
Abstract
Objectives. Quality of life (QoL) is possibly the most important variable for the patient when subjective results of heart procedures are evaluated. The purpose of this study was to analyze the change in the quality of life 1 year after surgical aortic valve replacement (SAVR). Design. A Finnish single-center prospective cohort intervention study was performed from 2013 to 2018. QoL was assessed with the EQ-5D-3L VAS questionnaire before surgery and 6 and 12 months after surgery. We used univariate analysis to assess the change in the number of people experiencing problems and logistic regression analysis to assess the patients’ characteristics on the change in QoL. Results. At one year follow-up, patients’ quality of life improved in all EQ-5D dimensions. The greatest decreases in patients experiencing problems 12 months after surgery occurred in the dimension “mobility” (–24.1% change in reporting problems, p < .01), “self-care” (–32.9%, p < .01), and “pain or discomfort” (–25.7%, p < .01). Before surgery mean of EQ visual analogue scale (VAS, from 0 to 100) was 63.0 (SD 17.7, n = 604), and 12 months after surgery 81.2 (SD 13.8, n = 367, p < .001). In multivariable analysis, preoperative obesity was associated with better quality of life (OR 3.39, 95% CI 1.007–11.439) in “daily activities” and patients’ higher operative risk was associated with better “self-care” after surgery. Conclusions. SAVR can improve the 1-year quality of life in all dimensions of EQ–5D and self-rated overall health (VAS).
Introduction
Aortic stenosis is a disease of the aortic valve, and it produces symptoms and greatly limits an individual’s life expectancy, if untreated. The three cardinal symptoms of aortic stenosis are angina, syncope, and heart failure. However, symptoms may vary, and limited exercise tolerance may be the first symptom experienced by the patient. Restricted blood outflow gradually damages the left ventricle, and the early treatment with valve replacement is aimed at correcting the symptoms and limitations [Citation1].
Surgery provides relief from the hemodynamic constraint. The evaluation of the results of aortic valve replacement surgery often focuses on specific outcomes. Many studies have focused on differences between biological and mechanical prosthetic valves and studied mortality, morbidity, number of re-operations, and bleeding complications [Citation2], but the patient quality of life has been less often the main outcome in these evaluations. The number of elderly people in open heart surgery increases [Citation3]. In elderly people, cardiac surgical procedures affect less the life expectancy or the risk of future morbidity, but the relief of symptoms and improved overall functional capacity may be of more value to the patient [Citation4].
Cardiac surgery requires modern and expensive technology and therefore it is important that the limited resources are directed to the best benefits to the patients. Standardized assessments of the quality of life provide useful approaches to view the patients’ perspectives [Citation4]. The purpose of this study was to evaluate the change in the quality of life after surgical aortic valve replacement (SAVR).
Materials and methods
The study protocol was approved by the institutional ethics committee (study ID R12265) and all the patients provided written informed consent. The survey was filed on ClinicalTrials.gov (NCT05220111).
Patients
This is a single-center prospective cohort intervention study about the change in the quality of life (QoL) after open aortic valve surgery with a one-year follow-up. The surgeries included in this study were performed in Tampere University Hospital in Finland during the years 2013–2018. Finnish-speaking patients who underwent open aortic valve surgery and filled in the questionnaire on quality of life were all included. The questionnaire form was filled in first immediately preoperatively, and then at 6 and 12 months after aortic valve prosthetic surgery.
Non-participants were patients, who underwent an operation at the time of research but did not fill in the first, preoperative questionnaire and were therefore excluded from the further analysis.
Quality of life measurements
QoL was measured with the EQ-5D-3L questionnaire [Citation5], which the patients filled in the hospital and later at home when the questionnaire was mailed to them 6 and 12 months after surgery. EQ-5D-3L has been widely used in different sectors of health care research [Citation6]. EQ-5D-3L is a standardized measure of health status and consists of questions in five different dimensions and a visual analogue scale (EQ VAS) of general well-feeling. Each dimension describes a different aspect of health. Dimensions consist of questions about “mobility”, “self-care”, “daily activities”, “pain or discomfort”, and “anxiety or depression”. The three answer options are “no problems”, “some problems”, and “extreme problems”. EQ VAS records the patient’s self-rated health on a vertical visual analogue scale, where the endpoints are labelled “best imaginable health state” and “worst imaginable health state”. The Finnish translation of the questionnaire was used with permission from the Euro QoL Group. The English version example of the EQ-5D-3L can be viewed at https://euroqol.org/publications/user-guides/.
Statistics
Data were analyzed by comparing the preoperative values to those at 6 or 12 months after the operation. With normally distributed values we report the mean with standard deviation (SD). Variables were partitioned by age, sex, type of operation, ejection fraction, EuroScore II, and BMI. Median with interquartile range was used to analyze EQ VAS. Odds ratio (OR) with 95% confidence intervals (95% CI) was used when reporting the results of the logistic regression model.
In the analysis, responses to the studied dimensions of QoL were dichotomized to “no problems” and “any problems” and analyzed as nominal variables. As an improvement of health status, we measured the change from “any problems” to “no problems”. Related-Samples Cochran's Q-test was used in analyses of dimensions and Friedman's test in VAS to compare the change of QoL between different points in time. We also evaluated differences between participants and non-participants using a t-test between those groups, when the parameters were normally distributed.
We used multivariable logistic regression analysis of dichotomized variables for determining, which factors had significant, independent effects on dimensional and EQ VAS score results. Covariates for analysis were patients’ physical characteristics (age, sex, and body mass index), preoperative cardiac function (ejection fraction, EF), and operative risk status (EuroScore II). Also, EQ-5D dimensions were chosen as nominal group covariates to assess the associations to the overall quality of life measured as EQ VAS. Hosmer–Lemeshow test was used to determine the goodness of fit of the logistic regression model.
p-Values of 0.05 or less were considered statistically significant. Statistical analyses were performed with IBM SPSS Statistics version 25 (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY, USA).
Results
Response rate
Between the years 2013 and 2018 overall 625 patients (71.0% of all 880 elective cases operated for SAVR) filled in the preoperative questionnaire. Five hundred and twenty-four (83.8%) of them returned the 6-month postoperative questionnaire and 366 (58.6%) returned the 12-month postoperative questionnaire. Response rate within the five dimensions varied but only slightly.
Characteristics of study participants
Participants, operation types, and covariates are shown in . The majority of the operations were isolated aortic valve replacements, and secondary operation on the mitral valve was included in 13.1% of patients and on the tricuspid valve in 13.3% of patients.
Table 1. Participants and non-participants.
In the 150 female and 273 male non-participant patients, emergent operations counted for 13.0% of operations. When evaluating differences between the groups of participants and non-participants, EuroScore2 was statistically significantly higher in non-participants (mean EuroScore 2 being 3.43) than in participants (2.32, correspondingly p < .05). With respect to other characteristics (such as the age, serum creatinine level, ejection fraction, aortic closure time, perfusion length, and patient weight) there were no differences between the participants and the non-participants.
Univariate analysis
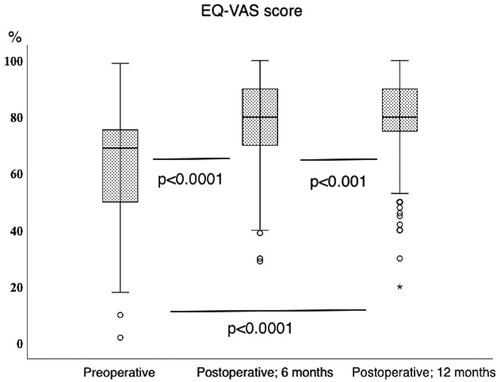
The increase in EQ VAS scores over time after surgery was seen throughout the data. shows patients’ overall assessment of the quality of life (in VAS score) before and after surgery. The mean preoperative VAS score was 63.0 (SD 17.7, n = 604), at 6-month postoperatively it was 77.6 (SD 14.8, n = 521) and at 12-months 81.2 (SD 13.8, n = 367), respectively.
Figure 1. EQ VAS score before and after surgery. Median with interquartile range of EQ VAS scores of the patients’ self-rated health at preoperative, 6- and 12-month evaluations. The improvement of EQ VAS score is better at 6 and 12 months as compared to preoperative score in related-samples Wilcoxon signed rank test.
shows the changes in the numbers of people experiencing QoL-related problems in EQ-5D at 6 and 12 months postoperatively.
Table 2. Change in the number of patients reporting problems.
The greatest postoperative reduction in the number of participants experiencing problems occurred in the dimensions of “mobility”, “self-care”, and “pain or discomfort”. The number of participants, who experienced problems with “daily activities” and “anxiety or depression” also decreased. In the latter dimensions, the number of people experiencing problems was small at the beginning and the percentage change thus was less. Compared to the preoperative situation, at 6 months there was a decrease in the number of people experiencing problems, but at 12 months postoperatively the decline in the problems was greatest.
Multivariable analysis using logistic regression
Postoperative EQ VAS score improvement was analyzed in the logistic regression analysis at 12 months, and the results by the dimensions of EQ-5D-3L are summarized in . The improvement in the EQ VAS score was affected by improved self-care and improved pain and discomfort status.
Table 3. Results of multivariable logistic regression analysis.
When individual dimensions were under investigation, improved “mobility” was associated with an improved VAS at 6 months. In addition, high-risk patients (EuroScore 2> 5%) were more likely to gain a smaller VAS score at 6 months.
The patient-related and preoperative characteristics (age group, sex, ejection fraction, body mass index class, and EuroScore 2 rating) were included in the logistic regression model as independent variables. Improvements in the 12-month assessments (as compared to preoperative) of the studied five dimensions were studied as dependent variables. In general, our finding was that these preoperative characteristics did not appear as predictors of improvement in the QoL dimensions.
Higher classes of EuroScore 2 (2–5 and >5%), indicating more risk in the operation, were associated with improved self-care at 12 months (EuroScore 2 2–5% indicating OR 1.793, CI 95% 1.020–3.150 and EuroScore 2 >5% OR 2.960, CI 95% 1.219–7.188, respectively. This was evident only later in the recovery since higher EuroScore 2 was not recognized as a significant predictor of improved self-care at 6-month postoperative evaluation in the logistic regression model (p = .064).
Also, overweight patients (with a BMI > 30 kg/m2) were more likely to have an improved assessment in usual activities at both 6 months (OR 3.790, CI 95% 1.293–11.110) and 12 months (12-month OR 4.009, CI 95% 1.138–14.125) after surgery.
Discussion
In this single-center one-year follow-up study we could demonstrate improvement in quality of life in all five dimensions of the EQ-5D-3L tool after surgical aortic valve replacement. In addition, the overall patients’ self-rated health on the visual analog scale (VAS) was higher after surgery at 6 and 12 months of follow-up. The improvement was most remarkable in the dimensions measuring mobility, self-care, and pain or discomfort. The improvement in individual VAS scores was mostly related to improvements in self-care and pain or discomfort when analyzed in logistic regression analysis.
In the logistic regression model, we measured all the QoL dimensions in relation to preoperative patient characteristics. Interestingly, the higher operative risk was related to the higher postoperative quality of life in the self-care dimension. We also observed overweight patients to be more likely to have an improved assessment of usual activities. We also examined the potential explanatory factors in the change of QoL but none of the selected variables were identified as predictive in our analyses. In the following paragraphs, we summarize our findings and compare them to other studies.
Higher operative risk
EuroScore 2 2–5% and >5% were related to the higher postoperative quality of life in the self-care dimension. This might reflect the general deviation from good health and restrictions in daily life related to many of the risk factors built into the EuroScore 2 risk model. On the other hand, it reflects that patients with a higher risk of SAVR still might benefit from the results of surgery, if the procedure is successful. We did not analyze here if any deviations from normal recovery could have changed the result.
In logistic regression analysis, improved self-care and improved status in relation to pain or discomfort were related to improved self-assessed general health (i.e. VAS score) one year after SAVR, when compared to the effects of other dimensions, such as mobility, usual activities, or anxiety. It has been shown that physical components of quality of life and vitality and general health have been better after SAVR [Citation7]. The improvement has been less when the age or physical or mental components of quality of life have been higher [Citation8].
Obesity
Morbid obesity has been shown to be related to complications after cardiac surgery, and long-term quality of life has been less than in less obese patients when CABG patients were studied [Citation9]. Still, it has been shown that also obese patients benefit from cardiac surgery [Citation9,Citation10]. Therefore, our results indicating that preoperative obesity was a favorable factor in terms of later QoL in usual activities after SAVR was novel and interesting.
Female sex
In earlier studies female sex has been shown to be related to a less favorable quality of postoperative life in SAVR [Citation11]. In general, as seen also in other studies, approximately one-third of women have not gained improvement in their quality of life after cardiac surgery [Citation12]. In our material, the women experienced more often than men negative changes in the QoL dimensions, especially in dimensions of pain or anxiety.
Age
Age itself doesn’t preclude operative treatment of aortic stenosis, since even symptomatic patients with higher age benefit from valve procedures and can experience HRQoL close to or better than the reference population [Citation3,Citation13]. The selection of procedures should more concentrate on co-morbidities than on age itself [Citation3,Citation13–15]. In our multivariate analysis, the patient’s age did not appear to be an independent factor in changes in the quality of life dimensions EQ VAS. This itself is an interesting finding and suggests, that higher age automatically is not related to poorer QoL after SAVR.
Mental health
It has been noted that depression before valve surgery is related to poorer outcomes in postoperative physical health and that increased immediate postoperative depression reflects worse outcomes also in the physical and mental components of QoL [Citation16]. This may even resemble post-traumatic stress disorder syndrome to some extent [Citation17]. In our study, the number of people, who experienced depression or anxiety decreased after SAVR. This might reflect the improved mobility and physical health of the respondents.
Aortic valve disease as an adaptative process
Symptomatic aortic valve disease seems to be an adaptive process because patients mostly reported “no problems” in usual activities before the surgical treatment. This may explain, why the treatment did not show any major change in this dimension in univariate analysis, but self-care was still improved after 6 or 12 months after SAVR. It is to be noted, that these dimensions do not necessarily measure the need for extraneous help outside the home or the need for help in daily activities at home. Overall improvement, however, was remarkable in other dimensions we measured.
Strengths and weaknesses
One strength of our approach was that we used a well-established questionnaire as a measurement of HRQoL. EQ-5D-3L is a relatively comprehensive measure for the patients and provides reliable results on dimensions of quality of life [Citation6]. Our catchment area comprises 1.2 million inhabitants and differential selection to cardiac surgical services is minor in our country with well-functioning cardiac health care. Our analysis also measured the inter-dimensional effects by controlling their combined effects in the logistic regression multivariable model, thus pinpointing what dimensions mostly affected the overall self-reported health improvement. Surgical indications for SAVR have not changed dramatically, so the results may be generalized to surgical populations of similar ages. However, the increasing number of catheter-based valve implantations may gradually change this.
The potential for selection bias we evaluated from our database comprising all SAVR patients operated on during the study. From there we can judge that no selection based on sex or age was present. However, we have no systematic research on the reasons why some patients did not participate in the study. Also, our legislation prevents us from adhering to these reasons.
A permanent dilemma in measuring HRQoL is that the measure is intra-personal and the subjective change over time is not necessarily objectively the same for all participants. Also, the judgement of HRQoL in the patient is often a “layman’s” view, and health care professionals might evaluate the situation differently than the patient does.
Moreover, the HRQoL measurements tend to carry a ceiling effect, where the sensitivity to small changes in QoL does not necessarily appear as significant [Citation18]. EQ-5D-3L also suffers from this effect due to the limited number of available options to choose from in each dimension and to reduce this, a new EQ-5D-5L has been developed [Citation19]. Unfortunately, when planning and starting this project, the new 5-level option was not available, and we, therefore, maintained the three-level measurements throughout the study to be consistent.
Conclusion
In a conclusion, our research suggests that SAVR can improve the 1-year quality of life and produces improvements in mobility, self-care, and pain and discomfort dimensions. Also, anxiety or depression as a dimension in HRQoL was better, especially at 12 months after surgery. Of patient-related factors, only obesity was related to improvement in daily activities 12 months after surgery. Similarly, the higher operative risk was related to improvement in the self-care dimension. The overall improvement in the VAS scale of QoL was evident in patients recovering from SAVR. This was greatly affected by the increase in QoL in the dimensions of self-care and pain or discomfort.
Acknowledgements
The authors want to express their gratitude to surgical ward nurses at Tampere University Hospital Heart Center for helping to collect the data for this survey.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Czarny MJ, Resar JR. Diagnosis and management of valvular aortic stenosis. Clin Med Insights Cardiol. 2014;8(Suppl 1):121–24.
- de Heer F, Gökalp AL, Kluin J, et al. Measuring what matters to the patient: health related quality of life after aortic valve and thoracic aortic surgery. Gen Thorac Cardiovasc Surg. 2019;67(1):37–43.
- Spaziano M, Carrier M, Pellerin M, et al. Quality of life following heart valve replacement in the elderly. J Heart Valve Dis. 2010;19(4):524–532.
- Bradley SM, Strauss CE, Ho PM. Value in cardiovascular care. Heart. 2017;103(16):1238–1243.
- EuroQol Research Foundation. EQ-5D-3L user guide; 2018. Available from: https://euroqol.org/publications/user-guides
- Rabin R, de Charro F. EQ-5D: a measure of health status from the EuroQol group. Ann Med. 2001;33(5):337–343.
- van Geldorp MWA, Heuvelman HJ, Kappetein AP, et al. The effect of aortic valve replacement on quality of life in symptomatic patients with severe aortic stenosis. Neth Heart J. 2013;21(1):28–35.
- Blokzijl F, Houterman S, van Straten BHM, et al. The impact of surgical aortic valve replacement on quality of life—a multicenter study. J Thorac Cardiovasc Surg. 2021;161(4):1204–1210.e7.
- Hokkanen M, Järvinen O, Huhtala H, et al. The effect of obesity on long-term survival and health-related quality of life after coronary artery bypass grafting: a 12-year follow-up. Coron Artery Dis. 2018;29(5):378–383.
- Barnett SD, Martin LM, Halpin LS, et al. Impact of body mass index on clinical outcome and health-related quality of life following open heart surgery. J Nurs Care Qual. 2010;25(1):65–72.
- Caponcello MG, Banderas LM, Ferrero C, et al. Gender differences in aortic valve replacement: is surgical aortic valve replacement riskier and transcatheter aortic valve replacement safer in women than in men? J Thorac Dis. 2020;12(7):3737–3746.
- Bjørnnes AK, Parry M, Falk R, et al. Impact of marital status and comorbid disorders on health-related quality of life after cardiac surgery. Qual Life Res. 2017;26(9):2421–2434.
- Shan L, Saxena A, McMahon R, et al. A systematic review on the quality of life benefits after aortic valve replacement in the elderly. J Thorac Cardiovasc Surg. 2013;145(5):1173–1189.
- Kurfirst V, Mokráček A, Krupauerová M, et al. Health-related quality of life after cardiac surgery – the effects of age, preoperative conditions and postoperative complications. J Cardiothorac Surg. 2014;9(1):46.
- Sundt TM, Bailey MS, Moon MR, et al. Quality of life after aortic valve replacement at the age of >80 years. Circulation. 2000;102(Supplement 3):III-70.
- Goyal TM, Idler EL, Krause TJ, et al. Quality of life following cardiac surgery: impact of the severity and course of depressive symptoms. Psychosom Med. 2005;67(5):759–765.
- Stoll C, Schelling G, Goetz AE, et al. Health-related quality of life and post-traumatic stress disorder in patients after cardiac surgery and intensive care treatment. J Thorac Cardiovasc Surg. 2000;120(3):505–512.
- Johnson JA, Pickard AS. Comparison of the EQ-5D and SF-12 health surveys in a general population survey in Alberta. Canada. Medical Care. 2000;38(1):115–121.
- Janssen MF, Pickard AS, Golicki D, et al. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: a multi-country study. Qual Life Res. 2013;22(7):1717–1727.