
Abstract
Background: Media frequently report on overall work-place challenges in Swedish schools, including teachers’ working conditions, their well-being, and students’ declining results. Language is the key to success in every school subject. Therefore, optimal language learning environments are important. Poor sound environments affect teachers’ vocal health, their general well-being, and students’ performance. To provide better conditions for teachers and students, it is necessary to combine optimized room acoustics with other preventive measures such as vocal training and evidence-based tools to improve classroom communication. Teachers play a key role in the classroom and need knowledge and skills in communicative strategies to ensure first-class communication. The purpose of this study is to explore the effects of an intervention program for primary-school teachers comprising strategies for enhanced language learning and interactions in the classroom, with focus on teachers’ verbal and body communication (voice, gaze, and gesture).
Methods: Teachers (n = 25) from seven schools teaching in school year 3–6 participated. Assessments were made pre/post intervention and at 5-weeks and 3-months follow-up. The assessments included teachers’ self-assessments (questionnaires) of vocal health, self-efficacy, stress, burnout, and psychosocial work-environment.
Results: The main results were significant decrease in voice problems at the 3-months follow-up and significant decrease of both stress and degree of burnout at 5-weeks follow-up. Self-efficacy score had increased significantly at 5-week follow-up.
Conclusion: It can be concluded that the intervention program improves teachers’ self-reported vocal health, decreases their perception of stress, and degree of burnout whilst increasing their sense of self-efficacy in classroom management.
Introduction
Communication is the key to learning, but today’s learning environments often challenge, rather than support, communication in the classroom. Poor sound conditions affect both teachers’ vocal health as well as general well-being and students’ performance [Citation1–7]. Teachers’ vocal health is affected by constantly talking in noise, leading to recurring periods of hoarseness, and vocal fatigue [Citation1–4]. The combination of teachers with dysphonic voices speaking in noisy environments appears to hamper students’ learning [Citation8,Citation9]. The overall classroom communication might be severely challenged. Classroom communication in this paper refers to the way teachers speak and use other aspects of body communication in their teaching and interaction with the students in the classroom. A range of aspects such as speech intelligibility, speech rate, vocal intensity, and voice quality are included, as well as teachers’ use of gaze, gestures, and positions in the classroom.
The challenges that teachers are exposed to take their toll, e.g. Lyberg-Åhlander [Citation10] found that 18% of the teachers reporting voice problems in her studies had considered leaving the occupation due to the high vocal load. In 2014, teaching was found to be the profession with the highest percentage of work-related disorders in Sweden due to “stress and other mental strain” [Citation11]. A study on burnout in Swedish teachers found that 15% were classified as having high burnout in at least two of the three dimensions: exhaustion, cynicism, and professional efficacy [Citation12]. In the current paper, burnout is defined in line with the questionnaire used for screening of burnout, which is fatigue and exhaustion in relation to three specific spheres in the person’s life. These spheres are personal-related, work-related, and client-related where client is a broad term including working with, e.g. students, children, or patients. Intervention programs should aim at increasing the sense of teacher self-efficacy in classroom management to decrease and prevent burnout [Citation13,Citation14]. Perceived self-efficacy in social cognitive theory is defined by Bandura as “beliefs in one’s capabilities to organize and execute the courses and actions required to produce given attainments” [Citation15,p.3]. Low self-efficacy was related to higher burnout in all the studies reviewed by Brown [Citation16].
Already in 1980, Beebe noted that body communication is poorly trained during teachers’ education [Citation17]. Though this work and knowledge have existed for nearly 40 years, body communication skills are still only partly trained in Sweden’s teacher educational programs today and are also lacking as in-service teacher training. Carter’s review of Initial Teacher Training (ITT) in England provides good examples of training both voice and body language for new teachers [Citation18]. One of the recommendations in the report regarding behavior management states “All ITT programmes, for example, should support teachers to develop their own classroom presence and cover use of voice, body language, as well as how to develop and establish classroom routines and defuse situations.” Due to their lack of classroom communication training, many teachers do not know how to optimize their interaction with students in general and to deal with possible obstacles. In particular, teachers often want to know more about how to adapt their practices to help students with different speech and language learning difficulties [Citation19].
Dockrell and colleagues categorized evidence-based language and factors supporting communication into three dimensions: language learning environments, language learning opportunities, and language learning interactions. The language learning environment dimension applies to the physical environment and learning context, e.g. the sound and light conditions; the language-learning opportunities are related to the structured opportunities to support children’s language development, e.g. opportunities for group work and interactive book reading. Finally, the language-learning interaction dimension regards the ways in which adults use verbal and body communication with children: verbal recasts, expansions, speech, voice, gesture, and gaze behavior [Citation20]. Based on these studies, an observation tool, the Communication Supporting Classroom Observation Tool (the CsC Observation Tool) was developed, piloted, and subjected to a feasibility study in over 100 classrooms [Citation21].
The teacher intervention program described in this paper is based on the dimensions of the CsC, focusing mainly on the dimension of language-learning interactions, where for example teachers’ speech rate, pause patterns, voice, gaze, and gesture behavior are used to support language learning. A series of studies have examined lab-based research on dynamic aspects of communication such as how speech rate and voice quality affect children’s performance and listening effort. Haake et al. [Citation22] showed that children listening to a recording and performing a digital version of a language comprehension test performed more poorly when listening to a speaker using a fast speech rate and benefited from a slower one. Voice quality has also been shown to affect performance: children listening to a dysphonic voice performed significantly poorer on more difficult items compared to children listening to a typical voice [Citation23]. Perhaps more important, perceived listening effort seems to increase when listening to a dysphonic voice even if test results are not affected [Citation24–26]. The in-service training in the present study is based on results from the above-mentioned studies.
There exist only a few randomized controlled studies of teacher intervention programs led by Speech Language Pathologists (SLP). Starling et al. [Citation27] studied the efficacy of a training-based teacher intervention program aiming at improving language learning environments. The trained teachers significantly increased their use of language and communication modification techniques, and their students showed a significant improvement in language and communication skills [Citation27]. The study by Starling et al. is one of few also investigating the effect of intervention on the students. Interactions in the classroom are culture-dependent and few studies have been made in Swedish schools. Few, if any, studies have systematically examined the effect of teacher training lead by SLPs focusing on teachers’ body communication skills and how it affects teachers and students. There is a lack of studies looking at the effects of intervention on teachers’ health, self-efficacy, and well-being, factors that seem crucial for good classroom management and communication with students. With a few exceptions reported above, it is not known whether intervention programs designed for school teachers, targeting training of voice, body communication and strategies to enhance students’ language learning are efficient or not when aiming at developing classrooms which foster communication. The importance of developing these competencies is, however, undeniable. Continuing professional development (CPD) enables teachers to develop and enhance competencies [Citation28]. In this study, an intervention program was delivered as an in-service training for teachers and is considered as CPD, but focus in the article is on the intervention.
This study describes a teacher intervention program which includes strategies for enhanced language learning and interactions in the classroom including teachers’ verbal and body communication. The effects of the program will be investigated by obtaining data on teachers’ health, self-efficacy, and well-being.
The specific research questions for this study were:
Is there an improvement in teachers' vocal health, self-efficacy, and well-being after a relatively short teacher intervention program?
How do such effects unfold over time?
Method
This study is part of a more comprehensive project. In this current paper, the results of the teachers’ questionnaires will be reported.
Design
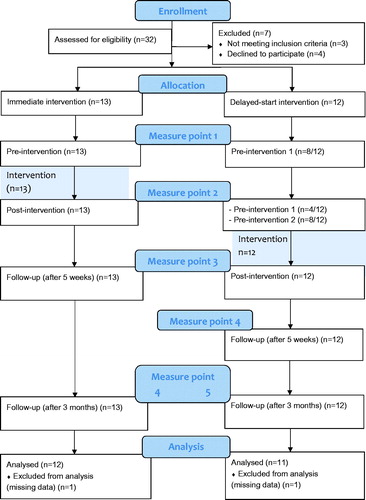
The study is designed as a delayed-start intervention study. The teachers received the in-service training in group sessions with 4–8 participants. They were either assigned to an immediate intervention group (early training group) or a delayed-start intervention group (late training group). Logistical factors at the schools determined teachers’ allocation to the groups: teachers working in a teaching team needed to be in the same intervention group to avoid schedule collisions. The teachers were gathered at two of the schools during the group sessions. The training was performed during the schools’ fixed conference-time and regular school activity continued throughout the study. The teacher intervention program consisted of 5 weeks of training, 1.5 h per week. Data collection and intervention were carried out between September 2016 and June 2017. The intervention was given to four subgroups: three during the fall with two subgroups in the early training group and just one subgroup in the late training group due to fewer participants. The reason was that two of the schools could not participate due to logistics. Therefore, one more subgroup was added to the late training group and was given intervention during the spring. Measurements for all groups were performed pre-and post-intervention with 5 weeks between, except for the last post-assessment which occurred 7 weeks after the previous one. Teachers in the early training group were assessed four times, as were the teachers from the late training group who trained during the spring. The remaining teachers in the late training group participated in two pre-training assessments: one concurrent with the pre-training assessment for the early group and one concurrent with the post-training assessment for the early training group. This allowed them to act as a passive control group for the early training group and was therefore assessed five times in total (see ).
Figure 1. Flow diagram based on the CONSORT 2010 Flow Diagram.
Participants
Teachers
Twenty-five primary school teachers (23F/2M) from seven different public mainstream schools in the same municipality in southern Sweden, grades 3–6, participated. The class sizes ranged from 17 to 37 students with a median of 22 students, which is just above the median class size in Sweden. In the municipality there is a larger proportion of students with a foreign background than the national average. The municipality in question had an ongoing refurbishment project regarding lighting and room acoustics; hence the light- and sound environments varied between schools. The schools were chosen to provide approximately the same number of teachers working in refurbished and non-refurbished classrooms. Grades 3–5 were chosen on the basis of the students’ age (9–11 years), the students had to be able to comprehend and complete a student-questionnaire (not reported here). The schools were contacted and the headmasters informed teachers in grades 3–5 about the project. The names of thirty-two teachers were thereafter passed on to the first author, responsible for the intervention. The first author gave spoken and written information about the study process and, the content, design, and process of the intervention. Seven teachers declined to participate after having received more information. Four did not wish to participate due to lack of time caused by sick-leave amongst colleagues. Three teachers were teaching in grade 2 and were therefore not included. Two teachers teaching in grade 6 were included. Eventually, 25 teachers (23F/2M) participated in the intervention program. Two teachers were later excluded from the data analysis due to too much missing information from the assessments (one participant from each group, both female), see .
Occasional absence was compensated by video-recordings for the teacher to watch later. Sessions with the majority of time spent on exercises were compensated for, the teacher then joined another subgroup. Seven teachers missed out on a part of one group session each, and this could not be compensated for. Reasons for missing a session were sickness, caring for sick children, scheduling conflicts, or due to a heavy workload. The demographics of the participating teachers is presented in .
Table 1. Distribution of the 25 participating teachers’ years of teaching, number of certified teachers (teachers that completed their education) and age.
Assessments
Hearing screening at 20 dB HL for frequencies .25, .50, 1, 2, 3, 4, 6, and 8 kHz was made before the intervention. Three teachers did not pass and were recommended to have further audiological examination. However, the slight hearing loss was not expected to have a negative effect on intervention outcomes.
Questionnaires
All the questionnaires have previously been validated in their original language. The Voice Handicap Index and QPS Nordic 34+ are validated in Swedish as well. Scorings and calculations were made according to the test manuals.
The Voice Handicap Index (VHI-11) (short version [Citation29], Swedish version [Citation30]) was used to target voice health. VHI-11 is a self-assessment of voice disorders and voice function. It has a core of 11 voice health statements to be answered on a 5-point scale (0 = never, 1 = almost never, 2 = sometimes, 3 = almost always, 4 = always). The total sum for all items is calculated and a higher score indicates a higher degree of subjective voice problems. An example statement is “I feel as though I have to strain to produce voice.” The questionnaire also includes a 10 cm visual analog scale (VAS) where the respondents are asked to mark their own assessment of their voice at the present time (0 = no voice disorders, 10 = maximum voice disorders).
Perceived Stress Questionnaire (PSQ [Citation31], Swedish version [Citation32]). PSQ emphasizes cognitive perceptions of stress rather than emotional states or specific life events. PSQ covers 30 statements describing experiences of stress applicable across a variety of situations. The statements are answered on a 4-point scale (1 = almost never, 2 = sometimes, 3 = often, 4 = almost always). The total sum for all items is used to calculate a PSQ-index ranging from 0 (no stress) to 1 (maximum stress). The scale is general or time limited (previous month). In this project, the time limited scale was used. Example statements are “You feel that too many demands are being made on you” and “You fear you may not manage to attain your goals.”
Copenhagen Burnout Inventory (CBI [Citation33], Swedish version [Citation34]). CBI is a questionnaire intended to measure burnout defined as fatigue and exhaustion in relation to specific domains. The form is divided into three scales addressing personal (6 questions), work related (7 questions) and client related (6 questions) fatigue. There are five response options for each item and depending on the question the response is either how often it is experienced (1 = always, 2 = often, 3 = sometimes, 4 = seldom, 5 = never/almost never) or to what extent one agrees (1 = to a very high degree, 2 = to a high degree, 3 = somewhat, 4 = to a low degree, 5 = to a very low degree). The answers are scored as 1 = 100, 2 = 75, 3 = 50, 4 = 25, 5 = 0. A mean score (i.e. a score between 0 and 100) is calculated both for all the items together and for the three subscales separately. A higher score indicates a higher degree of burnout. An example question from the client-related subscale (the word client is exchanged for student in accordance to the authors’ recommendation to use the appropriate term) is “Do you find it frustrating to work with students?”
Teachers' Sense of Efficacy Scale: Long Form: Subscale Classroom Management (TSES [Citation35], Swedish version [Citation32]). TSES classroom subscale covers 8 questions intended to target teachers sense of ability to manage the classroom and create pedagogical prerequisites despite distracting events. Responses are given on a 9-point scale ranging from 1 = nothing, 3 = very little, 5 = some influence, 7 = quite a bit and 9 = a great deal. Mean for the 8 items is calculated and a higher score indicates a greater sense of ability in managing the classroom. An example question is “How much can you do to control disruptive behavior in the classroom?”
QPS Nordic 34 + [Citation36]. A questionnaire developed by the Nordic Council that consists of 37 questions targeting self-assessment of psychological and social aspects at the work-place. Responses are given on a 5-point scale either on a frequency scale (1 = very seldom or never, 2 = rather seldom, 3 = sometimes, 4 = rather often, 5 = very often or always) or an intensity/amount scale (1 = very little or not at all, 2 = rather little, 3 = somewhat, 4 = rather much, 5 = very much). A mean score is calculated for the 37 items. An example question is “Can you influence decisions that are important for your work?”
Intervention
The intervention program aimed to increase teachers’ knowledge about classroom communication and to strengthen their practical skills by using evidence-based language learning interactions to support classroom communication. The interactions focused on were: using healthy voice technique; adapting voice use to the sound environment; optimizing body communication and improving language learning environments.
A collaborative learning approach was used under guidance and supervision of an SLP, the first author. According to Houmann and Saether [Citation37], rich opportunities to increase one’s own understanding, to receive feedback on teaching practices, observe competent model teachers and refine and develop teaching practices by learning from each other are required to improve language learning interactions. The intervention was designed accordingly. Group reflections on actual experiences were used to improve the teachers’ own communicative strategies and language learning techniques used in the classroom. This was one of several aspects to keep the training close to practice. Video-recordings and peer observations of real classroom situations were used. It was possible for the teachers to focus on specific areas within the intervention depending on the teachers’ needs and preferences.
Voice technique included a presentation on voice function in theory, advice on vocal hygiene and vocal health, and practical voice exercises (posture, breathing, and phonation). Voice ergonomics introduced actions to improve the conditions for verbal communication, both for the speaker and the listener. Voice ergonomic factors in their workplace such as air quality and possibility to voice rest were discussed. The teachers received the voice ergonomic assessment protocol developed by Sala et al. [Citation38] to be able to identify potential risk factors at their work-place. Room acoustics included information on sound environments in schools and how different aspects of the sound environment affect individuals. This information was provided by a guest lecturer, an acoustician specialized on educational facilities. This was later followed up by discussions and reflections about the sound environments at their workplaces. Teacher reflections were for example on ventilation system noise and high noise levels in the canteen. The discussions covered, e.g. how to manage excessive noise from students in the classroom. Language interaction aimed to raise awareness of and develop skills in classroom communication. The CsC Observation Tool [Citation21] (Swedish version [Citation39]) was used as an observation tool to make the teachers aware of how language learning environments, opportunities, and interactions can support oral language skills in students. Observations with the CsC were made by a colleague twice during the period of in-service training. Discussions included the teachers sharing of good practice on language interaction in the classroom. Body communication included SLPs input on different aspects of speech and body communication alternating with practical exercises and feedback on delivering a message, with variation in speech rate, pitch, stress, and intonation, in combination with gaze, mimics, gestures, and voice.
The sessions occurred after class at two of the schools. The group sessions were led by the SLP and lasted 1.5 h per week for five consecutive weeks. Besides the included domains, the sessions also included introduction and presentation of the training, discussions combining the different sessions together, dealing with expectations, previous knowledge, and experience within the domains. Video recordings from class were strongly recommended to teachers, but not compulsory. If not recorded in class, the participants were recorded during the training sessions. The recordings were watched in the training sessions and the teacher in focus received feedback on body communication and voice use from colleagues and the SLP. All recordings were made by a colleague and iPads available at the schools were used. An action-reflection-learning approach was used with different tasks of reflection on what the individual teacher had experienced and learned and how to put their new competence into practice.
Data analysis and statistics
To investigate the effects on the teachers’ vocal health and well-being, their responses on VHI-11 (visual analog scale + sum of statements), PSQ, CBI, TSES, and QPS Nordic 34 + were compared pre and post intervention. Post-intervention results are reported both directly after intervention and at the two follow-ups at 5-weeks and 3-months. All statistical analyses and plots were made using the statistical software R [Citation40]. Linear mixed-effects regression was used to assess changes over time, as this method has superior power and retains more data while still handling within-subject variance, compared to a regular ANOVA [Citation41,Citation42]. Maximal random effects were as far as possible retained in all models, following the recommendations from Barr and colleagues [Citation43]. The clustering structure was somewhat simplified since the ratio between the number of participants and the number of random effects was too low for the fully specified model to be computable. For this reason, the two subgroups training with sessions after each other starting from the 38th week of 2016 were collapsed into one, for all analyses. In practice, this implies that the analysis disregards within-group regularities among participants training at the same time but in different sessions, an impact that we expect to be minor to the model's fidelity. Linear mixed effects models were computed using the function “lme” from the R package “nlme” [Citation44]. Two participants were excluded from the analysis due to more than two data points missing (one participant from each training group) yielding 23 subjects for all analyses. Ten percent of the questionnaire data entries in Excel were verified by another project member with 100% concurrence.
The data on VHI-11 (both VAS and statements) were skewed towards the lower end. Therefore, all analyses were performed on the logarithms of these scales to mitigate some of the skewness. provides an overview of the questionnaire’s variables and a reminder of which questionnaires are designed so that a lower score is a more positive result and vice versa.
Table 2. Overview of questionnaires with respective range and values from validation studies of which some are based on clinical populations.
Ethics
This study was approved by the Regional Ethical Review Board in Lund (2016/567). The headmasters of the schools approved the project to be conducted at their schools. Informed, written consent was obtained from each participant.
Results
Descriptive data
All values from measure point 0 weeks pre-training are presented in , in order to enable a comparison with previous studies.
Table 3. Values from 0 weeks pre-training for all measures presented with mean, standard deviation, and number of responding participants.
Short-term training effect (early training group vs. late training group over first two measurements)
In a first set of analyses, the differences between pre- and post-intervention measures in the early training group were compared to the differences over the same time in the late training group, excluding the four participants that trained during the spring of 2017. This allowed a matched comparison of teachers training at different points in time while still being measured at the same calendar time points. The purpose of this analysis was to rule out the possibility of differences in workload over the semester accounting for the measured effects of training. Consequently, a total of 19 teachers were included in this analysis, 12 in the early training group and 7 in the late training group. The pre- and post-intervention measures correspond to measure points 0 weeks pre and 0 weeks post-training for the early training group, and five weeks pre-training and 0 weeks pre-training for the late training group, respectively. A linear mixed-effects model with VHI11-VAS (logarithmized) as dependent variable, (Measure point * Treatment group) as fixed factors and (Time | Subject) as random factors revealed a significant interaction between group and post-test (B = 1.54, p = .01), indicating an effect of the intervention. A follow up of this interaction in each group revealed that the early training group had increased their voice problem ratings (B = 1.26, p = .01), in contrast to the group that had not yet started their training, which had no significant changes. No effects at post-test nor any interaction effects were found for VHI11-sum (logarithmized), PSQ, CBI, TSES, or QPS Nordic 34 + (ps > .14), indicating no significant effect of the training for these measures on this short time scale. The groups were not equal on all measures at the pre-test; they differed in VHI-11 and PSQ. For VHI-11, the means are presented on the unlogarithmized scale, but t-tests were performed on the logarithmized scale. VHI differed both on VAS (Mearly training = 1.27, Mlate training = .18, t = 2.25, p = .039) and VHI-sum (Mearly training = 1.42, Mlate training = .14, t = 3.19, p = .006). However, the differences in VHI are not clinically relevant since both groups’ scores were far from what would be clinically considered a voice problem. There was also a small difference between the groups at the pre-test in PSQ (Mearly training = .33; Mlate training = .20, t = 2.9, p = .019). Both groups fall under the same category (low stress). Importantly, the regression analyses control for this baseline difference when intervention effects are estimated.
Intervention effects over time
We combined the early training and late training groups, including the previously excluded group that received their training starting in the second month of 2017 (N = 4), yielding an analysis containing all 23 participants. Six linear mixed-effects regressions were conducted, with (Measure point + Week of training) as fixed factors and (Time | Subject) as random factors. The week of training in the model (reference = 2016 week 38) was included to control for temporal effects of the school semester on the individual measurements as far as possible. The results of these regressions (coefficients and confidence intervals) are shown in , and the respective plots (mean values and regression confidence intervals) are shown in . The results can be summarized as follows.
Figure 2. Aggregated data from all teachers participating in the study. Points correspond to mean values and confidence intervals are the same as in , for the respective scales (see titles of sub-panels). The dotted line through the first measure point (Pre-training) indicates the baseline so that changes at the other points are more clearly visible. Note that confidence intervals overlap the baseline for some effects that are nevertheless significant (cf. ). This is due to small differences between predicted values and calculated means, as the model included covariates.
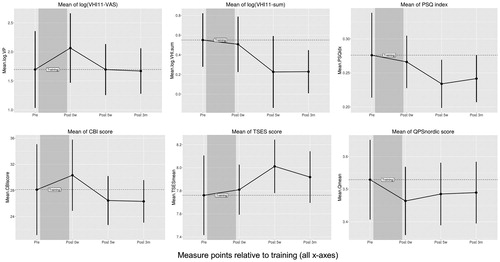
Table 4. Regression (LME) coefficients and confidence intervals for the analysis including all participants, all scales (subpanels a–f) and all measurements (except the delayed training-group’s five weeks pre-test) relative to training.
VHI11-VAS. The above reported finding that experienced voice problems increased significantly after training was not replicated when pooling all training groups. At 3-month follow-up, perceived voice problems had returned to baseline (, ).
VHI11-sum. Specifically reported voice problems show a decreasing trend post-treatment. At the three months post-treatment follow-up responses are significantly below baseline (p < .05) (, ).
PSQ index. Responses showed decrease below baseline post-intervention, significantly so at 5 weeks (p < .05) (, ).
CBI. The observed decrease below baseline was significant at five weeks post-treatment (p < .05). At the 3-month follow-up, the results were still but not significantly below baseline (, ). Further statistical analyses on the three separate subscales of CBI with linear mixed-effects regression, showed that the effect was driven almost entirely by the student-related subscale. The degree of burnout had decreased significantly (p < .05) at both 5-week follow-up (B = −6.85, CI = [−10.89, −2.81]), and 3-month follow-up (B = −4.55, CI = [−8.85, −0.25]), for this subscale, whereas the other two subscales showed only small and non-significant decreases below baseline.
TSES. Teachers estimated sense of self-efficacy increased post-intervention, but only significantly (p < .05) at five weeks post-intervention (, ).
QPS Nordic 34 +. There was no evidence that the intervention has an influence on QPS Nordic 34 +. Only small and non-significant changes were seen (, ).
Discussion
The present study used a teacher intervention program to investigate the effects on the teachers' vocal health, self-efficacy, and well-being, by comparing self-assessments before and after intervention. The intervention was designed to increase the teachers’ knowledge of classroom communication. It also aimed at strengthening practical skills in using evidence-based language learning interactions, adapting voice use to the acoustic environment, optimizing body communication and improving language learning environments to support communication fostering classrooms. The findings indicate that the intervention program improves self-reported vocal health, decreases the perception of stress and reduces degree of burnout while increasing self-efficacy, i.e. the sense of ability to manage the classroom and create pedagogical prerequisites despite distracting events such as disruptive behavior in the classroom or a noisy student.
The first research question of this study sought to determine whether the intervention improved teachers' vocal health, well-being, and self-efficacy after a relatively short intervention program. The short answer is yes, as there were positive and significant effects for all three aspects. The study also set out to answer how the effects of the intervention unfolded over time. The current study found that most of the effects had appeared by five weeks after intervention, in addition, a few results remained significant also three months after the intervention.
Self-assessment of vocal health (VHI-11)
Surprisingly, the ratings on self-reported voice problems pre-intervention () were lower than for the controls in previous studies () on both VHI11-VAS and VHI11-sum. This finding was unanticipated and is contrary to many studies showing that voice problems are common amongst teachers, e.g. [Citation47–49]. A possible explanation for this finding is the teachers’ view on what constitutes a voice problem. For example, both dysphonia and even aphonia were perceived by the first author when meeting the teachers during both intervention and data collection. However, the dysphonia/aphonia was apparently not considered as a problem by the teachers themselves.
Other teachers could describe their voices becoming strained but did not consider it a big problem. Morton and Watson [Citation50] found that despite their experience of voice problems, teachers were less likely to seek help and were more persevering with their problems compared to a non-teacher control group. Teachers in their survey thought the teaching situations caused their vocal problems and one-third had observed improvements in their vocal quality during the school holidays. This suggests that teachers may view their voice problems as an occupational hazard. It is thus important to increase the teachers’ awareness of the voice for their personal health and to increase the understanding of how their communication and voice affect the listeners [Citation26].
The voice problems rated on the visual analog scale (VHI11-VAS) increased immediately after intervention. This could be interpreted as increased awareness of the individual voice, rather than an actual increase in the problems, in line with clinical experience. There are two findings to support this interpretation. The sum of specific statements on voice problems (VHI11-sum) did not increase immediately after intervention and VHI11-VAS had returned to baseline at the 3-month follow-up. However, notably in spite of the quite low degree of voice problems pre-intervention, there was a significant decrease below baseline for VHI11-sum at the 3-month follow-up.
Well-being (PSQ and CBI)
Official statistics in Sweden show that stress is common in teachers [Citation11,Citation51]. In a survey carried out in 2015 by the teacher labor union’s magazine (Skolvärlden) including 1100 teachers, 78% of the teachers reported considering leaving the occupation, the majority due to workload and 46% due to often feeling stressed [Citation52]. We expected that teachers’ perceived stress would be higher in the present study, given the stress prevalence and the teachers descriptions of their workload.
Despite the low levels of stress (according to the categories by Bergdahl and Bergdahl [Citation45], ) rated before the intervention our results showed a significant improvement in well-being measured with the PSQ at the 5-week follow-up. We considered if the improvement could be due to that participating in the intervention added on to the teachers’ stress and hence, the perception of stress decreased when the intervention was finished. However, then, we would have expected the decrease to be larger directly after the intervention and that the stress ratings would return to baseline at the 3-month follow-up, which they did not. Another possible explanation could be that the intervention provided the teachers with new knowledge and tools for their work resulting in decreased stress ratings. Also, the mere participation in sharing thoughts and practice with peers could reduce the stress levels.
The experienced fatigue and exhaustion measured by CBI were at baseline just below the mean from the validation studies [Citation33] (). The experience of fatigue and exhaustion had decreased significantly at the 5-week follow-up. Our results for the student-related CBI subscale show significantly decreased the degree of burnout at both 5-week follow-up and 3-month follow-up. The results for the subscale covering questions related to work with the students were more salient than for the total scale. This result is interesting since the teachers seem less fatigued by their work with students and the intervention program aims to benefit communication with the students in the classroom.
Self-efficacy (TSES)
The teachers’ beliefs about their ability to manage students’ behavior in the classroom had increased significantly at the five-week follow-up. In combination with the decrease in the degree of burnout, this result is in line with previous studies showing a negative relation between teachers’ self-efficacy and burnout [Citation16]. Aloe et al. [Citation53] reported a relationship between classroom management self-efficacy and burnout. In comparison to the validation study across five countries by Klassen et al. [Citation46] (), the teachers in the current study had higher ratings already at baseline.
Self-assessment of psychological and social aspects at the work-place (QPS Nordic 34 +)
The present findings show that the self-assessments of psychological and social aspects at the work-place were almost unchanged during the whole study period. Thus, they seem not to be influenced by the intervention. This was an expected outcome since the aim of the intervention did not target aspects at the workplace. This questionnaire was included to check for possible changes in working conditions concurrent with the intervention. Due to the unchanging results at all measure points, we interpret that there were not any considerable structural, organizational changes at the workplace during the time of our study. This is consistent with the effects of the intervention being due to the actual intervention and not due to any changes in the workplace.
Out of the five questionnaires, only one (TSES) is validated on teachers. This should be considered when interpreting the results and might be a part of an explanation why the ratings of burnout and stress were lower than expected. There are many studies showing that voice problems are common in teachers e.g. [Citation47–49] and there are statistics showing that teaching is one of the occupations with both the highest numbers of sick-leave and work-related disorders due to stress [Citation11,Citation51]. Yet, the teachers in this study reported neither voice problems nor high levels of stress. More research of the possible interplay between burnout and voice problems is warranted. In a study by Holmqvist et al. [Citation54], a significant correlation was found between stress symptoms and the occurrence of voice symptoms. One possible explanation is that the present teachers have a high workload and therefore do not have the time to reflect on their own well-being to any greater extent. The teachers’ reports on their work life gave the impression that their work is rather intense.
Our experience suggests several crucial factors to consider when planning and performing a similar intervention study. First, the scope and extent of the study have to be fully understood by both teachers and headmasters, so that sufficient amount of time is provided for teachers to put theory into practice. The lack of time was brought up by the teachers several times in our discussions as well as in the overall evaluation of the intervention program. Despite several meetings during the semester before the study with the school management and with the headmasters where the project and the intervention were presented and discussed, several of the teachers had not understood, or had forgotten, that the training consisted of several sessions until they received spoken information directly from the first author. Our conclusion is that it is necessary to plan ahead and to communicate the intended projects a year in advance before the start, for the head masters to be able to allocate time for their teachers to fully engage in it.
Methodological considerations
Due to limitations in our ethical approval, video recordings of lessons as part of the data collection before and after the intervention were not allowed to be used as an evaluating tool but only as a training tool. Video-recordings and/or observations of the teachers acting in the classroom would have been optimal in order to evaluate any changes in classroom communication. Many of the teachers were first quite skeptic about video recording themselves as a part of the intervention. Afterward, several teachers emphasized that looking at the video recordings of themselves and getting feedback on their behavior were particularly important.
For those post-training changes compared to pre-training which were apparent from the 5-week follow-up or later, we lack a suitable control condition (as all teachers started their training at the latest after the second measurement). It is thus possible that something else may have caused the changes in responses at these data collections. However, the fact that we included groups of teachers training at three different periods in time and used their time of training as a covariate in the model alleviates this risk. A more thorough control structure would have been obtained if we let the study run for a longer period and with additional measure points. However, this would have been too time-consuming for the participants and it would have implied a large risk of attrition.
A larger sample size would be beneficial for statistical power. However, intervention studies are time consuming. This study included teachers from seven different schools in different parts of the municipality. This required increased time and challenged the logistics. In future studies, a contact or a research partner within the schools is recommended to help with issues of facilities, schedules, and other logistical concerns. Information needs to be very explicit when informing about an intervention study in schools to assure that the extent of the intervention and effort required has been fully appreciated. In our study, the extent had not been fully understood. Some of the assignments that were planned for between the sessions were not introduced to avoid an unrealistic burden on the teachers’ workload. One thing that was kept was the CsC Observation Tool. Despite being developed for younger grades, it did work in the grades in this study: 3–6. The sessions were mandatory. However, this piece of information was lost in the communication chain and did not reach all teachers.
A weakness in the present study could be that the SLP who led the intervention collected the questionnaires. There is, of course, a risk that the teachers wanted to please the SLP. The participating teachers were, however, informed that the questionnaires would be anonymized by another member of the project before they were analyzed, so the SLP would not know which teacher had answered which questionnaire. There was a total of 116 questions to be answered at each measure point and there was also other data collected that are not presented in this study. The extensive test battery along with the teachers’ heavy workload could also have influenced how teachers answered the questionnaires. The teachers’ lack of time was evident during the whole intervention. Unfortunately, they sometimes had to prioritize concurring courses or meetings.
A part of conducting practice-embedded educational research is the necessary adaptation to the schools’ logistic possibilities. In this case, the schools needed the teaching teams to be kept together. Hence, due to a rather small sample size and the lack of possibility to do a randomized control study based on individuals, the results must be interpreted with some caution. The teachers hence participated with their “normal” teaching teams that were randomly allocated to the training groups. The training groups were combined to include teachers from different schools, grades, and refurbished and non-refurbished schools.
Future implications
Swedish school teachers today are heavily burdened. This results in many sick-leaves, in teachers leaving the occupation, and work-related disorders are common [Citation10,Citation55]. Hence, it is of utmost importance to support their well-being in every possible way.
The intervention presented in this study improved the participating teachers’ well-being. To the best of our knowledge, improved well-being supports better communication in the classroom. Thus, teachers’ well-being is important not only for the individual teacher but also for the students. This type of intervention is relatively short in time, cost effective and could be adapted to the schools’ schedule and is recommended to schools as in-service training. Classroom communication training is often lacking in teacher education programs, at least in Sweden. It would, therefore, be even more advantageous to implement similar training already during teacher education. A couple of intervention studies give support to the effectiveness of teacher training, both as in-service training and training during teacher education. Goodyear conducted an intervention study on professional development, with a mixture of theoretical and practical content, which was adapted to the school's needs and logistical possibilities as well as the individual teachers’ different ways of learning [Citation56]. The results showed that sustained collaborative support from both a facilitator and colleagues had an impact on teachers’ practices and students’ learning.
Although not adapting a communication perspective, the intervention study by Simberg et al. [Citation57] showed that group voice therapy is an effective method to treat student teachers with mild voice disorders. A decrease in reports on vocal symptoms among students in the treatment group was significant at a three-month follow-up and 1 year after the intervention. This strengthens our belief in applying communication training in teacher education programs. Future studies within our project aim to further investigate the effects of the intervention. The future studies will examine room acoustics, potential change in teachers’ voice use and explore effects of the intervention on students’ well-being and self-efficacy. Finally, a qualitative paper with the purpose to evaluate the intervention is planned.
Conclusions
In summary, the intervention program improves teachers’ self-reported vocal health, decreases their perception of stress, and the degree of burnout while increasing their self-efficacy. Specifically, post-intervention measurements showed significant improvements in terms of lesser voice problems at the 3-month follow-up, and lower stress scores and higher self-efficacy at the 5-week follow-up. The assessment of burnout also showed a significant decrease in the student related subscale at both 5-week and 3-month follow-ups.
Teachers' vocal health, self-efficacy, and well-being are improved after the intervention and long-term effects can be inferred. The improvement is likely due to the intervention and not due either to temporal effects of the school semester or organizational changes. We thus conclude that training of voice and body communication can be recommended as in-service training for teachers and as a compulsory subject in teacher educational programs.
Acknowledgments
The authors wish to express their gratitude to the participants taking part in this study, to two anonymous reviewers whose comments greatly improved this article, and to Heike von Lochow for assisting with the first hearing screenings and teaching the procedure to the first author.
Disclosure statement
Viveka Lyberg-Åhlander is Deputy Editor-in-Chief of LPV.
Additional information
Funding
Notes on contributors
Suvi Karjalainen
Suvi Karjalainen is a PhD student at the Department of Clinical Sciences, Logopedics, Phoniatrics and Audiology at Lund University. Her PhD project focuses on the effects of a teacher intervention program on both teachers, their students and investigates the impact of differences in the classrooms’ acoustics.
Birgitta Sahlén
Birgitta Sahlén is Professor in Speech Pathology at the Department of Clinical Sciences, Logopedics, Phoniatrics and Audiology, Lund University, Sweden. Her main research focus is on cognition and communication in normal hearing children (SLI) and children with hearing loss and language problems.
Andreas Falck
Andreas Falck received his PhD in psychology from Lund University and is currently a post-doctoral researcher at Institut Nicod in Paris, France. His research interests include attention and learning in social contexts, developmental social cognition, and statistical modeling.
Jonas Brännström
Jonas Brännström is an associate professor in audiology at Lund University in Sweden and works as a senior lecturer at the audiology and speech pathology programs. His research interests include psychoacoustics, cognition and hearing (including tinnitus), hearing rehabilitation, hearing aid outcomes, and tele-audiology.
Viveka Lyberg-Åhlander
Viveka Lyberg-Åhlander is a reg. Speech Pathologist and Assistant Professor at the department of Logopedics, Phoniatrics and Audiology, Lund University. Her researchfocus is voice and voice disorders with starting point from the teacher voice in relation to the sound environment in the classroom and the teachers’ occupational and vocal health.
References
- Kob M, Behler G, Kamprolf A, et al. Experimental investigations of the influence of room acoustics on the teacher’s voice. Acoust Sci Tech. 2008;29:86–94.
- Lyberg-Åhlander V, Rydell R, Löfqvist A. Speaker's comfort in teaching environments: voice problems in Swedish teaching staff. J Voice. 2011;25:430–440.
- Sala E, Airo E, Olkinuora P, et al. Vocal loading among day care center teachers. Logoped Phoniatr Vocol. 2002;27:21–28.
- Sapir S, Keidar A, Mathers SB. Vocal attrition in teachers: survey findings. Int J Lang Commun Disord. 1993;28:177–185.
- Kristiansen J, Persson R, Lund SP, et al. Effects of classroom acoustics and self-reported noise exposure on teachers' well-being. Environ Behav. 2013;45:283–300.
- Osman H, Sullivan JR. Children’s auditory working memory performance in degraded listening conditions. J Speech Lang Hear Res. 2014;57:1503–1511.
- Shield BM, Dockrell JE. The effects of environmental and classroom noise on the academic attainments of primary school children. J Acoust Soc Am. 2008;123:133–144.
- Lyberg-Åhlander V, Brännstrom KJ, Sahlen BS. On the interaction of speakers' voice quality, ambient noise and task complexity with children's listening comprehension and cognition. Front Psychol. 2015;6:871.
- von Lochow H, Lyberg-Åhlander V, Sahlen B, et al. The effect of voice quality and competing speakers in a passage comprehension task: performance in relation to cognitive functioning in children with normal hearing. Logoped Phoniatr Vocol. 2018;43:11–19.
- Lyberg-Åhlander V. Voice use in teaching environments: speakers' comfort [dissertation]. Lund (Sweden): Lund University; 2011.
- Swedish Work Environment Authority. Arbetsmiljöstatistik Rapport 2014:4. Arbetsorsakade besvär [Work environment statistics report 2014:4. Work-related disorders]. In: Ponton Klevestedt A, editor. Arbetsmiljöstatistik. Stockholm (Sweden): Swedish Work Environment Authority; 2014.
- Arvidsson I, Hakansson C, Karlson B, et al. Burnout among Swedish school teachers – a cross-sectional analysis. BMC Public Health. 2016;16:1–11.
- Schwarzer R, Hallum S. Perceived teacher self-efficacy as a predictor of job stress and burnout: mediation analyses. Appl Psychol. 2008;57:152–171.
- Dicke T, Parker PD, Marsh HW, et al. Supplemental material for self-efficacy in classroom management, classroom disturbances, and emotional exhaustion: a moderated mediation analysis of teacher candidates. J Educ Psychol. 2014;106:569–583.
- Bandura A. Self–efficacy: the exercise of control. New York (NY): W. H. Freeman and Company; 1997.
- Brown CG. A systematic review of the relationship between self-efficacy and burnout in teachers. Educ Child Psychol. 2012;29:47–63.
- Beebe SA. The role of nonverbal communication in education: research and theoretical perspectives. Annual Meeting of the Speech Communication Association; 1980 Nov 13–16; New York, NY.
- Carter A. Carter review of Initial Teacher Training (ITT). London (UK): Department for Education; 2015 [2018 Sep]. Retrieved from: https://www.gov.uk/government/publications/carter-review-of-initial-teacher-training.
- Dockrell JE, Lindsay G. Children with specific speech and language difficulties-the teachers' perspective. Oxford Rev Educ. 2001;27:369–394.
- Dockrell JE, Bakopoulou I, Law J, et al. Capturing communication supporting classrooms: The development of a tool and feasibility study. Child Lang Teach Ther. 2015;31:271–286.
- Dockrell JE, Bakopoulou I, Law J, et al. Developing a communication supporting classrooms observation tool. London (UK). Department for Education; 2012. (DFE-RR247-BCRP8); [2016 Sep]. Retrieved from: https://www.gov.uk/government/publications/developing-a-communication-supporting-classrooms-observation-tool
- Haake M, Hansson K, Gulz A, et al. The slower the better? Does the speaker's speech rate influence children's performance on a language comprehension test? Int J Speech Lang Pathol. 2014;16:181–190.
- Lyberg-Åhlander V, Haake M, Brännstrom J, et al. Does the speaker's voice quality influence children's performance on a language comprehension test? Int J Speech Lang Pathol. 2015;17:63–73.
- Sahlen B, Haake M, von Lochow H, et al. Is children's listening effort in background noise influenced by the speaker's voice quality? Logoped Phoniatr Vocol. 2018;43:47–55.
- von Lochow H, Lyberg-Åhlander V, Sahlen B, et al. The effect of voice quality and competing speakers in a passage comprehension task: perceived effort in relation to cognitive functioning and performance in children with normal hearing. Logoped Phoniatr Vocol. 2018;43:32–41.
- Evitts PM, Starmer H, Teets K, et al. The impact of dysphonic voices on healthy listeners: listener reaction times, speech intelligibility, and listener comprehension. Am J Speech Lang Pathol. 2016;25:561–575.
- Starling J, Munro N, Togher L, et al. Training secondary school teachers in instructional language modification techniques to support adolescents with language impairment: a randomized controlled trial. LSHSS. 2012;43:474–495.
- de Vries S, Jansen E, van de Grift W. Profiling teachers' continuing professional development and the relation with their beliefs about learning and teaching. Teach Teach Educ. 2013;33:78–89.
- Rosen CA, Lee AS, Osborne J, et al. Development and validation of the voice handicap index-10. Laryngoscope. 2004;114:1549–1556.
- Nyman M, Åradsson S. Voice Handicap Index-Lund-11. Ett självskattningsformulär för patienter med röstbesvär. Översättning, bearbetning och validering. [Voice Handicap Index-Lund-11. A self-assessment form for patients with voice problems. Translation, adaptation and validation] [master’s thesis]. Lund (Sweden): Lund University; 2008.
- Levenstein S, Prantera C, Varvo V, et al. Development of the perceived stress questionnaire: a new tool for psychosomatic research. J Psychosom Res. 1993;37:19–32.
- Wedholm D, Wideklint M. Effekten av Psykologisk Fallkonsultation på Förskollärare – En Grupprandomiserad Studie. [The Effect of Consultee–Centered Case Consultation on Preschool Teachers – A Group Randomized Trial] [master’s thesis]. Örebro (Sweden): Örebro University; 2015.
- Kristensen TS, Borritz M, Villadsen E, et al. The Copenhagen burnout inventory: a new tool for the assessment of burnout. Work Stress. 2005;19:192–207.
- Arneson H. Empowerment and health promotion in working life [dissertation]. Linköping (Sweden): Linköping University; 2006.
- Tschannen-Moran M, Hoy AW. Teacher efficacy: capturing an elusive construct. Teach Teach Educ. 2001;17:783–805.
- Dallner M. Validation of the General Nordic Questionnaire (QPSNordic) for Psychological and Social Factors at Work. Copenhagen (Denmark): Nordic Council of Ministers; 2000.
- Houmann A, Saether E. Using a survey on creativities as reflective practice and for reforming practice in music teacher education. In: Burnard. P, editor. Developing creativities in higher music education. International perspectives and practices. Abingdon (UK): Routledge; 2014. p. 176–185.
- Sala E, Hellgren U-M, Ketola R, et al. Röstergonomisk bedömning av arbetsmiljön. Handbok i röstergonomisk utredning. [Voice ergonomic assessment in work environment – handbook and checklist]. Sjöholm M, Sjöholm B, translators; Metanen V, editor. Helsinki (Finland): The Finnish Institute of Occupational Health; 2012. Swedish and Finnish.
- Waldmann C, Dockrell J, Sullivan K. Supporting indigenous bilingual children’s oral language development. ALAA/ALANZ/ALTAANZ 2015: Learning in a Multilingual World; 2015; Dec 1; Adelaide (Australia). p. 132–132.
- R Core Team. R: a language and environment for statistical computing. Vienna (Austria): R Foundation for Statistical Computing; 2017. Available from: https://www.R-project.org/.
- Pinheiro JC, Bates DM. Mixed–effects models in S and S-PLUS. [e-book]. New York (NY): Springer; 2000.
- Tasca GA, Gallop R. Multilevel modeling of longitudinal data for psychotherapy researchers: I. The basics. Psychother Res. 2009;19:429–437.
- Barr DJ, Levy R, Scheepers C, et al. Random effects structure for confirmatory hypothesis testing: Keep it maximal. J Mem Lang. 2013;68:255–278.
- Pinheiro J, Bates D, DebRoy S, et al. nlme: Linear and Nonlinear Mixed Effects Models. R package version 3.1–131. 2017. Available from: https://CRAN.R-project.org/package=nlme
- Bergdahl J, Bergdahl M. Perceived stress in adults: prevalence and association of depression, anxiety and medication in a Swedish population. Stress Health. 2002;18:235–241.
- Klassen RM, Bong M, Usher EL, et al. Exploring the validity of a teachers’ self-efficacy scale in five countries. Contemp Educ Psychol. 2009;34:67–76.
- Smith E, Lemke J, Taylor M, et al. Frequency of voice problems among teachers and other occupations. J Voice. 1998;12:480–488.
- Roy N, Merrill RM, Thibeault S, et al. Prevalence of voice disorders in teachers and the general population. J Speech Lang Hear Res. 2004;47:281–293.
- Lyberg Åhlander V, Rydell R, Fredlund P, et al. Prevalence of voice disorders in the general population, based on the Stockholm public health cohort. J Voice. 2018.
- Morton V, Watson DR. The teaching voice: problems and perceptions. Logoped Phoniatr Vocol. 1998;23:133–139.
- The Swedish Social Insurance Agency. Startade sjukfall per 1000 efter yrke och diagnos 2005–2014 [Started sickness cases per 1000 by profession and diagnosis 2005–2014]. Stockholm (Sweden): Försäkringskassan; 2015. Swedish.
- Stridsman S. Mer än tre av fyra lärare funderar på att sluta. [More than three out of four teachers consider quitting their job]. Skolvärlden [Internet]. 2015 Dec 10 [cited 2018 Mar 2]. Available from: http://skolvarlden.se/artiklar/mer-tre-av-fyra-larare-funderar-pa-att-sluta
- Aloe AM, Amo LC, Shanahan ME. Classroom management self-efficacy and burnout: a multivariate meta-analysis. Educ Psychol Rev. 2014;26:101–126.
- Holmqvist S, Santtila P, Lindstrom E, et al. The association between possible stress markers and vocal symptoms. J Voice. 2013;27:787.e1–787.e10.
- Fritzell B. Voice disorders and occupations. Logoped Phoniatr Vocol. 1996;21:7–12.
- Goodyear VA. Sustained professional development on cooperative learning: impact on six teachers' practices and students' learning. Res Q Exerc Sport. 2017;88:83–94.
- Simberg S, Sala E, Tuomainen J, et al. The effectiveness of group therapy for students with mild voice disorders: a controlled clinical trial. J Voice. 2006;20:97–109.