
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Objectives. To compare the ability of the E/a′ ratio and the recommended diastolic parameters in the American Society of Echocardiography (ASE) and the European Association of Cardiovascular Imaging (EACVI), in predicting a dominant diastolic pulmonary vein flow in patients with normal ejection fraction. Design. We retrospectively evaluated the diastolic function according to the ASE/EACVI guidelines, the S/D ratio and the septal, lateral and average E/a′ ratio in 293 unselected in-hospital patients, aged 39–86 years, in sinus rhythm and with no or mild valve disease, having a normal systolic function (EF > 50%). Results. The S/D ratio had a positive association to septal, lateral and average E/a ratio (R2 = 0.25, 0.35 and 0.32). The association to average E/e′ ratio, LA vol index and TR velocity was weak (R2 = 0.037, 0.033 and 0.087) and for e′ velocity negatively. In patients with S/D ratio <1, septal, lateral, average E/a′ ratio, average E/e ratio, LA vol index (p<.001) and TR velocity (p<.05) were significantly higher compared to patients with S/D ratio ≥1. No significant difference was seen in e′ velocity. The septal, lateral and average E/a′ ratio were significantly higher in patients with S/D ratio <1 regardless a normal or impaired diastolic function according to the ASE/EACVI guidelines (p<.001). The ASE/EACVI algorithm detected 21 patients with S/D ratio <1 compared to 28 patients using average E/a′ ratio with cut-off >14. Conclusion: E/a′ ratio might be a useful new diastolic parameter in patients with a normal ejection fraction as it is more closely related to the S/D ratio than the established ASE/EACVI diastolic parameters.
Introduction
Previous studies have shown that in patients with a preserved systolic function, the presence of a dominant diastolic component in the pulmonary venous flow and a decreased left atrial contractile function can identify patients with an impaired clinical short and long-term outcome [Citation1–5]. The easily eligible a′ velocity in the tissue Doppler reflects the left atrial contraction and a reduced a′ velocity has been shown to correlate to a diastolic dysfunction and to S/D ratio <1 [Citation6–9]. The ASE/EACVI guidelines from 2016 do not include the a′ velocity in their criteria and the S/D ratio has only a minor supplementary role in the evaluation of LV diastolic function in patients with a normal ejection fraction [Citation10,Citation11]. A recently published study found a very good correlation between a new parameter, the E/a′ ratio and the ASE/EACVI guidelines in detecting a diastolic dysfunction and an increased left ventricle filling pressure in patients with a decreased ejection fraction [Citation8]. The same study also showed an exponential correlation between the E/a′ ratio and the S/D ratio in this patient category. This study tested if this new parameter, the E/a′ ratio where the E reflects the early diastolic pressure gradient across the mitral valve and the a′ velocity reflects the left atrial contractile response to the late diastolic filling pressure could have additional information beyond the diastolic parameters in the current ASE/EACVI guidelines in patients with a normal ejection fraction.
Aim of the study: To compare the ability of the E/a′ ratio and the ASE/EACVI diastolic parameters in predicting a dominant diastolic pulmonary vein flow (S/D ratio <1) in patients with normal ejection fraction.
Methods and material
Study population
This retrospective study included acute (90%) and elective patients (10%), totally 441 patients, who during the time period April 2011 to January 2016 underwent a clinically indicated complete echocardiographic examination in the department of physiology at Sundsvall Hospital, performed by one cardiologist (BJ), using the same echocardiographic system, where the major issue at hospitalisation was left ventricular systolic or diastolic heart failure. The systolic ejection fraction could be evaluated in all patients but in order to evaluate the different diastolic parameters, the patient had to be in sinus rhythm and suffer from no more than a mild valve disease. Consequently, the exclusion criteria were: atrial fibrillation, atrial flutter and moderate or severe valve disease. A total of 113 patients had a decreased systolic function (EF ≤50%), twenty-three patients had atrial fibrillation, twelve patients had a significant valve disease and in thirty-two patients the pulmonary vein flow was not obtainable or of poor quality and all these patients were excluded from the study. The remaining 293 patients (147 men; mean age 64.8 ± 12.4 years) had a normal systolic function (EF >50%), sinus rhythm and no or only mild valve disease and constituted the study group. The study protocol was approved by the ethics committee of Umeå University (Dnr 2016-209-31) and a written informed consent was obtained from all patients.
Echocardiographic analysis
The ultrasound system used for the echocardiographic examinations of the study group was a commercially available Philips iE33 ultrasound system, Philips Electronics, Netherlands using an S5-1 with 1–5 MHz transducer. All measurements were performed using the incorporated calculation program in the ultrasound machine. The tissue velocity of the myocardium, the e′ velocity and the a′ velocity was measured (cm/s) just below the AV-plane in the 4-chamber view of the left ventricle in both the septal and lateral wall and the average e′ = (septal e′ lateral e′)/2 and the average a′ = (septal a′+ lateral a′)/2 were calculated. The derivatives, average E/e′ ratio and the septal, lateral and average E/a′ ratio were calculated. The maximal velocity of the pulmonary vein inflow into the left atrium during systole (S) and diastole (D) was recorded (cm/s) and the S/D ratio was calculated. The maximum tricuspid (TR) velocity in the regurgitation jet between the right ventricle and the right atrium was measured (m/s). The left atrial volume was estimated from the 4 chamber and 2 chamber view using the area-length method with correction for the body surface area [Citation12]
Evaluation of the left ventricular function
The ejection fraction (EF) was used as a measure of the left ventricular systolic function. A normal systolic function was defined as EF >50% [Citation13]. The diastolic left ventricular function was defined in accordance to the current ASE/EACVI guideline algorithms from 2016 using four criteria [Citation10,Citation11]. Septal e′ velocity <7 cm/s or lateral e′ velocity <10 cm/s, average E/e′ ratio >14, LA vol index >34 ml/m2 and TR velocity > 2.8 m/s were considered pathological. A diastolic dysfunction was considered present if a majority of the criteria in the ASE/EACVI guidelines were fulfilled. The S/D ratio, septal, lateral and average a′ velocity were measured and septal, lateral and average E/a′ ratio were calculated. S/D ratio <1 was considered decreased.
Reproducibility
High intra-observer and inter-observer correlation coefficients of 0.944–0.982 respective 0.927–0.983 between measurements for septal, lateral a′ velocity and the S/D ratio at two different occasions have been validated in an earlier study by our group [Citation8].
Statistics
Baseline characteristics were described using relative and absolute frequencies for categorical variables and means and standard deviations for continuous variables. Between groups differences in mean were tested using an independent samples t-test. To describe the association between measures of heart function we used a non-parametric running line smoother with default bandwidth [Citation14]. We used a non-parametric technique since it generates a curve from data without any assumptions regarding function class or shape. To measure the amount of variation explained by the estimated curve we used the R2-statistic recommended: where
is the estimate from the running line smoother [Citation15]. All statistical analyses were made in Stata MP/4 15.1, using two sided tests and significance level 0.05.
Results
A systolic or diastolic heart failure had to be confirmed or excluded during hospitalization in all patients in this study.
All patients without stratifications
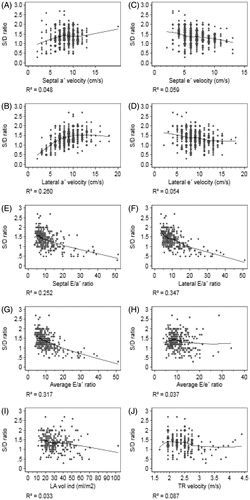
shows that in all patients with a normal ejection fraction, there was a positive association between S/D ratio and the E/a′ ratio both septal, lateral and average (R2 = 0.25, 0.35 and 0.32) while the correlation to the average E/e′ ratio, LA vol index and TR velocity was weak (R2 = 0.037, 0.033 and 0.087). The correlation to the e′ velocity was negative, both septal and lateral.
Figure 1. (A–J) The correlation between the S/D ratio and different tissue-Doppler parameters, their derivatives and the ASE/EACVI diastolic parameters.
Patients stratified for S/D ratio ≥1 or <1
The patient characteristics and the assessment of the left ventricular systolic and diastolic function of the 293 patients stratified for S/D ratio ≥1 or <1 are presented in . The results of the E/a′ ratio, the a′ velocity and the diastolic parameters in the ASE/EACVI guidelines in the two S/D groups are seen in . The results of the E/a′ ratio and the a′ velocity in patients divided into normal and impaired diastolic function according to the ASE/EACVI guidelines are presented in .
Table 1. Characteristics and assessment of the left ventricular systolic and diastolic function in the study population stratified for S/D ratio ≥1 or <1.
Table 2. Different tissue-Doppler and their derivatives correlation to S/D ratio ≥1 or <1 compared to the criteria in the ASE/EACVI guidelines in all patients.
Table 3. Different tissue-Doppler and their derivatives correlation to S/D ratio ≥1 or <1 in patients with a normal diastolic function or a diastolic dysfunction according to the ASE/EACVI guidelines.
As seen in , there was a highly significantly lower a′ velocity and increased E/a′ ratio both septal, lateral and average in patients with S/D ratio <1 compared to S/D ratio ≥1 (p<.001). The average E/e′ ratio and the LA vol index were also highly significantly increased in patients with S/D ratio <1 (p<.001). The TR velocity was significantly higher (p<.05) but no significant difference was seen in the e′ velocity. No significant difference was seen in the ejection fraction between the two groups. shows that there was a highly significantly lower a′ velocity and increased E/a′ ratio both septal, lateral and average in patients with S/D ratio <1, both in patients with a normal and impaired diastolic function according the ASE/EACVI guidelines.
Comparison between the E/a′ ratio and the ASE/EACVI guidelines in detecting S/D ratio <1
S/D ratio <1 was seen in 43 patients. A diastolic dysfunction according to the ASE/EACVI guidelines detected 22 of these patients while the remaining 21 patients had a normal diastolic function. An average E/a′ ratio with cut-off >14 detected 28 out of the 43 patients with S/D ratio <1. A lateral E/a′ ratio with cut-off ≥20 applied on all patients with a normal ejection fraction had a sensitivity, specificity, PPV and NPV of 48.8, 98.8, 87.5 and 91.8% to detect S/D ratio <1.
Discussion
The diagnosis of an isolated diastolic heart failure in patients with a preserved systolic function still seems to be an enigma as two large invasive studies presented the last year, where the purpose was to validate the ASE/EACVI guidelines criteria of a diastolic dysfunction with an elevated invasive LV filling pressure, only showed a modest correlation and the invasive correlation to the individual criteria in the guidelines was only marginal [Citation16,Citation17]. The authors in the Euro filling study concluded that there was a particular need for improving the diagnostic accuracy of echocardiography in this patient group [Citation16].
Studies have shown that the presence of a dominant diastolic component in the pulmonary venous flow and a decreased left atrial contractile function can identify patients with an impaired clinical short and long-term outcome [Citation1–5]. The easily eligible a′ velocity in the tissue Doppler reflects the left atrial contraction and a reduced a′ velocity has been shown to correlate to a diastolic dysfunction and to S/D ratio <1 [Citation6–9]. The current ASE/EACVI guidelines do not include any direct parameter reflecting the left atrial function and the S/D ratio has only a complementary role and the correlation if any exists between these two parameters has never been clarified in detail. The a′ velocity in the tissue Doppler is a simple, robust and easily obtainable parameter of the left atrial contraction [Citation6,Citation7]. Normally the a′ velocity increases with age in patients without heart failure [Citation18]. A reduced a′ velocity on the other hand has been shown to correlate with severe diastolic dysfunction and S/D ratio <1 both in patients with normal and a decreased ejection fraction. [Citation6–9]. Furthermore, a new parameter, the E/a′ ratio with a cut-off of 10 correlated very well with the current ASE/EACVI guidelines in detecting/ruling out a diastolic LV dysfunction and an increased LV filling pressure in patients with a reduced ejection fraction [Citation8]. In the same study the correlation between the E/a′ ratio and the S/D ratio was exponential.
The present study shows a strong association between S/D ratio and the E/a′ ratio both septal, lateral and average while the association between the S/D ratio and the LA vol index, TR velocity and the average E/e′ ratio in the guidelines is weak. Interestingly, the association with the e′ velocity, both septal and lateral is negative while the association between the S/D ratio and the a′ velocity is positive. These results could indicate two things. In patients with a normal ejection fraction, the S/D ratio is more closely related to the a′ velocity than to the e′ velocity and furthermore the E/a′ ratio has a better correlation to the S/D ratio than the individual criteria in the current ASE/EACVI guidelines. Interestingly, the entire ASE/EACVI algorithm was not an optimal tool to detect S/D ratio <1 as half of the patients with S/D ratio <1 had a normal diastolic function according to the guidelines and only 1/3 of the patients with a diastolic dysfunction had S/D ratio <1. Our study showed a highly significantly lowered a′ velocity and increased E/a′ ratio in patients with S/D ratio <1, both in patients with a normal and abnormal diastolic function according to the ASE/EACVI guidelines. How can this be interpreted? Is S/D ratio <1 really an indicator of an increased diastolic filling pressure in this patient category?
In this study there is a strong correlation between the S/D ratio and both the E/a′ ratio and the a′ velocity both in general and especially in patients with S/D ratio <1 regardless the diastolic classification according to the ASE/EACVI guidelines. This may suggest that a left atrial failure seen as a decreased a′ velocity could be a major hemodynamic explanation for the occurrence of S/D ratio <1 and that this finding is amplified by the E/a′ ratio. Hatle and other authors have shown that the main underlying factor for a decreased systolic vein flow component is the LV filling pressure and an increased mean LA pressure [Citation19–22]. This could support that S/D ratio <1 in our study really reflects an increased LV filling pressure in absence of invasive data
Limitation of the study
There are several major limitations in the study. Firstly, invasive filling pressure was not measured in our patients. Secondly, we did not evaluate the occurrence of a clinical heart failure or correlated the results to the BNP or pro-BNP values in the patients. Furthermore, we did not correlate our results to the final diagnosis and the pharmacological treatment at discharge was not eligible. Finally, this is a retrospective study with its known limitations
Disclosure statement
There is no conflict of interest related to the present study.
References
- Ren X, Na B, Ristow B, et al. Usefulness of diastolic dominant pulmonary vein flow to predict hospitalization for heart failure and mortality in ambulatory patients with coronary heart disease (from the Heart and Soul Study). Am J Cardiol. 2009;103:482–485.
- Buffle E, Kramarz J, Elazar E, et al. Added value of pulmonary venous flow Doppler assessment in patients with preserved ejection fraction and its contribution to the diastolic grading paradigm. Eur Heart J Cardiovasc Imaging. 2015;16:1191–1197.
- Kaminski M, Steel K, Jerosch-Herold M, et al. Strong cardiovascular prognostic implication of quantitative left atrial contractile function assessed by cardiac magnetic resonance imaging in patients with chronic hypertension. J Cardiovasc Magn Reson. 2011;13:42.
- Hedberg P, Selmeryd j, Leppert J, et al. Long-term prognostic impact of left atrial volumes and emptying fraction in a community-based cohort. Heart. 2016;0:1–7.
- Santos ABS, Kraigher-Krainer E, Gupta DK, for the PARAMOUNT Investigators, et al. Impaired left atrial function in heart failure with preserved ejection fraction. Eur J Heart Fail. 2014;16:1096–1103.
- Hesse B, Schuele SU, Thamilasaran M, et al. A rapid method to quantify left atrial contractile function: Doppler tissue imaging of the mitral annulus during atrial systole. Eur J Echocardiogr. 2004;5:86–92.
- Khankirawatana B, Khankirawatana S, Peterson B, et al. Peak atrial systolic mitral annular velocity by Doppler tissue reliably predicts left atrial systolic function. Am Soc Echocardiogr. 2004;17:353–360.
- Johansson B, Lundin F, Tegerback R, et al. E/a′ ratio a simple detector of left ventricular dysfunction in patients with decreased ejection fraction. Scand Cardiovasc Journal. 2018;52:20–27.
- Johansson B, Lundin F. Tegeback R, et al. The a′velocity in the tissue Doppler predicts S/D ratio <1 in patients with a normal ejection fraction. Scand Cardiovasc Journal. 2018;52:183–188.
- Nagueh SF, Smiseth OA, Appleton CP, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. An update from the American society of echocardiography and the European association of cardiovascular imaging. J Am Soc Echocardiogr.2016;29:277–314.
- Nagueh SF, Smiseth OA, Appleton CP, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. An update from the American society of echocardiography and the European association of cardiovascular imaging. Eur Heart J Cardiovasc Imaging. 2016;17:1321–1360.
- Lang RM, Bierig M, Devereux RB, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography's Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005;18:1440–1463.
- Paulus WJ, Tschöpe C, Sanderson JE, et al. How to diagnose diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society of Cardiology. Eur Heart J. 2007;28:2539–2550.
- Royston P, Sauerbrei W. Multivariable model-building: a pragmatic approach to regression analysis based on fractional polynomials for modelling continuous variables. New York: John Wiley & Sons Ltd; 2008.
- Kvålseth TO. Cautionary note about R2. Am Stat. 1985;39:279–285.
- Lancellotti P, Galderisi M, Edvardsen T, et al. Echo-Doppler estimation of left ventricular filling pressure: results of the multicentre EACVI Euro-Filling study. Eur Heart J Cardiovasc Imaging. 2017;18:961–968.
- Andersen OS, Smiseth OA, Dokainish H, et al. Estimating left ventricular filling pressure by echocardiography. J Am Coll Cardiol. 2017;69:1937–1948.
- Thomas L, Levett K, Boyd A, et al. Changes in regional left atrial function with aging: evaluation by Doppler tissue imaging. Eur J Echocardiography. 2003;4:92–100.
- Rossvoll O, Hatle LK. Pulmonary venous flow velocities by transthoracic doppler ultrasound: Relation to left ventricular diastolic pressures. J Am Coll Cardiol. 1993;21:1687–1696.
- Kuecherer HF, Kusumot F, Muhiudeen JA, et al. Pulmonary venous flow patterns by transesophageal pulsed Doppler echocardiography: relation to parameters of left ventricular systolic and diastolic function. Am Heart J. 1991;122:1683–1693.
- Basnight MA, Gonzalez MS, Kershenovich SC, et al. Pulmonary venous flow velocity: relation to hemodynamics, mitral flow velocity and left atrial volume, and ejection fraction. J Am Soc Echocardiogr. 1991;4:547–558.
- Kuecherer HF, Muhiudeen IA, Kusumoto FM, et al. Estimation of mean left atrial pressure from transesophageal pulsed doppler echocardiography of pulmonary venous flow. Circulation. 1990;82:1127–1139.