
ABSTRACT
Blaszczynski and Nower conceptualized in 2002 an integrative Pathways Model leading to gambling disorder by postulating three subtypes of individuals with problem gambling characterized by common and specific characteristics (sociodemographic features, comorbidities, psychological factors). Here we propose a clinical illustration that fits each subtype. For each pathway, we (1) describe a corresponding clinical case, (2) propose a symptom-based clinical description, and (3) elaborate a process-based case formulation to explain the development and maintenance of the problematic gambling behavior. We argue that the clinical work with patients benefited from this two-level approach (symptoms vs. psychological processes) combined with a more holistic approach that takes into account intrapersonal (e.g. personality), interpersonal (e.g. family functioning), and environmental variables (e.g. life events). Crucially, our approach not only considers psychopathological dimensions (e.g. symptoms, diagnostic criteria), but it also views as central individual differences (personality traits) and cognitive and affective processes postulated to mediate relationships between biopsychosocial antecedents and psychopathological symptoms. In the current paper, we aim to demonstrate how the Pathways Model can be used as a framework to embrace a holistic perspective that promotes individualized and process-centered psychological interventions for individuals with gambling problems.
Twenty years ago, Blaszczynski and Nower (Citation2002) formulated an integrative model of problem gambling (encompassing biological, personality, developmental, cognitive, learning theory, and environmental factors) and postulated three distinct pathways that lead to problematic gambling (i.e. behaviorally conditioned, emotionally vulnerable, and antisocial-impulsivist pathways). The various pathways described in the model are characterized by common (e.g. ecological determinants such as availability and accessibility, as well as acceptability of gambling, operant conditioning effects, cognitive distortions) and specific characteristics (sociodemographic features, comorbidities, and psychological factors). According to Blaszczynski and Nower (Citation2002; see also, Nower & Blaszczynski, Citation2017), the characteristics of the first pathway are shared by the second and third pathways, whereas the characteristics of the second pathway are shared by the third pathway (Pathway 3 was thus considered a subset of Pathway 2). Recently, Nower et al. (Citation2022, pp. 5–6) revised their model and suggested that Pathway 3 (antisocial-impulsivist) was distinct from Pathway 2 (emotionally vulnerable) and thus constitutes a subgroup with additional features.
Studies conducted on samples of treatment-seeking gamblers (Álvarez-Moya et al., Citation2010; Nower et al., Citation2013; Suomi et al., Citation2014) or samples that include individuals with various degrees of problematic gambling patterns (Chamberlain et al., Citation2017; Devos et al., Citation2020; Moon et al., Citation2016; Turner et al., Citation2008; Valleur et al., Citation2015) have globally reproduced the three pathways postulated by Blaszczynski and Nower (Citation2002), although several studies identified more than three classes or clusters aligning with the pathways via a range of possible mappings (Delfabbro & King, Citation2022, for a review). Furthermore, although the Pathways Model (PM) is considered useful in clinical practice because it contributes to subtype individuals with gambling problems, some authors have suggested that clinical reality is more complex and that the different factors operating in clinical samples interact in a more complex manner than what is theorized in the PM (Mestre-Bach et al., Citation2022). As suggested by Kurilla (Citation2021), there is a need to focus on how the PM can be used to develop individualized treatment approaches for each gambler subtype.
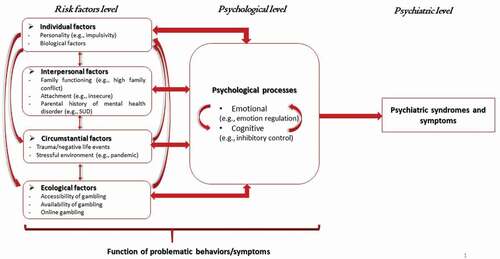
This paper aims to propose a structured analysis of clinical cases by using the PM as a framework. Capitalizing on our clinical experience with patients with problem gambling, and relying on various theoretical frameworks such as the biopsychosocial model (Engel, Citation1980, Citation1997) or the psychological model of mental disorders (Kinderman & Tai, Citation2007), we aimed to provide a comprehensive clinical case illustration for each of the pathways theorized by Blaszczynski and Nower (Citation2002), as well as to propose a framework that clarifies the different levels of analyses used to individualize psychological intervention. In the next sections, after (1) reviewing the evidence supporting each of the three pathways, we (2) describe a corresponding clinical case (each case is summarized in the main article and more comprehensively described in the online supplementary material), (3) propose a symptom-based clinical description (i.e. diagnostic-based approach), and (4) elaborate a process-based case conceptualization (Dudley et al., Citation2011; Philippot et al., Citation2019) that aims to explain the development and maintenance of the problematic gambling behavior. Our holistic and process-based analysis comprises different levels of analysis (see, ): biopsychosocial risk factors, psychological processes, and psychiatric symptoms (and syndromes). Regarding biopsychological risk factors, we distinguished between different elements: first, ecological factors that refer to cultural habits and the availability or legality of gambling in a specific environment; second, circumstantial factors that correspond to negative life events (e.g. trauma) or stressful environments (e.g. pandemic) that are likely to promote psychopathological symptoms from a stress-diathesis perspective (Rende & Plomin, Citation1992: Windle, Citation2010); and third, intra- and interpersonal risk factors. Intrapersonal factors refer to specific biological dimensions and individual differences (e.g. personality traits). Because of the importance of family relationships in the onset of risky (Riesch et al., Citation2010) and addictive behaviors (Waldron et al., Citation2013), we mainly refer here to interpersonal factors related to the close environment of the individual. Notably, these four types of risk factors are in constant interaction (Bronfenbrenner, Citation1979). Moreover, according to the psychological process model of mental disorders (Kinderman & Tai, Citation2007), these risk factors also entertain close relationships with specific cognitive (e.g. dysfunctional cognitions, cognitive biases, or deficits) or affective processes (e.g. emotion regulation strategies).
Figure 1. Adaptation of the psychological model of Kinderman and Tai (Citation2007) based on the Pathways Model. SUD = substance use disorder.
The three patients described herein had access to the information reported in the article and provided written consent for us to describe their case.
1. Behaviorally conditioned pathway
1.1. Characteristics and supporting evidence
Individuals from the first pathway are characterized by specific gambling-related cognitive distortions or beliefs, behavioral conditioning (e.g. associative processes promoting cue reactivity), and the absence of premorbid psychopathology or comorbid symptoms. They are postulated to develop gambling problems because of exposure and continued participation in gambling activities that foster associative learning effects (conditioning) and ‘cognitive distortions regarding the probability of winning, and the nature of randomness and control’ (Nower & Blaszczynski, Citation2017, p. 96). These cognitive distortions are derived from the heuristics defined by Kahneman and Tversky (Citation1972), mainly availability (e.g. illusory correlations or inherent memory bias; see, Fortune & Goodie, Citation2012), representativeness (e.g. overconfidence; see, Koriat et al., Citation1980), or trends in number picking (Haigh, Citation1997; Holtgraves & Skeel, Citation1992; Rogers & Webley, Citation2001). Other cognitive distortions such as the illusion of control (Langer, Citation1975) or near-miss effects (Clark et al., Citation2009) have been established but not directly related to existing heuristics (Goodie & Fortune, Citation2013). Numerous studies have shown the role of cognitive biases or distortions in the development, maintenance, and severity of gambling disorder (e.g. Challet-Bouju et al., Citation2017; Cunningham et al., Citation2014; Devos et al., Citation2020; Labrador et al., Citation2020; Michalczuk et al., Citation2011; Navas et al., Citation2017; Raylu & Oei, Citation2004). Several studies supported the view that problem gambling in some individuals is mainly driven by such cognitive distortions and beliefs (Devos et al., Citation2020; Turner et al., Citation2008), and several standardized approaches to the treatment of problem gambling include cognitive and behavioral techniques that aim to mitigate them (Challet-Bouju et al., Citation2017; Okuda et al., Citation2009).
1.2. Clinical illustration
Franck is a 24-year-old young Caucasian adult university student. He gambles on sport betting (Tennis games). His first bet was a win, which has played a pivotal role in the perpetuation of his betting behaviors: ‘If I lost, I don’t think I would have bet again.’ He does not bet at random: ‘I study the players, their health, and their performance. In short, all the elements that allow me to rank a player. I thought to myself, if I spot the health and mental state of the player, then there’s no reason it shouldn’t go through. And when I lose, I think to myself, I’m out of luck, this player wasn’t supposed to lose.’ After betting at point of sale, he started downloading smartphone apps. After 6 months of controlled gambling, his behavior changed: ‘Until last April, it was holding on and then it all suddenly accelerated. I started betting big amount of money on small odds and no longer low amount of money on big odds.’ Betting money completely altered his relationship to sport and engendered important changes in his fundamental beliefs and cognitive schemata: Until then, I was positive, I was more a winner than a loser even if there were losses that I did not fully understand. For example, the 150th world player who beats the 15th world player. Outside of betting, I would have thought it was great, but when I bet, I just don’t understand that kind of result at all, I find it hard to understand and I don’t accept it. I say to myself, it’s not possible, it cannot be true, it must not be like that … In fact, this is the beauty of the sport and it is part of the sport!”. Playing on his smartphone apps has resulted in an increase in the frequency and amounts of bets: ‘ … And there, I started to be out of control, I no longer bet small amount but I bet minimum 100 euros, and I did a series of bets … Once, I made 13 lost bets in a row and I started to be overdrawn of 1,300 euros on my bank account while I have a monthly purse of 104 euros! So I tried not to play anymore. I found a job in a sports store, and I felt relieved. I said to myself, it’s good, it’s over, it’s behind me … but when I received my first salary, I started again even if I really wanted to quit. I said to myself something very stupid “the next bet, he is certain,” as if the previous one wasn’t!! And there, everything deteriorated again and it was even worse.’
1.3. Symptom-based clinical description
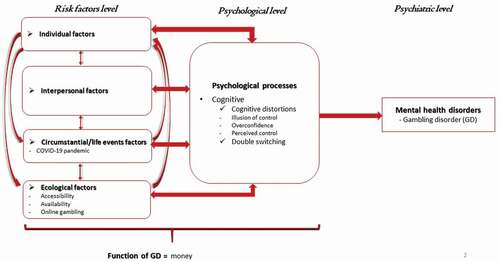
Franck presents with a mild episodic gambling disorder (he endorses four of the nine criteria for gambling disorder according to the fifth edition of the Diagnostic and Statistical Manual for Mental Disorders [DSM-5]; American Psychiatric Association, Citation2013), since it has been more than 12 months without premorbid or other current mental health disorders (see, ). For over a year, he was often preoccupied with gambling (‘I was always thinking about how I was going to bet next time, what will be my next bet, and at the same time, I kept going over what had happened in my previous bets and I was obsessed with it’), and when he started to bet higher amounts of money and lost money, he often bet to chase losses (‘When I lost, it was not normal, and because it was not normal, I absolutely had to redo myself, I had to regain what I should have won’). Franck lied to his relatives, especially his family, to cover up the true extent of his gambling habits (‘I couldn’t tell them, so I was hiding, I was lying about what I was doing when I was spending so much time on my computer’). He also jeopardized educational opportunity (he ruined his second year of undergraduate studies) because of his gambling (‘It took up so much space that I was not able to concentrate more on my classes and homework. It’s clear that my year, I missed it because of sport betting. It became more important than my university education’). There was no evidence of a comorbid psychiatric disorder.
Figure 2. Case of Franck.
1.4. Risk factors and process-based clinical case formulation
Several ecological factors have led Franck to modify his gambling behavior. The accessibility and the availability of online gambling (thanks to smartphone apps) are such that Franck has increased the frequency and the amount of his bets. In addition, convenience, meaning being in a familiar and comfortable environment (at home), reduced his sense of risk and allowed him to engage in more risky behaviors than he had when betting at points of sale (Bonnaire, Citation2012; Griffiths et al., Citation2006).
In the context of the COVID‑19 pandemic, university teaching was no longer provided face to face, but online. It was thus difficult for Franck to stay focused and motivated to study. This situation also challenged his self-control and promoted betting behavior. Boredom and the need for money further increased his gambling behavior, consistent with recent studies conducted during the COVID-19 pandemic showing associations between boredom and both the frequency of gambling (Fluharty et al., Citation2020) and reduced self-control (Boylana et al., Citation2021).
Franck’s gambling behavior is mainly driven by financial reasons, a motive that has frequently been related to problematic gambling patterns (McGrath et al., Citation2010; Schellenberg et al., Citation2016).
Franck is characterized by several irrational beliefs and gambling-related cognitive distortions. First, Franck displays an illusion of control (Langer, Citation1975). He presents with an exaggerated belief about the veracity of his predictions, overestimates his chances of winning, and is convinced that he has control over his bets and their outcomes. As suggested by Ladouceur et al. (Citation1988), even a few wins are able to foster this illusion of control in individuals. Here the initial wins, attributed by Franck to his personal skills and knowledge (about sport), contributed to shaping his overconfidence in predicting outcomes in sport events. The perceived control over the outcome of the game, as well as Franck’s overconfidence in his personal skills, generated less favorable bets (higher stake on lower odds) and thus more gambling-related harm (Goodie, Citation2005).
Betting money was associated with a significant switch in his cognitive state. Ladouceur and Walker (Citation1998) suggested that gamblers’ verbalizations were erroneous during gambling even though they had an accurate understanding that the outcome of the game is determined by chance. This is in line with Sévigny and Ladouceur’s (Citation2003) double switching concept. Individuals with problem gambling could oscillate between two cognitive states of mind: one focused on an objective and rational view of the odds (cold cognition) and the other centered on the activity itself and the related outcomes (hot cognition). For Frank, such emotional betting tended to promote impulsive and automatic behaviors and hinder him from taking into account the factual information that he previously used to consider (e.g. that a lower ranked tennis player can beat a higher ranked tennis player). This cognitive switch is a representative illustration of how emotional arousal linked to betting has a strong impact on beliefs, self-control, and decision making.
2. Emotionally vulnerable pathway
2.1. Characteristics and supporting evidence
Besides the characteristics of Pathway 1 (i.e. availability and accessibility of gambling, operant conditioning effects, and cognitive distortions), gamblers of Pathway 2 display specific premorbid risk factors such as comorbid psychopathology (e.g. anxiety, depression) and emotional (dys)regulation processes (Bonnaire et al., Citation2009; Milosevic & Ledgerwood, Citation2010; Moon et al., Citation2016). For them, gambling has a primary function of coping (with aversive emotional states) through a negative reinforcement process (i.e. it modulates affective states or compensates for unmet psychological needs). Gamblers belonging to this pathway also frequently present poor stress-coping and problem-solving skills, as well as childhood maltreatment.
Scientific evidence supports the existence of an emotionally vulnerable type characterized by emotional instability, comorbid psychopathology, and history of traumatic events (Álvarez-Moya et al., Citation2010; Lane et al., Citation2016; Lotzin et al., Citation2018; Moon et al., Citation2016; Suomi et al., Citation2014; Turner et al., Citation2008). A recent meta-analysis suggests that specific components of emotion dysregulation (e.g. maladaptive cognitive emotion regulation strategies) play a pivotal role in the etiology of gambling disorder (Velotti et al., Citation2021). Other constructs related to emotion dysregulation have also been related to gambling disorder (Bonnaire et al., Citation2013; Estévez et al., Citation2022; Marchetti et al., Citation2019), such as alexithymia (Taylor et al., Citation1997).
2.2. Clinical illustration
Jeanne is a 34-year-old Caucasian woman, married, the mother of a child, and coming to therapy because she ‘gambles too much’ at slot machines. She won during this first gaming experience (3,000 euros for a bet of 50 euros). When she plays, she thinks only about the game and forgets the rest: ‘I have a daughter and I could buy her a toy, but I spend the money. When weFootnote1 gamble, we don’t think about all that, when we gamble, we forget everything.’ Jeanne hides her gambling activity from her relatives. Not talking about it is a way of not addressing the why, a way of not trying to understand: ‘I never wanted to ask myself why I gamble and that’s why we don’t talk about it to others. It would hurt others to think that we have an emotional lack that we fill by playing … I’ve never asked myself the question what it’s for because I don’t want to find out why. And then I would be too ashamed to say it, it’s as if we were saying that we are alcoholics. In addition, they will say to themselves that I am fulfilling something.’ For her, ‘gambling is an antidepressant that does not work.’ Jeanne does not choose her slot machine(s) at random. Jeanne is superstitious, preferring rather isolated slot machines to be quiet and not to have someone behind her who could bring her bad luck.
Jeanne presents suicidal ideations that she links to the losses and debts contracted because of her gambling. Jeanne is also a heavy smoker whose smoking behavior increases when she is gambling. There are several negative life events in Jeanne’s life, one of them being major and easily evoked by her. In a detached and factual way, she recounts, with emotional distance, the suicide of her sister, which occurred 6 years earlier. Jeanne began to gamble excessively shortly after this trauma. However, she does not consciously link gambling and this life event: ‘I don’t know why I started gambling, today I can’t stop and I don’t know why.’ Jeanne’s parents divorced when she was 5 years old. Afterward, she lived with her mother, about whom she speaks very little (‘There’s nothing to say about her, she’s depressed and can’t stop thinking about her’). She describes an absent father, who consumed cocaine heavily and focused on his professional success. She felt like she was abandoned. She describes her childhood as a difficult period during which she felt extremely alone.
2.3. Symptom-based clinical description
According to DSM-5 criteria, Jeanne presents with a persistent severe gambling disorder (see, ). For more than 12 months, she has presented all nine diagnostic criteria for gambling disorder. The loss of freedom and the loss of control over her gambling behavior were also associated with a loss of pleasure. In addition, Jeanne presents with a major recurrent depressive disorder of severe intensity (without psychotic features). She feels sad and experiences feelings of emptiness daily (i.e. depressed mood most of the day); she shows anhedonia (i.e. markedly diminished pleasure) in some activities in which she was previously invested (‘I have more taste for dancing class then I stopped, yet I loved it but there … what’s the point !’), asthenia (i.e. fatigue) and attentional difficulties (i.e. diminished ability to concentrate) (‘I’m tired all the time, everything is an effort for me, whether physically or mentally. Anyway, I’m like a goldfish, I can’t concentrate on anything’), compromised sleep (i.e. insomnia), and recurrent suicidal ideations. Depressive symptoms began during adolescence (‘I started to feel really bad around the age of 20, that’s when I told myself that I was depressed. And since then, it hasn’t didn’t really let me down, except for a few times when I felt better’), but were significantly aggravated following the suicide of her sister.
Figure 3. Case of Jeanne.
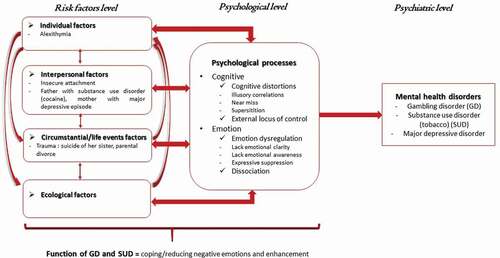
Jeanne also presents a tobacco use disorder. Her tobacco use increased during gambling sessions. The co-occurrence of tobacco use disorder and gambling disorder is high (Jiménez-Murcia et al., Citation2021; McGrath & Barrett, Citation2009), which can partly be explained by the cross-cue reactivity hypothesis (Wulfert et al., Citation2016).
2.4. Risk factors and process-based clinical case formulation
Both of Jeanne’s parents had a history of mental disorders. Her father was diagnosed with a substance use disorder and her mother had experienced major depressive disorder episodes. As shown in several studies on attachment (Di Trani et al., Citation2017), given the familial climate of uncertainty and the nonstable attachment figure of the parents, it can be postulated that Jeanne is characterized by a preoccupied attachment style (i.e. insecure and anxious; see, Bartholomew & Horowitz, Citation1991).
Jeanne shows alexithymic traits. She has difficulties identifying and describing her feelings (‘I don’t know how to answer your question, it’s confusing for me what I feel’), as well as difficulties differentiating feelings from bodily sensations of emotional arousal. When asked about her feelings and emotions, she goes into a detailed description of her physical sensations (‘heart beating, palms sweaty, legs a little less solid’). Likewise, she addresses her physical pain when asked to talk about her relationships with others or her reactions to certain difficult situations. Regarding emotions, her words seem to fall short and Jeanne expresses little or no emotional feelings at all.
For Jeanne, gambling is a way to self-medicate and cope with emotional pain and relieve negative affect linked to previous traumatic life events (e.g. the suicide of her sister, parental divorce; Bonnaire et al., Citation2017; Felsher et al., Citation2010; Lane et al., Citation2016; Lotzin et al., Citation2018; Petry & Steinberg, Citation2005). Gambling maintains anesthesia or avoidance of painful emotions: ‘I go elsewhere in my head, I am no longer myself, I don’t give a damn about everything, even my daughter, once in the casino, it goes beyond the rest.’ Jeanne can thus temporarily or permanently cut herself off from her emotional pain. The positive emotions experienced during gambling is a means of alleviating pain and unbearable states of mind. Gambling behavior promotes a need for stimulation or arousal that allows her to experience positively valenced emotional states. Gambling is both liberating and destructive: ‘It’s my antidepressant and at the same time it’s my depression.’ It functions as refuge, ‘shelter’ against traumatic experiences, and constitutes an attempt to face the difficulties of her existence: ‘We don’t want to face real life in a casino, it’s is an escape from reality. Gambling stops time and buys time. While we play, we forget our problems, we put them aside. And it buys time in the sense that it occupies, it avoids being at home, being bored and thinking about your problems.’ She spends time on the slot machine because this activity is intrinsically worthwhile apart from the money that is lost. Slot machine gambling allows her to modulate, relieve, or escape her painful emotional states (linked to her past) through escapism. Gambling results from a need to cope with painful emotional experiences, a process that has also been found in depressed gamblers (Brown & Coventry, Citation1997; Getty et al., Citation2000).
The fear of hurting those around her and the shame experienced are ways to rationalize her behavior. Not telling others about her gambling problems protects her from processing the reason for gambling: ‘I have never asked myself the question what it is for because I do not want to find out why. And then I would be too ashamed to say it, it’s as if we were saying that we are alcoholics. In addition, they will say that I am fulfilling something.’ This projection mechanism underlines her difficulties and her inability to recognize the function of gambling. The guilt linked to her gambling behaviors seems more accessible and acceptable than that that felt following the suicide of her sister or when her parents divorced.
During the case formulation, several irrational beliefs and cognitive distortions were identified, more specifically illusory correlations. Jeanne mistakenly perceives a causal relationship between unrelated events and believes her personal luck influences her gambling outcomes (see, Petry, Citation2004). This is perfectly illustrated when she says, ‘I earn more with other people’s money,’ but also when she puts her cardigan on backwards: ‘The first time I won, I had my cardigan on backwards and I know it brought me luck so I always put it upside down when I go to the casino.’ Jeanne did not choose her slot machine at random. Her choice is made according to her perceived payback percentage (Coates & Blaszczynski, Citation2013): ‘I know very well which slot machines give the most and that’s how I know where I am going to gamble.’ While gambling, some of her verbalizations became irrational or erroneous; that is, she ignores or even denies randomness, regardless of her initial perceptions of chance as determining the outcome of gambling (Ladouceur et al., Citation1988), highlighting the concept of double switching. Indeed, outside and before gambling, she recognized that slot machines are pure games of chance that do not require any kind of knowledge or skills and that nothing she could do would ever influence the outcome of the slot machine. However, during playing sessions, when she is, for example, faced with ‘near-miss’ events (an unsuccessful outcome proximal to a win; see, Reid, Citation1986), she then feels that ‘it’s coming soon I was almost there,’ which corresponds to a cognitive distortion frequently experienced by slot machine gamblers (Griffiths, Citation1991). Furthermore, she tends to be superstitious. She performs many gestures and rituals with the aim of influencing the outcome of her gambling, and she has charms in her purse. For example, she hides the paylines of the slot machine, convinced that she will have a better chance of winning this way. In line with previous research (Kusyszyn & Rubenstein, Citation1985; Von der Heiden & Egloff, Citation2021), Jeanne seems to be characterized by an external locus of control (the belief that events in one’s life are controlled by factors beyond one’s influence or control).
Jeanne has emotional regulation deficits. She presents a lack of emotional awareness (lack of attention paid to emotional responses) and lack of emotional clarity (difficulty naming the emotion experienced; Gratz & Roemer, Citation2004). The case formulation revealed a link between tobacco use and emotion regulation. Indeed, tobacco appears to be a means of alleviating the internal tension inherent in the expectation of the gambling outcome. Tobacco regulates her sensations, just as gambling regulates her emotions, the commonality being the perceived feeling of control about her emotional state, through confusion between bodily sensations and emotions (Bonnaire et al., Citation2009).
Jeanne tends to be dissociated while gambling (dissociation between emotion and cognition), forgets time and space, and is in a state close to depersonalization that cuts her off from her thoughts and emotions. Jeanne is totally absorbed by the slot machine: ‘The game stops time and buys time. While playing, we forget our problems, we put them aside. When I gamble, I am not there anymore, I am 100% with the slot.’ She is in a flow-like state called ‘dark flow’ that has been linked to gambling disorder and depression (Dixon et al., Citation2018). This state of dissociation is what Jeanne is looking for when playing slot machines. Such dissociation – present in many persons with a gambling disorder (Diskin & Hodgins, Citation1999; Gupta & Derevensky, Citation1998; Kofoed et al., Citation1997; Kuley & Jacobs, Citation1988; Ledgerwood & Petry, Citation2006) – echoes for her the way in which she experienced the suicide of her sister. The emotion has not been sufficiently experienced and thus processed. The cognitive and emotional impact of the traumatic event has been for her strong and painful (‘It was horrible, I have never experienced anything worse’). However, Jeanne shows a severe emotional detachment regarding this event. In that sense, gambling can be conceptualized here as a way to perpetuate this emotional process (i.e. expressive suppression strategy). This dysfunctional emotional regulation strategy of expressive suppression allows her to remain in a ‘daze,’ that is, a state ‘outside’ of reality, whose function is to cope with painful emotional experiences. This coping function of gambling is well established and described in previous literature (Gupta & Derevensky, Citation1998; Jacobs, Citation1988). The occurrence of dissociative symptoms and a history of childhood trauma is frequent in addictive disorders (Craparo et al., Citation2014; Langeland et al., Citation2002; Schafer et al., Citation2010; Somer, Citation2003), including gambling disorder (Imperatori et al., Citation2017). Persons with greater proneness to dissociation are more likely to use gambling as a means of escape from painful emotional experiences (Ledgerwood & Petry, Citation2006). Both dissociation and escape are strategies for coping with painful emotional experiences that involve avoidance of the painful situation (Gupta & Derevensky, Citation1998; Jacobs, Citation1988).
3. Antisocial-impulsivist pathways
3.1. Characteristics and supporting evidence
Individuals from this pathway have been described as the most severe cases of gambling disorder. Their main characteristics include heightened impulsivity traits and antisocial or narcissistic personality features, as well as risk-taking behaviors. They generally present with various behavioral problems unrelated to gambling (e.g. suicidality, irritability, low tolerance for boredom, and criminal behaviors). This pathway is in line with the many studies showing that impulsivity is associated with the development and severity of gambling disorder (Grall-Bronnec et al., Citation2012; Maccallum et al., Citation2007; Mallorquí-Bagué et al., Citation2018; Rogier et al., Citation2020), or with research showing that gambling disorder is associated with poor inhibitory control and decision making (Brevers et al., Citation2013; Ioannidis et al., Citation2019). Several studies have supported the existence of the antisocial-impulsivist pathway (Álvarez-Moya et al., Citation2010; Chamberlain et al., Citation2017; Devos et al., Citation2020; Moon et al., Citation2016; Valleur et al., Citation2015).
3.2. Clinical illustration
Gilles is a 38-year-old man who comes to therapy because he lost a lot of money at online roulette. He comes, not because he has a gambling problem, but because he has lost a lot of money. He has been playing roulette online for 9 months and thinks he has contracted around 300,000 euros in debt with various bank loans and revolving loans. Gilles started gambling because he was already using the logic of ‘chasing loss.’ Indeed, 3 years earlier, he lost a lot a money in stock market speculation. Gilles has an over-indebtedness file in his bag and would like us to support him in this process, but is ambivalent about it. Gilles plays with a calculation system that he developed by studying online roulette outcomes. He spotted repeating gambling sequences: ‘When there is a gambling sequence that goes black, black, red, black, red, red, I know that another gambling sequence will follow which will be, red, black, black, red, red, red, black.’ He cannot stand the fact that his calculation system does not work anymore: ‘It worked really well at the beginning and it’s still surprising this change … it’s not normal.’
Gilles is Eurasian. His father is Asian – born in Vietnam and came to France when communism took power – and his mother is French. His parents separated when he was 12 years old. His father-in-law is a shoe seller, but what Gilles highlights is the illegal side of his activity. Gilles’ father is a restaurant owner but what Gilles immediately emphasizes is the money that his father does not declare in his accounts. Gilles describes his father as a cold man who speaks little or not at all and is extremely severe and rigid. He has specific memories of his father’s verbal and physical abuse. As soon as he became independent, Gilles began to masturbate massively and to consume a lot of pornographic films. He introduces himself as a chartered accountant. In reality, he is a simple accountant and does not have his diploma as a chartered accountant, but he works as such. Gilles was summoned by the Order of Chartered Accountants because he practiced this profession illegally. He instantly created a new one in which he officially claims to be a simple accountant but unofficially to practice the profession of chartered accountant.
He describes a cycle that repeats itself in his romantic relationships. When he begins a relationship, Gilles has an ‘exacerbated and uninhibited’ libido. He has sexual activity several times a day and likes to ‘test things that are out of the ordinary.’ On the other hand, as soon as he begins to have feelings for a woman and as soon as a feeling of love is born, he no longer desires his partner sexually. Sexuality becomes taboo. His sexual needs then lead him to have at first significant masturbatory behavior and then multiple ‘extra-marital’ relationships. He reports that it is the same pattern that occurred with his former partner and generated their separation.
3.3. Symptom-based clinical description
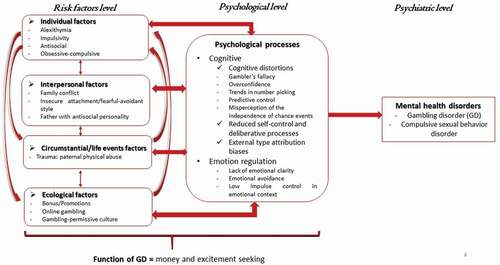
According to the DSM-5, Gilles presents with a severe persistent gambling disorder (see, ) and has endorsed the nine proposed diagnostic criteria for 9 months. In the past, he was involved in stock market speculation in a way that was comparable to his current gambling disorder related to roulette (Granero et al., Citation2012). Roulette appeared for him as a way to repay his debts related to online stock market speculation. Thus, we hypothesized that he has had the diagnostic criteria for gambling disorder for more than 3 years. Gilles also endorses the proposed criteria for compulsive sexual behavior disorder, as defined in the 11th revision of the International Classification of Diseases (Kraus et al., Citation2018). This condition occurred prior to his gambling disorder and there is an alternation between the two in terms of environmental and situational factors. Despite displaying antisocial behaviors, he does not fulfil all criteria to be diagnosed with an antisocial personality disorder.
Figure 4. Case of Gille.
3.4. Risk factors and process-based clinical case formulation
Gilles presents alexithymic characteristics, a trait that might also characterize his father, who appears to be a man who does not express his emotions. Gilles has difficulties identifying and describing his feelings: ‘We do not talk about that in my family, since I was a kid I understood that I is wrong to talk about what I felt, that no one, none of my parents would be there to understand what I felt.’
Gilles is clearly characterized by impulsivity (translated into his gambling behaviors but in professional and affective domains), antisocial personality traits, and disinhibition. When involved in rewarding behaviors (e.g. sexual behaviors, gambling, stock option trading), Gilles tend to lose control and manifest compulsive involvement. Gilles frequently performs illegal acts and he proved unable to adhere to social norms and societal values. Even when confronted with his actions, he does not experience remorse or bring himself to stop illegal activities. Although threatened with judicial sanctions for his illegal activities, it is still inconceivable for him to stop such activities and work ‘as a simple bookkeeper.’ For example, he decided to relocate his professional activity to India in order to ‘pervert the system and earn more money’ and to open a bank account in a ‘tax heaven’ in order to save money for when his over-indebtedness file would be completed (after 8 years, an assessment would be made and it would be possible for his debt to be ‘erased’). In view of the amounts of repayments put in place and his official professional situation, he has calculated that he would repay barely 5% of his debts: ‘It is out of the question that I work more, otherwise I will have to pay more. But my money, it is out of the question for me to give it to the state.’ According to Gilles, his father and his stepfather also presented antisocial behavior. The male figures he was able to identify with are all outside the law, which did not allow Gilles to have a male reference rooted in legality.
The online modality of his gambling was also an important factor that aggravated his loss of control and compulsivity. This observation is consistent with previous research showing that various factors such as promotional activities available from online gambling platforms tend to increase gambling behavior (Hing et al., Citation2014). Moreover, when playing online, Gilles is frequently involved in gambling at several roulette tables simultaneously. Furthermore, he has increased his gambling frequency because of bonus offers (that required matched deposits and gambling before any winnings could be collected). When he started to reduce his online gambling behavior, he began to receive individualized advertisements and promotions that promoted cravings: ‘It was impossible to resist. They sent me bonuses all the time, offers so interesting that I couldn’t resist.’
His high impulsivity is associated with impaired and short-term-based decision making (Kräplin et al., Citation2014; Mallorquí-Bagué et al., Citation2018; Sharman et al., Citation2019). Decision-making deficits encountered in the antisocial-impulsivist pathway have been related to a reduction in self-control abilities and deliberative (controlled) processes (Schiebener et al., Citation2014).
Gilles also displays some characteristics of obsessive-compulsive personality: He is a perfectionist and meticulous and has a concern for order (material and moral in some respects). Previous research has shown that a subgroup of individuals with problem gambling is characterized by obsessive-compulsive personality traits (Dowling et al., Citation2015; Petry et al., Citation2005). In an attempt to regain control, Gilles displays selective attention to trivial details, such as how to close the kitchen doors: ‘My roommate, I showed him how to close the doors properly and he keeps closing them badly … I think that I will have to fire him.’ He finds it difficult to trust others at the professional level because he thinks they do not perform as well as he does.
His two parental attachment figures appear to be dysfunctional. Gilles grew up with a father who physically abused him regularly and a mother who could not protect him from the violence she witnessed. Childhood maltreatment is prevalent in gambling disorder (Felsher et al., Citation2010), and physical or emotional abuse is usually associated with an intermediate severity of gambling disorder symptoms (Lotzin et al., Citation2018). His adverse childhood experiences probably contributed to the development of a ‘fearful attachment style’ (Bartholomew, Citation1990), a type of dysfunctional attachment that has been linked to problem gambling (Di Trani et al., Citation2017): ‘I never knew what to expect with my father, I was always afraid that he would unwind on me and freak out.’ Before parental divorce, family conflicts were high: ‘There were very often conflicts between my parents and it was not uncommon for them to come to blows.’ Furthermore, comparable to what is found in adults with avoidant attachment style in romantic relationships (Brassard et al., Citation2007), Gilles uses a strategy for limiting intimacy in sexual relationships: avoidance of sexual fantasies about one’s partner. Indeed, avoidant attachment is associated with trying not to become overly intimate with, or reliant upon, a partner (by avoiding sexual intercourse altogether or engaging only in casual sex), which can also explain the preference for solitary masturbation (Bogaert & Sadava, Citation2002).
One of Gilles’ main motives for gambling is earning money, but he is also looking for excitement and pleasure. Gambling is a risk-taking activity that maintains a high level of arousal. Excitement-seeking gamblers are more likely than non-excitement-seeking gamblers to demonstrate problems in multiple areas characterized by impaired impulse control (Pantalon et al., Citation2008).
Gilles also presents with several distorted cognitions: the gambler’s fallacy, overconfidence, and trends in number picking (Tversky & Kahneman, Citation1971). Gilles is convinced that certain sequences of color in roulette occur and that he can predict the results (i.e. predictive control), which highlights his misperception of the independence of chance events (Hardoon et al., Citation2001; Ladouceur et al., Citation1996). Overconfidence, that is, his tendency to display a confidence that is not justified by his actual abilities (Goodie, Citation2005; Koriat et al., Citation1980; Lakey et al., Citation2007), led him to be convinced that he is able to predict the outcome in a game of chance, which leads him to wager a large amount of money. When he loses, he tends to display external-type attribution biases (Ohtsuka & Hyam, Citation2003), implying that he does not feel responsible for the losses.
Gilles has a marked tendency toward intellectualization, which allows him to put his emotions away. We postulate that this process of emotional avoidance might be a consequence of the necessity to deal with paternal violence (experienced as traumatic) during his childhood: ‘It was so unfair and incomprehensible to me when he hit me like that. In those moments, it’s as if I was above the stage. I was so mad at him but at the same time too small to defend myself.’ Currently, any situation that reminds him of the injustice experienced in the face of his father’s behavior causes him to be emotionally overwhelmed. He experiences overwhelming anger, leading him to be physically violent (i.e. low impulse control in emotional context). Nevertheless, it is difficult for him to be conscious and mindful of what he feels (i.e. lack of emotional awareness): ‘It is very difficult for me to understand what I feel, I just know that I want to hit the guy.’
Finally, it is worth noting that cultural aspects might have affected Gilles’s motivation to gamble (Oei & Raylu, Citation2010), as previous research shown that the combination of gambling availability and a gambling-permissive culture contribute to promote problem gambling in Asians living in western countries (Kim, Citation2012; Kim et al., Citation2012).”
Implications and conclusion
The three cases depicted here emphasized both the similarities and the uniqueness of the three distinct pathways theorized by Blaszczynski and Nower (Citation2002). In the three clinical situations described, ecological factors, erroneous cognitions, or the effects of operant conditioning (linked to early wins and repeated small wins) were present, which is in line with the view that the characteristics of Pathway 1 are shared between Pathways 2 and 3. The case used to depict Pathway 3 presented with specific personality traits, such as impulsivity or antisocial traits, although he also shares with Pathway 2 many similarities in terms of psychological processes and motives underlying gambling. In that sense, and although no generalization can be made from the analysis of selected clinical cases, the two cases retained to depict Pathways 2 and 3 are well aligned with the initial model of Blaszczynski and Nower (Citation2002), in which Pathway 3 is conceptualized as a subtype of Pathway 2, but less with the revised model in which Pathways 2 and 3 are viewed as separate subtypes (Nower et al., Citation2022). Furthermore, as gambling participation and clinical presentation varies as a function of race and ethnicity (Alegría et al., Citation2009; Barry et al., Citation2011; Chamberlain & Grant, Citation2020; Williams et al., Citation2021), more attention is needed to include diverse racial/ethnic background in future problem gambling research capitalizing on clinical cases depiction. Indeed, taking into account these aspects is important to design culturally effective gambling treatment (Kim, Citation2012).
What can also be observed from the analysis proposed in this paper is that the PM mixes different levels of analyses (risk factors, psychological processes, and psychiatric symptoms), which is likely to complicate case conceptualization and treatment elaboration from a clinical perspective. Considering these three levels of analysis differentially is indeed crucial for designing sound and individualized psychological interventions (e.g. specific techniques, attitudes, or settings used by the therapist).
Indeed, considering risk factors (in which the therapist does not intervene directly) is relevant for several reasons: (1) to determine which psychotherapeutic framework or attitudes are adapted for a specific case (e.g. taking into account interpersonal factors might inform about the relevance of using a family therapy setting, whereas taking into account individual factors such as personality makes it possible to determine the level of directness to be used in sessions; see, Beutler & Harwood, Citation2000; Kazdin, Citation2008); (2) to identify related psychological processes (e.g. relevant psychological processes in the context of borderline personality might be dysfunctional emotion regulation strategies or impaired impulse control); and (3) to select specific harm reduction techniques based on relevant ecological factors (e.g. relying on online gambling sites tools available to regulate or limit gambling involvement).
As evidence-based psychological interventions typically target psychological processes (e.g. dysfunctional emotion regulation strategies, cognitive deficits) and not risk factors per se (e.g. personality traits), it is crucial to apply process-based analysis when conceptualizing cases and designing treatment (Billieux et al., Citation2015; Dudley et al., Citation2011; Philippot et al., Citation2019). An understanding of the specific psychological processes implicated in the onset and maintenance of the disorder helps tailor treatment depending on the specific psychological processes incriminated, which, according to the PM, are different for each problem gambling subtype. For the clinical cases depicted here, individuals with gambling problems from each pathway would benefit from treatment that aimed to mitigate or modify gambling-related dysfunctional cognitions (Challet-Bouju et al., Citation2017; Petry et al., Citation2006), along with behavioral interventions that aimed to identify and cope with environmental gambling triggers (Petry et al., Citation2017). In contrast, only Gilles (the case used to depict Pathway 3) would benefit from an intervention that targeted impulse control, which could, for example, consist of helping him to pursue specific goals, improve problem-solving skills, and optimize self-control and inhibitory control (e.g. Friese et al., Citation2011; Gollwitzer, Citation1999). Finally, individuals with gambling problems from Pathways 2 and 3 (i.e. Jeanne and Gilles in the current paper) would benefit from interventions that targeted improvement of emotion regulation and/or emotional acceptance (e.g. Barlow et al., Citation2017; Elliott et al., Citation2004; Greenberg et al., Citation2019; Timulak & Koegh, Citation2021). Applying a process-based approach thus allows for individualizing treatment in order to omit parts of standardized treatment that would not necessarily be relevant for a specific subtype of gambler. For example, the part of standardized treatment for gambling disorder that focuses on improving impulse control would not be useful for individuals with gambling problems from Pathways 1 and 2.
The psychiatric level is generally used to identify standardized treatment that targets specific syndromes (e.g. gambling disorder, depressive disorder). Nevertheless, we relied here on a psychological model that conceptualizes psychiatric symptoms as a consequence of impaired or disturbed psychological processes (Kinderman, Citation2005). Symptoms are those things that bring patients to look for treatment, but efficient treatments are those that target the processes underlying these symptoms. Nonetheless, similar symptoms might be driven by heterogeneous etiopathological processes and thus have different functions for individuals displaying them (Ramnerö & Törneke, Citation2008). As a consequence, designing treatments based on psychiatric diagnosis could risk overlooking the various idiosyncratic psychological processes underlying presenting symptoms, which might ultimately compromise the relevance and efficacy of treatment (Billieux et al., Citation2015). To our view, one of the main advantages of the PM is that it illuminates how different etiological mechanisms (e.g. psychological processes), not necessarily shared among gamblers, explain impaired control over gambling behavior.
Thus, we believe it important for people involved in the psychological treatment of gambling disorder and capitalizing on the well-known PM to be mindful that this model includes many variables that do not necessarily reflect a similar level of analysis and are thus not equivalent in terms of their role in the etiology versus the treatment of gambling disorder.
Ethics approval
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. All patients gave written consent stating their agreement to the use of data collected as part of their treatment for their gambling disorder. They have all read the parts of the article concerning them and have therefore given their informed consent. In the article, all relevant ethical safeguards have been met in relation to the protection of subjects. The names and sociodemographic characteristics of the patients were modified to guarantee anonymity, and we have voluntarily restricted the case description to aspects that are relevant for the purposes of the current article.
Funding sources
No funding sources were declared by the authors in relation to this manuscript.
Constraints on publishing
No constraints on publishing were declared by the authors in relation to this manuscript.
Competing interests
No competing interests were declared by the authors in relation to this manuscript.
Preregistration statement
No preregistration was declared by the authors in relation to this manuscript.
Supplemental Material
Download MS Word (50.5 KB)Data availability statement
No data set was declared by the authors in relation to this manuscript.
Supplementary material
Supplemental data for this article can be accessed here
Additional information
Notes on contributors
Céline Bonnaire
Dr. Celine Bonnaire is a PhD of clinical psychology and psychopathology. Her areas of research include: 1) Psychological (intra and interpersonal) factors involved in the etiology of addictive behaviors (especially gambling and gaming) with a particular focus on personality, identity and emotional processes; 2) Effectiveness of psychotherapeutic and preventive interventions in individuals with addictive behaviors.
Joël Billieux
Dr. Joël Billieux is an Associate Professor of clinical psychology, psychopathology, and psychological assessment at the University of Lausanne, Switzerland. His areas of research include the psychological factors involved in the etiology of addictive behaviors, the conceptualization and diagnosis of behavioral addictions, and the effects of emerging technologies on human behaviour.
Notes
1. When Jeanne says ‘we,’ this refers to the general group of ‘gamblers.’ We interpret this as a distancing technique.
References
- Alegría, A., Petry, N., Hasin, D., Liu, S., Grant, B., & Blanco, C. (2009). Disordered gambling among racial and ethnic groups in the US: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. CNS Spectrums, 14(3), 132–143. https://doi.org/10.1017/S1092852900020113
- Álvarez-Moya, E. M., Jiménez-Murcia, S., Aymamí, M. N., Gómez-Peña, M., Granero, R., Santamaría, J., Menchón, J. M., & Fernández-Aranda, F. (2010). Subtyping study of a pathological gamblers sample. Canadian Journal of Psychiatry, 55(8), 498–506. https://doi.org/10.1177/070674371005500804
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
- Barlow, D. H., Farchione, T. J., Bullis, J. R., Gallagher, M., Murray-Latin, H., Sauer‐Zavala, S., Bentley, K., Thompson-Hollands, J., Conklin, L. R., Boswell, J. F., Ametaj, A. A., Carl, J., Boettcher, H. T., & Cassiello-Robbins, C. F. (2017). The unified protocol for transdiagnostic treatment of emotional disorders compared with diagnosis-specific protocols for anxiety disorders: A randomized clinical trial. JAMA Psychiatry, 74(9), 875–884. https://doi.org/10.1001/jamapsychiatry.2017.2164
- Barry, D. T., Stefanovics, E. A., Desai, R. A., & Potenza, M. N. (2011). Differences in the associations between gambling problem severity and psychiatric disorders among black and white adults: Findings from the National Epidemiologic Survey on Alcohol and Related Conditions. American Journal on Addictions, 20(1), 69–77. https://doi.org/10.1111/j.1521-0391.2010.00098.x
- Bartholomew, K. (1990). Avoidance of intimacy: An attachment perspective. Journal of Social and Personal Relationships, 7(2), 147–178. https://doi.org/10.1177/0265407590072001
- Bartholomew, K., & Horowitz, L. M. (1991). Attachment styles among young adults: A test of a four-category model. Journal of Personality and Social Psychology, 61(2), 226–244. https://doi.org/10.1037/0022-3514.61.2.226
- Beutler, L. E., & Harwood, T. (2000). Prescriptive psychotherapy: A practical guide to systematic treatment selection. Oxford University Press.
- Billieux, J., Philippot, P., Schmid, C., Maurage, P., de Mol, J., & Van der Linden, M. (2015). Is dysfunctional use of the mobile phone a behavioural addiction? Confronting symptom-based versus process-based approaches. Clinical Psychology and Psychotherapy, 22(5), 460–468. https://doi.org/10.1002/cpp.1910
- Blaszczynski, A., & Nower, L. (2002). A pathways model of problem and pathological gambling. Addiction, 97(5), 487–499. https://doi.org/10.1046/j.1360-0443.2002.00015.x
- Bogaert, A. F., & Sadava, S. (2002). Adult attachment and sexual behavior. Personal Relationships, 9(2), 191–204. https://doi.org/10.1111/1475-6811.00012
- Bonnaire, C., Bungener, C., & Varescon, I. (2009). Subtypes of French pathological gamblers: Comparison of sensation seeking, alexithymia and depression scores. Journal of Gambling Studies, 28(4), 455–471. http://dx.doi.org/10.1007/s10899-009-9142-z
- Bonnaire, C. (2012). Jeux de hasard et d’argent sur Internet: Quels risques? L’Encéphale, 38(1), 42–49. https://doi.org/10.1016/j.encep.2011.01.014
- Bonnaire, C., Bungener, C., & Varescon, I. (2013). Alexithymia in pathological gambling: A risk factor for all gamblers? Journal of Gambling Studies, 29(1), 83–96. http://dx.doi.org/10.1007/s10899-012-9297-x
- Bonnaire, C., Kovess-Masfety, V., Guignard, R., Richard, J. B., du Roscoät, E., & Beck, F. (2017). Gambling type, substance abuse, health and psychosocial correlates of male and female problem gamblers in a nationally representative French sample. Journal of Gambling Studies, 33(2), 343–369. http://dx.doi.org/10.1007/s10899-016-9628-4
- Boylana, J., Selib, P., Scholera, A. A., & Danckert, J. (2021). Boredom in the COVID-19 pandemic: Trait boredom proneness, the desire to act, and rule-breaking. Personality and Individual Differences, 171. 110387. https://doi.org/10.1016/j.paid.2020.110387
- Brassard, A., Shaver, P. R., & Lussier, Y. (2007). Attachment, sexual experience, and sexual pressure in romantic relationships: A dyadic approach. Personal Relationships, 14(3), 475–493. https://doi.org/10.1111/j.1475-6811.2007.00166.x
- Brevers, D., Bechara, A., Cleeremans, A., & Noël, X. (2013). Iowa Gambling Task (IGT): Twenty years after – Gambling disorder and IGT. Frontiers in Psychology, 4, 665 . https://doi.org/10.3389/fpsyg.2013.00665
- Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design. Harvard University Press.
- Brown, S., & Coventry, L. (1997). Queen of hearts: The needs of women with gambling problems. Financial and Consumer Rights Council.
- Challet-Bouju, G., Bruneau, M., IGNACE Group, Victorri-Vigneau, C., & Grall-Bronnec. (2017). Cognitive remediation interventions for gambling disorder: A systematic review. Frontiers in Psychology, 8, 1961 . https://doi.org/10.3389/fpsyg.2017.01961
- Chamberlain, S. R., Stochl, J., Redden, S. A., Odlaug, B. L., & Grant, J. E. (2017). Latent class analysis of gambling subtypes and impulsive/compulsive associations: Time to rethink diagnostic boundaries for gambling disorder? Addictive Behaviors, 72, 79–85. https://doi.org/10.1016/j.addbeh.2017.03.020
- Chamberlain, S. R., & Grant, J. E. (2020). Racial-ethnic differences in impulsivity and compulsivity in recreational gambling. Comprehensive Psychiatry, 97, 152153. https://doi.org/10.1016/j.comppsych.2019.152153
- Clark, L., Lawrence, A. J., Astley-Jones, F., & Gray, N. (2009). Gambling near-misses enhance motivation to gamble and recruit win-related brain circuitry. Neuron, 61(3), 481–490. https://doi.org/10.1016/j.neuron.2008.12.031
- Coates, E., & Blaszczynski, A. (2013). An analysis of switching and nonswitching slot machine player behaviour. Journal of Gambling Studies, 29(4), 31–645. http://dx.doi.org/10.1007/s10899-012-9329-6
- Craparo, G., Ardino, V., Gori, A., & Caretti, V. (2014). The relationships between early trauma, dissociation, and alexithymia in alcohol addiction. Psychiatry Investigation, 11(3), 330–335. http://dx.doi.org/10.4306/pi.2014.11.3.330
- Cunningham, J. A., Hodgins, D. C., & Toneatto, T. (2014). Relating severity of gambling to cognitive distortions in a representative sample of problem gamblers. Journal of Gambling Issues, 29(29), 1–6. https://doi.org/10.4309/jgi.2014.29.2
- Delfabbro, P., & King, D. L. (2022). Conceptual and methodological issues in pathways model research. International Gambling Studies, . Advance online publication. https://doi.org/10.1080/14459795.2021.2003843
- Devos, G., Clark, L., Bowden-Jones, H., Grall-Bronnec, M., Challet-Bouju, G., Khazaal, Y., Maurage, P., & Billieux, J. (2020). The joint role of impulsivity and distorted cognitions in recreational and problem gambling: A cluster analytic approach. Journal of Affective Disorders, 260, 473–482. https://doi.org/10.1016/j.jad.2019.08.096
- Di Trani, M., Renzi, A., Vari, C., Zavattini, G. C., & Solano, L. (2017). Gambling disorder and affect regulation: The role of alexithymia and attachment style. Journal of Gambling Studies, 33(2), 649–659. https://doi.org/10.1007/s10899-016-9637-3
- Diskin, K. M., & Hodgins, D. C. (1999). Narrowing of attention and dissociation in pathological video lottery gamblers. Journal of Gambling Studies, 15(1), 17–28. https://doi.org/10.1023/A:1023062912062
- Dixon, M. J., Stange, M., Larche, C. J., Graydon, C., Fugelsang, J. A., & Harrigan, K. A. (2018). Dark flow, depression and multiline slot machine play. Journal of Gambling Studies, 34(1), 73–84. https://doi.org/10.1007/s10899-017-9695-1
- Dowling, N. A., Cowlishaw, S., Jackson, A. C., Merkouris, S. S., Francis, K. L., & Christensen, D. R. (2015). The prevalence of comorbid personality disorders in treatment-seeking problem gamblers: A systematic review and meta-analysis. Journal of Personality Disorders, 29(6), 735–754. https://doi.org/10.1521/pedi_2014_28_168
- Dudley, R., Kuyken, W., & Padesky, C. A. (2011). Disorder specific and trans-diagnostic case conceptualisation. Clinical Psychology Review, 31(2), 213–224. https://doi.org/10.1016/j.cpr.2010.07.005
- Elliott, R., Watson, J. C., Goldman, R. N., & Greenberg, L. S. (2004). Learning emotion-focused therapy. American Psychological Association.
- Engel, G. L. (1980). The clinical application of the biopsychosocial model. American Journal of Psychiatry, 137(5), 535–544. https://doi.org/10.1176/ajp.137.5.535
- Engel, G. L. (1997). From biomedical to biopsychosocial: Being specific in the human domain. Psychosomatics, 38(6), 521–528. https://doi.org/10.1016/S0033-3182(97)71396-3
- Estévez, A., Jauregui, P., Macía, L., & Martín-Pérez, C. (2022). Alexithymia and emotion regulation strategies in adolescent gamblers with and without at-risk profiles. Journal of Gambling Studies 38 (1), 15–29 . . https://doi.org/10.1007/s10899-021-10057-8
- Felsher, J. R., Derevensky, J. L., & Gupta, R. (2010). Young adults with gambling problems: The impact of childhood maltreatment. International Journal of Mental Health and Addiction, 8(4), 545–556. https://doi.org/10.1007/s11469-009-9230-4
- Fluharty, M., Paul, E., & Fancourt, D. (2020). Predictors and patterns of gambling behaviour across the COVID-19 lockdown: Findings from a UK cohort study. PsyArXiv. https://doi.org/10.31234/osf.io/8qthw
- Fortune, E. E., & Goodie, A. S. (2012). Cognitive distortions as a component and treatment focus of pathological gambling: A review. Psychology of Addictive Behaviors, 26(2), 298–310. https://doi.org/10.1037/a0026422
- Friese, M., Hofmann, W., & Wiers, R. W. (2011). On taming horses and strengthening riders: Recent developments in research on interventions to improve self-control in health behaviors. Self and Identity, 10(3), 336–351. https://doi.org/10.1080/15298868.2010.536417
- Getty, H. A., Watson, J., & Frisch, G. R. (2000). A comparison of depression and styles of coping in male and female GA members and controls. Journal of Gambling Studies, 16(4), 377–391. http://dx.doi.org/10.1023/A:1009480106531
- Gollwitzer, P. M. (1999). Implementation intentions: Strong effects of simple plans. American Psychologist, 54(7), 493–503. https://doi.org/10.1037/0003-066X.54.7.493
- Goodie, A. S. (2005). The role of perceived control and overconfidence in pathological gambling. Journal of Gambling Studies, 21(4), 481–502. http://dx.doi.org/10.1007/s10899-005-5559-1
- Goodie, A. S., & Fortune, E. E. (2013). Measuring cognitive distortions in pathological gambling: Review and meta-analyses. Psychology of Addictive Behaviors, 27(3), 730–743. https://doi.org/10.1037/a0031892
- Grall-Bronnec, M., Wainstein, L., Feuillet, F., Bouju, G., Rocher, B., Vénisse, J. L., & Sébille-Rivain, V. (2012). Clinical profiles as a function of level and type of impulsivity in a sample group of at-risk and pathological gamblers seeking treatment. Journal of Gambling Studies, 28(2), 239–252. https://doi.org/10.1007/s10899-011-9258-9
- Granero, R., Tárrega, S., Fernández-Aranda, F., Aymamí, N., Gómez-Peña, M., Moragas, L., Custal, N., Orekhova, L., Savvidou, L. G., Menchón, J. M., & Jiménez-Murcia, S. (2012). Gambling on the stock market: An unexplored issue. Comprehensive Psychiatry, 53(6), 666–673. http://dx.doi.org/10.1016/j.comppsych.2011.12.004
- Gratz, K. L., & Roemer, L. (2004). Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the Difficulties in Emotion Regulation Scale. Journal of Psychopathological Behavior Assessment, 26(1), 41–54. https://doi.org/10.1007/s10862-008-9102-4
- Greenberg, L. S., Malberg, N. T., & Tompkins, M. A. (2019). Working with emotion in psychodynamic, cognitive-behavior, and emotion-focused psychotherapy. American Psychological Association.
- Griffiths, M. D. (1991). The psychobiology of the near miss in fruit machine gambling. Journal of Psychology, 125(3), 347–357. https://doi.org/10.1080/00223980.1991.10543298
- Griffiths, M. D., Parke, A., Wood, R. T. A., & Parke, J. (2006). Internet gambling: An overview of psychosocial impacts. UNLV Gaming Research & Review Journal, 10(1), 27–39. https://digitalscholarship.unlv.edu/grrj/vol10/iss1/4
- Gupta, R., & Derevensky, J. L. (1998). An empirical examination of Jacobs’ general theory of addictions: Do adolescent gamblers fit the theory? Journal of Gambling Studies, 14(1), 17–49. https://doi.org/10.1023/A:1023046509031
- Haigh, J. (1997). The statistics of the national lottery. Journal of the Royal Statistical Society, Series A, Statistics in Society, 160(2), 187–206. https://doi.org/10.1111/1467-985X.00056
- Hardoon, K. K., Baboushkin, H. R., Derevensky, J. L., & Gupta, R. (2001). Underlying cognitions in the selection of lottery tickets. Journal of Clinical Psychology, 57(6), 749–763. https://doi.org/10.1002/jclp.1047
- Hing, N., Cherney, L., Blaszczynski, A., Gainsbury, S. M., & Lubman, D. I. (2014). Do advertising and promotions for online gambling increase gambling consumption? An exploratory study. International Gambling Studies, 14(3), 394–409. https://doi.org/10.1080/14459795.2014.903989
- Holtgraves, T., & Skeel, J. (1992). Cognitive biases in playing the lottery: Estimating the odds and choosing the numbers. Journal of Applied Social Psychology, 22(12), 934–952. https://doi.org/10.1111/j.1559-1816.1992.tb00935.x
- Imperatori, C., Innamorati, M., Saverio Bersani, F., Imbimbo, F., Pompili, M., Contardi, A., & Farina, B. (2017). The association among childhood trauma, pathological dissociation and gambling severity in casino gamblers. Clinical Psychology and Psychotherapy, 24(1), 203–211. http://dx.doi.org/10.1002/cpp.1997
- Ioannidis, K., Hook, R., Wickham, K., Grant, J. E., & Chamberlain, S. R. (2019). Impulsivity in Gambling Disorder and problem gambling: A meta-analysis. Neuropsychopharmacology, 44(8), 1354–1361. https://doi.org/10.1038/s41386-019-0393-9
- Jacobs, D. F. (1988). Evidence for a common dissociative-like reaction among addicts. Journal of Gambling Behavior, 4(1), 27–37. https://doi.org/10.1007/BF01043526
- Jiménez-Murcia, S., Giménez, M., Granero, R., Masuet-Aumatell, C., Ramón, J. M., Agüero, F., Morchón, S., Moragas, L., Baenas, I., Del Pino-Gutiérrez, A., Codina, E., Valenciano-Mendoza, E., Mora-Maltas, B., Valero-Solís, S., Etxandi, M., Guillén-Guzmán, E., Menchón, J. M., & Fernández-Aranda, F. (2021). Gambling disorder seeking treatment patients and tobacco use in relation to clinical profiles. Addictive Behaviors, 114, 106723. https://doi.org/10.1016/j.addbeh.2020.106723
- Kahneman, D., & Tversky, A. (1972). Subjective probability: A judgment of representativeness. Cognitive Psychology, 3(3), 430–454. https://doi.org/10.1016/0010-0285(72)90016-3
- Kazdin, A. (2008). Evidence-based treatment and practice: New opportunities to bridge clinical research and practice, enhance the knowledge base, and improve patient care. American Psychologist, 63(3), 146–159. https://doi.org/10.1037/0003-066X.63.3.146
- Kim, W. (2012). Acculturation and gambling in Asian Americans: When culture meets availability. International Gambling Studies, 12(1), 69–88. https://doi.org/10.1080/14459795.2011.616908
- Kim, W., Kim, I., & Nochajski, T. H. (2012). Predictors of gambling behaviors in Filipino Americans living in Honolulu or San Francisco. Journal of Gambling Studies, 28(2), 297–314. https://doi.org/10.1007/s10899-011-9248-y
- Kinderman, P. (2005). A psychological model of mental disorder. Harvard Review of Psychiatry, 13(4), 206–217. https://doi.org/10.1080/10673220500243349
- Kinderman, P., & Tai, S. (2007). Empirically grounded clinical interventions: Clinical implications of a psychological model of mental disorder. Behavioural and Cognitive Psychotherapy, 35(1), 1–14. https://doi.org/10.1017/S1352465806003274
- Kofoed, L., Morgan, T. J., Buchkoski, J., & Carr, R. (1997). Dissociative Experience Scale and MMPI-2 scores in video poker gamblers, other gamblers, and alcoholic controls. Journal of Nervous and Mental Disease, 185(1), 58–60. https://doi.org/10.1097/00005053-199701000-00011
- Koriat, A., Lichtenstein, S., & Fischhoff, B. (1980). Reasons for confidence. Journal of Experimental Psychology: Human Learning and Memory, 6(2), 107–118. https://doi.org/10.1037/0278-7393.6.2.107
- Kräplin, A., Dshemuchadse, M., Behrendt, S., Scherbaum, S., Goschke, T., & Bühringer, G. (2014). Dysfunctional decision-making in pathological gambling: Pattern specificity and the role of impulsivity. Psychiatry Research, 215(3), 675–682. https://doi.org/10.1016/j.psychres.2013.12.041
- Kraus, S. W., Krueger, R. B., Briken, P., First, M. B., Stein, D. J., Kaplan, M. S., Voon, V., Abdo, C. H. N., Grant, J. E., Atalla, E., & Reed, G. M. (2018). Compulsive sexual behavior disorder in the ICD-11. World Psychiatry, 17(1), 109–110. https://doi.org/10.1002/wps.20499
- Kuley, N., & Jacobs, D. F. (1988). The relationship between dissociative-like experiences and sensation seeking among social and problem gamblers. Journal of Gambling Behavior, 4(3), 197–207. https://doi.org/10.1007/BF01018332
- Kurilla, A. (2021). Is subtyping of gamblers based on the Pathways Model of problem and disordered gambling valid? A systematic review. Journal of Gambling Studies, 37(3), 983–1006. https://doi.org/10.1007/s10899-020-09995-6
- Kusyszyn, I., & Rubenstein, L. (1985). Locus of control and race track betting behaviors: A preliminary investigation. Journal of Gambling Studies, 1(2), 106–110. https://doi.org/10.1007/BF01019863
- Labrador, M., Labrador, F. J., Crespo, M., Echeburúa, E., & Becoña, E. (2020). Cognitive distortions in gamblers and non-gamblers of a representative Spanish sample. Journal of Gambling Studies, 36(1), 207–222. https://doi.org/10.1007/s10899-019-09870-z
- Ladouceur, R., Gaboury, A., Dumont, M., & Rochette, P. (1988). Gambling: Relationship between the frequency of wins and irrational thinking. Journal of Psychology, 122(4), 409–414. https://doi.org/10.1080/00223980.1988.9915527
- Ladouceur, R., Dubé, D., Giroux, I., Legendre, N., & Gaudet, C. (1996). Cognitive biases and playing behavior on American roulette and the 6/49 lottery [Unpublished manuscript]. Université de Laval.
- Ladouceur, R., & Walker, M. (1998). The cognitive approach to understanding and treating pathological gambling. In A. S. Bellack & M. Hersen (Eds.), Comprehensive clinical psychology (pp. 588–601). Pergamon.
- Lakey, C. E., Goodie, A. S., Lance, C. E., Stinchfield, R., & Winters, K. C. (2007). Examining DSM-IV criteria in gambling pathology: Psychometric properties and evidence from cognitive biases. Journal of Gambling Studies, 23(4), 479–498. https://doi.org/10.1007/s10899-007-9063-7
- Lane, W., Sacco, P., Downton, K., Ludeman, E., Levy, L., & Tracy, J. K. (2016). Child maltreatment and problem gambling: A systematic review. Child Abuse & Neglect, 58, 24–38. https://doi.org/10.1016/j.chiabu.2016.06.003
- Langeland, W., Draijer, N., & van den Brink, W. (2002). Trauma and dissociation in treatment-seeking alcoholics: Towards a resolution of inconsistent findings. Comprehensive Psychiatry, 43(3), 195–203. https://doi.org/10.1053/comp.2002.32350
- Langer, E. J. (1975). The illusion of control. Journal of Personality and Social Psychology, 32(2), 311–328. https://doi.org/10.1037/0022-3514.32.2.311
- Ledgerwood, D. M., & Petry, N. M. (2006). Psychological experience of gambling and subtypes of pathological gamblers. Psychiatry Research, 144(1), 17–27. https://doi.org/10.1016/j.psychres.2005.08.017
- Lotzin, A., Ulas, M., Buth, S., Milin, S., Kalke, J., & Schäfer, I. (2018). Profiles of childhood adversities in pathological gamblers—A latent class analysis. Addictive Behaviors, 81, 60–69. https://doi.org/10.1016/j.addbeh.2018.01.031
- Maccallum, F., Blaszczynski, A., Ladouceur, R., & Nower, L. (2007). Functional and dysfunctional impulsivity in pathological gambling. Personality and Individual Differences, 43(7), 1829–1838. https://doi.org/10.1016/j.paid.2007.06.002
- Mallorquí-Bagué, N., Tolosa-Sola, I., Fernández-Aranda, F., Granero, R., Fagundo, A. B., Lozano-Madrid, M., Mestre-Bach, G., Gómez-Peña, M., Aymamí, N., Borrás-González, I., Sánchez-González, J., Baño, M., Del Pino-Gutiérrez, A., Menchón, J. M., & Jiménez-Murcia, S. (2018). Cognitive deficits in executive functions and decision-making impairments cluster gambling disorder sub-types. Journal of Gambling Studies, 34(1), 209–223. https://doi.org/10.1007/s10899-017-9724-0
- Marchetti, D., Verrocchio, M. C., & Porcelli, P. (2019). Gambling problem and alexithymia: A systematic review. Brain Sciences, 9(191), 1–16. https://doi.org/10.3390/brainsci9080191
- McGrath, D. S., & Barrett, S. P. (2009). The comorbidity of tobacco smoking and gambling: A review of the literature. Drug and Alcohol Review, 28(6), 676–681. https://doi.org/10.1111/j.1465-3362.2009.00097.x
- McGrath, D. S., Stewart, S. H., Klein, R. M., & Barrett, S. P. (2010). Self-generated motives for gambling in two population-based samples of gamblers. International Gambling Studies, 10(2), 117–138. https://doi.org/10.1080/14459795.2010.499915
- Mestre-Bach, G., Granero, R., Fernández-Aranda, F., Potenza, M. N., & Jiménez-Murcia, S. (2022). Exploring the pathways model in a sample of patients with gambling disorder. International Gambling Studies. Advance online publication. https://doi.org/10.1080/14459795.2022.2029527
- Michalczuk, R., Bowden-Jones, H., Verdejo-Garcia, A., & Clark, L. (2011). Impulsivity and cognitive distortions in pathological gamblers attending the UK national problem gambling clinic: A preliminary report. Psychological Medicine, 41(12), 2625–2635. http://doi.org/10.1017/S003329171100095X
- Milosevic, A., & Ledgerwood, D. M. (2010). The subtyping of pathological gambling: A comprehensive review. Clinical Psychology Review, 30(8), 988–998. https://doi.org/10.1016/j.cpr.2010.06.013
- Moon, M., Lister, J. J., Milosevic, A., & Ledgerwood, D. M. (2016). Subtyping non-treatment seeking problem gamblers using the pathways model. Journal of Gambling Studies, 33(3), 841–853. https://doi.org/10.1007/s10899-016-9658-y
- Navas, J. F., Billieux, J., Perandrés-Gómez, A., López-Torrecillas, F., Cándido, A., & Perales, J. C. (2017). Impulsivity traits and gambling cognitions associated with gambling preferences and clinical status. International Gambling Studies, 17(1), 102–124. https://doi.org/10.1080/14459795.2016.1275739
- Nower, L., Martins, S. S., Lin, K. H., & Blanco, C. (2013). Subtypes of disordered gamblers: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. Addiction, 108(4), 789–798. http://dx.doi.org/10.1111/add.12012
- Nower, L., & Blaszczynski, A. (2017). Development and validation of the Gambling Pathways Questionnaire (GPQ). Psychology of Addictive Behaviors, 31(1), 95–109. http://dx.doi.org/10.1037/adb0000234
- Nower, L., Blaszczynski, A., & Anthony, W. L. (2022). Clarifying gambling subtypes: The revised pathways model of problem gambling. Addiction 117(7),2000–2008. http://dx.doi.org/10.1111/add.15745
- Oei, T. P. S., & Raylu, N. (2010). Gambling behaviours and motivations: A cross-cultural study of Chinese and Caucasians in Australia. International Journal of Social Psychiatry, 56(1), 23–34. https://doi.org/10.1177/0020764008095692
- Ohtsuka, K., & Hyam, P. (2003). Internal and external attribution of success and failure in gambling and nongambling situation. In G. Coman, M. Walker, A. Jackson, & P. Thomas (Eds.), The proceedings of the 12th Annual National Association for Gambling Studies Conference, Melbourne, November 2002 (pp. 357–369).
- Okuda, M., Balàn, I., Petry, N. M., Oquendo, M., & Blanco, C. (2009). Cognitive-behavioral therapy for pathological gambling: Cultural considerations. American Journal of Psychiatry, 166(12), 1325–1330. https://doi.org/10.1176/appi.ajp.2009.08081235
- Pantalon, M. V., Maciejewski, P. K., Desai, R. A., & Potenza, M. N. (2008). Excitement-seeking gambling in a nationally representative sample of recreational gamblers. Journal of Gambling Studies, 24(1), 63–78. https://doi.org/10.1007/s10899-007-9075-3
- Petry, N. P. (2004). Pathological gambling: Etiology, comorbidity, and treatment. American Psychological Association.
- Petry, N. M., & Steinberg, K. L. (2005). Childhood maltreatment in male and female treatment-seeking pathological gamblers. Psychology of Addictive Behaviors, 19(2), 226–229. https://doi.org/10.1037/0893-164X.19.2.226
- Petry, N. M., Stinson, F. S., & Grant, B. F. (2005). Comorbidity of DSM-IV pathological gambling and other psychiatric disorders: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. Journal of Clinical Psychiatry, 66(5), 564–574. http://dx.doi.org/10.4088/JCP.v66n0504
- Petry, N. M., Ammerman, Y., Bohl, J., Doersch, A., Gay, H., Kadden, R., Molina, C. A., & Steinberg, K. (2006). Cognitive-behavioral therapy for pathological gamblers. Journal of Consulting and Clinical Psychology, 74(3), 555–567. https://doi.org/10.1037/0022-006X.74.3.555
- Petry, N. M., Ginley, M. K., & Rash, C. J. (2017). A systematic review of treatment for problem gambling. Psychology of Addictive Behaviors, 31(8), 951–961. https://doi.org/10.1037/adb0000290
- Philippot, P., Bouvard, M., Baeyens, C., & Dethier, V. (2019). Case conceptualization from a process-based and modular perspective: Rationale and application to mood and anxiety disorders. Clinical Psychology & Psychotherapy, 26(2), 175–190. http://dx.doi.org/10.1002/cpp.2340
- Ramnerö, J., & Törneke, N. (2008). ABCs of human behavior: Behavioral principles for the practicing clinician. New Harbinger; Context Press.
- Raylu, N., & Oei, T. P. S. (2004). The Gambling Related Cognitions Scale (GRCS): Development, confirmatory factor validation and psychometric properties. Addiction, 99(6), 757–769. https://doi.org/10.1111/j.1360-0443.2004.00753.x
- Reid, R. L. (1986). The psychology of the near miss. Journal of Gambling Behavior, 2(1), 32–39. https://doi.org/10.1007/BF01019932
- Rende, R., & Plomin, R. (1992). Diathesis-stress models of psychopathology: A quantitative genetic perspective. Applied and Preventive Psychology, 1(4), 177–182. https://doi.org/10.1016/S0962-1849(05)80123-4
- Riesch, S. K., Anderson, L. S., Pridham, K. A., Lutz, K. F., & Becker, P. T. (2010). Furthering the understanding of parent child relationships: A nursing scholarship review series. Part 5: Parent-adolescent and teen parent-child relationships. Journal for Specialists in Pediatric Nursing, 15(3), 182–201. http://dx.doi.org/10.1111/j.1744-6155.2009.00228.x
- Rogers, P., & Webley, P. (2001). “It could be us!”: Cognitive and social psychological factors in UK national lottery play. Applied Psychology: An International Review, 50(1), 181–199. https://doi.org/10.1111/1464-0597.00053
- Rogier, G., Beomonte Zobel, S., & Velotti, P. (2020). Pathological personality facets and emotion (dys) regulation in gambling disorder. Scandinavian Journal of Psychology, 61(2), 262–270. https://doi.org/10.1111/sjop.12579
- Schafer, I., Langeland, W., Hissbach, J., Luedecke, C., Ohlmeier, M. D., Chodzinski, C., Kemper, U., Keiper, P., Wedekind, D., Havemann-Reinecke, U., Teunissen, S., Weirich, S., & Driessen, M., & the TRAUMAB-Study group. (2010). Childhood trauma and dissociation in patients with alcohol dependence, drug dependence, or both: A multi-center study. Drug and Alcohol Dependence, 109(1–3), 84–89. https://doi.org/10.1016/j.drugalcdep.2009.12.012
- Schellenberg, B. J. I., McGrath, D. S., & Dechant, K. (2016). The Gambling Motives Questionnaire financial: Factor structure, measurement invariance, and relationships with gambling behaviour. International Gambling Studies, 16(1), 1–16. https://doi.org/10.1080/14459795.2015.1088559
- Schiebener, J., Wegmann, E., Gathmann, B., Laier, C., Pawlikowski, M., & Brand, M. (2014). Among three different executive functions, general executive control ability is a key predictor of decision making under objective risk. Frontiers in Psychology, 5, 1386. Article. https://doi.org/10.3389/fpsyg.2014.01386.
- Sévigny, S., & Ladouceur, R. (2003). Gamblers’ irrational thinking about chance events: The ‘double switching’ concept. International Gambling Studies, 3(2), 149–161. https://doi.org/10.1080/1356347032000142261
- Sharman, S., Clark, L., Roberts, A., Michalczuk, R., Cocks, R., & Bowden-Jones, H. (2019). Heterogeneity in disordered gambling: Decision-making and impulsivity in gamblers grouped by preferred form. Frontiers in Psychiatry, 10, 588. https://doi.org/10.3389/fpsyt.2019.00588
- Somer, E. (2003). Prediction of abstinence from heroin addiction by childhood trauma, dissociation, and extent of psychosocial treatment. Addiction Research & Theory, 11(5), 339–348. https://doi.org/10.1080/1606635031000141102
- Suomi, A., Dowling, N. A., & Jackson, A. C. (2014). Problem gambling subtypes based on psychological distress, alcohol abuse and impulsivity. Addictive Behaviors, 39(12), 1741–1745. https://doi.org/10.1016/j.addbeh.2014.07.023
- Taylor, G. J., Bagby, R. M., & Parker, J. D. A. (1997). Disorders of affect regulation: Alexithymia in medical and psychiatric illness. Cambridge University Press.
- Timulak, L., & Koegh, D. (2021). Transdiagnostic emotion-focused therapy: A clinical guide for transforming emotional pain. American Psychological Association.
- Turner, N. E., Jain, U., Spence, W., & Zangeneh, M. (2008). Pathways to pathological gambling: Component analysis of variables related to pathological gambling. International Gambling Studies, 8(3), 281–298. https://doi.org/10.1080/14459790802405905
- Tversky, A., & Kahneman, D. (1971). Belief in the law of small numbers. Psychological Bulletin, 76(2), 105–110. https://doi.org/10.1037/h0031322
- Valleur, M., Codina, I., Vénisse, J. L., Romo, L., Magalon, D., Fatséas, M., Chéreau-Boudet, I., Gorsane, M. A., Guilleux, A., Groupe, J. E. U., Grall-Bronnec, M., & Challet-Bouju, G. (2015). Towards a validation of the three pathways model of pathological gambling. Journal of Gambling Studies, 32(2), 757–771. https://doi.org/10.1007/s10899-015-9545-y
- Velotti, P., Rogier, G., Beomonte Zobel, S., & Billieux, J. (2021). Association between gambling disorder and emotion (dys)regulation: A systematic review and meta-analysis. Clinical Psychology Review, 87, 102037. https://doi.org/10.1016/j.cpr.2021.102037.
- von der Heiden, J. M., & Egloff, B. (2021). Associations of the Big Five and locus of control with problem gambling in a large Australian sample. PLoS One, 16(6), e0253046. Article. https://doi.org/10.1371/journal.pone.0253046
- Waldron, H. B., Brody, J. L., Robbins, M. S., & Alexander, J. F. (2013). Functional family therapy for adolescent substance use disorders. In P. M. Miller, S. A. Ball, M. E. Bates, A. W. Blume, K. M. Kampman, D. J. Kavanagh, M. E. Larimer, P. M. Nancy, & P. De Witte (Eds.), Comprehensive addictive behaviors and disorders: Vol. 3. Interventions for addiction (pp. 109–116). Elsevier Academic Press.
- Williams, R. J., Leonard, C. A., Belanger, Y. D., Christensen, D. R., El-Guebaly, N., Hodgins, D. C., McGrath, D. S., Nicoll, F., Smith, G. J., & Stevens, R. M. G. (2021). Predictors of gambling and problem gambling in Canada. Canadian Journal on Public Health, 112(3), 521–529. https://doi.org/10.17269/s41997-020-00443-x
- Windle, M. (2010). A multilevel developmental contextual approach to substance use and addiction. BioSocieties, 5(1), 124–136. https://doi.org/10.1057/biosoc.2009.9
- Wulfert, E., Harris, K., & Broussard, J. (2016). The role of cross-cue reactivity in coexisting smoking and gambling habits. Journal of Gambling Issues, 32(32), 28–43. https://doi.org/10.4309/jgi.2016.32.3