
Abstract
Objectives. Reduced muscular strength (measured by grip strength) has been associated with an increased risk of cardiovascular complications. Further research is needed to identify how muscular strength is associated with various markers of cardiovascular function to provide at least some mechanistic explanation for observed interrelations. We, therefore, addressed the question of whether handgrip (HG) strength is associated with descriptors of peripheral and central hemodynamics in the population of healthy individuals. Design. Two hundred thirty-one healthy volunteers (90 men and 141 women, mean age 54 years) were studied. Patients were asked to perform the maximum handgrip trial in the standing position with the dominant arm, using hydraulic hand dynamometer. Applanation tonometry was used to execute the non-invasive assessment of the pressure waveform. Results. HG strength was associated with various markers of hemodynamics and clinical characteristics, e.g. correlated significantly and positively with BMI [body mass index, r = 0.21, p = .001], PPA [pulse pressure amplification, r = 0.43, p < .0001], Tr [time to return of pressure wave, r = 0.43, p < .0001] and significantly and negatively with AP [augmentation pressure, r = −0.45, p < .0001]. Multiple linear regression showed that sex, handgrip and mean blood pressure were independently associated with AP (R2 = 0.38), PPA (R2 = 0.21) and Tr (R2 = 0.29). Conclusions. Our study demonstrated the association between handgrip strength and central hemodynamic metrics. These interactions may add a mechanistic explanation for the role of muscle strength as a risk marker for incident cardiovascular complications.
Introduction
Reduced muscular strength (measured by grip strength) has been associated with an increased risk of cardiovascular complications [Citation1–3]. Measurement of the handgrip (HG) is a straightforward, inexpensive risk-stratifying method not only for various cardiovascular complications but also for prediction of nutritional status in hospitalized patients or estimation of cognitive performance [Citation4,Citation5]. Skeletal muscle function is an essential component of physical fitness, which in turn correlates with lower cardiovascular disease mortality across the lifespan. Further research is needed to identify how muscular strength is associated with cardiovascular outcomes and various markers of general health to provide at least some mechanistic explanation for observed interrelations.
Cohem et al. [Citation6] showed that muscle strength is associated with lower diastolic blood pressure in school children, while Blanchard et al. [Citation7] demonstrated (contrary to initial hypothesis) that adults with high BP displayed greater muscle strength than subjects with normal blood pressure. We, therefore, addressed the question of whether handgrip strength is associated with descriptors of peripheral and central hemodynamics in the population of healthy individuals.
Material and methods
Two hundred thirty-one healthy volunteers (90 men and 141 women, mean age 54 years) were studied. The subjects were recruited through a local advertisement. Study subjects did not suffer from chronic conditions and did not require protracted treatments with pharmacological therapy. The University Ethics Committee approved the study protocol.
Anthropometric measurements (height, weight) were all made according to standard guidelines. Brachial blood pressure measurement was performed by an oscillometric method (705IT, Omron Healthcare Co, Ltd, Kyoto, Japan) in the supine position after 10-min rest. Bio-impedance analysis was performed with a single frequency (50 kHz) device (Bodystat 1500, Bodystat Ltd, UK) to measure the fat content as a proportion of total body mass.
Patients were asked to perform the maximum handgrip trial in the standing position with the dominant arm, using Jamar Hydraulic Hand Dynamometers (Sammons Preston Rolyan, Bolingbrook, Illinois, USA). A mean of three maximal isometric contractions was calculated for each patient. Verbal encouragement was used to obtain maximal effort, and 10 s interval was applied between measurements. To decrease variability between subjects, a dominant arm was used for handgrip assessment.
Non-invasive assessment of the pressure waveform
With the use of a piezoelectric tonometer (Colin BPM 7000, Japan) the radial pressure waveform was recorded non-invasively. The recorded analog signal was sent in real time to SphygmoCor Mx (AtCor Medical, Australia) for on-line reconstruction (with the use of a validated transfer function) of a pressure waveform characteristic for an ascending aorta. To assess the peripheral and central hemodynamics Pulse Wave Analysis was applied. Indices of central pressure were obtained with the use of commercial software. The central pulse pressure consists of 2 components – pressure at first systolic shoulder (P1) in the arterial pulse waveform and augmentation pressure (AP) – the height of central systolic pressure above the P1. The pulse pressure amplification (PPA) ratio was defined as the peripheral pulse pressure/central pulse pressure [Citation8].
Statistical analysis
All analyses were performed with SPSS (version 23.0, IBM Corp, USA). Continuous data are reported as mean ± SD. Baseline characteristics are reported as standard descriptive statistics. The differences between mean were estimated with the use of unpaired t-test. Univariate and multivariate regression analysis, as well as Pearson correlation analysis, were used to confirm associations between augmentation pressure, pulse pressure amplification or time to return of pressure wave and covariates. A general linear model (GLM) was used to examine the interaction between sex and tested covariates and results are represented as the adjusted mean and standard error. The partial regression coefficient to adjust for body weight or body fat was also calculated. All tests were two-tailed, and p < .05 was taken as statistically significant.
Results
Clinical and hemodynamic characteristics of all studied participants followed by details and comparison of the same parameters between men and women are presented in and . In general, the average age of all participants was 54.1 years, and their BMI was just above the upper range for the normal values showing some overweight, peripheral systolic and diastolic blood pressures were within normal limits as well as resting heart rate.
Table 1. Clinical characteristics of study subjects.
Table 2. Hemodynamics of the study group.
Table 3. Regression coefficients of multiple linear regression with changes in AP, PPA or Tr as dependent variables, and sex, handgrip, BMI, and mean blood pressure as independent variables.
There were 141 women and 90 men. Comparing with men, women were significantly leaner, smaller and demonstrated weaker handgrip. Their peripheral diastolic, central diastolic and mean blood pressures were lower, but their peripheral and central pulse pressure, as well as augmentation pressure, were higher. Pulse pressure amplification was lower in women and time to return of pulse wave was shorter in comparison with men.
The association of handgrip with clinical characteristics and hemodynamics
As shown in handgrip strength correlated significantly and positively with BMI (r = 0.2, p = .001), pulse pressure amplification (r = 0.43, p < .0001), time to return of pressure wave (r = 0.43, p < .0001) and significantly and negatively with augmentation pressure (r = −0.45). This association remained significant after controlling for weight or body fat weight, as demonstrated by partial correlations between measures of handgrip and indices of AP, PPA and Tr [(r = −0.46, p < .0001; r = 0.38, p < .001; r = 0.38, p < .0001) and (r = −0.44, p < .0001; r = 0.41, p < .0001, r = 0.42, p < .0001), respectively)].
Further investigation demonstrated that HG strength correlated with peripheral and central diastolic pressure (r = 0.25, p < .0001; r = 0.24, p < .0001, respectively) and mean BP (r = 0.14, p = .04) but not with systolic blood pressure. Moreover, HG strength was associated significantly and negatively with peripheral and central pulse pressure (r = −0.16, p = .01; r = −0.27, p < .0001, respectively).
Interaction between handgrip, augmentation pressure, pulse pressure amplification, time to return of pressure wave and clinical variables
Multiple linear regression showed that sex, handgrip and mean blood pressure were independently associated with AP (R2 = 0.38). In a model where PPA was evaluated as the dependent variable only handgrip and mean BP was significantly associated with pulse pressure amplification (R2 = 0.21). Sex, mean BP and handgrip were independently associated with time to return in pressure wave (R2 = 0.29) although handgrip strength association was of borderline significance in this last case ().
BMI was significantly correlated with body fat weight (r = 0.86, p < .0001), therefore replacing BMI by fat weight did not improve R2 in multiple regression (data not shown).
Interaction between sex, augmentation pressure and time to return of pressure wave
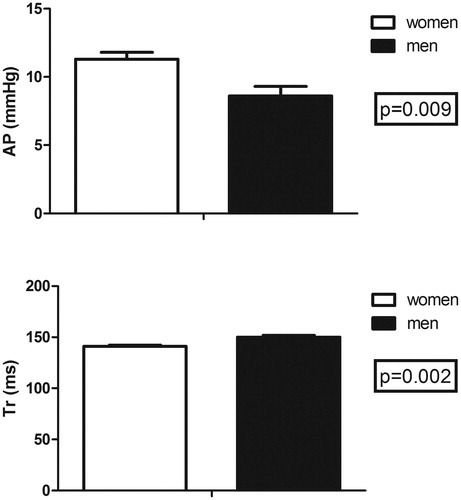
Female sex was associated with higher AP and shorter time of the return of pressure wave. Moreover, sex influence independently these descriptors in the multiple regression model. The direct comparison of the AP between women and men after adjustment for handgrip strength and BPmean demonstrated that AP remained significantly higher in females (11.3 ± 0.5 mmHg vs 8.7 ± 0.7 mmHg, p = .009), . Time to return of the pressure wave persists shorter in women after adjustment for HG and BP mean (141.2 ± 1.3 ms vs 149.7 ± 1.9, p = .002), .
Figure 1. The interaction between mean handgrip strength (HGmean) body mass index (BMI), augmentation pressure (AP), time to return of pressure wave (Tr) and pulse pressure amplification (PPA).
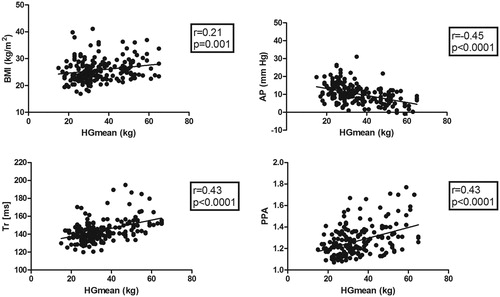
Figure 2. Augmentation pressure (AP) and time to return of pressure wave (Tr) adjusted for handgrip strength and mean blood pressure in both sexes. Data represent adjusted mean ± SE.
Discussion
This study, performed on healthy subjects, showed that muscle strength estimated by handgrip is associated with descriptors of central hemodynamics.
Handgrip strength is associated with cardiovascular complications even after adjustment for common confounding risk factors. However, it is currently unknown what mechanisms are responsible for the correlation between the loss of muscular strength and cardiovascular sequela. Some mechanistic insight into these problems was provided recently by observational studies. Beyer et al. [Citation9] determined the association between HG strength and changes in heart structure and function. In a sample of 4654 participants of the UK Biobank Study (mean age 55 years), left ventricular (LV) ejection fraction (EF), end-diastolic volume (EDV), end-systolic volume (ESV), stroke volume (SV), mass (M), and mass-to-volume ratio (MVR), as well as a handgrip, were measured [Citation9]. After adjustment, a higher level of handgrip strength at baseline was associated with higher EDV, higher SV, lower left ventricular mass, and lower left ventricular mass-to-volume ratio (LVMVR). It was shown that the association between handgrip strength and EDV and SV was strongest among younger individuals, while the association with left ventricular mass and LVMVR was strongest among older individuals. The authors concluded that a stronger handgrip was associated with cardiac structure and function in a pattern indicative of less cardiac hypertrophy and remodeling. These patterns are, in turn, associated with a lower risk of cardiovascular complications. It is well known that muscle tissue is vascularized by an extensive vascular network. Therefore Taekema et al. [Citation10] estimated the association between blood pressure (BP) and muscle function in a population of 670 middle-age subjects (mean 63.2 years) and 550 very old patients (all 85 years). It was observed that in middle-age subjects BP and handgrip strength were not associated, while in the in “oldest old” subjects, higher systolic BP (SBP), mean arterial pressure (MAP), and pulse pressure (PP) were associated with higher handgrip strength after adjusting for comorbidity and medication use. In contrast, we observed in our much younger population of healthy subjects that HG strength correlates significantly and positively with diastolic and mean BP, while negatively with both peripheral and central pulse pressure. Pulse pressure is a rough estimated of arterial stiffness, so it is tempting to speculate that HG strength may also correspond with this arterial metric. This view is corroborated by our current observation that the longer Tr correlated positively with stronger handgrip. It was demonstrated by
Hickson et al. [Citation11] that central to peripheral arterial stiffness gradient influence the timing and amplitude of wave reflections. It is also noteworthy that the time to return of reflected pressure wave was implicated in the severity of coronary artery disease.
De-Lima Junior et al. [Citation12] evaluated the association between handgrip strength and vascular function in patients with hypertension. In 72 hypertensive subjects (mean age 56 years) ambulatory arterial stiffness index (AASI), carotid-femoral pulse wave velocity (cfPWV) and reflected wave indicator (central augmentation index – AIx) were estimated. The analysis revealed a negative association between handgrip strength and AASI, as well as AIx and lack of association with cfPWV. These interactions remained significant after adjustments for age, sex, body mass index, and mean blood pressure.
Results obtained in our study are in the line of those observed by De-Lima [Citation12]. We found that handgrip strength significantly and negatively correlates with augmentation pressure. This association remains significant after adjustment for other clinical variables. It was established by Chirinos et al. [Citation13] that AP derived from the aortic pressure waveform was associated with substantial adverse cardiovascular events and death independently of pulse pressure. Thus the finding that lower HG is associated with higher AP may represent another mechanistic explanation for the role of muscle strength in CV complications. The next parameter estimated in the present study was pulse pressure amplification, which not only predicts cardiovascular events but is also associated with gender difference in age-dependent risk. It was demonstrated by Regnault et al. [Citation14] that in women, particularly post-menopause, the attenuation of PP amplification (mainly related to increased aortic stiffness), contributes to the significant increase in cardiovascular risk. We noticed that HG strength correlated positively with PPA, both in bivariate and multivariate analysis.
Moreover, since sex was independently associated with PPA as well as with Tr, we showed that mean adjusted (for handgrip strength and BP) augmentation pressure was higher in women, while time to return of reflected wave was shorter in females. These hemodynamic traits are associated with an increased risk of adverse cardiovascular outcomes in females. Furthermore, the obtained results support the concept of possible interaction between muscle strength and cardiovascular sequela.
In summary, our study demonstrated the association between handgrip strength and central hemodynamic metrics. These interactions may add a mechanistic explanation for the role of muscle strength as a risk marker for incident cardiovascular complications.
Ethical standards and informed consent
The University Ethics Committee approved the study protocol and written informed consent was obtained from all participants.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Kodama S, Saito K, Tanaka S, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. 2009;301(19):2024–2035.
- Artero EG, Lee DC, Lavie CJ, et al. Effects of muscular strength on cardiovascular risk factors and prognosis. J Cardiopulm Rehabil Prev. 2012;32(6):351–358.
- Leong DP, Teo KK, Rangarajan S, et al. Prognostic value of grip strength: findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet. 2015;386(9990):266–273.
- Firth J, Stubbs B, Vancampfort D, et al. Grip strength is associated with cognitive performance in schizophrenia and the general population: a UK Biobank Study of 476 559 participants. Schizophr Bull. 2018;44(4):728–736.
- Flood A, Chung A, Parker H, et al. The use of hand grip strength as a predictor of nutrition status in hospital patients. Clin Nutr. 2014;33(1):106–114.
- Cohen DD, López-Jaramillo P, Fernández-Santos JR, et al. Muscle strength is associated with lower diastolic blood pressure in school children. Prevent Med. 2017;95:1–6.
- Blanchard AR, Taylor BA, Thompson PD, et al. The influence of resting blood pressure on muscle strength in -healthy adults: resting blood pressure and muscle strength. Blood Press Monit. 2018; 23:185–190.
- Wykretowicz A, Rutkowska A, Krauze T, et al. Pulse pressure amplification in relation to body fatness. Br J Clin Pharmacol. 2012;73(4):546–552.
- Beyer SE, Sanghvi MM, Aung N, et al. Prospective association between handgrip strength and cardiac structure and function in UK adults. PLoS One. 2018;14:e0193124.
- Taekema DG, Maier AB, Westendorp RGJ, et al. Higher blood pressure is associated with higher handgrip strength in the oldest old. Am J Hypertens. 2011;24(1):83–89.
- Hickson SS, Nichols WW, Yasmin , et al. Influence of the central-to-peripheral arterial stiffness gradient on the timing and amplitude of wave reflections. Hypertens Res. 2016;39:723–729.
- Lima-Junior D, Farah BQ, Germano-Soares AH, et al. Association between handgrip strength and vascular function in patients with hypertension. Clin Exp Hypertens. 2019;41(7):692–695.
- Chirinos JA, Zambrano JP, Chakko S, et al. Aortic pressure augmentation predicts adverse cardiovascular events in patients with established coronary artery disease. Hypertension. 2005;45(5):980–985.
- Regnault V, Thomas F, Safar ME, et al. Sex difference in cardiovascular risk: role of pulse pressure amplification. J Am Coll Cardiol. 2012;59(20):1771–1777.