a loved one. Qualitative Health Research, 27(7), 994–1005. https://doi.org/10.1177/1049732316637590
- Cerel, J., McIntosh, J. L., Neimeyer, R. A., Maple, M., & Marshall, D. (2014). The continuum of “survivorship”: Definitional issues in the aftermath of suicide. Suicide & Life-Threatening Behavior, 44(6), 591–600. https://doi.org/10.1111/sltb.12093
- Chinn, S. (2000). A simple method for converting an odds ratio to effect size for use in meta-analysis. Statistics in Medicine, 19(22), 3127–3131. https://doi.org/10.1002/1097-0258(20001130)19:22<3127::aid-sim784>3.0.co;2-m
- Chorpita, B. F., Reise, S., Weisz, J. R., Grubbs, K., Becker, K. D., & Krull, J. L. (2010). Evaluation of the Brief Problem Checklist: Child and caregiver interviews to measure clinical progress. Journal of Consulting and Clinical Psychology, 78(4), 526–536. https://doi.org/10.1037/a0019602
- Clute, M. A., & Kobayashi, R. (2013). Are children’s grief camps effective? Journal of Social Work in End-of-Life & Palliative Care, 9(1), 43–57. https://doi.org/10.1080/15524256.2013.758927
- Cohen, J. (1988). The concepts of power analysis. In Statistical power analysis for the behavioral sciences (2nd ed., pp. 1–17). https://doi.org/10.4324/9780203771587
- Daigle, M. S., & Labelle, R. J. (2012). Pilot evaluation of a group therapy program for children bereaved by suicide. Crisis, 33(6), 350–357. https://doi.org/10.1027/0227-5910/a000147
- Danvers, A. F., Scott, B. G., Shiota, M. N., Tein, J. Y., Wolchik, S. A., & Sandler, I. I. (2020). Effects of therapeutic intervention on parentally bereaved children’s emotion reactivity and regulation 15 years later. Prevention Science, 21(8), 1017–1027. https://doi.org/10.1007/s11121-020-01142-2
- Davis, S., & Tungol, J. R. (2019). The transactional model of acceptance art therapy (TAAT) among parentally bereaved female adolescents: A pilot study. Indian Journal of Positive Psychology, 10(3), 178–181. https://www.proquest.com/scholarly-journals/transactional-model-acceptance-art-therapy-taat/docview/2316721835/se-2?accountid=17227
- De Haan, A., Petermann, F., Meiser-Stedman, R., & Goldbeck, L. (2016). Psychometric Properties of the German Version of the Child Post-Traumatic Cognitions Inventory (CPTCI-GER). Child Psychiatry and Human Development, 47(1), 151–158. 10.1007/s10578-015-0552-0 25990307
- Degroot, J. M., & Carmack, H. J. (2022). “I know they meant well…”: Helpful and hurtful memorable messages during mourning. Journal of Loss and Trauma, 27(5), 418–430. https://doi.org/10.1080/15325024.2021.1994224
- Doka, K. J. (1989). Disenfranchised grief: Recognizing hidden sorrow. Lexington Books.
- Doka, K. J. (1999). Disenfranchised grief. Bereavement Care, 18(3), 37–39. https://doi.org/10.1080/02682629908657467
- Dyregrov, K. (2011). What do we know about needs for help after suicide in different parts of the world? A phenomenological perspective. Crisis, 32(6), 310–318. https://doi.org/10.1027/0227-5910/a000098
- Eccles, J. S. (1997). Parents make a difference: Influences on adolescents’ college graduation plans. Presented in the annual conference of the American Educational Research Association., March 1997
- Elhai, J. D., Layne, C. M., Steinberg, A. M., Brymer, M. J., Briggs, E. C., Ostrowski, S. A., & Pynoos, R. S. (2013). Psychometric properties of the UCLA PTSD reaction index. Part II: Investigating factor structure findings in a national clinic-referred youth sample. Journal of Traumatic Stress, 26(1), 10–18. https://doi.org/10.1002/jts.21755
- Faulstich, M. E., Carey, M. P., Ruggiero, L., Enyart, P., & Gresham, F. (1986). Assessment of depression in childhood and adolescence: An evaluation of the Center for Epidemiological Studies Depression Scale for Children (CES-DC). Am J Psychiatry, 143(8), 1024–1027. https://doi.org/10.1176/ajp.143.8.1024
- Foa, E. B., Johnson, K. M., Feeny, N. C., & Treadwell, K. R. H. (2001). The Child PTSD Symptom Scale: A preliminary examination of its psychometric properties. Journal of Clinical Child Psychology, 30(3), 376–384. https://doi.org/10.1207/s15374424jccp3003_9
- Goldbeck, L., Muche, R., Sachser, C., Tutus, D., & Rosner, R. (2016). Effectiveness of trauma-focused cognitive behavioral therapy for children and adolescents: A randomized controlled trial in eight German mental health clinics. Psychotherapy and Psychosomatics, 85(3), 159–170. https://doi.org/10.1159/000442824
- Goodman, R., Meltzer, H., & Bailey, V. (1998). The strengths and difficulties questionnaire: A pilot study on the validity of the self-report version. European Child & Adolescent Psychiatry, 7(3), 125–130. https://doi.org/10.1007/s007870050057
- Gough, B., & Madill, A. (2012). Subjectivity in psychological science: from problem to prospect. Psychological Methods, 17(3), 374–384. https://doi.org/10.1037/a0029313 22799622
- Graham, F., Bartik, W., Wayland, S., & Maple, M. (2021). Research protocol: Systematic review of the effectiveness and acceptability of interventions offered for those bereaved by parental loss to suicide in childhood. [Research proposal]. Retrieved December, 2021, from https://www.researchgate.net/publication/368454422. https://doi.org/10.13140/RG.2.2.27665.92009/1
- Grant, M. J., & Booth, A. (2009). A typology of reviews: An analysis of 14 review types and associated methodologies. Health Information and Libraries Journal, 26(2), 91–108. https://doi.org/10.1111/j.1471-1842.2009.00848.x
- Grassetti, S. N., Herres, J., Williamson, A. A., Yarger, H. A., Layne, C. M., & Kobak, R. (2015). Narrative focus predicts symptom change trajectories in group treatment for traumatized and bereaved adolescents. Journal of Clinical Child and Adolescent Psychology: The Official Journal for the Society of Clinical Child and Adolescent Psychology, American Psychological Association, Division 53, 44(6), 933–941. https://doi.org/10.1080/15374416.2014.913249
- Griffiths, N., Mazzucchelli, T. G., Skinner, S., Kane, R. T., & Breen, L. J. (2022). A pilot study of a new bereavement program for children: Lionheart Camp for Kids. Death Studies, 46(4), 780–790. https://doi.org/10.1080/07481187.2019.1702121
- Guldin, M.-B., Li, J., Pedersen, H. S., Obel, C., Agerbo, E., Gissler, M., Cnattingius, S., Olsen, J., & Vestergaard, M. (2015). Incidence of suicide among persons who had a parent who died during their childhood. JAMA Psychiatry, 72(12), 1227–1234. https://doi.org/10.1001/jamapsychiatry.2015.2094
- Hamdan, S., Mazariegos, D., Melhem, N. M., Porta, G., Payne, M. W., & Brent, D. A. (2012). Effect of parental bereavement on health risk behaviors in youth: A 3-year follow-up. Archives of Pediatrics & Adolescent Medicine, 166(3), 216–223. https://doi.org/10.1001/archpediatrics.2011.682
- Hanschmidt, F., Lehnig, F., Riedel-Heller, S. G., & Kersting, A. (2016). The stigma of suicide survivorship and related consequences—A systematic review. PloS One, 11(9), e0162688. https://doi.org/10.1371/journal.pone.0162688
- Harris, C. B., Brookman, R., & O’Connor, M. (2021). It’s not who you lose, it’s who you are: Identity and symptom trajectory in prolonged grief. Current Psychology, 42(13), 11223–11233. https://doi.org/10.1007/s12144-021-02343-w
- Hawke, L. D., Mehra, K., Settipani, C., Relihan, J., Darnay, K., Chaim, G., & Henderson, J. (2019). What makes mental health and substance use services youth friendly? A scoping review of literature. BMC Health Services Research, 19(1), 1-16. https://doi.org/10.1186/s12913-019-4066-5
- Herres, J., Williamson, A. A., Kobak, R., Layne, C. M., Kaplow, J. B., Saltzman, W. R., & Pynoos, R. S. (2017). Internalizing and externalizing symptoms moderate treatment response to school-based trauma and grief component therapy for adolescents. School Mental Health, 9(2), 184–193. https://doi.org/10.1007/s12310-016-9204-1
- Hill, R. M., Oosterhoff, B., Layne, C. M., Rooney, E., Yudovich, S., Pynoos, R. S., & Kaplow, J. B. (2019). Multidimensional Grief Therapy: Pilot open trial of a novel intervention for bereaved children and adolescents. Journal of Child and Family Studies, 28(11), 3062–3074. https://doi.org/10.1007/s10826-019-01481-x
- Hogan, D., Halpenny, A. M., & Greene, S. (2002). Experiences of parental separation. The Children’s Research Centre, Trinity College, University of Dublin. https://tcd.ie/tricc/assets/pdfs/crc-archive/2002-Hogan-Halpenny-Greene-Parental-Separation.pdf
- Holland, J. M., Nam, I., & Neimeyer, R. A. (2013). A psychometric evaluation of the core bereavement items. Assessment, 20(1), 119–122. https://doi.org/10.1177/1073191112446656
- Hong, Q. N., Pluye, P., Bujold, M., & Wassef, M. (2017). Convergent and sequential synthesis designs: Implications for conducting and reporting systematic reviews of qualitative and quantitative evidence. Systematic Reviews, 6(1), 1-14. https://doi.org/10.1186/s13643-017-0454-2
- Hua, P., Bugeja, L., & Maple, M. (2019). A systematic review on the relationship between childhood exposure to external cause parental death, including suicide, on subsequent suicidal behaviour. Journal of Affective Disorders, 257, 723–734. https://doi.org/10.1016/j.jad.2019.07.082
- Hua, P., Huang, C., Bugeja, L., Wayland, S., & Maple, M. (2020). A systematic review on the protective factors that reduce suicidality following childhood exposure to external cause parental death, including suicide. Journal of Affective Disorders Reports, 2, 100032. https://doi.org/10.1016/j.jadr.2020.100032
- Institute of Medicine. (1994). Reducing risks for mental disorders: Frontiers for preventive intervention research. R. J. Haggerty & P. J. Mrazek, Eds. The National Academies Press. https://doi.org/10.17226/2139
- Jakobsen, I. S., & Christiansen, E. (2011). Young people’s risk of suicide attempts in relation to parental death: A population-based register study. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 52(2), 176–183. https://doi.org/10.1111/j.1469-7610.2010.02298.x
- Journot-Reverbel, K., Raynaud, J.-P., Bui, E., & Revet, A. (2017). Support groups for children and adolescents bereaved by suicide: Lots of interventions, little evidence. Psychiatry Research, 250, 253–255. https://doi.org/10.1016/j.psychres.2017.01.077
- Kaltenthaler, E., Sutcliffe, P., Parry, G., Beverley, C., Rees, A., & Ferriter, M. (2008). The acceptability to patients of computerized cognitive behaviour therapy for depression: A systematic review. Psychological Medicine, 38(11), 1521–1530. https://doi.org/10.1017/s0033291707002607
- Koblenz, J. (2016). Growing from grief: Qualitative experiences of parental loss. OMEGA - Journal of Death and Dying, 73(3), 203–230. https://doi.org/10.1177/0030222815576123
- Kovacs, M. (1992). Children’s depression inventory manual. Multi-Health Systems.
- Kovacs, M. (2003). Children’s depression inventory (CDI). Multi-Health Systems.
- Kuramoto, S. J., Brent, D. A., & Wilcox, H. C. (2009). The impact of parental suicide on child and adolescent offspring. Suicide and Life-Threatening Behavior, 39(2), 137–151. https://doi.org/10.1521/suli.2009.39.2.137
- Kuramoto, S. J., Runeson, B., Stuart, E. A., Lichtenstein, P., & Wilcox, H. C. (2013). Time to hospitalization for suicide attempt by the timing of parental suicide during offspring early development. JAMA Psychiatry, 70(2), 149–157. https://doi.org/10.1001/jamapsychiatry.2013.274
- Kuramoto, S. J., Stuart, E. A., Runeson, B., Lichtenstein, P., Långström, N., & Wilcox, H. C. (2010). Maternal or paternal suicide and offspring’s psychiatric and suicide-attempt hospitalization risk. Pediatrics, 126(5), e1026–e1032. https://doi.org/10.1542/peds.2010-0974
- Langley, A., Mintzberg, H., Pitcher, P., Posada, E., & Saint-Macary, J. (1995). Opening up decision making: The view from the black stool. Organization Science, 6(3), 260–279. https://doi.org/10.1287/orsc.6.3.260
- Larsen, D. L., Attkisson, C. C., Hargreaves, W. A., & Nguyen, T. D. (1979). Assessment of client/patient satisfaction: Development of a general scale. Evaluation and Program Planning, 2(3), 197–207. https://doi.org/10.1016/0149-7189(79)90094-6
- Layne, C., Kaplow, J., & Pynoos, R. (2014). Persistent complex bereavement disorder (PCBD) checklist–Youth version 1.0. University of California., CA.
- Light, R., & Smith, P. (1971). Accumulating evidence: Procedures for resolving contradictions among different research studies. Harvard Educational Review, 41(4), 429–471. https://doi.org/10.17763/haer.41.4.437714870334w144
- Lucas, P. J., Baird, J., Arai, L., Law, C., & Roberts, H. M. (2007). Worked examples of alternative methods for the synthesis of qualitative and quantitative research in systematic reviews. BMC Medical Research Methodology, 7(1), 1-7. https://doi.org/10.1186/1471-2288-7-4
- Luecken, L. J., Hagan, M. J., Sandler, I. N., Tein, J.-Y., Ayers, T. S., & Wolchik, S. A. (2014). Longitudinal mediators of a randomized prevention program effect on cortisol for youth from parentally bereaved families. Prevention Science: The Official Journal of the Society for Prevention Research, 15(2), 224–232. https://doi.org/10.1007/s11121-013-0385-7
- Maple, M., Pearce, T., Sanford, R., Cerel, J., Castelli Dransart, D. A., & Andriessen, K. (2018). A systematic mapping of suicide bereavement and postvention research and a proposed strategic research agenda. Crisis, 39(4), 275–282. https://doi.org/10.1027/0227-5910/a000498 29256269
- Mattejat, F., & Remschmidt, H. (2006). Das Inventar zur Erfassung der Lebensqualität bei Kindern und Jugendlichen (ILK.) [The inventory of life quality in children and adolescents (ILC). ] Huber.
- McClatchey, I. S., King, S., & Domby, E. (2021). From grieving to giving: When former bereavement campers return as volunteers. Omega, 84(1), 228–244. https://doi.org/10.1177/0030222819886734
- McClatchey, I. S., Vonk, M. E., & Palardy, G. (2009). Efficacy of a camp-based intervention for childhood traumatic grief. Research on Social Work Practice, 19(1), 19–30. https://doi.org/10.1177/1049731508314276
- McClatchey, I. S., & Wimmer, J. S. (2012). Healing components of a bereavement camp: Children and adolescents give voice to their experiences. Omega, 65(1), 11–32. https://doi.org/10.2190/OM.65.1.b
- Melhem, N. M., Porta, G., Payne, M. W., & Brent, D. A. (2013). Identifying prolonged grief reactions in children: Dimensional and diagnostic approaches. Journal of the American Academy of Child and Adolescent Psychiatry, 52(6), 599–607.e7. e597 https://doi.org/10.1016/j.jaac.2013.02.015
- Meyer-Lee, C. B., Jackson, J. B., & Gutierrez, N. S. (2020). Long-term experiencing of parental death during Childhood: A qualitative analysis. The Family Journal, 28(3), 247–256. https://doi.org/10.1177/1066480720926582
- Mortell, S. (2015). Assisting clients with disenfranchised grief: The role of a mental health nurse. Journal of Psychosocial Nursing and Mental Health Services, 53(4), 52–57. https://doi.org/10.3928/02793695-20150319-05
- Nader, K., Kriegler, K., Blake, D. , Pynoos, R., Newman, E., Weathers, F. (1996). Clinician-administered PTSD scale for children and adolescents. APA PsycNet. https://psycnet.apa.org/record/9999-08962-000?doi=1
- Oexle, N., Feigelman, W., & Sheehan, L. (2020). Perceived suicide stigma, secrecy about suicide loss and mental health outcomes. Death Studies, 44(4), 248–255. https://doi.org/10.1080/07481187.2018.1539052
- Page, M. J. McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., … Moher, D. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ, 372(n71), 1–9. https://doi.org/10.1136/bmj.n71
- Pham, S., Porta, G., Biernesser, C., Walker Payne, M., Iyengar, S., Melhem, N., & Brent, D. A. (2018). The burden of bereavement: Early-onset depression and impairment in youths bereaved by sudden parental death in a 7-year prospective study. The American Journal of Psychiatry, 175(9), 887–896. https://doi.org/10.1176/appi.ajp.2018.17070792
- Pfeffer, C. R., Jiang, H., Kakuma, T., Hwang, J., & Metsch, M. (2002). Group intervention for children bereaved by the suicide of a relative. Journal of the American Academy of Child and Adolescent Psychiatry, 41(5), 505–513. https://doi.org/10.1097/00004583-200205000-00007
- Pitman, A., De Souza, T., Putri, A. K., Stevenson, F., King, M., Osborn, D., & Morant, N. (2018). Support needs and experiences of people bereaved by suicide: Qualitative findings from a cross-sectional British study of bereaved young adults. International Journal of Environmental Research and Public Health, 15(4), 666. https://doi.org/10.3390/ijerph15040666
- Popay, J., Roberts, H., Sowden, A., Petticrew, M., Arai, L., Rodgers, M., Britten, N., Roen, K., & Duffy, S. (2006). Guidance on the conduct of narrative synthesis in systematic reviews. A product from the ESRC methods programme Version, 1., b92.
- Prigerson, H. G., Horowitz, M. J., Jacobs, S. C., Parkes, C. M., Aslan, M., Goodkin, K., Raphael, B., Marwit, S. J., Wortman, C., Neimeyer, R. A., Bonanno, G., Block, S. D., Kissane, D., Boelen, P., Maercker, A., Litz, B. T., Johnson, J. G., First, M. B., & Maciejewski, P. K. (2009). Prolonged Grief Disorder: Psychometric Validation of Criteria Proposed for DSM-V and ICD-11. PLoS Medicine, 6(8), e1000121. https://doi.org/10.1371/journal.pmed.1000121
- Prigerson, H. G., Maciejewski, P. K., Reynolds, C. F., Bierhals, A. J., Newsom, J. T., Fasiczka, A., Frank, E., Doman, J., & Miller, M. (1995). Inventory of complicated grief: A scale to measure maladaptive symptoms of loss. Psychiatry Research, 59(1-2), 65–79. https://doi.org/10.1016/0165-1781(95)02757-2
- Pynoos, R., Rodriguez, N., Steinberg, A., Stuber, M., & Frederick, C. (1998). The UCLA PTSD reaction index for DSM IV (revision 1). University of California Trauma Psychiatry Program.
- QSR International Pty Ltd. (2020). NVivo 12. https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home
- Robins, L. N., Wing, J., Wittchen, H. U., Helzer, J. E., Babor, T. F., Burke, J., Farmer, A., Jablenski, A., Pickens, R., & Regier, D. A. (1988). The Composite International Diagnostic Interview: An epidemiologic instrument suitable for use in conjunction with different diagnostic systems and in different cultures. Archives of General Psychiatry, 45(12), 1069–1077. https://doi.org/10.1001/archpsyc.1988.01800360017003
- Rostila, M., Berg, L., Arat, A., Vinnerljung, B., & Hjern, A. (2016). Parental death in childhood and self-inflicted injuries in young adults-a national cohort study from Sweden. European Child & Adolescent Psychiatry, 25(10), 1103–1111. https://doi.org/10.1007/s00787-016-0833-6
- Sandler, I. N., West, S. G., Baca, L., Pillow, D. R., Gersten, J. C., Rogosch, F., Virdin, L., Beals, J., Reynolds, K. D., & Kallgren, C. (1992). Linking empirically based theory and evaluation: the Family Bereavement Program. American Journal of Community Psychology, 20(4), 491–521. https://doi.org/10.1007/BF00937756 1481786
- Sandler, I., Gunn, H., Mazza, G., Tein, J. Y., Wolchik, S., Kim, H., Ayers, T., & Porter, M. (2018). Three perspectives on mental health problems of young adults and their parents at a 15-year follow-up of the Family Bereavement Program. Journal of Consulting and Clinical Psychology, 86(10), 845–855. https://doi.org/10.1037/ccp0000327
- Sandler, I., Tein, J. Y., Wolchik, S., & Ayers, T. S. (2016). The effects of the Family Bereavement Program to reduce suicide ideation and/or attempts of parentally bereaved children six and fifteen years later. Suicide & Life-Threatening Behavior, 46 (Suppl 1), S32–S38. https://doi.org/10.1111/sltb.12256
- Sandler, I. N., Ayers, T. S., Wolchik, S. A., Tein, J.-Y., Kwok, O.-M., Haine, R. A., Twohey-Jacobs, J., Suter, J., Lin, K., Padgett-Jones, S., Weyer, J. L., Cole, E., Kriege, G., & Griffin, W. A. (2003). The Family Bereavement Program: Efficacy evaluation of a theory-based prevention program for parentally bereaved children and adolescents. Journal of Consulting and Clinical Psychology, 71(3), 587–600. https://doi.org/10.1037/0022-006X.71.3.587
- Schoenfelder, E. N., Tein, J. Y., Wolchik, S., & Sandler, I. N. (2015). Effects of the Family Bereavement Program on academic outcomes, educational expectations and job aspirations 6 Years later: The mediating role of parenting and youth mental health problems. Journal of Abnormal Child Psychology, 43(2), 229–241. https://doi.org/10.1007/s10802-014-9905-6
- Sekhon, M., Cartwright, M., & Francis, J. J. (2017). Acceptability of healthcare interventions: An overview of reviews and development of a theoretical framework. BMC Health Services Research, 17(1), 88. https://doi.org/10.1186/s12913-017-2031-8
- Shaffer, D., Gould, M. S., Brasic, J., Ambrosini, P., Fisher, P., Bird, H., & Aluwahlia, S. (1983). A children's global assessment scale (CGAS). Archives of General Psychiatry, 40(11), 1228–1231. https://doi.org/10.1001/archpsyc.1983.01790100074010 6639293
- Shiota, M. N., & Levenson, R. W. (2009). Effects of aging on experimentally instructed detached reappraisal, positive reappraisal, and emotional behavior suppression. Psychology and Aging, 24(4), 890–900. https://doi.org/10.1037/a0017896
- Sidani, S., Epstein, D. R., Bootzin, R. R., Moritz, P., & Miranda, J. (2009). Assessment of preferences for treatment: Validation of a measure. Research in Nursing & Health, 32(4), 419–431. https://doi.org/10.1002/nur.20329
- Singh, B., Prabhuappa, K. P., Eqbal, S., & Singh, A. R. (2013). Depression, anxiety and stress scale: Reliability and validity of Hindi adaptation. International Journal of Education and Management Studies, 3(4), 446–449.
- Snyder, C. R., Hoza, B., Pelham, W. E., Rapoff, M., Ware, L., Danovsky, M., Highberger, L., Rubinstein, H., & Stahl, K. J. (1997). The development and validation of the Children's Hope Scale. Journal of Pediatric Psychology, 22(3), 399–421. https://doi.org/10.1093/jpepsy/22.3.399 9212556
- Spuij, M., Dekovic, M., & Boelen, P. A. (2015). An open trial of ‘Grief-Help’: A cognitive-behavioural treatment for prolonged grief in children and adolescents. Clinical Psychology & Psychotherapy, 22(2), 185–192. https://doi.org/10.1002/cpp.1877
- Steinberg, A. M., Brymer, M. J., Decker, K. B., & Pynoos, R. S. (2004). The University of California at Los Angeles post-traumatic stress disorder reaction index. Current Psychiatry Reports, 6(2), 96–100. https://doi.org/10.1007/s11920-004-0048-2 15038911
- Stern, C., Lizarondo, L., Carrier, J., Godfrey, C., Rieger, K., Salmond, S., Apostolo, J., Kirkpatrick, P., & Loveday, H. (2021). Methodological guidance for the conduct of mixed methods systematic reviews. JBI Evidence Implementation, 19(2), 120–129. https://journals.lww.com/ijebh/fulltext/2021/06000/methodological_guidance_for_the_conduct_of_mixed.2.aspx https://doi.org/10.1097/XEB.0000000000000282
- Stiffman, A. R., Horwitz, S. M., Hoagwood, K., Compton, W., Cottler, L., Bean, D. L., Narrow, W. E., & Weisz, J. R. (2000). The service assessment for children and adolescents (SACA): Adult and child reports. Journal of the American Academy of Child and Adolescent Psychiatry, 39(8), 1032–1039. https://doi.org/10.1097/00004583-200008000-00019
- Sturmberg, J. P., O'Halloran, D. M., & Martin, C. M. (2012). Understanding health system reform–a complex adaptive systems perspective. Journal of Evaluation in Clinical Practice, 18(1), 202–208. https://doi.org/10.1111/j.1365-2753.2011.01792.x
- Tarrier, N., Liversidge, T., & Gregg, L. (2006). The acceptability and preference for the psychological treatment of PTSD. Behaviour Research and Therapy, 44(11), 1643–1656. https://doi.org/10.1016/j.brat.2005.11.012
- Thurman, T. R., Luckett, B. G., Nice, J., Spyrelis, A., & Taylor, T. M. (2017). Effect of a bereavement support group on female adolescents’ psychological health: A randomised controlled trial in South Africa. The Lancet Global Health, 5(6), e604–e614. https://doi.org/10.1016/S2214-109X(17)30146-8
- Tidemalm, D., Runeson, B., Waern, M., Frisell, T., Carlström, E., Lichtenstein, P., & Långström, N. (2011). Familial clustering of suicide risk: A total population study of 11.4 million individuals. Psychological Medicine, 41(12), 2527–2534. https://doi.org/10.1017/S0033291711000833
- Tucker, C., Barber, B., & Eccles, J. (1997). Adolescents’ Discussion with Siblings, Mothers, and Fathers about Life Plans,. In annual meetings of the National Council on Family Relations, MN, USA.
- Vacha-Haase, T., & Thompson, B. (2004). How to estimate and interpret various effect sizes. Journal of Counseling Psychology, 51(4), 473–481. https://doi.org/10.1037/0022-0167.51.4.473
- Veale, A. (2014). Longitudinal evaluation of a therapeutic group work intervention with suicide-bereaved children. The Irish Journal of Psychology, 35(4), 188–204. https://doi.org/10.1080/03033910.2015.1058177
- Veritas Health Innovation. (2021). Covidence systematic review software. www.covidence.org
- Weisz, J. R., Chorpita, B. F., Frye, A., Ng, M. Y., Lau, N., Bearman, S. K., Ugueto, A. M., Langer, D. A., & Hoagwood, K. E. (2011). Youth Top Problems: using idiographic, consumer-guided assessment to identify treatment needs and to track change during psychotherapy. Journal of Consulting and Clinical Psychology, 79(3), 369–380. https://doi.org/10.1037/a0023307 21500888
- Wilson, D. M., Errasti-Ibarrondo, B., & Rodríguez-Prat, A. (2021). A research literature review to determine how bereavement programs are evaluated. Omega, 83(4), 831–858. https://doi.org/10.1177/0030222819869492
- Worden, J. (1991). Grieving special types of losses. Grief Counseling and Grief Therapy. Springer Publishing Company, Inc.
- World Health Organization. (2021). Suicide worldwide in 2019: Global health estimates. World Health Organization,. https://www.who.int/publications/i/item/9789240026643
- World Health Organization. (2022a). World health statistics 2022: Monitoring health for the SDGs, sustainable development goals. World Health Organization. https://www.who.int/publications/i/item/9789240051157
- World Health Organization. (2022b). Data platform: Maternal, newborn, child and adolescent health and ageing. World Health Organization. Retrieved from https://platform.who.int/data/maternal-newborn-child-adolescent-ageing/indicator-explorer-new/MCA/women-of-reproductive-age-(15-49-years)-population-(thousands)
- Zimmer, L. (2006). Qualitative meta-synthesis: A question of dialoguing with texts. Journal of Advanced Nursing, 53(3), 311–318. https://doi.org/10.1111/j.1365-2648.2006.03721.x
