
ABSTRACT
The cognitive intervention programme ‘New Challenges’ targeting adult men with a criminal lifestyle was evaluated in a pilot study. The participants were divided into a cognitive treatment group (n = 32) and a control group (n = 11). In the control group, six participants had no treatment and five participated in 12-step treatment. The participants were measured pre and post using the Psychological Inventory of Criminal Thinking Styles (PICTS), the abridged version of sense of coherence (SOC), Positive and Negative Affect Scale, and Bergström’s quality of programme delivery (QPD). The results of the treatment group showed that criminal thinking patterns dropped significantly from high values to close to normal level. SOC and positive affect increased significantly in the treatment group. Both SOC and positive affect showed positive correlation with QPD. Regarding the possible influence of the 12-step treatment, there was no difference in the control group between participants receiving 12-step treatment and those not receiving treatment. The main conclusion is that the cognitive treatment programme ‘New Challenges’ can contribute to reduced criminal thinking and increased SOC and positive affect, which may prove to be important precursors of reduced criminality.
Introduction
Present knowledge regarding the treatment of long-term criminality is primarily based on risk models and prison studies (Kriminalvården, Citation2014; Mitchell, Wilson & Mackenzie, 2006; Ward & Brown, Citation2004; Öberg & Holmberg, Citation2008). However, established methods such as cognitive therapy and cognitive behavioural therapy have less effect in prisons because of the fellow-inmate group processes that inevitably result in conformity to criminal norm systems (Fridell & Hesse, Citation2005). Fridell and Hesse (Citation2005) also argue that a problem regarding research on criminal rehabilitation effects is that variables such as criminal thinking patterns, antisocial norms and attitudes and personality variables (e.g. negative affect) are seldom included although they have proved to be important predictors of relapse. In positive criminology, focusing on developing inner and outer protective factors, salutogenic value systems and positive affect are central.
Lifestyle criminality is habitual criminality, defined in terms of debut, frequency and permanence as well as social and psychological factors (Andersson & Nordh, Citation2014; Torstensson Levander, Citation2013; Walters, Citation1990, Citation2002). This involves early debut (<15 years of age), high frequency of different types of crime with increasing gravity, permanent connections with criminal persons, documented drug abuse and/or psychiatric problems.
According to cognitive theory, criminal acts can be related to an automatic information processing (Beck, Citation1995), which takes place spontaneously on the basis of cognitive schemata. This is habitual thinking that functions with little or no critical thinking. Individual cognitive schemata comprise both positive and negative thinking patterns that involve thinking errors (Beck, Citation1995). Thinking errors are irrational thinking, meaning seeing something categorically without nuances. It can involve assuming something without grounds, focussing on negative events that may happen, seeing occasional events as a pattern and magnifying or diminishing isolated aspects. If the individual’s thinking patterns and automatic thoughts are too negative or unrealistic, the result is misinterpretations of situations, negative or unrealistic feelings and in some cases mental illness or destructive behaviour such as criminality (Beck, Citation1995). According to Walters (Citation1990), lifestyle criminality can be related to eight specific thinking patterns consisting of mollification, cut-off, entitlement, power orientation, sentimentality, super-optimism, cognitive indolence and discontinuity. According to cognitive theory, thinking patterns are assumed to influence how the individual views him/herself and existence and reacts in different situations.
In similar ways, salutogenic theory links the individual’s general perception of self and surroundings and coping ability to sense of coherence (SOC; Antonovsky, Citation1993). The concept is based on comprehensibility, manageability and meaningfulness, and is linked to the individual’s trust in inner and outer resources. Comprehensibility is the cognitive aspect of SOC, and it is developed through predictable social interaction that makes the individual aware of the connections in social relationships. Manageability is the subjective experience of having sufficient inner resources and ability through others to handle different situations in life. Manageability is dependent on comprehensibility in that the individual needs to understand an event to act adequately. Meaningfulness is the emotional and motivational aspect of SOC, which increases when the individual is involved and participates in social situations. Konarski (Citation1996) demonstrates that meaningfulness is partly dependent on the values structuring the individual’s life. Low values of SOC have shown to correlate with high levels of criminality and antisocial behaviour (Lindblom, Eriksson, & Hiltunen, Citation2017; Ristkari et al., Citation2009). Similarly, the degree of emotional stability, so-called neuroticism, relates to antisocial behaviour such as criminality (Ellison, Citation2006; Van Dam, Janssens, & De Bruyn, Citation2005). Neuroticism is a personality variable that comprises negative affects such as anxiety, irritability, dysphoria, insecurity, impulsivity and stress sensitivity (Paunonen & Ashton, Citation2001). Persons with antisocial behaviour have higher values of neuroticism than the normal population (Ellison, Citation2006; Van Dam et al., Citation2005), and the correlation is stronger with increased age (Ellison, Citation2006). This relation between neuroticism and criminality can seem contradictory since criminal behaviour is often associated with antisocial personality disorder and psychopathy that seemingly lack neurotic characteristics such as fear and anxiety (Bulten, Nijman, & Van Der Staak, Citation2009; Mitchell & Tafrate, Citation2012). However, research on affective states shows that such anxiety-free states rather can be a result of specific coping strategies (Brody & Rosenfeld, Citation2002; Gacono, Citation1990; Gacono, Meloy, & Berg, Citation1992). Lack of anxiety is assumed to be dependent on the immediate acting out of inner sensations in combination with denying own weakness (i.e. escape from anxiety), as the coping strategy of an antisocial person is control (Sundell & Sundell, Citation2005).
Emotions are also linked to the self-image, which, according to Johnson (Citation2003), is defined by the affective experience of ourselves. A good self-image is thus associated with high values of SOC (Johnson, Citation2003, Citation2004). For the individual, SOC can change in a positive direction through external events and experiences of being able to handle new challenges. Changes that strengthen the SOC are, however, rare and relate to consistent changes in attitudes and behavioural patterns (Svartvik & Nilsson, Citation1998). Hult, Waad, Cederblad, and Hansson (Citation1996) have translated the concepts comprehensibility, manageability and meaningfulness into how they are used in treatment (i.e. salutogenic practice). To make a change, the individual has to understand that a certain change is necessary (comprehensibility). In addition, the individual needs to feel involved in relation to his/her value system where change is desirable (meaningfulness). Finally, the individual needs to have practical knowledge of assets, resources and opportunities (manageability). The salutogenic approach to change in treatment meets the requirements for individual experience of SOC (Hult et al., 1996).
In the same way as the salutogenic perspective, positive criminology clarifies the experiences that help the individual to develop personally and socially (Ronel & Segev, Citation2015). Aspects such as the environment, meaning-creating activities and relationships are seen as significant to the individual’s value system and reduced risk of criminal behaviour. Research on criminal treatment in prisons has shown that the therapeutic environment in the prison section is of great importance to the treatment results (Mitchell et al., Citation2006; Öberg & Holmberg, Citation2008). The therapeutic environment refers to the basic character of the treatment units; the treatment units are separate from other prison sections, run frequent urine screens to prevent drug abuse and often practice self-governance with activities such as work, study, parental groups and artistic projects to a greater extent than in other prison sections. Also, Öberg and Holmberg (Citation2008) show that the effects of cognitive treatment are greater if the intern is reintegrated from prison by inpatient care, which often provides 12-step treatment. Inpatient care means that the intern is under treatment outside of the prison during the last time of the sentence. Interns participating in 12-step treatment display a greater SOC and meaning in life with gradual decrease of negative feelings compared to interns who only receive social support through self-help groups (Chen, Citation2006). The results show that developing a salutogenic value system gives a greater effect than only social support. Similarly, Bergström (Citation2012) claims that it is important to develop a value system that is incompatible with criminality. Here, logic processing is not enough and it should be combined with rituals, symbolic actions and shared experiences that give an emotional conviction of the possibility of change. Walters (Citation2001) emphasizes the importance of achieving a strong alliance and trustful relationship between therapist and client. This allows criminal rituals to be replaced with more salutogenic rituals.
Aim of the study
The general aim of the study was to contribute to evidence-based research of criminal rehabilitation by combining the risk and protective factors. The cognitive intervention programme ‘New Challenges’ targeting adult men with a criminal lifestyle was evaluated with a major focus on criminal thinking styles and salutogenic factors. Using a quasi-experimental design, the Val-Bo model was studied, which involves 1 week of group treatment, 4 weeks of individual treatment, and 1 week of group treatment. The effects of concurrent 12-step treatment on criminal thinking patterns and SOC were also analysed.
Material and methods
Participants
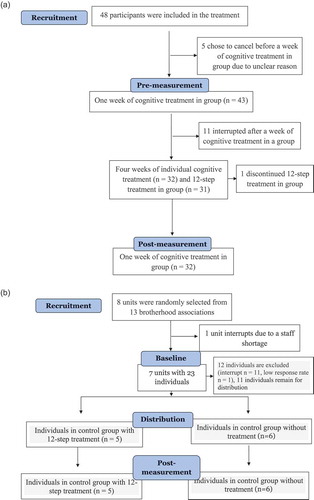
The participants were men aged 19 to 60 years of age in the advanced phase of lifestyle criminality, recruited from one treatment institution and seven control units. The participants in the treatment group received (1) 1 week of cognitive group treatment (40 h), 4 weeks of individual treatment (20 h) and 1 week of group treatment (40 h) combined with 12-step treatment (100 h, five hours/day for 4 weeks). Participants in the control group received (2) no treatment or (3) 12-step treatment (107 h in outpatient care, three hours/day for seven weeks). The therapy group consisted of 32 participants with a mean age of 30.6 (SD = 9.1). The control included 11 participants with a mean age of 28.4 (SD = 2.2), of whom six participated in no treatment and five participated in 12-step treatment. Only the participants who completed a whole programme according to the Val-Bo model were included in the study. Five participants were excluded from the study because they withdrew before the conclusion of the first week of treatment. An additional 11 participants were excluded, but they completed the first week of group treatment and were used to measure differences in client satisfaction and the programme leaders’ adherence to the programme. The distribution in terms of age, ethnicity, creed, level of education and previous treatment was the same for the treatment and control groups ().
Table 1. Descriptive data on the therapy and participants in the study, N = 43.
The participants were matched by self-screening procedures instead of register data because the target group was defined by Walters (Citation1990) definition of lifestyle criminality. The difference between lifestyle criminality and other forms of criminality is that the latter depicts criminality per se (debut, frequency and duration), whereas the former include also other circumstances such as habits, social activities and alcohol and drug use (Torstensson & Levander, Citation2013). Thus, a more detailed picture of the individual and the living circumstances is needed when lifestyle criminality is assessed, and therefore a self-screening instrument developed by Bergström (Citation2014) was used. This included lifestyle analysis made by The Lifestyle Criminality Screening Form, assessment of psychosocial history (phases of criminal career), screening of cognitive thought patterns (The Psychological Inventory of Criminal Thinking Styles; PICTS), as well as assessment of the phases of drug dependence (Gorski & Miller, Citation1993).
The treatment institution was an inpatient care facility where the programme was implemented with the so-called Val-Bo model. Inclusion criteria were that the unit was licenced to use the programme and that the therapists met the required formal qualifications, which were training as therapy assistant and 8 days of programme leader training. Inclusion criteria for participants were a minimum age of 18, no ongoing alcohol or drug abuse and being in an advanced phase of criminal lifestyle (Walters, Citation1990). The criteria were tested with Bergström’s (Citation2014) self-report instrument (see Instruments section).
Participation was voluntary, and the study was approved by the Regional Ethics Review Board in Uppsala. However, the treatment programme ‘New Challenges’ is mandatory in the Val-Bo model.
According to Bergstrom’s (Citation2014) instructions, ongoing alcohol or drug abuse must be treated before or possibly concurrent with participation in ‘New Challenges’. Urine testing was carried out during the programme and the participants were discharged if the result was positive. Also, the cohort study of Nilsson, Estrada, and Bäckman (Citation2014) shows that drug abuse, social inclusion and/or exclusion in adult life are correlated with criminality. Taken together, these studies demonstrate that drug abuse is a central factor for maintaining the process of criminality as well as to keep a distance from positive changes in their lives.
The control units were recruited from eight randomly selected organizations affiliated to KRIS (Kriminellas Revansch i Samhället [Reintegration of Prisoners into Society]), which is a non-profit organization helping ex-prisoners and addicts to re-enter society. One control unit withdrew from participating because of lack of staff. Inclusion criteria for the control group were identical with the treatment group. Instead of urine testing, the recruiters from KRIS used their knowledge of psychological and social circumstances to recruit participants whose main problem was criminal behaviour and not alcohol and/or drug abuse. The control group participants received 12-step treatment and were screened for abuse (urine testing) according to the Swedish guidelines for addiction treatment. Exclusion criteria for the control group were the same as for the treatment group (environmental crime, traffic misdemeanours (fines), financial crime involving companies and sexual crimes). In total, 12 control persons were excluded from the study. Eleven control persons were excluded because they withdrew from the study and one was excluded on the grounds of missing answers in the questionnaires.
Treatment
The programme ‘New Challenges’ combines the risk and protective factors through the cognitive and salutogenic practice in the attempt to change thinking patterns and self- and world perception. The programme includes 15 mandatory sessions and 38 additional sessions, which can be implemented if needed. The exercises of the programme are based on Walters’ (Citation2002) theory of change processes regarding responsibility, self-confidence, meaning and coherence. ‘New Challenges’ is usually practised in individual treatment for several weeks and during one to two intensive weeks in groups. However, the so-called Val-Bo model means 1 week of group treatment, 4 weeks of individual treatment, and finally, one further week of group treatment. The number of treatment hours during the period is usually around 80 to 100 h. The factors that the programme is designed to influence are individual self- and world perception and the criminal thought patterns, according to Walters (Citation1990). The aim of the programme is to increase the individual´s understanding of the criminal norm system underlying the criminal lifestyle. The norm system is based on motives derived from unfulfilled psychological needs that also underlie the criminal thinking (i.e. pathological coping strategies) (Bergström, Citation2012). The motives and thinking patterns are related to the self- and world perceptions and are expressed in criminal behaviour. Through the programme the clients become aware of the causal links in the decision-making process towards a criminal act. This is the crime process that shows individuals commit criminal acts based on their own choices (Walters, Citation1990). The behavioural patterns emerging in lifestyle criminality are defined as a career including of four phases: the pre-criminal phase, the early criminal phase, advanced criminality and the burnout phase (Walters, Citation1990). Different prime motives such as peer pressure, excitement, status, money and anger are characteristics that vary for the various phases.
The most common technique to change thinking patterns is cognitive skills training, which means collecting information, developing alternative solutions and evaluating results (Lipsey, Landenberger, & Wilson, Citation2007). This process takes place with the psychological testing to map the client’s thinking pattern. Based on the results, the therapist and client reach a mutual understanding of the thinking patterns that underlie the client’s problems. Then, together with the group and the therapist, the client can find more functional interpretations of problem situations and alternative ways of acting. To raise awareness of the causal links in the crime process, the therapist uses psycho-education. The change of the criminal self and world perception primarily takes place through discussions and role play about values in different problem situations, dilemmas and issues. In addition, Bergstrom (Citation2012) stresses the difficulty in changing a criminal lifestyle. Challenging criminal thinking patterns usually makes the client consider giving up crime. The moral development, however, requires time to merge with the emotional progress. Thus, Bergstrom (Citation2012) regards the concurrent and subsequent 12-step treatment and the self-help groups as important parts of the rehabilitation process. The programme is presently used in residential institutions in Sweden combined with 12-step-based treatment.
Instrument
The Bergstrom’s (Citation2014) self-report instrument used for inclusion is based on The Lifestyle Criminality Screening Form (Walters, White, & Denney, Citation1991), an analysis of psychosocial history illustrating the phases of the criminal career of Walters (Citation1990), dependency phases (Gorski & Miller, Citation1993) and the PICTS, in accordance with Walters (Citation2006). Data from the test were not available for this study.
The part of Bergstrom’s (Citation2014) assessment that measures criminal lifestyles consists of the four sections – irresponsibility, pleasure, abusive conduct and violation of social rules. Section 1, which measures irresponsibility, has four questions about the breadwinning of children, discontinued education, redundancies and ability to stay in a workplace. Section 2 measures pleasure and has three questions about alcohol and drug history, marital status and physical attributes related to criminal identity. Section 3, which measures abusive behaviour, has four issues of the latest crime, such as murder, rape, robbery, burglary or assault, previous arrests for offensive crimes, the use of weapons at the latest crime and physical abuse of relatives or other related persons. Section 4 that measures break of social rules has three questions about the number of previous arrests, age at first arrest and behavioural problems in school. The test has a total of 0–22 points. A total score of 0–6 points means low probability of a criminal lifestyle (pre-criminal phase), 7–9 points some risk (early criminal phase) and 10 or higher means high risk (advanced criminal phase). The tested must also have at least 1 point on each section.
Self-reporting can measure criminal tendencies early in life before it is possible to be prosecuted for crimes and can reveal crimes undetected in the criminal law system. The thinking patterns investigated in this study are the characteristics of lifestyle criminality, which include crimes of violence, vandalism, theft, shoplifting, fraud, receiving stolen goods, burglary, robbery, drug offences, drunk and drugged driving and driving without a licence. Other types of criminality such as environmental crime, traffic misdemeanours (fines), financial crime involving companies and sexual crimes are associated with other thinking patterns and therefore excluded from this study.
The PICTS questionnaire measures criminal thinking and comprises 80 items with a four-grade Likert scale, 1 to 4. The instrument identifies the values of eight different criminal thinking patterns and a total sum of 32–104 scores, indicating the general degree of criminal thinking (GCT) with the limit value of >50. Values from 61 to 70 indicate a high GCT. Values above 70 indicate a very high level of GCT. According to Walters (Citation1990), criminal thinking patterns are defined as an integration of negative irrational thoughts (thought errors) and different types of denial and distortion of reality (pathological coping strategies). PICTS has a moderate to moderately high internal validity and reliability (Walters, Citation2002). The total score has shown to predict relapse into crime for a 24-month period after release (Walters, Citation2009). The instrument was chosen to fit the purpose of the programme to have an impact on criminal thinking. PICTS is mandatory for the programme and does not involve an extra strain on the participants.
SOC-13 is an abridged version of the original scale SOC-29 (Antonovsky, Citation1991). SOC-13 measures the SOC and encompasses13 items on a seven-grade Likert scale with response alternatives from Very Often to Very Seldom/Never, with the lowest value of 13 and the highest of 91. Score are obtained for comprehensibility, manageability and meaningfulness, which together indicate a total value of SOC. SOC-13 has shown good internal consistency close to the high internal consistency that SOC-29 has shown (Cronbach´s α: SOC-13 = .89, SOC-29 = .93) (Olsson, Gassne, & Hansson, Citation2009). SOC also provides an indication of individuals’ self-image and perception of their surroundings and has an empirical validity concerning the following areas: (1) general perception of self and others (r = .19), (2) stressors (r = .11), (3) health, illness and well-being (r = .32) and (4) attitudes and behaviour (r = .50) (Antonovsky, Citation1993). SOC is negatively correlated with crime, antisocial and rule-breaking behaviour (Ristkari et al., Citation2009).
SOC-13 was chosen for the purpose of providing a measure of an individual’s image of self and the world, which is one of the variables that the programme aims to change. The shorter version of the scale was chosen to facilitate the participant’s concentration during the test, which was assumed to increase reliability.
Positive and Negative Affect Scale (PANAS) includes 20 items describing 10 positive and 10 negative mood states on a five-grade Likert scale with the response alternatives from Very Seldom to Very Often. The lowest value is 20 and the highest is 100. The scale has shown high internal consistency, and the factors positive affect and negative affect are to a high extent non-correlated and stable over a 2-month period (Watson, Clark, & Tellegen, Citation1988). PANAS has high validity for measuring psychological stress, anxiety and depression (Watson, Clark & Tellegen, Citation1988). Personality variables such as emotional instability have proved to be important predictions for crime cases (Ellison, Citation2006; Fridell & Hesse, Citation2005). Emotional instability implies negative affects such as anxiety, irritability, depression, self-esteem, impulsivity and stress sensitivity (Paunonen & Ashton, Citation2001). PANAS was chosen to measure the impact of the programme on the participants’ affects.
Bergström’s quality of programme delivery (QPD) is an evaluation that is included as a concluding element of the programme, which comprises 14 questions (15 if next-of-kin participates) with a five-grade Likert scale from 0 to 4. The test estimates a total score between 0 and 56 (60 if next-of-kin participates). Clients assess the therapeutic relationship, the therapist’s pedagogical ability and the therapist’s methodological competence. Therapeutic relationship is evaluated on the basis of how respected the client has felt during treatment regarding feelings and thoughts. The pedagogical ability is rated on the basis how well the client has understood the purpose of the programme. The methodological competence is rated in terms of how theoretically knowledgeable the therapist was perceived to be and how well the therapist followed the content of programme sections. QPD was used in this study to measure the relation between the client’s assessment of treatment quality, thinking patterns, SOC and positive affect and negative affect.
Multiple-choice questions on age, ethnicity, creed, level of education and previous and concurrent treatment were used for comparison of the demographic composition of the groups.
Procedure
The recruited programme leaders and the contact persons consented to participate asked the persons in the units that met the inclusion criteria to participate. Inclusion criteria were established with Bergstrom’s (Citation2014) self-report instrument. For the treatment group, chemical addiction was treated before the programme. The treatment group filled in a questionnaire with questions on demography, previous and concurrent treatment, PICTS, SOC-13 and PANAS pre- and post-treatment with the programme ‘New Challenges’. QPD was answered after the first and final weeks, respectively, of the programme.
The same procedure was applied to the control group participants, except they did not answer the QPD. The control group participated for the same time period as the treatment group. For the selection process and flow of the participants, see .
Figure 1. Flow charts depicting the recruitment process of the two groups. a) Flowchart of treatment subjects and b) Flowchart of control subjects.
Data analysis
Mixed ANOVA was used to analyse the effect of the treatment on criminal thinking patterns, SOC and positive and negative affect. Mixed ANOVA was used to analyse the effects of the 12-step treatment and no treatment, respectively, regarding criminal thinking patterns and SOC. Cronbach’s alpha was used to test the QPD scale’s internal consistency. Independent t test was used to analyse differences in client-assessed quality between clients who withdrew from and completed treatment, respectively. Pearson’s correlation was used to analyse the correlation between programme quality and other dependent variables (criminal thinking patterns, SOC and positive and negative affect). The independent variable used in the analysis was treatment, with the conditions of cognitive treatment with concurrent 12-step treatment, only 12-step treatment and no treatment. The dependent variables were criminal thinking patterns, SOC, positive and negative affect and quality of programme delivery.
Results
Criminal thinking patterns – PICTS
Treatment vs. control
Mixed ANOVA showed significant main effect of time, F(1,40) = 39.69, p < .01, partial, η2 = .50, d = 1.0, and significant interaction of group × time, F(1,40) = 18.94, p < .01, partial η2 = .32, d = 0.99. The main effect of group was not significant, F(1,40) = 0.97, p = .33. shows the mean value with confidence interval for each condition. Post hoc comparisons with Bonferroni showed that there was no significant difference in the PICTS mean value between the treatment group and the control group at pre-measurement (p = .24). The treatment group had a significantly higher mean value in PICTS before compared with after the treatment (p < .001). The control group showed no significant difference in PICTS mean value between pre- and post-measurement (p = 1.0). Post-measurement, the treatment group had a significantly lower mean value in PICTS compared with the control group (p < .005). shows the mean values of PICTS measurement for both the treatment and control group at pre- and post-measurement.
Table 2. Mean (M), standard deviation (SD) and 95% CI of mean regarding criminal thinking patterns for each group before and after..
Figure 2. Mean score of the psychological inventory of criminal thinking styles (PICTS) before and after for the therapy group and the control group. Each mean with ±SE.
Treatment vs. only 12-step vs. no treatment
Mixed ANOVA was used, which showed a significant main effect of time, F(1,39) = 15.83, p < .001, partial, η2 = .29, d = 0.97, and significant interaction of group × time, F(2,39) = 9.25, p < .001, partial η2 = .32, d = 0.97 (). The main effect of group was not significant, F(2,39) = 0.56, p = .58. Post hoc comparisons with Bonferroni showed no significant differences in PICTS between pre- and post-measurement for control persons undergoing 12-step treatment or for control persons without treatment (p = 1.0 in all comparisons).
Sense of coherence – SOC-13
Treatment vs. control
Mixed ANOVA showed significant main effect of time, F(1,39) = 8.92, p < .01, partial, η2 = .19, d = 0.83, and significant interaction of group × time, F(1.39) = 6.70, p < .02, partial η2 = .15, d = 0.71. The main effect of group was not significant, F(1,39) = .02, p = .89. shows the mean values with confidence interval in all conditions. Post hoc with Bonferroni showed that there was no significant difference in mean value in SOC between the treatment and control group at pre-measurement (p = .46). The treatment group had a significantly lower mean value in the SOC pre-measurement compared with the post-measurement (p < .001). The control group showed no significant difference in SOC mean value between pre- and post-measurement (p = .26). There was no significant difference in SOC mean value between the treatment and the control group at post-measurement (p = .71). shows the mean values for SOC-13 in the treatment and the control group at pre- and post-measurement.
Table 3. Mean (M), standard deviation (SD) and 95% CI of mean regarding sense of coherence for each group before and after..
Figure 3. Mean score of the brief version of the sense of coherence scale (SOC-13) before and after for the therapy group and the control group. Each mean with ±SE.
Treatment vs. only 12-step vs. no treatment
Mixed ANOVA was used, which showed a significant interaction of group × time, F(2,38) = 5.05, p < .01, partial η2 = .21, d = 0.79 (). The main effects of group [F(2,38) = 0.94, p = .40] or time [F(1,38) = 3.90, p = .06] were not significant. Except for a significant (p = .001) difference in the treatment group (pre- and post-treatment), post hoc with Bonferroni showed no significant differences in SOC between pre- and post-measurement for control persons under 12-step treatment or for control persons without treatment (p = 1.0).
Positive and negative affect – PANAS
Analysis with mixed ANOVA showed significant interaction of group × time regarding positive affect, F(1,39) = 6.0, p < .02, partial η2 = .13, d = 0.67. Interaction showed (post hoc with Bonferroni) that positive affect increased significantly (p = .02) for the treatment group between pre- and post-measurement, while it remains the same (p = 1.0) for the control group. There were no significant differences regarding negative affect for time, F(1,39) = 0.0, p = .96, group, F(1,39) = 0.32, p = .57, or group × time, F(1,39) = 1.42, p = .24. shows the PANAS’s mean values with confidence interval in all conditions. shows the mean values for positive affect for the treatment and the control group at pre- and post-measurement.
Table 4. Mean (M), standard deviation (SD) and 95% CI of mean regarding positive and negative affect for each group before and after.
Figure 4. Mean score of the PANAS positive affect before and after for the therapy group and the control group. Each mean with ±SE.
Quality of Programme Delivery – QPD
Analysis with Cronbach’s alpha showed high internal consistency for QPD, α = .89, and the subscales pedagogical ability, α = .83, and therapeutic relationship, α = .88, and relatively good internal consistency for the subscale methods, α = .68. Analysis with independent t -test showed no significant difference in mean value of QPD after the first week of treatment between those who withdrew from treatment and those who withdrew after the first week (M = 46.36, SD = 7.86) and those who completed 6 weeks (M = 47.16, SD = 7.06), t(34) = –0.30, p = .77.
Analysis with independent t test showed no significant difference in mean value in QPD for those who withdrew from the programme after the first week (M = 47.16, SD = 7.06) and those who withdrew after 6 weeks (M = 49.21, SD = 5.60), t(23) = −1.13, p = .27.
Pearson’s correlation showed a significant positive correlation after the treatment between QPD and SOC, r = .39, p < .05, and QPD and PA, r = .64, p < .01. There was also a significant positive correlation between SOC and PA, r = .49, p < .01, and a significant negative correlation between PICTS and SOC, r = –.56, p < .01, and PICTS and PA, r = –.38, p < .05. shows the correlation between QPD, PICTS, SOC and positive affect after treatment.
Table 5. Correlation matrix for quality of programme delivery, PICTS, SOC and positive affect after treatment, N = 31.
Discussion
The positive criminology is a new perspective, which emphasizes positive experiences that potentially prevent or hinder deviant and criminal behaviour, including alcohol and drug abuse (Openhaim & Timor, Citation2005; Ronel, Frid, & Timor, Citation2013). An example of this is the Good Lives Model (GLM) with the main idea of building an internal capacity and coping skills of an individual to elevate the risk of criminality (Ward & Brown, Citation2004). The perspective widens the traditional criminology that primarily aims at understanding risk factors and processes leading to criminal behaviour (Ronel & Elisha, Citation2011). In the present study, the effects of the treatment programme ‘New Challenges’, which combines the two perspectives, are studied. This study is a small-scale pilot study according to the Val-Bo model’s combined group and individual treatment. The main result of the study shows that combined group and individual treatment during 6 weeks reduced criminal thinking patterns and increased SOC as well as positive affect. The result relates to the high degree of client satisfaction and to programme leaders’ adherence to the programme.
The result also shows that the degree of criminal thinking was very high for both the treatment and control groups prior to the treatment. After the treatment, the treatment group’s criminal thinking was reduced to a level near that of the normal population.
Also the effects of the 12-step treatment and the effect of no treatment regarding criminal thinking were compared. All participants except one in the treatment group received 12-step treatment concurrently, while half of the control group received 12-step treatment and the other half no treatment. The result showed no difference in the control group between participants receiving treatment and not receiving treatment. This means that none of the conditions in the control group reduced criminal thinking. The number of participants in the control group was low, however, and the result should be interpreted with caution. A reasonable interpretation is that 12-step treatment on its own does not have a direct impact on criminal thinking patterns, but that a combination of 12-step treatment and cognitive treatment is effective. On the other hand, the study cannot show if a combination of 12-step treatment and the cognitive treatment is more or less effective than only cognitive treatment. On the basis of the fact that concurrent 12-step treatment did not turn out to have a significant effect on the reduction of criminal thinking, however, a conclusion is that a significant change factor for reduced criminal thinking during the 6-week treatment is the cognitive intervention, which is a prediction for reduction of relapse into criminality (Walters, Citation2009). This interpretation is supported by the previous youth study where the participants reduced their criminal thinking and behaviour as a result of cognitive treatment only (Lindblom et al., Citation2017).
The result showed a low degree of SOC in both the treatment and control group prior to treatment. After treatment, the SOC increased to normal values in the treatment group, while the control group remained at its low level.
Further, the effect of 12-step treatment and no treatment, respectively, in the control group was analysed. There were no differences in the control group between participants receiving 12-step treatment or no treatment in the control group. In short, none of the conditions in the control group increased SOC. In the light of the low number of participants, the result should be treated with caution. In contrast to our result, earlier studies show that there is a positive correlation between increased SOC and 12-step treatment (Chen, Citation2006, Citation2010). Besides the low number of participants, a reasonable explanation to the result may be that the control group’s 12-step treatment in outpatient treatment does not provide the same type of impact as in inpatient treatment. Another difference is that the control group’s outpatient 12-step treatment took place in 7 weeks, while the treatment group’s inpatient treatment took place in 4 weeks. However, the number of treatment hours was the same for both groups. The result can also be an effect of a simultaneous salutogenic effect on the treatment participants through both cognitive and 12-step treatment. Control group participants, in contrast, only received 12-step treatment. Yet, an increase in SOC was shown with only cognitive treatment in the previous youth study (Lindblom et al., Citation2017). A further aspect is time. Chen and Gueta (Citation2015) assume that a 12-step programme contributes to a better SOC and gradually decreasing negative affect in the long run. The most immediate change factor for increased SOC is therefore assumed to be the cognitive treatment with ‘New Challenges’.
The result also shows that the degree of positive affect increased for the treatment group while remaining at the normal value level for the control group. No division was made of the control group regarding 12-step treatment or no treatment because comparison of pre- and post-measurement was non-significant for both of these subgroups. No significant differences in negative affect were found after the treatment. Both the treatment and control group bordered on increased values of negative affect. The result can be interpreted to mean that the treatment increased positive feelings while the negative feelings remained constant on the border of increased level for both groups during the measuring period. The non-decrease of negative feelings can be assumed to relate to the fact that neuroticism (i.e. negative affect) is characteristic of the target group criminals and difficult to change with increased age (Ellison, Citation2006; Van Dam et al., Citation2005).
Finally, the programme quality was assessed to be good by the participants. The average quality index was 4 (out of 5). Test with Cronbach’s alpha showed that the scale has a high internal consistency. The assessment applied to both during and after the programme. There were no differences in the assessment of programme quality for the 11 participants that withdrew from the programme after the first week and the participants that completed the 6-week programme. The 11 participants who withdrew after the first week did so because they had completed their time at the inpatient care. It is not uncommon that certain participants are in for only 1 week in group treatment. This has to do with how often the programme is run in the unit. The participants’ scheduled time at the inpatient facility is sometimes over before they have completed a second week. The result can be interpreted to indicate that the clients’ assessment of programme quality does not vary during the programme for clients who complete their whole treatment period. On the other hand, there is no information on how the five clients who chose to withdraw from treatment before the end of the first week assessed the programme.
There was, however, a correlation between programme quality and the outcome variables SOC and positive affect. The client-assessed quality increased with increased SOC and increased positive affect. There was also a positive correlation between the last mentioned variables. As the effect sizes were small and medium sized, the result must be treated with caution. A possible interpretation is the good quality of the treatment in terms of therapeutic relationship, pedagogical skills and methodological competence, which contribute to positive affects and a more salutogenic self- and world-image. Regarding the factors SOC and positive affect, the result is in line with the result of previous research, which indicates that a greater client satisfaction is combined with greater alleviation of symptoms (Clifford Attkisson & Zwick, Citation1982). There was also a correlation between reduced criminal thinking and increased SOC. An interpretation can be that a more salutogenic image of self and the world correlates with reduced criminal thinking but without a causal relationship. In conclusion, the high number of participants completing the programme is assumed to support the positive results regarding programme quality. Only five participants chose themselves to withdraw. A contributing factor to the high number of participants completing, however, can be that some clients were in inpatient care and would have been sent back to prison if they had chosen to withdraw. We have no information about the number of participants who were reintegrated from prison in the inpatient care.
There was also a difference in terms of dropouts in the treatment and control group, which might have slightly influenced the results. While only five participants in the treatment group chose to withdraw, 11 participants in the control group chose to do so. Primarily, the difference is assumed to be an effect of the better circumstances provided for the programme leaders to maintain a continual contact with the participants than the contact persons at the control units. The control units also had a harder time recruiting participants because of the low inflow of individuals meeting the inclusion criteria. This affected the size of the control group. There is also a difference between how alcohol and drug abuse was checked in the treatment group and the six persons in the control group who did not partake in any treatment. Instead of urine screening, the contact persons, who had past experience of chemical addiction and criminality, used their experience-based knowledge which makes it difficult for participants to hide using alcohol or drugs. According to KRIS policy, their members are not allowed to use alcohol, drugs or addictive pharmaceuticals. The contact persons’ special knowledge, the KRIS policy and the relatively short measure period are substantially assumed to be as safe as urine screening. If no-treatment participants had used alcohol or drugs, the result would have shown a higher degree of PICTS and a lower degree of SOC in comparison with the 12-step control participants. The control group participants in the 12-step programme were screened according to the guidelines in Swedish addiction treatment. However, there were no significant differences.
Another difficulty concerning the reliability of the study is that only self-screening instruments were used. Therefore, we were unable to compare the distribution of offence and verdict between the groups. These variables have often been correlated with crime relapses and therefore frequently reported (Fridell & Hesse, Citation2005; Lipsey, Chapman & Landenberger, Citation2001; Tong & Farrington, Citation2004). However, Fridell and Hesse (Citation2005) emphasized that criminal thought patterns, norms, and affects are often ignored, although it has been shown that these variables predict crime relapses. Therefore, our focus was on these factors instead of the common outcome measures.
In subjective reporting, there is also a risk that the results would be influenced by the participants wishing to please (Bryman, Citation2002). It is also well known that there is a placebo effect in subjective reporting, which is influenced, inter alia, by the attendant’s attitudes. Factors in the treatment can therefore have contributed to the improved results. One such factor is that there is often a recognition factor between participants and therapists, as the therapists often have a background in abuse and crime. However, in the youth study by Lindblom et al. (Citation2017), the therapist’s background varied, but the results were still positive. The therapists both in the previous and in the present study were committed and could convincingly communicate the lifestyle model. The improvement can therefore be seen as part of the general process factors described by Frank and Frank (Citation1991), namely an emotionally charged and confidential relationship with the therapist, a particular arrangement for treatment, a theory that provides a way of change and a method that both therapists and participants are involved in and believe in. The relapse analysis of the previous youth study also confirms that the results are maintained over time. This contradicts that the treatment effect to a greater extent would be a result of the participants’ willingness to please or the attitudes of the therapists would have contributed to a placebo effect.
Motivational level of the participants in the treatment group can be discussed, even though it is difficult to estimate. Participants in the treatment group consisted both of persons who were chosen by the Correctional System, as well as of persons who sought the treatment by themselves. Persons at risk to be put back to prison in case of non-compliance to the treatment programme are not necessarily more motivated to treatment than the other participants. One possibility may be that they adopt the treatment with no depth and thus avoid the prison. Even the motivation of the persons who sought the treatment by themselves can be questioned. Reasons for participation can be other than the will to quit the criminality, e.g. a pressure from the relatives or difficult life circumstances (i.e. escape due to threat, dispossession, etc.). In general, there is a lack of motivation to change (Levander, Adler, Gefvert, & Tuninger, Citation2008). Persons with antisocial personality characteristics often prefer simple solutions instead of proposals implicating own responsibility and own efforts (Ekselius, Isaksson & Luciano, Citation2006).
Further, the distribution of age, gender, ethnicity, creed, level of education and previous treatment was similar across the groups, but due to the low number of participants an analysis of these variables was not deemed meaningful. The sociocultural context of the control unit is in agreement with the Swedish general population, with approximately 16% foreign-born citizens (Statistiska central byrån, Citation2018).
The result of the study can be considered to be valid for Swedish men in their thirties in the advanced phase of criminality, according to Walters’ (Citation1990) definition. The main results regarding reduced criminal thinking and increased SOC show the same trend as the results from the youth studies (Lindblom et al., Citation2017). Both studies show substantial effectiveness despite low number of participants. The present adult study, however, displays the effect in a shorter time (6 weeks) compared with the youth study (M = 17 weeks) (Lindblom et al., Citation2017). The adults, however, have had a higher dose of treatment in terms of treatment hours (M = 100) compared with the young people (M = 20). The adults, however, were in the advanced phase of criminality, while the young people were in a pre-criminal or the early phase, which motivates the difference in treatment hours, according to the risk-need-responsitivity model (Andrews, Bonta, & Hoge, Citation1990; Andrews, Bonta, & Wormith, Citation2011). Similarly, the result of the present study corresponds with the youth study regarding SOC (Lindblom et al., Citation2017). Although the studies differ in terms of treatment form (individual and group) as well as in intensity, frequency and duration, the results still indicate that the programme affects the intended factors and target groups. The most probable direct change factor for reduced criminal thinking and increased SOC for the treatment period is assumed to be the cognitive intervention programme ‘New Challenges’. The 12-step programme is presumed to have a more indirect and long-term effect and to be of importance for the sustainability of new thinking and new lifestyle. This assumption is supported by Holmberg and Öberg (Citation2012) who shows positive results against relapse into crime both for cognitive and 12-step treatment. Greatest differences were shown for the sub-population of men above 30 years of age who after the intervention also finished outpatient care during 4½ months. In this longer treatment setting, it looks like 12-step treatment might be more effective compared to cognitive treatment, even though the design of that study was not specifically aimed for this comparison. Therefore, these results might be tentative.
An issue for further research may be to investigate the combined 12-step programme and cognitive intervention compared with only cognitive intervention and only the 12-step programme. A relevant future research focus would therefore be to investigate a larger number of participants over a longer period, investigating both self-reported psychological factors and records of previous culprits, number of convictions, types of crimes and recurrence rate after treatment.
Furthermore, research on rehabilitation efforts for criminals has overruled psychological factors such as criminal thinking and personality variables (Fridell & Hesse, Citation2005). Current research on personality organization relates the criminal thinking primarily to antisocial personality disorder (Bulten et al., Citation2009) and psychopathic personality traits (Mitchell & Tafrate, Citation2012). One common opinion is that the target group is not vulnerable to loss or in need of interpersonal intimacy, and treatment interventions that change the personality structure show poor results (Brody & Rosenfeld, Citation2002). However, these ideas have been questioned because the development of treatment efforts has been hampered by the relatively limited knowledge of how these individuals perceive themselves and the world. The treatment programmes that are used today in lifestyle criminality are based on a cognitive or cognitive behavioural therapeutic perspective (Kriminalvården, Citation2014; Lipsey et al., Citation2007). The ‘New Challenges’ programme focusing on challenging the criminal thought patterns is therefore assumed to contribute to a cognitive understanding that can help the client to change his behaviour (Bergstrom, Citation2012; Lindblom et al., Citation2017). Therefore, if the psychological factors that predict crimes are scrutinized more in research, this may contribute to better-tailored treatment programmes for the target group.
Additional information
Funding
References
- Andersson, J., & Nord, M. (2014). Satsningen mot livsstilskriminellas brottslighet:Genomslag i polisorganisationen (Rapport 2014: 2). Stockholm: Rikspolisstyrelsen.
- Andrews, D. A., Bonta, J., & Hoge, R. D. (1990). Classification for effective rehabilitation:Rediscovering psychology. Criminal Justice and Behavior, 17, 19–52.
- Andrews, D. A., Bonta, J., & Wormith, J. S. (2011). The Risk-Need-Responsivity (RNR)Model. Criminal Justice and Behavior, 38, 735–755.
- Antonovsky, A. (1991). Hälsans mysterium. Stockholm: Natur och Kultur.
- Antonovsky, A. (1993). The structure and properties of the sense of coherence scale. Social Science and Medicine, 36(6), 725–733.
- Beck, J. S. (1995). Cognitive therapy: Basic and beyond. New York: Guilford Press.
- Bergstrom, G. (2012). Kriminalitet som livsstil 5:Erev. Upplagan..Lund: Studentlitteratur.
- Bergstrom, G. (2014). Nya utmaningar: Ledarhandledning. [A new direction: A guide for project leaders]. Stockholm: G and K Pedagogkonsult och Ekonomi AB.
- Brody, Y., & Rosenfeld, B. (2002). Object relations in criminal psychopaths. International Journal of Offender Therapy and Comparative Criminology, 46, 400–411.
- Bryman, A. (2002). Samhällsvetenskapliga metoder. Stockholm: Liber AB.
- Bulten, E., Nijman, H., & Van Der Staak, C. (2009). Psychiatric disorders and personality characteristics of prisoners at regular prison wards. International Journal of Law and Psychiatry, 32, 115–119.
- Chen, G. (2006). Social support, spiritual program, and addiction recovery. International Journal of Offender Therapy and Comparative Criminology, 50, 306–323.
- Chen, G. (2010). The meaning of suffering in drug addiction and recovery from the perspective of Buddhism, Existentialism and 12 step. Journal of Psychoactive Drugs, 42, 363–375.
- Chen, G., & Gueta, K. (2015). Applications of positive criminology in the 12-step program. In I. Ronel, N & D. Segev (Eds.), Positive Criminology (pp. s208–220). London and New York: Routledge Taylor & Francis Group.
- Clifford Attkisson, C., & Zwick, R. (1982). The client satisfaction questionnaire: Psychometric properties and correlations with service utilization and psychotherapy outcome. Evaluation and Program Planning, 5, 233–237.
- Ekselius, L., Isaksson, K., & Luciani, L. (2006). Personlighetsstörningar: Kliniska riktlinjer för utredning och behandling. Stockholm: Svenska Psykiatriska Föreningen och Gothia AB.
- Ellison, M. C. (2006). A quantitative review of the relations between the “Big 3” higher order personality dimensions and antisocial behaviour. Journal of Research in Personality, 40, 250–284.
- Frank, J. D., & Frank, J. B. (1991). Persuasion and healing: A comparative study of psychotherapy (3rd ed.). Baltimore: The Johns Hopkins University press.
- Fridell, M., & Hesse, M. (2005). Psykosociala interventionsmetoder vid kriminalitet och drogmissbruk: Meta-analyser och randomiserade kontrollerade studier. Institutionen för Psykologi: Lunds Universitet och Center for Rusmiddelsforskning, Århus Universitet i Köpenhamn.
- Gacono, C. B. (1990). An impirical study of object relations and defensive operations in antisocial personality disorder. Journal of Personality Assessment, 54, 589–600.
- Gacono, C. B., Meloy, J. R., & Berg, J. L. (1992). Objekt relations, defensive operations and affective states in narcissistic, borderline and antisocial personality disorder. Journal of Personality Assessment, 59, 32–49.
- Gorski, T., & Miller, M. (1993). Vid sunda vätskor: Handbok i återfallsprevention vid kemiskt beroende. Täby: Larsons Förlag.
- Holmberg, S., & Öberg, J. (2012). Effects of drug treatment units in Swedish prisons. Journal of Scandinavian Studies in Criminology and Crime Prevention, 13, 44–63.
- Hult, S., Waad, T., Cederblad, M., & Hansson, K. (1996). Salutogen miljöterapi i teori och praktik: En introduktion för blivande salutogener. Lund: Avdelningen för barn- och ungdomspsykiatri.
- Johnson, M. (2003). Självkänsla och anpassning. Lund: Studentlitteratur.
- Johnson, M. (2004). Approaching the salutogenesis of sense of coherence: The role of ’active’ self-esteem and coping. British Journal of Health Psychology, 9, 419–432.
- Konarski, K. (1996). Meningsfullt sammanhang: en skyddsfaktor för hälsa. Psykisk Hälsa, 1, 32-44.
- Kriminalvården. (2014). Årsredovisning 2014: Från ord till handling. Norrköping: Kriminalvården. Retrieved May 3, 2015 from https://www.kriminalvarden.se/globalassets/publikationer/ekonomi/ar-2014-kriminalvarden-tryckt-versionpdf
- Levander, S., Adler, H., Gefvert, O., & Tuninger, E. (2008). Psykiatri: En orienterande översikt. Lund: Studentlitteratur.
- Lindblom, S., Eriksson, L., & Hiltunen, A. J. (2017). Evaluation of the cognitive intervention programme “A New Direction” targeting young offenders in Sweden. Journal of Scandinavian Studies in Criminology and Crime Prevention, 18, 176–190.
- Lipsey, M. W., Landenberger, N. A., & Wilson, S. W. (2007). Effects of cognitive behavioral programs for criminal offenders. The Campbell Collaboration, 3(6), 1–27.
- Mitchell, D., & Tafrate, R. C. (2012). Conceptualization and measurement of criminal thinking: Initial validation of the criminogenic thinking profile. International Journal of Offender Therapy and Comparative Criminology, 56, 1080–1102.
- Nilsson, A., Estrada, F., & Bäckman, O. (2014). Offending, drug abuse and life chances—A longitudinal study of a Stockholm birth cohort. Journal of Scandinavian Studies in Criminology and Crime Prevention, 15, 128–142.
- Öberg, J., & Holmberg, S. (2008). Behandling av narkotikamissbrukare i fängelse: En effektstudie. (BRÅ-rapport 2008:18). Stockholm: Brottsförebyggande rådet.
- Olsson, M., Gassne, J., & Hansson, K. (2009). Do different scales measure the same construct? Three senses of coherence scales. Journal of Epidemiol Community Health, 63, 166–167.
- Openhaim, M., & Timor, U. (2005). Imprisonment, education and self-image: The influence of studying in Prison Learning Centers on convicts’ self-image. Mifgash – Social-Educational Work, 22, 57–73.
- Paunonen, S. V., & Ashton, M. C. (2001). Big five factors and facets and the prediction of behaviour. Journal of Personality and Social Psychology, 81, 524–539.
- Ristkari, T., Sourander, A., Ronning, J. A., Helonheimo, H., Helenius, H., & Salokangas, R. K. R. (2009). Sense of coherence and criminal offences among young males: Findings from the Finnish from a boy to a man study. Nordic Psychology, 61, 4–13.
- Ronel, N., & Elisha, E. (2011). A different perspective: Introducing positive criminology. International Journal of Offender Therapy and Comparative Criminology, 55(2), 305–325.
- Ronel, N., Frid, N., & Timor, U. (2013). The of positive criminology: A Vipassana course in prison. International Journal of Offender Therapy and Comparative Criminology, 57(2), 133–153.
- Ronel, N., & Segev, D. (2015). Positive Criminology. London and New York: Routledge Taylor & Francis Group.
- Statistiska central byrån (SCB). (2018). Befolkningsstatistik i sammandrag 1960–2017. Stockholm: Statistiska centralbyrån (SCB). Retrieved June 14, from https://www.scb.se/hitta-statistik/statistik-efter-amne/befolkning/befolkningens-sammansattning/befolkningsstatistik/pong/tabell-och-diagram/helarsstatistik–riket/befolkningsstatistik-i-sammandrag/
- Sundell, M., & Sundell, S. (2005). Behavior change in the human services - behavioral and cognitive principles and applications, 5th edition. California: Sage.
- Svartvik, L., & Nilsson, P. (1998). Antonovsky i sitt sammanhang., Ur 15 forskare granskar begreppet känsla av sammanhang. Ord och vetande AB: Uppsala: Forskningsrådsnämnden.
- Tong, L. S. J., & Farrington, D. P. (2006). How effective is the “reasoning and rehabilitation” programme in reducing reoffending? A meta-analysis of evaluations in four countries. Psychology, Crime & Law, 12, 3–24.
- Torstensson Levander, M. (2013). Kronisk kriminalitet som livsstil. (Rapport 2013:2). Stockholm: Rikspolisstyrelsens utvärderingsfunktion.
- Van Dam, C., Janssens, J. M. A. M., & De Bruyn, E. E. J. (2005). PEN, Big Five, juvenile delinquency and criminal recidivism. Personality and Individual Differences 39, 7–19.
- Walters, G. D. (1990). The criminal lifestyle: Patterns of serious criminal conduct. Newbury park: Sage Publications.
- Walters, G. D. (2001). The shaman effect in counseling clients with alcohol problems. Alcoholism Treatment Quarterly, 19, 31–43.
- Walters, G. D. (2002). The psychological inventory of criminal thinking styles (PICTS): A review and meta-analysis. Assessment, 9, 278–291.
- Walters, G. D. (2006). The Psychological Inventory of Criminal Thinking Styles (PICTS) professional manual. Allentown, PA: Center for Lifestyle Studies.
- Walters, G. D. (2009). Effect of a longer versus shorter test-release interval on recidivism prediction with the psychological inventory of criminal thinking styles (PICTS). International Journal of Offender Therapy and Comparative Criminology, 53, 665–678.
- Walters, G. D., White, T. W., & Denney, D. (1991). The lifestyle criminality screening form: Preliminary data. Criminal Justice and Behavior, 18, 406–418.
- Ward, T., & Brown, M. (2004). The good lives model and conceptual issues in offender rehabilitation. Psychology, Crime & Law, 10, 243–257.
- Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54, 1063–1070.