ABSTRACT
Whereas assessing health is a mandatory feature of environmental impact assessments (EIAs) in Sweden, health impacts are often vaguely described, making their health preventive role meaningless. In 2006, a mine was planned in the reindeer grazing lands of a Sámi community in northern Sweden. While an EIA was conducted in 2013, health was superficially addressed. The aim of this study was to describe and reflect on the health impact assessment (HIA) process that assessed the potential health risks and/or benefits that the mine establishment could bring to the Sámi community.
The classic five steps of an HIA are presented. The literature review showed a scarcity of studies regarding HIA on mining in indigenous territories. Participants in the study were currently experiencing negative psychosocial health effects and described potential adverse social and health effects originating from the loss of their traditional way of life.
Despite certain challenges, this study proved that it is possible to conduct a comprehensive HIA in the context of Sámi health research. Given that mining in Sweden occurs mostly in Sámi territory and the adverse health effects found in this study, the lack of comprehensive HIAs on mining projects in Sweden raises serious concerns.
Introduction
Health impact assessment (HIA) has gained acknowledgement internationally as a feasible method to assess health at the population level when a new policy or project is planned to be implemented (Finer et al. Citation2005; Knutsson and Linell Citation2010; Birley Citation2011; Fischer and Cave Citation2018) and thus as a universal decision-support tool in policymaking (Kemm Citation2001; Wismar et al. Citation2007; Winkler et al. Citation2020). The World Health Organization (WHO) through the Gothenburg Consensus paper defined HIA as ‘a combination of procedures, methods and tools by which a policy, program or project may be judged as to its potential effects on the health of a population, and the distribution of those effects within the population’ (WHO Regional Office for Europe Citation1999). Both the WHO European Region and the European Union (EU) have endorsed HIA to promote good and equal health among citizens.
Sweden has 21 regions and 290 municipalities led by directly elected politicians as a form of decentralized governing. Regions are responsible for health care and other services, such as public transport, whilst municipalities oversee, for example, child and elder care and education. The development of HIA in the country began in the mid-1990s as a response to the needs of local government sectors, which required an instrument to achieve ‘healthier decisions’ in policymaking (Berensson Citation2004). HIA was perceived as a tool to aid professionals in weighing gains against losses of a policy, and as such make decisions in accordance with the national public health objectives (Berensson and Tillgren Citation2017). The Swedish government took on the task to create pathways for the regions and municipalities to incorporate HIA into their regular practice (Knutsson and Linell Citation2010), and the development of HIA guidelines was commissioned to the Swedish National Institute of Public Health (SNIPH). During 2005–2008, two guides on how to perform HIA were published (Swedish National Institute of Public Health Citation2005; Brodin and Hodge Citation2008), and at least two assessments in the areas of infrastructure and physical planning were undertaken by the SNIPH (Linell Citation2005; Linell et al. Citation2008). Today, the Swedish Association of Local Authorities and Regions (SALAR) has the responsibility to keep developing HIAs on a regional level, and the municipalities are instructed by the government to routinely apply HIAs (Berensson Citation2004; Berensson and Tillgren Citation2017). Yet, a survey distributed by the SALAR among regions and municipalities showed that the use of HIA had declined over the years. In 2013, about one third out of 36 sampled municipalities, and four of 21 regions, reported the use of HIA or ‘similar methods’ (Berensson and Tillgren Citation2017). While there still seems to be a positive interest in HIA among local managers and policymakers, the skills required, the voluntary application, and the lack of funding remain strong barriers to its general implementation. Although many sectors would like to see mandatory HIA legislation or the merger of different assessments into one statutory assessment (Finer et al. Citation2005), HIA is still not a common practice in Sweden, particularly in environment-impacting-related sectors like mining.
Sweden’s economy is greatly dependent on mining, and new ventures are currently planned at different sites, mostly in northern Sweden (Geological Survey of Sweden Citation2019). Since mining has significant negative effects on the environment (Haddaway et al. Citation2019), environmental impact assessments (EIAs) are compulsory by law (Ministry of Health and Social Affairs Citation2017). EIAs have been criticized on three main grounds, in relation to its general appliance and to mining: i) conflict of interest, since the mining company itself hires a consultant firm to assess the potential environmental effects of a project; ii) assessments that are not subject to any official review; and iii) inadequate consultation and decision-making process with the Sámi, the indigenous people of Sweden, when the mine is on their territory (Hedlund and Johansson Citation2008; Lawrence and Larsen Citation2017, Citation2019, Citation2019). While assessing health is a mandatory feature of an EIA, preferably using an HIA (Swedish Environmental Protection Agency Citation2020), health impacts are often vaguely described in EIAs. Kågström (Citation2009) argued that it is the disparate interpretations of what (good) health is and how it should be measured that marginalize the relevance of health in EIAs. Consequently, this often leaves the potential impacts of these projects on the local population’s health inconclusive. To our knowledge, no comprehensive HIA related to mining has ever been performed in Sweden.
The Gállok/Kallak case
Gállok/Kallak is a peninsula, located between the lakes Parkijaur and Skalka, in the valley of the Lesser Lule River, Norrbotten county. About 40 km south-east lies Jokkmokk which is the nearest town. The area is inhabited by approximately 100 people (both Sámi and non-Sámi), and the land is used all year round for reindeer herding by the Sámi community Jåhkågasska tjiellde. Since 2006, the British mining company Beowulf Mining plc has had an interest in the same grounds due to its high value of ore, an area which concerns about 103 hectares (Beowulf Mining plc Citation2019). A new mine would split the land of Jåhkågasska tjiellde in half as well as decimate the reindeers’ grazing grounds. This, in turn, would mean that the Sámi community would not be able to keep the same number of reindeers due to higher feeding costs, which, in a long-term perspective, could lead to the disappearance of reindeer herding in this area (Persson et al. Citation2017). Test drillings began in 2013, and the company is currently awaiting a decision from the Swedish government on whether they will obtain the concession permit needed to have the full right to exploit Gállok/Kallak (Beowulf Mining plc Citation2019). An EIA was performed in 2013/2014 on behalf of the mining company as part of the exploration permit process. Health was briefly mentioned and only in relation to the potential environmental effects (impacts on health due to levels of dust, noise, and vibrations). The report concluded that the potential health impacts of the future mine on humans as well as animals were minor (Hifab Citation2013).
Sámiid Riikkasearvi (the Swedish Sámi People’s National Association, SSR), as part of a broader participatory research collaboration, presented the case of Gállok/Kallak to researchers of the Department of Epidemiology and Global Health (EpiGH), Umeå University, in the autumn of 2019. The SSR is a national Sámi civil society organization that represents reindeer herders’ interests, and as such has broad knowledge of concerns regarding reindeer herding in Sweden. The possibilities to conduct an HIA were discussed, and prior informed consent from the Jåhkågasska tjiellde community was sought before commencing the first phase of the HIA.
The aim of this study was to describe and reflect on the HIA process that assessed the potential health risks and/or benefits that the mine establishment in Gállok/Kallak could bring to the Sámi community Jåhkågasska tjiellde.
Methods
The HIA process
Given the agreement between the SSR and the EpiGH, the principles of community-based participatory research (CBPR) were applied regarding who decided the research question, the methods implemented to gather data, and the research dissemination process. The key principles of CBPR include among other things to recognize the community as its own identity, to enable collaborative and equitable engagement of all partners in all phases of the research, and to make findings available to all partners involved (Israel et al. Citation2001). As such, all the stages of the HIA were carried out in constant dialogue between the community leadership and the researchers.
This HIA was designed to identify the potential future health impacts of the possible mining site and was thus prospective in nature. We followed the classic five steps of an HIA as recommended by the SNIPH: i) screening, ii) scoping, iii) appraisal, iv) results and recommendations, and v) monitoring and evaluation. All but step 5 could be carried out at the time of writing this article.
Before starting a full HIA, it is required to determine whether it is relevant and viable to perform it in relation to the specific intervention, the so-called screening phase. A reference group consisting of two scholars (a Sámi phycologist and a non-Sámi expert in extractive industries and Indigenous peoples) and representatives from two national Sámi organizations (SSR and Sáminuorra, the Sámi youth organization) was established to support the research team in this phase. A screening checklist was then prepared to determine the appropriateness and feasibility of the HIA and to make a preliminary assessment of the potential mine’s positive and negative effects on health. The checklist was based on the goals of the new Swedish Public Health Policy (Ministry of Health and Social Affairs Citation2017) and on the National Environment Quality Objectives (Swedish Environmental Protection Agency Citation2018). It was sent to the reference group, and the results were summarized into a screening report (Appendix A1). The conclusion of the screening report indicated the need for a full HIA.
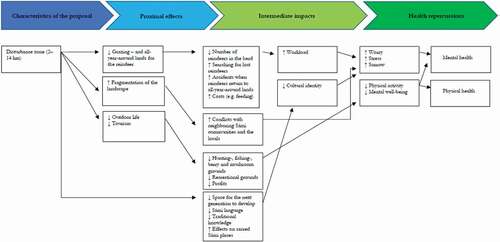
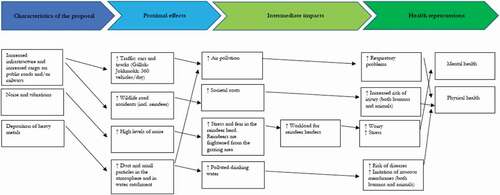
In the second stage (scoping), the logistics of the subsequent steps in the HIA are planned, and the plausible links between the mine establishment and health are mapped out and summarized into a so-called logic model. The logic model was created based on the results of the screening report and consultation with the reference group and of relevant literature. The model facilitated an understanding of the potential determinants of health, as well as its mediators and outcomes that the mine project could influence. The model was also relevant for the development of the interview guide in the next step. The logic model is included in Appendix A2.
Collecting and analyzing data are the core of step 3 of the HIA (appraisal), which we present together with the results (step 4). Two methods were used to assess the potential health impacts of the mine. First, a literature review was conducted to identify current knowledge and existing gaps in relation to HIA and mining. Keywords used for the search included ‘HIA, mining, indigenous, (mental) health’ and were combined with the following countries: Sweden, Norway, Greenland, Canada, USA (Alaska), Australia, and New Zealand. Countries were chosen due to their similarities to Sweden in terms of income level, presence of mining projects, and indigenous populations. The PubMed and Google Scholar databases were used for this purpose. The literature review revealed that studies concerning the health of indigenous populations in relation to mining sites were few and that most of the health assessments were limited in their scope (Gibson and Klinck Citation2005; Docherty et al. Citation2010; Lewis et al. Citation2017). A systematic review from 2016 examined health and well-being associated with mining activity in rural communities of high-income countries. It reported evidence of an increased prevalence of chronic diseases (e.g. mental health issues and cancers), poorer self-reported health status, loss of social connectedness, and decreased access to health services in the communities affected by mining projects. None of the reviewed studies were from the Scandinavian countries (Mactaggart et al. Citation2016).
Additionally, in-depth interviews with participants from the Sámi community Jåhkågasska tjiellde were held in spring 2019. Potential participants were urged to contact the research team themselves via a message in the community’s closed Facebook group chat. Ensuring anonymity was especially important since the Sámi community in Jokkmokk is small, and identification of individuals can be easily made. While the research team was in contact with ten potential informants, six agreed to participate. These six (three men and three women) were all connected to reindeer herding either directly or through their families. The rest of the contacted persons declined to be interviewed for reasons related to their work as reindeer herders. The informants choose the location of the interview. The interview guide aimed at capturing the current and future health impacts of the mining project. The interviews were recorded, transcribed, and later analyzed using a thematic analysis approach. Further methodological details and results can be found elsewhere (Blåhed & San Sebastian Citation2021). In summary, the results showed both current and potential future health impacts due to the mining project. The current health effects were expressed as feelings of anxiety, stress, and worry created by the marginalization and evident power asymmetry in the negotiation process as well as by the uncertainty regarding the mine concession and the implications for reindeer herding. As commented by the participants:
You feel a grim hopelessness, you feel, you become depressed, … [after] you have been to these meetings [with other mine actors] … and you go to the reindeer forest, and then you see all of that … then you feel fucking depressed, and you think, “Am I [going to be] the last generation to do this [reindeer husbandry]?”
I have felt it [the mine process] in the way that I have been stressed over [it]. I have felt uncertainty over my income (…) for sure I have felt health effects in such a way that I have been stressed.
A future without grazing lands in Gállok/Kallak would mean the end of reindeer herding for many in the community. The interviewed members of Jåhkågasska tjiellde also feared not being able to pass over a tradition of many centuries to the next generation. Possible health consequences of the mine mentioned included depression, increased alcoholism and substance abuse, and lower well-being among the community members. The following quotes illustrate these concerns:
What we love the most is the reindeer. And when we do not have grazing lands, because the mine has possessed it, well, what are we then? Nothing.
I think of the general health, of the risk of getting depressed, and that you would not want to live — that it [the potential establishment of a mine] would produce such consequences.
It would feel so very hard [if the mining company wins the process], because it would mean that what I do in my life is pointless.
Step 4 of the HIA also includes recommendations after the results have been interpreted. A report in Swedish was prepared to make the results easily accessible for the community and other stakeholders. Before the final publication, a draft was circulated among participants and the reference group as part of member checks and complemented with an oral presentation in the 2020 annual meeting of Jåhkågasska tjiellde. Four main recommendations were included in the report, which was published by the SSR in October 2020: i) HIA should become a praxis regulated by law, in any extractivist or development project; ii) HIA should be performed in a systematic, participatory, and transparent way; iii) HIA should investigate and monitor both present as well as potential future health effects in the local communities; and iv) relevant Swedish authorities should develop preventative mental health plans, enabling access to mental health support services from the start of any development project or policy affecting Sámi communities (Blåhed and San Sebastian Citation2020).
Discussion
To our knowledge, this is the first HIA related to mining conducted in Sweden, and specifically in Sápmi, the traditional land of the Sámi, contributing to the scarce international literature on HIA of mining projects in indigenous communities. Given that mining in Sweden occurs mostly in this territory and the adverse health effects found in this study, the lack of comprehensive HIAs on mining projects in Sweden raises serious concerns. But even when health is considered in the EIA, the limited view of health applied is disappointing (such as referring only to somatic but not to psychosocial health consequences). Several studies have noted that the way that health is commonly framed in current EIAs in Sweden is still narrow and focused only on environmental determinants, further marginalizing the cumulative effect that infrastructures can have in the health of the population (Kågström Citation2009; Kågström et al. Citation2013). Leaving aside crucial social determinants of health, it completely diminishes the health protection and preventive role that EIAs should aim for. This creates a conflicting situation with other ambitious governmental public health goals, such as the one aiming to close the avoidable health gaps in the country within one generation (Ministry of Health and Social Affairs Citation2017).
This study has highlighted that, in addition to potential future health impacts, the initial process of a mine establishment was already creating a series of adverse negative health impacts on the community members. Participants in the interviews were experiencing a series of symptoms related to psychosocial distress (anxiety, stress, worry) that seemed to be mediated by the lengthy mining permit permission process and the concern for the potential loss of their livelihood. Structural social determinants such as power differential among actors and discriminatory attitudes towards the community also influenced the current negative health consequences (Blåhed & San Sebastian Citation2021). While these negative health consequences have been observed across the globe among other indigenous peoples in similar mining settings (Gibson and Klinck Citation2005; Docherty et al. Citation2010; Lewis et al. Citation2017), the health effects have usually been reported after the mine establishment. This finding enhances methodologically the role of HIA as a tool to capture current impacts but also demands from government and private actors’ actions to prevent the health consequences from the early stages of a mine development.
Beyond the application of the HIA itself, a series of relevant reflections on the process is worth highlighting. This study proved that it is possible to conduct a rapid yet comprehensive HIA of a particular project in the context of Sámi health research. Trust between indigenous communities and researchers is crucial to the success of intervention studies. Previous experiences where indigenous communities have been analyzed, stereotyped, and exploited by outside groups have generated a suspicious attitude towards researchers (Beans et al. Citation2019; Bobba Citation2019). While this experience has also been part of the Sámi history (Eriksen et al. Citation2021), and certain resistance towards research might persist, this study has shown that it is possible to establish a partnership leading to successful collaboration. We followed a CBPR approach in the design and application of this assessment. This meant the involvement of the SSR and Jåhkågasska tjiellde as equal partners in the process, from the design of the aim to the dissemination of the results. The legitimacy of the SSR in the eyes of the Sámi community and the rapport established between the SSR and the EpiGH paved the way to developing and maintaining a trust-based relationship with the specific Sámi community as well. While trust is not automatically ensured by using a research methodology such as CBPR, it offers pathways to collaboration not often seen in traditional research approaches by consciously moving away from conventional top-down research towards a democratization of the scientific endeavor (Christopher et al. Citation2008). Methodologically, the study was however led by the researchers in terms of design, data collection, and analysis; while this might not necessary follow certain strict principles of community participation, it was the way decided by the SSR and the community.
Researchers interacted all the time with representatives of the organizations (SSR and Jåhkågasska tjiellde); to what extent they represented the views of their members is difficult to assess, but it is necessary to be aware of the potential implications, since who represents the community becomes a crucial matter in processes of CBPR (Flicker et al. Citation2007).
Conflict arising from timelines, expectations, insider–outsider tensions, as well as power differentials between academic researchers and the community have been brought up in the literature as potential challenges of CBPR (Minkler Citation2004; Wilson et al. Citation2018). The small-scale project in terms of scope and funding, the time and space adaptation to the availability of participants, and the confirmation of the expected findings helped to minimize some of these potential conflicts in the current project. The previous experience of the research team of working with indigenous health research and the constant discussions with the reference group further contributed to create a reflexive practice that redressed some of these imbalances.
Methodological reflections on the HIA
There are several approaches to using HIA, usually organized into four types – desktop, rapid, intermediate, and comprehensive – depending on the amount of resources needed and the duration of the assessment (Bhatia et al. Citation2010). These types of assessments should be adapted to the budget, logistics, and contextual factors of each project. In this case, a comprehensive HIA was adopted, where a reference group was formed, a literature search was performed, and in-depth interviews were carried out.
When HIAs are conducted targeting specific communities, their involvement in the process is an important prerequisite. However, community participation implies ethical issues that should be considered (Wilson et al. Citation2018). The HIA can become a community intervention in its own right and as such influence what is being communicated outwards (Campbell Citation1998; Parry and Stevens Citation2001; Den Broeder et al. Citation2017). The mere acknowledgment that an HIA is needed may change the community’s perception of the risk of the intervention. This could have been operating in this case, but the fact that participation was voluntary (and the community did not know who participated) as well as the similarity of the narratives in terms of health impacts contributed to the belief that the interviews reflect the current view and experience of participants.
This HIA focused on a specific Sámi community directly affected by the mining project. Given the complexity in terms of the affected population by this kind of project, other Sámi or non-Sámi communities, indirectly affected because of the environmental, economic, and health (positive or negative) consequences, were not included. We acknowledge that their involvement would have expanded the perspectives presented in this study.
One of the major criticisms of HIA is that the methods of collecting and analyzing evidence are not sufficiently rigorous to withstand scrutiny and challenge (Haigh et al. Citation2013). Often, the current evidence base for many health determinants is inadequate for accurately informing a process of assessment (Lock Citation2000). HIA is characterized by being a context-sensitive and methodologically neutral tool, where a mix of quantitative and qualitative designs is recommended. Although complementary quantitative measures of health impact would have been desirable in this case, only qualitative methods were used, given the difficulty to apply quantitative approaches to such a small community. Nevertheless, the study followed all the rigorous steps required by a qualitative methodology, thus providing the best available evidence to the case.
As common practice in HIA, a reference group was formed from the beginning of the HIA process. The group was active in designing the outline of the HIA as well as facilitating contacts in the screening phase and commenting on the interpretations of the results. Often, reference groups should involve a multidisciplinary working group in which different stakeholders participate. In this case, the reference group represented the Sámi society (SSR and Sáminuorra), the Sámi health research field, and the research expertise in mining conflicts in Sápmi. As previously mentioned, the inclusion of representatives of the Sámi reindeer herding society was an invaluable asset to this study and furthermore a strength of it. Mining or government representatives, however, were not involved, due to conflict of interest with the community and the sensitivity of the topic investigated. Involvement of these stakeholders could have been important to facilitate the role of the HIA in the policymaking process.
Given that the ultimate goal of an HIA is to contribute to evidence-informed policy, it is early to state to what extent this was achieved. While researchers have disseminated the report in academic and health policy environments, the SSR and the community have done so in government and mining settings. However, the outcome of these processes is unknown.
Conclusions
Sámi reindeer herding communities in Sweden are continuously impacted by different major infrastructure projects, such as dams, roads, wind power turbines, and mining. How these encroachments on traditional indigenous lands may impact the health of the Sámi is presently explored in an unsatisfactory way. This study has shown that it is feasible to conduct a comprehensive and participatory HIA in a Sámi community affected by a mine. The HIA served to reveal not only future potential health impacts but also current ones. Given the adverse health consequences found in this study and the numerous ongoing and planned mining projects in Sápmi, HIA should be clearly incorporated into Swedish legislation and thus become compulsory in any infrastructure project.
Acknowledgments
The authors would like to extent their gratitude to the Jåhkågasska tjiellde Sámi community for participating in this study.
Disclosure statement
The authors report no conflict of interest.
Additional information
Funding
References
- Beans JA, Saunkeah B, Woodbury RB, Ketchum TS, Spicer PG, Hiratsuka VY. 2019. Community protections in American Indian and Alaska Native participatory research—A scoping review. Social Sciences. 8(4):127. doi:https://doi.org/10.3390/socsci8040127.
- Beowulf Mining plc. 2019. Annual Report 2019. London: Beowulf Mining plc.
- Berensson K. 2004. HIA at the local level in Sweden. In: Kemm J, Parry J, Palmer S, editors. Health Impact Assessment. Oxford: Oxford University Press; p. 213–222.
- Berensson K, Tillgren P. 2017. Health impact assessment (HIA) of political proposals at the local level: successful introduction, but what has happened 15 years later? Glob Health Promot. 24(2):43–51. doi:https://doi.org/10.1177/1757975916683386.
- Bhatia R, et al. 2010. Minimum elements and practice standards for health impact assessment. GHPC Materials:11.
- Birley M. 2011. Health impact assessment: principles and practice. Routledge.
- Blåhed H, San Sebastian M. 2020. Det är ju faktiskt framtiden som tas ifrån en: en hälsokonsekvensbedömning med anledning av den potentiella gruvetableringen i Gállok/ Kallak,svenska Sápmi. [Actually, it is the future that is being taken away from you: a health impact assessment on account of the potential mine establishment in Gállok/ Kallak,Swedish Sámpi]. Umeå: Umeå University.
- Blåhed H, San Sebastian M. 2021. “If the reindeer die, everything dies”: the mental health of a Sámi community exposed to a mining project in Swedish Sápmi. Int J Circumpolar Health. 80(1):1935132. doi:https://doi.org/10.1080/22423982.2021.1935132.
- Bobba S. 2019. Ethics of medical research in Aboriginal and Torres Strait Islander populations. Aust J Prim Health. 25(5):402–405. doi:https://doi.org/10.1071/PY18049.
- Brodin H, Hodge S. 2008. A guide to Quantitative Methods in Health Impact Assessment. Stockholm: Swedish National Institute of Public Health.
- Campbell D. 1998. Risk language and dialects: expressing risk in relative rather than absolute terms is important. BMJ (Clinical Research Ed). 316(7139):1242. doi:https://doi.org/10.1136/bmj.316.7139.1242b.
- Christopher S, Watts V, McCormick AKHG, Young S. 2008. Building and maintaining trust in a community-based participatory research partnership. Am J Public Health. 98(8):1398–1406. doi:https://doi.org/10.2105/AJPH.2007.125757.
- Den Broeder L, Uiters E, Ten Have W, Wagemakers A, Schuit AJ. 2017. Community participation in Health Impact Assessment. A scoping review of the literature. Environ Impact Assess Rev. 66:33–42. doi:https://doi.org/10.1016/j.eiar.2017.06.004.
- Docherty BL, et al. 2010. Bearing the burden: the effects of mining on First Nations in British Columbia. Cambridge: International Human Rights Clinic, Harvard Law School.
- Eriksen H, et al. 2021. Ethical considerations for community-based participatory research with Sami communities in North Finland. In: Ambio. p. 1–15.
- Finer D, Tillgren P, Berensson K, Guldbrandsson K, Haglund BJA. 2005. Implementation of a Health Impact Assessment (HIA) tool in a regional health organization in Sweden—a feasibility study. Health Promot Int. 20(3):277–284. doi:https://doi.org/10.1093/heapro/dai009.
- Fischer TB, Cave B. 2018. Health in impact assessments – introduction to a special issue. Impact Assessment and Project Appraisal. 36(1):1–4. doi:https://doi.org/10.1080/14615517.2017.1363976.
- Flicker S, Travers R, Guta A, McDonald S, Meagher A. 2007. Ethical dilemmas in community-based participatory research: recommendations for institutional review boards. J Urban Health. 84(4):478–493. doi:https://doi.org/10.1007/s11524-007-9165-7.
- Geological Survey of Sweden. 2019. Bergverksstatistik 2018 [Statistics of the Swedish Mining Industry 2018]. Retrieved from http://resource.sgu.se/produkter/pp/pp2019-2-rapport.pdf
- Gibson G, Klinck J. 2005. Canada’s resilient north: the impact of mining on aboriginal communities. Pimatisiwin. 3(1):116–139.
- Haddaway NR, Johannesdottir SL, Piniewski M, Macura B. 2019. What ecotechnologies exist for recycling carbon and nutrients from domestic wastewater? A systematic map protocol. Environmental Evidence. 8(1):1–11. doi:https://doi.org/10.1186/s13750-018-0145-z.
- Haigh F, Harris E, Chok HN, Baum F, Harris-Roxas B, Kemp L, Spickett J, Keleher H, Morgan R, Harris M, et al. 2013. Characteristics of health impact assessments reported in Australia and New Zealand 2005-2009. Australian and New Zealand Journal of Public Health. 37(6):534–546. doi:https://doi.org/10.1111/1753-6405.12102
- Hedlund A, Johansson V. 2008. Miljökonsekvensbeskrivning. [Environmental Impact Assessment]. Uppsala: SLU - Sveriges lantbruksuniversitet [Swedish University of Agricultural Sciences]. No. 4/2008.
- Hifab. 2013. Miljökonsekvensbeskrivning - tilll ansökan om bearbetningskoncession för fyndigheten Kallak Norra [Environmental Impact Assessment - to the application for an exploitation concession permit regarding findings in North Kallak]. Umeå:Hifab.
- Israel BA, et al. 2001. Community-based participatory research: policy recommendations for promoting a partnership apprach in health research. Educ Health. 14:2.
- Kågström M. 2009. Hur ska man hantera det här med hälsa?: en kunskapsöversikt om hälsans roll i konsekvensbeskrivning och transportplanering [How to handle this with health?: a review of the role of health in impact assessments and transport planning]. Uppsala: institutionen för stad och land, Sveriges lantbruksuniversitet SLU. Uppsala: Department of Urban and Rural Development, Swedish University of Agricultural Sciences.
- Kågström M, Hilding-Rydevik T, Sjöberg I. 2013. Human health frames in EIA – the case of Swedish road planning. Impact Assessment and Project Appraisal. 31(3):198–207. doi:https://doi.org/10.1080/14615517.2013.772708.
- Kemm J. 2001. Health impact assessment: a tool for healthy public policy. Health Promot Int. 16(1):79–85. doi:https://doi.org/10.1093/heapro/16.1.79.
- Knutsson I, Linell A. 2010. Review Article: health impact assessment developments in Sweden. Scand J Public Health. 38(2):115–120. doi:https://doi.org/10.1177/1403494809357097.
- Lawrence R, Larsen RK. 2017. The politics of planning: assessing the impacts of mining on Sami lands. Third World Q. 38(5):1164–1180. doi:https://doi.org/10.1080/01436597.2016.1257909.
- Lawrence R, Larsen RK. 2019. Fighting to be herd: impcts of the Propsed Boliden Copper Mine in Laver, Älvsbyn, Sweden for the Semisjaur Njarg Sami Reindeer Herding Community. Stockholm: Stockholm Environmental Institute.
- Lewis J, Hoover J, MacKenzie D. 2017. Mining and environmental health disparities in Native American communities. Curr Environ Health Rep. 4(2):130–141. doi:https://doi.org/10.1007/s40572-017-0140-5.
- Linell A. 2005. Health impact assessment of a road traffic project. Stockholm: Swedish National Institute of Public Health.
- Linell A, et al. 2008. Health impact assessment in physical planning: in-depth comprehensive plan for the Fyrvalla-Remonthagen area, Östersund. Östersund: Swedish National Institute of Public Health.
- Lock K. 2000. Health impact assessment. BMJ. 320(7246):1395–1398. doi:https://doi.org/10.1136/bmj.320.7246.1395.
- Mactaggart F, McDermott L, Tynan A, Gericke C. 2016. Examining health and well-being outcomes associatedwith mining activity in rural communities of high-income countries: a systematic review. Aust J Rural Health. 24(4):230–237. doi:https://doi.org/10.1111/ajr.12285.
- Ministry of Health and Social Affairs. 2017. God och jämlik hälsa - en utvecklad folkhälsopolitik. Stockholm: regeringskansliet. Stockholm: Swedish Government Offices. ( Miljöbedömningsförordning (2017:966) (SE))
- Minkler M. 2004. Ethical challenges for the “outside” researcher in community-based participatory research. Health Educ Behav. 31(6):684–697. doi:https://doi.org/10.1177/1090198104269566.
- Parry J, Stevens A. 2001. Prospective health impact assessment: pitfalls, problems, and possible ways forward. BMJ. 323(7322):1177–1182. doi:https://doi.org/10.1136/bmj.323.7322.1177.
- Persson S, Harnesk D, Islar M. 2017. What local people? Examining the Gállok mining conflict and the rights of the Sámi population in terms of justice and power. Geoforum. 86:20–29. doi:https://doi.org/10.1016/j.geoforum.2017.08.009.
- Swedish Environmental Protection Agency. 2018. Sweden’s Environmental Objectives - An introduction. Stockholm:Swedish Environmental Protection Agency.
- Swedish Environmental Protection Agency. (2020). Befolkning och hälsa i miljöbedömningen. [Population and health in the environmental impact assessment]. Retrieved from https://www.naturvardsverket.se/Stod-i-miljoarbetet/Vagledningar/Miljobedomningar/Specifik-miljobedomning/Miljoaspekter-i-miljobedomning/Befolkning-och-halsa/
- Swedish National Institute of Public Health. 2005. A guide to health impact assessments: focusing on social and environmental sustainability. Stockholm:Swedish National Institute of Public Health.
- WHO Regional Office for Europe. 1999. Gothenburg Consensus Paper on Health Impact Assessment: main Concepts and Suggested Approach. Copenhagen:World Health Organization. Regional Office for Europe.
- Wilson E, Kenny A, Dickson-Swift V. 2018. Ethical challenges in community-based participatory research: a scoping review. Qual Health Res. 28(2):189–199. doi:https://doi.org/10.1177/1049732317690721.
- Winkler MS, Furu P, Viliani F, Cave B, Divall M, Ramesh G, Harris-Roxas B, Knoblauch AM. 2020. Current global health impact assessment practice. Int J Environ Res Public Health. 17(9):2988. doi:https://doi.org/10.3390/ijerph17092988.
- Wismar M, et al. 2007. The effectiveness of health impact assessment: scope and limitations of supporting decision-making in Europe. Cophenhagen: World Health Organization. Regional Office for Europe.
Appendix A1.
Excerpt from the screening report (step one of the HIA). Translated from Swedish to English by the authors. This excerpt shows the first page of the screening grid. The full screening grid includes a questionnaire relating to the proposed mine and how it corresponds to Sweden’s eight public health goals and furthermore Sweden’s environmental goals. The full screening report is not included in Appendix A1 because of its length, but readers are encouraged to contact the first author for more information.
Table
Appendix A2
The logic model from step two, scoping, of the HIA. Translated from Swedish to English by the authors. The model represents the expected effects on health and well-being, its potential determinants, as well as the mediators that the mine project could influence. The logic model is based on the responses of the reference group, from the first step of the HIA (screening) and a review of the literature on health impacts of mining projects.