
Abstract
Objectives: We have noticed an increasing number of publications in relation to atrial fibrillation (AF) based on Swedish and Danish health care registries and therefore found it of interest to perform a systematic review of study aims, data sources, exposures, outcomes, journal impact factor, and citation statistics.
Materials and methods: We searched PubMed from 2000 to 31 December 2014. We included publications which were entirely or partly based on administrative registries and clinical quality databases, and where AF defined the study population or constituted the study exposure or outcome.
Results: Our review returned 1445 studies, of which 173 met the criteria for inclusion in the reviews. We noticed an abundant diversity in study aims, data sources, exposures, and outcome. The annual number of publications increased from 1 to 50. The mean (range) and median journal impact factor in the year of publication was 6.9 (0.8–51.7) and 5.7. The total cumulated number of citations up to the end of 2014 for all 173 publications was 3721, and the mean (range) and median cumulated number of citations per publication was 22.4 (0–250) and 6.0, respectively.
Conclusions: The number of registry-based studies on AF reported from Sweden and Denmark increased substantially from 2000 to 2014, had a great diversity, were well cited and have added information to the understanding of AF epidemiology.
Introduction
Atrial fibrillation (AF) is a major public health and clinical challenge due to the increasing prevalence and the high costs of the disease. AF is associated with a substantial risk of dementia,[Citation1] stroke,[Citation2] systemic embolism,[Citation3] heart failure,[Citation4] and death.[Citation5] Many aspects of AF remain to be further explored including the etiology and outcome, the effectiveness and safety of applied care, and the organization of care pathways. Furthermore, continuously updated and accurate information on the trends in the epidemiology of AF is required for health care planners and decision makers. Sweden and Denmark host a wide range of population-based administrative population and health care registries including clinical quality databases, holding individual-level information about key aspects of public life and health. These registries include basic demographic information (e.g. date of birth and emigration and vital status) as well as detailed health care data (e.g. dispensed drug prescriptions) and contacts with hospital and general practitioners linked to the unique personal identification numbers that are given to all inhabitants upon birth or immigration, and constitute potentially valuable data sources for studies requiring large populations, large number of outcomes, for studies on rare occurrences, for long-term follow-up and for studies that cannot use randomization for practical and ethical reasons.[Citation6] Coupling of registry information may therefore have an important role to play in unraveling outstanding questions about AF and may assist stakeholders, including patients, clinicians, administrators, and policymakers, in making informed choices on AF prevention and treatment. In the present context, we consider registry-based studies as studies based on data sources that were mainly generated for administrative purposes. An important requirement for this type of studies is that existing registry data can be used in legally approved research without obtaining informed consent from the registered. Research using registry linkages is built on confidence and relies on ethical evaluation to make sure that registry linkages do not provide direct identifiable information.
In order to provide an overview of the contributions by the administrative population and health care registries, including clinical quality databases, in Sweden and Denmark to research on AF epidemiology, we conducted a review of published articles (including early online publications) on AF based on such registries during 2000–2014.
Methods
Structured literature searches were executed in PubMed 31 December 2014 by a research librarian:
Search 1: (“Sweden”[MeSH Terms] OR “Sweden”[All Fields]) AND (“atrial fibrillation”[MeSH Terms] OR (“atrial”[All Fields] AND “fibrillation”[All Fields]) OR “atrial fibrillation”[All Fields]) AND (“2000/01/01”[PDAT]: “2014/12/31”[PDAT]).
Search 2: (“Denmark”[MeSH Terms] OR “Denmark”[All Fields]) AND (“atrial fibrillation”[MeSH Terms] OR (“atrial”[All Fields] AND “fibrillation”[All Fields]) OR “atrial fibrillation”[All Fields]) AND (“2000/01/01”[PDAT]: “2014/12/31”[PDAT]).
Search 3: (“Sweden”[MeSH Terms] OR “Sweden”[All Fields]) AND (“atrial fibrillation”[MeSH Terms] OR (“atrial”[All Fields] AND “fibrillation”[All Fields]) OR “atrial fibrillation”[All Fields]) AND (“registries”[MeSH Terms] OR “registries”[All Fields] OR “registry”[All Fields]) AND (“2000/01/01”[PDAT]: “2014/12/31”[PDAT]).
Search 4: (“Denmark”[MeSH Terms] OR “Denmark”[All Fields]) AND (“atrial fibrillation”[MeSH Terms] OR (“atrial”[All Fields] AND “fibrillation”[All Fields]) OR “atrial fibrillation”[All Fields]) AND (“registries”[MeSH Terms] OR “registries”[All Fields] OR “registry”[All Fields]) AND (“2000/01/01”[PDAT]: “2014/12/31”[PDAT]).
We excluded duplicate publications and all publications that were not registry-based. We included publications which were based on populations of AF patients or where AF was the study exposure or outcome. Each publication was examined for information on data sources, study purpose, and exposure and outcome measures. In addition, we retrieved information for each publication on number of authors, journal impact factor in publication year, or most recent reported impact factor to publication year, and the cumulated number of citations per 31 December 2014. Information on impact factor was obtained from Journal Citations Reports®. If a journal was not included in Journal Citations Reports®, we sought information about impact factor on the journal’s web page. The cumulated number of citations was retrieved from Web of Science Core Collection. If a publication’s cumulated number of citations was not included in Web of Science, we used Scopus.
Results
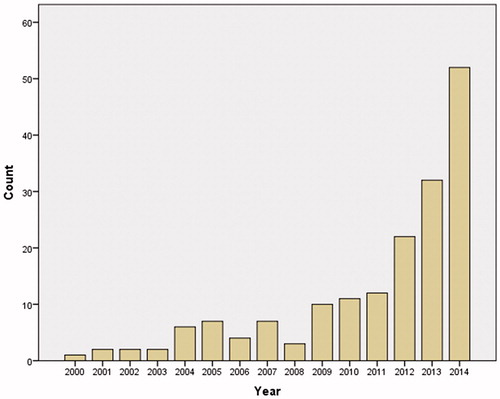
shows the flow diagram of the retrieved publications. Among 1445 retrieved records, 199 were duplicates, and 1073 publications were not registry-based. Thus, 173 studies were included in this review. These studies have reference numbers from s1–s173, and the reference list can be found in the supplement. shows that the number of publications by year increased from 1 to 50.
Figure 1. Flow diagram of retrieved publications.
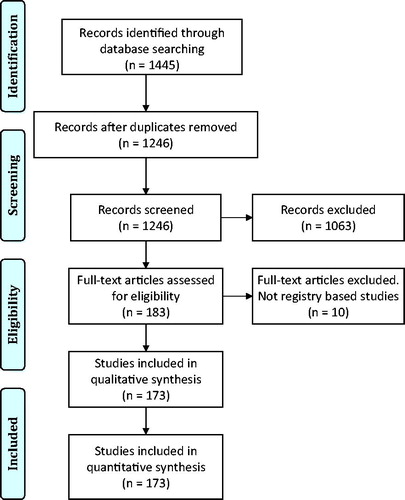
Figure 2. Annual number of registry-based studies on atrial fibrillation published from Sweden and Denmark, 2000–2014.
Data sources
Twenty-eight mandatory national administrative population and health care registries including clinical quality databases were used as data sources in the included publications ().
Table 1. National data sources used for registry-based studies on atrial fibrillation in Sweden and Denmark, 2000–2014.
A number of voluntary population-based cohorts have been used as a basis for registry-based follow-up studies on AF, and included Malmö Diet and Cancer (MDC) study (s1–s6), Malmö Prevention Project (s7–s10), Cohort of Swedish Men (COSM), Västmanland and Örebro counties cohort study (s11–s13), Swedish Mammography Cohort (SMC), Västmanland and Uppsala counties cohort study (s12, s13), The Study of Men Born in 1913 and 1923 (s14), The Primary Prevention Study (s15–s17), Screening cohort (Malmö) (s18), Seven prospective Swedish cohort studies (s19), Good Ageing in Skåne (s20), The Kungsholmen Project (s21), Danish Diet Cancer and Health study (s22–s34), Copenhagen City Heart Study (s35–s42), Copenhagen General Population Study (s35–s37), and Copenhagen Holter Study (s43). In addition, a number of local data sources such as data located to an administrative region, a city, one or more hospitals, or a cluster of general practitioners have been used (s43–s80).
Risk factors for AF
A number of exposures have been examined as potential risk factors for AF. Life style related risk factors included smoking (s25), Scandinavian moist tobacco (snus) consumption (s19), alcohol consumption (s12, s13, s27, s39, s81), caffeine consumption (s32), physical activity (s11), work-related physical activity (s34), and consumption of marine n-3 fatty acids (s22, s33). In addition, a number of anthropometric measures have been examined including birth weight and preterm birth (s13), adult height (s72), body mass index (s28, s31, s73, s82), body fat, body surface area and weight gain (s16), body fat distribution and lean body mass (s23). The examined potential environmental risk factors for AF include season of year (s83–s86), calendar year (s42), job strain (s15), and neighborhood deprivation (s87). Genetic risk factors for AF have also been examined, family history of AF (s88-s90), AF in twins (s91, s92), AT1 mutation (s35), and genetic polymorphisms (e.g. ceruloplasmin (s7), and angiotensinogen and ACE gene polymorphisms (s38). The examined electrophysiological risk factors for AF included QTc interval duration (s67), PR interval duration (s68), and supraventricular ectopic activity (s43). Biomarker studies have explored the role of marine n-3 fatty acids in adipose tissue (s26), forced expiratory volume (s9, s41), carotid intima-media thickness (s1), red blood cell distribution (s2), inflammatory biomarkers (s18, s39), soluble urokinase plasminogen activator receptor (s3), atrial natriuretic peptide (s14), YKL-40 levels (s36), and plasma insulin (s8).
Other studies have examined the risk of AF by exposures such as glucocorticoid use (s76), use of bisphosphonates (s78, s79, s93, s94), statins (s74, s95), antihypertensive treatment (s96), hormone replacement therapy (s97), and nonsteroidal anti-inflammatory drug use (s75), and ablation for the Wolf–Parkinson–White syndrome (s70). Finally, studies have examined the potential role of inflammatory bowel disease (s98), psoriasis (s99), rheumatoid arthritis (s100), ortostatic hypotension (s10), and other morbidities including coeliac disease (s100), colorectal cancer (s102), and thyroid disease (s69, s103).
Exposures in AF prognosis
Exposures included having AF (s17, s21, s40, s44, s46, s65, s66, s80, s104-s110), type of AF (s50, s52), CHADS2 score (s29, s110-s112), CHA2DS2-VASc score (s29, s111-s114), bleeding risk scores (s115), age (s116), gender (s24, s40, s117), chronic kidney disease (s118), renal failure (s119), vascular disease (s120), year of AF diagnosis (s121-s126), stroke (s127, s128), type of stroke (s129), retinal vein and artery occlusions (s130), cardiovascular hospitalization (s48), and DC cardioversion of AF (s51).
Outcome measures
Outcome measures included, stroke (s21, s25, s40, s43, s44, s47, s50, s83, s85, s99, s100, s111, s113, s114, s116–s119, s123, s125, s130–s144), systemic thromboembolism (s24, s105, s109, s133, s134, s136, s141, s145–s149), mortality (s24, s40, s47–s49, s51, s52, s55–s58, s60, s65, s66, s70, s80, s83, s85, s104, s105, s110, s113, s119, s124, s126, s133, s135–s137, s140, s143, s150–s156), lost life years (s127), coronary events (s132, s133, s147, s148, s157), pulmonary embolism (s133), hospitalization (s17, s107, s133), length of hospital stay (s137), performance of stroke and bleeding risk scores (s29, s111, s114, s115), CHA2DS2-VASc score (s54), dementia (s21), liver toxicity (s153), congestive heart failure (s140), and cancer (s106).
AF care and management
Exposures included ethnicity (s158), acetylsalicylic acid (s47, s141, s147), single, dual, or triple therapy with warfarin, aspirin, and clopidogrel (s135), use of oral anticoagulation (s44, s47, s52, s77, s131, s135, s142–s146, s150, s152, s159, s160), dabigatran vs. warfarin (s133, s134, s157), interruption of warfarin treatment (s161), and digoxin use (s156). Outcomes included quality of in-hospital care (s137), inpatient cost (s128), no treatment with antiplatelet therapy and oral anticoagulation (s132, s147, s148, s162, s163), initiation and persistence with warfarin (s158, s164), variation in use of oral anticoagulation (s136, s165), quality of warfarin treatment (s61, s62), 3-month drug persistence probability (s131), type of oral anticoagulation (s166), use of oral anticoagulation (s53, s54, s62, s63, s122, s167, s168), dynamics of use of vitamin K antagonist and new oral anticoagulant (s71), bleed (s47, s114, s118, s119, s132–s135, s141, s146–s148, s160, s162), type of antiarrhythmic drug (s151), use of dronedarone (s153), and digoxin treatment (s49).
Bibliometrics
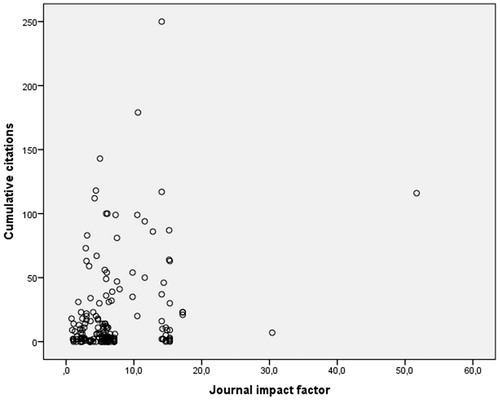
The mean (range) number of authors was 6 (1–16). shows a plot of cumulated citations as a function of journal impact factor. Mean (range) journal impact factor in publication year was 6.9 (0.8–51.7). The median impact factor (25–75% percentiles) was 5.7 (2.4–7.2). The total cumulated number of citations for all 173 publications was 3721. The mean (range) cumulated number of citations per publication was 22.4 (0–250). The median (25%–75% percentiles) cumulated number of citations was 6.0 (1.0–23.0). Nine publications had ≥100 cumulated citations (s31, s33, s42, s111, s114, s118, s141, s161).
Figure 3. Plot of cumulative citations as a function of journal impact factor.
Discussion
We found that the number of published registry-based studies on AF from Sweden and Denmark increased substantially during the 15-year period from 2000 to 2014. There was a great diversity of study aims, exposures and outcomes based on different populations and registry data. Studies were published in recognized medical journals, and were well cited.
Strengths and weaknesses of the current study
This is the first review of studies on AF epidemiology based on data from administrative population and health care registries published from Sweden and Denmark. We used a systematic literature search strategy to identify relevant publications, and focused on study aims, exposure, outcomes, and bibliometric analyses. It is possible that we have not identified all eligible publications. However, the possibility of some unidentified studies will likely not change main findings or conclusions in the current review. We did not examine each publication for risk of error imposed by the use of registries as data sources. Such analyses for potential bias would best be performed in studies focusing on specific research questions such as identification of risk factors or outcomes from AF.
Perspectives
Observational studies based on registries are typically characterized by a number of methodological advantages. Firstly, using mandatory population-based registries lower risk of selection bias and information bias, in particular, recall and nonresponse bias since the data are registered prospectively. Secondly, these registries in Sweden and Denmark capture the entire population reflecting the patient spectrum seen in routine clinical practice as opposed to the voluntary population-based cohorts in which participation may often have risk of selection bias due to nonresponders.[Citation6] Also, the registries ensure large sample sizes. Finally, the data already exist and studies based on registry data can therefore be done at relatively low costs compared to primary data collection. However, there are also important limitations when using administrative registries for research, and these should be kept in mind whenever planning, conducting or interpreting register-based studies. Important concerns are the completeness and validity of the recorded data, which has often not been formally assessed. The complex and changing natural history of AF constitute a particular challenge in this context leading to concerns about trends over time in data completeness and validity. Validation of registry information can be challenging for several reasons. It is costly and is usually done in retrospect by consulting “gold standard” source documents such as the medical record including electrocardiographic documentation, imaging documentation, etc. These source documents were not created for retrospective validation purposes. Also, when studying AF, there are inherent problems related to the evaluation of the true incidence and prevalence of AF, because AF can be asymptomatic (and therefore undiagnosed) [Citation7] and consequently not reported to any registries. However, the few studies which have examined the validity of recordings of AF in Swedish and Danish health care registries have reported the positive predictive value to be high (s6, s30).
The publications identified in this review represent a substantial contribution to this research area and have provided new important insights into the etiology and clinical aspects of AF. The contribution is an example of the two countries “punching above their weight” (e.g. the combined total population in Sweden and Denmark is only 15.2 million corresponding to approximately 0.2% of the world population). The ability to produce such a high volume of timely and relevant research on AF has only been possible due to the availability of high quality administrative and health care registries, which have been accessible for researchers. The future use of these valuable data sources for research has been threatened by proposals of international legalization based on a more restrictive approach, such as requirement of informed consent of the registered, advocated by a number of stakeholders including the World Medical Association in the recent draft declaration on ethical considerations regarding health databases and biobanks. However, the recently adopted EU General Data Protection Regulation “on the protection of individuals with regard to the processing of personal data and on the free movement of such data” has secured the possibility for the continuation of such use of registries in medical research in Sweden, Denmark, and other Nordic countries.[Citation8]
Conclusion
Administrative and health care registries in Sweden and Denmark have provided basis for a substantial research effort within the last 15 years covering all key aspects of AF epidemiology resulting in a high and continuously increasing number of publications, which has been well-received by the scientific community.
Supplement_Frost_R3.docx
Download MS Word (42.6 KB)Disclosure statement
The authors report no declarations of interest. The authors alone are responsible for the content and writing of the paper.
References
- Jacobs V, Cutler MJ, Day JD, et al. Atrial fibrillation and dementia. Trends Cardiovasc Med. 2015;25:44–51.
- Wolf PA, Dawber TR, Thomas HE Jr., et al. Epidemiologic assessment of chronic atrial fibrillation and risk of stroke: the Framingham study. Neurology. 1978;28:973–977.
- Andersen LV, Vestergaard P, Deichgraeber P, et al. Warfarin for the prevention of systemic embolism in patients with non-valvular atrial fibrillation: a meta-analysis. Heart. 2008;94:1607–1613.
- Santhanakrishnan R, Wang N, Larson MG, et al. Atrial fibrillation begets heart failure and vice versa: temporal associations and differences in preserved versus reduced ejection fraction. Circulation. 2016;133:484–492.
- Benjamin EJ, Wolf PA, D'Agostino RB, et al. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998;98:946–952.
- Olsen J. Register-based research: some methodological considerations. Scand J Public Health. 2011;39:225–229.
- Kennedy HL. Silent atrial fibrillation: definition, clarification, and unanswered issues. Ann Noninvasive Electrocardiol. 2015;20:518–525.
- Available at: http://ec.europa.eu/justice/data-protection/reform/index_en.htm. 2016.