Abstract
Objectives. A systematic estimation of the effects of some clinically important artefact provoking and artefact-preventing manoeuvres. Design. A test protocol for the evaluation of technical modifications of continuous ECG recordings was tested in 17 patients. The programme comprised ECG recordings during five artefact-provoking manoeuvres (slight shaking of the ECG cables, rotating shoulders, slight electrode touching, washing, teeth-brushing) and two simple artefact-preventing manoeuvres (taping ECG cables and covering electrodes with paper cups). Results. The artefact-provoking manoeuvres induced a substantial increase in artefactual ECG. The artefact-preventing manoeuvres only incompletely prevented this increase. Conclusion. There is a great need of technical improvements to reduce the distortion of ECG by artefacts. The test protocol developed by us exposes a broad spectrum of different categories of ECG qualities and is therefore suitable for evaluating technical improvements concerning artefactual ECG.
Continuous ECG monitoring is an essential diagnostic procedure at modern cardiac care units. This procedure often results in diagnostic findings of major importance in patients with chest pain, syncope and palpitations, for example. ECG involves recording electrical activity generated by cardiac depolarisation and repolarisation, as detected by electrodes on the skin. The resulting electrical potentials are only a few millivolts, at most, and occur over a frequency range of 0.05 to 100 Hertz. Signals of similar frequency and of similar or larger amplitude generated by non-cardiac sources cause ECG artefacts. Some artefacts are produced physiologically, which is exemplified by muscle activity caused by tremor in Parkinson's disease. Most artefacts, however, have no physiological background and are produced by electromagnetic interference or poor electrode contact, for example. Artefacts can be substantially reduced by limiting the frequency range of the recorder at both the upper and lower ends of the frequency band Citation1. A low-distortion filter method to reject muscle noise has also been described Citation2.
Artefacts often represent a major problem during continuous ECG monitoring. Some artefacts are easily recognisable as such and simply result in periods in which information on the appearance of the patient's ECG is lacking. Occasionally, however, artefacts may closely mimic clinically important conditions such as ventricular tachycardia Citation3–7 with serious consequences for the patient, who may even be subjected to unnecessary diagnostic procedures, including cardiac catheterisation and the implantation of cardiac devices Citation4. Finally, the misleading computerised interpretation of artefacts often produces a large number of false alarms, resulting in a noisy, stressful working environment for the staff at cardiac care units.
To some extent, simple manoeuvres such as skin abrasion may reduce ECG artefacts Citation8–11. However, further technical improvements to reduce the frequency of artefacts in ECG are urgently needed. Future technical modifications must, however, be evaluated in a systematic way to make sure that the intended reduction in the frequency of artefacts really occurs.
According to the staff at our coronary care unit, some daily life activities, such as teeth-brushing, are especially prone to induce ECG artefacts. These activities are therefore potentially suitable to form the components of a standardised, clinically relevant protocol for testing the artefact reducing ability of different modifications of technical devices. The present paper relates to an estimation of the artefact producing ability of five such activities. It also includes an evaluation of the artefact-reducing ability of two simple technical modifications, which are easy to carry out in routine clinical work.
Methods
Sample
The study involved 17 patients subjected to continuous ECG recording at the Department of Cardiology, Central Hospital, Västerås, Sweden. The age range was 55 to 82 years and there were six females and eleven males. Four patients had atrial fibrillation and 13 patients had sinus rhythm.
Procedures
The investigation was performed in a real-life clinical context with members of the ordinary staff applying ECG electrodes and interpreting the ECG recordings
Two-channel ECG equipment, Danica T2025, was used. This equipment has been used at our department for several years and is also used extensively in the Scandinavian countries. Coronary care nurses applied the ECG electrodes according to their usual routines. One bipolar recording was obtained between an electrode (negative) near the cardiac apex and an electrode (positive) under the right clavicle. Another bipolar ECG recording was obtained between the cranial (positive electrode) and caudal (negative electrode) parts of the sternum. Finally, a neutral electrode was centrally positioned on the sternum. The nurses performed skin preparations if they felt this was necessary. Disposable, pregelled silver/silver chloride button electrodes (ConMed Corporation, Utica, NY, USA) with an area of 3.4 cm2 were used.
Protocol
For each patient, a test programme designed to provoke artefacts, including the following items, was performed: 1) active rotation of the arms; 2) movements imitating washing of the upper part of the body; 3) movements imitating teeth-brushing; 4) slight shaking of the cables connecting the skin electrodes with the box containing equipment for analysing and sending the ECG signal to the central monitor and 5) slight touching of the skin electrodes performed by the test leader. One ECG strip during each of these five procedures was selected. The five artefact-provoking manoeuvres were repeated with and without each of the following techniques designed to reduce artefacts: 1) fixation of the cables by means of tape; 2) covering the skin electrode with cups made of stiff paper and 3) a combination of these two manoeuvres. The test programme was performed with the patients in a sitting position.
From each combination of the above manoeuvres, one 30-second ECG strip was recorded. As illustrated in and , the number of combinations was 24. The length of artefactual ECG recordings during basal conditions (no provocation/no prevention) was calculated as the mean of the length of artefactual ECG in three 30-second ECG strips.
Table I. Perfect ECG for QRS interpretation.
In eight patients, another member of our staff repeated the above programme with artefact-producing and artefact-reducing manoeuvres after applying the ECG devices. This means that the test protocol was performed a total of 25 times using 17 patients. Because of atrial fibrillation, the influence of the artefacts on the P wave could only be studied in 21 of the 25 performances of the programme.
The ECG strips were analysed separately for QRS complexes and P waves. Every part of the strip was categorised as perfect, when the recordings from both ECG channels were free of artefacts, and valueless, when neither of the ECG channels could be interpreted because of artefacts. The remaining parts of the ECG were categorised as being of intermediate quality. The cardiologist (GN) performed this categorisation blinded to the patient's identity and the type of manoeuvre used.
Statistics
Differences were tested for statistical significance between the proportions of perfect and valueless ECGs with and without any of the artefact-provoking manoeuvres and with and without any of the artefact-preventing manoeuvres.
Due to the non-normality of data distribution the paired differences between the lengths of ECGs in different categories of quality were tested using Wilcoxon's signed rank test. One-tailed instead of two-tailed exact p-values were computed, assuming that the possibility of improving ECG quality by means of artefact-provoking manoeuvres and of impairing ECG quality by artefact-preventing manoeuvres was unlikely. The Statistical Package of Social Sciences (SPSS), version 11.0, was used for all analyses. P-values of < 0.05 were regarded as significant.
Differences between ECG quality relating to the application of the ECG recording device by two different persons in eight patients were tested by the Mann-Whitney test.
Results
As the electrical activity originating from the atria is much smaller than that from the ventricles, it is natural that artefacts more commonly disturb the P waves than the QRS complexes. Examples of artefacts obscuring the interpretation of QRS complexes are given in . The mean percentage of perfect and valueless ECG strips from each combination of artefact-provoking and artefact-preventing manoeuvre is given in and for the QRS complexes and in and for the P waves. Furthermore the proportions of different categories of ECG quality during artefact provocation are illustrated in and .
Figure 1. Examples of ECG recordings distorted by artefact provocations. Lines below the tracings indicate artefactual ECG. A and B: slight touching of the skin electrodes. C and D: teeth-brushing. E: rotation of the arms. In recording A, for example, some parts of the ECG are valueless for interpretation because of the concealment of ordinary P waves and QRS complexes. In recording B, QRS complexes but not P waves can be discerned.
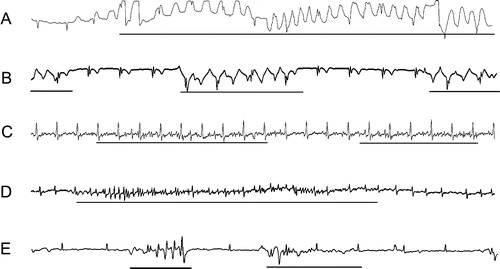
Figure 2. Mean percentage of categories of quality during different types of artefact provocation. QRS complexes without artefact prevention.
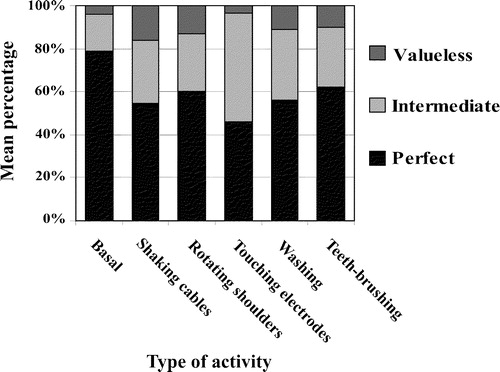
Figure 3. Mean percentage of categories of quality during different types of artefact provocation. P waves without artefact prevention.
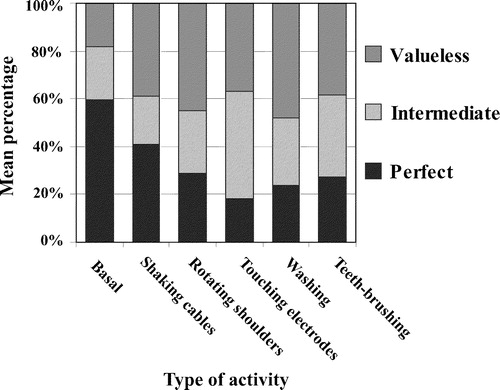
Table II. Valueless ECG for QRS interpretation.
Table III. Perfect ECG for P wave interpretation.
Table IV. Valueless ECG for P wave interpretation.
When it came to QRS complexes, the artefact-provoking manoeuvres generally had a more pronounced effect on reducing perfect ECGs than on increasing valueless ECGs. This was especially the case in connection with slight touching of the electrodes. The impairment in QRS quality by artefact-provoking manoeuvres was reduced, but it could not be avoided by the artefact-preventing measures. QRS artefacts provoked by touching electrodes could largely be prevented by placing cups over the electrodes. The observations relating to artefact-distorted P waves were similar to those relating to artefact-distorted QRS complexes. Placing paper cups over the electrodes had a striking artefact preventing ability with regard to P waves.
Even without artefact-provoking manoeuvres, there were considerable parts of the ECG distorted by artefacts, which could not be improved using cups or tape. Evidently, more effective technical improvements are needed to avoid these artefacts. The most striking effects of tape and cups are found in artefact-provoking situations and this applies in particular to cups while touching the electrodes. Touching of this kind is difficult to avoid in patients wearing clothes on their chest.
The difference between applications of the ECG recording device by two different persons was tested for all combinations of artefact-preventing and artefact-provoking manoeuvres described in (24 combinations in each table; a total of 96 combinations). A significant difference (p < 0.05) was found in four of these 96 comparisons. In three of these four comparisons, the ECG from the first applier of the device was the most artefactual (P wave/perfect ECG /no provocation/no prevention, P wave/perfect ECG/electrode touching/no prevention, and P wave/valueless ECG/teeth-brushing/ covering electrodes in combination with taping the cables). In one comparison, the reverse was true (QRS complex/perfect ECG/teeth-brushing/covering the electrodes in combination with taping the cables). These findings are probably due to chance in view of the fact that as many as 96 comparisons were performed.
The percentage of perfect ECGs for QRS interpretation without artefact-provoking andartefact-preventing manoeuvres was skewly distributed in the patient cohort (median 93; interquartile range 63 – 100). In the same way, an uneven distribution was found concerning perfect and valueless ECGs, regarding both QRS complexes and P waves, in the other combinations of artefact-provoking and artefact preventing manoeuvres (data not shown).
Discussion
The ECG signal is derived from differences in electrical potential between two electrodes as a result of cardiac action. It is well known that artefacts induced by electromagnetic and electrostatic interference easily swamp the signal. Several technical modifications to eliminate artefacts have been described. Abrasion and pricking of the skin improves the quality of the ECG but may cause skin irritation Citation9. The introduction of the floating silver/silver chloride electrode has eliminated motion artefacts and noise caused by the electrode Citation10. Our investigation confirms that substantial technical improvements can be achieved by simple measures such as placing paper cups over the electrodes and fixing the ECG cables with tape. However, a need for further and more sophisticated technical improvements to devices for continuous ECG recording still remains. These improvements would considerably improve the clinical utility of continuous ECG recording and expand the applications of the technique.
It is important to confirm that technical innovations really improve the quality of ECG recordings in a relevant clinical context. We feel that the test protocol investigated by us, which contains both artefact-provoking and simple artefact-preventing measures, is of considerable value for this purpose. Our protocol is not unreasonably time consuming and exposes a broad spectrum of different categories of ECG qualities enabled by clinically relevant simple artefact-provoking and artefact-preventing manoeuvres.
This study was supported by the Knowledge Foundation, Sweden and the Swedish Agency for Innovation Systems (VINNOVA).
References
- Jones PL. Artefact and safety in ECG monitoring. Proc R Soc Med 1973; 66: 1211–14
- Wei D, Harasawa E, Hosaka H. A low-distortion filter method to reject muscle noise in multi-lead electrocardiogram systems. Front Med Biol Eng 1999; 9: 315–30
- Lin SL, Wang SP, Kong CW, Chang MS. Artefact Simulation Ventricular and Atrial Arrhythmia. Jpn Heart J 1991; 32: 847–51
- Knight BP, Pelosi F, Michaud GF, Strickberger SA, Morady F. Clinical Consequences of Electrocardiographic Artefact Mimicking Ventricular Tachycardia. N Engl J Med 1999; 341: 1270–4
- Srikureja W, Darbar D, Reeder GS. Tremor-induced ECG artefact mimicking ventricular tachycardia. Circulation 2000; 102: 1337–8
- Chase C, Brady WJ. Artifactual electrocardiographic change mimicking clinical abnormality on the ECG. Am J Emerg Med 2000; 18: 312–6
- Knight BP, Pelosi F, Michaud GF, Strickberger SA, Morady F. Physician interpretation of electrocardiographic artefact that mimics ventricular tachycardia. Am J Med 2001; 110: 335–8
- Tam HW, Webster JG. Minimizing electrode motion artefact by skin abrasion. IEEE Trans Biol Eng Comput 1977; 24: 134–9
- Burbank DP, Webster JG. Reducing skin potential motion artefact by skin abrasion. Med Biol Eng Comput 1978; 16: 31–8
- Webster JG. Reducing Motion Artefacts and Interference in Biopotential Recording. IEEE Trans Biomed Eng 1984; 31: 823–6
- Oster CD. Improving ECG trace quality. Biomed Instrum Technol 2000; 34: 219–22