
ABSTRACT
The Novel Coronavirus Pandemic causes heightened risk perceptions, in particular related to health, mortality and economic security. In 'normal' times, these are risks covered by social welfare states via social insurance and protection policies. My research question is what role the welfare state plays in a global emergency - here the SARS-Cov-2 pandemic. I test for an impact of the welfare state on risk perceptions using COVIDiSTRESS data comparing 70 countries in April, 2020. Adjusting for local timing and severity of outbreak, I demonstrate that strength of the welfare state predicts lower risk perceptions. However, this depends on the speed of government intervention: rapid intervention removes the effect of the welfare state. Therefore, I conclude from this study that when governments fail to take swift measures, the welfare state plays a major role in alleviating risk perceptions.
Introduction
Individuals perceiving a greater risk of negative life events are often unhappy. For example, perceptions of a higher likelihood of dying, losing income or experiencing war increases stress, fear and negative well-being (Tompkins et al. Citation2018). Even if those events do not actually transpire, the perception of a higher risk alone often causes psychological problems. The Novel Coronavirus Pandemic adds or intensifies actual and perceived social risks across entire societies, in particular those related to employment and health. Therefore, the Pandemic may disrupt overall well-being. This makes it a test of how well societies are prepared to deal with a sudden global change to social risks. Since the Industrial Revolution, societies started pooling risks socially as welfare states (Briggs Citation1961). Social insurance shifts the burden of risk from individuals to the societal-level and protects the public in case of emergency or need. This has strong implications for risk perceptions under normal conditions. The question I ask herein is if these implications extend to an abnormal shock to risk as experienced in the Pandemic.
Risk perceptions alone are a negative source of well-being, but they also lead to choices that may cause further problems. Risk is a fundamental aspect of human action. Theories of human behaviors spanning the social sciences rely on risk perceptions, because they provide the basis for human decision-making (Taylor-Gooby and Zinn Citation2006). Research demonstrates the role of these perceptions across diverse decision-making spheres such as health, finance and leisure (Ferrer and Klein Citation2015; Nosić and Weber Citation2010; Sönmez and Graefe Citation1998). When risk perceptions are a negative psychological load on individuals and societies, then fear or frustrated-anger may result. These are known causes of over-reactions to situations either through avoidance or unnecessary risk-seeking (Lerner and Keltner Citation2001).
Given the wide global variation and timing of the highly infectious SARS-CoV-2 virus and the life threatening Covid-19 disease it causes; a natural experiment emerges for observing risk perceptions. As of late April, 2020, the pandemic claimed 200 thousand lives in just 3 months of mass infection outside of China. Known Covid-19 deaths at that time ranged from zero cases in Vietnam to over 100,000 in the United States. The rate of infection globally was increasing rapidly in South America and Central Asia. The OECD projected a 6% decline in global Gross Domestic Product in 2020, the largest in 60 years of reporting (Gurría Citation2020). Unemployment soared, and a host of health problems arose for those surviving infection. Suffice to say that in April and still as I write this in July of 2020, these have been abnormally risky times.
Early in the pandemic, a group of researchers started a global survey project called COVIDiSTRESS (CiS), to assess the impact of the pandemic on people’s emotional well-being (Lieberoth et al. Citation2020a). The Lieberoth team made their internet collected data immediately available via the Open Science Framework, thus social scientists have the opportunity to immediately study risk perceptions during the pandemic. gives an overview of the severity of the outbreak and the period of the survey used in this study.
Figure 1. Outbreak Severity of COVID-19 across 70 Countries
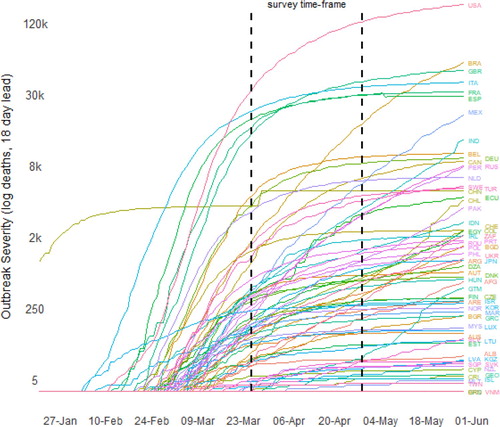
Given that testing varies widely by country, using confirmed cases as a measure of outbreak severity is unreliable. Instead, confirmed deaths indicate a cross-nationally comparable ratio of the number of infected persons 18 days ago, as this is roughly the average time-to-death from Covid-19 (Verity Citation2020). This of course requires an assumption that the death ratio is similar across all societies, which may not be true, but I trust that it is similar enough for comparison. The 18-day-lead of the death toll is logged to shed light on the infection curves shown in . All data and code for this study are available in an online Technical Appendix (https://osf.io/muhdz/).
The CiS survey started March 26th, and is still ongoing. I chose to focus on responses through the end of April because a majority of countries were surveyed in this period. After April, the country sampling becomes sporadic. Longitudinal analysis is not possible because only 7–10 countries have consistent weekly data (see Technical Appendix). Moreover, there is a risk of introducing global period effects bias when using the entire time period. The time-frame under investigation should roughly capture a cross-section during the transition to a global impact of the Pandemic. On March 15th, 174 countries and territories still had no known deaths. By April 15th, this number dropped to 51 and by May it was 37.
Testing the risk-alleviating role of welfare states
Risk perceptions are particular to individuals. Socio-economic status, race/ethnicity, religion, sex, gender, sexuality, family status, psychological risk aversion and many more factors lead to heterogeneous risk perceptions. I cannot focus on these individual-level factors in this study for two reasons. The first is that a sizeable portion of CiS respondents did not give permission to use their personal data. The second is that the survey asked only basic demographic questions, not enough to adjudicate sociological processes.
To measure risk perceptions, the CiS data includes five questions related to, ‘Concern about the consequences of the coronavirus' for ‘yourself’, ‘family’ and ‘friends’, and for ‘your country’ and ‘other countries’. Respondents answer along a six-point ‘thermometer’ from not at all concerned to very concerned. In the Technical Appendix, Table 1, Panel A lists aggregated responses and their correlations with country-level variables. Table 1, Panel B provides fit indices from confirmatory factor analyses of the questions. Model 1 lumped all six together to construct a latent variable, Model 2 divided the questions into separate self-concern and societal-concern factors (indicated by the shaded areas in Panel A), and Model 3 tested for measurement invariance across the 47 countries for which there were at least 100 respondents. As indicated by Model 2, the two-factor solution is preferable and it exhibits basic configural invariance with an RMSEA of 0.69 suggesting somewhere around 93% confidence that the fitted model, with fixed loadings across countries, does not lead to a significantly different implied covariance matrix than what is freely observed in the survey data after correcting for sample size. For my purposes this is enough to understand something about risk across societies, without delving too deep into psychometrics and measurement modeling. As such, I create two mean scales, Personal and Societal concerns about the virus for all countries that had at least 20 respondents in April. My main interest here is Personal concerns as these should be the ones most directly linked to well-being and decision-making (although I also present results for Societal concerns in the Technical Appendix).
I want to identify welfare state strength as my test variable, but measurement is a subject of great debate. Concepts such as ideal-type regimes, spending, replacement rates, historical timing, coverage and even normative principles are among social scientists’ measurement approaches (Arts and Gelissen Citation2001; Esping-Andersen Citation1989; Green-Pedersen Citation2004; Scruggs and Allan Citation2006). I do not aim to resolve this debate. My research suggests a focus on risk for the entire population. Replacement rates and coverage would be ideal, but these data are not available outside of the rich democracies of the world. Therefore, I use social spending and multiply it by the percent of the population covered by employment accident and disability protection legislation, both provided by the International Labor Organization (ILO Citation2014, Citation2019).
Work-related accidents, disability and survivor benefits are the oldest and most basic form of welfare policy (Flora and Alber Citation2009). Coverage of pensions and unemployment is equal to or, usually, less than the coverage of accident and disability, making it a good conservative baseline proxy of overall coverage. Thus, societies that spend much more but have low population coverage get adjusted downward in the index and societies that spend less but cover more adjusted upward in comparison to using just spending. The index is standardized to make it easily interpretable and I label it Welfare State Strength. visualizes the relationship of this variable and risk perceptions.
Figure 2. Welfare State and Risk Perceptions of the Novel Coronavirus Pandemic
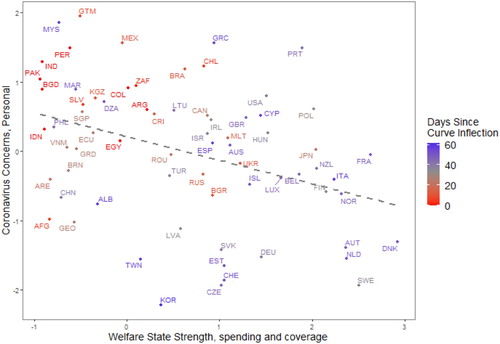
Visual results in reveal a strong association of the strength of the welfare state and personal coronavirus concerns, as indicated by the correlation of −0.41. Similar but slightly weaker association exists between societal coronavirus concerns and the welfare state (r = −0.12, Figure 3 in Technical Appendix).
Whether the level of spending and coverage of the welfare state represents an underlying set of causal mechanisms that explain risk-perceptions is unclear in . The number of days since the outbreak curve inflected has a very strong association with individual concerns. Those who are further past successful efforts to ‘flatten the curve’ are less concerned (r = −0.44) as indicated by data points shaded blue. The welfare state’s impact can only be tested while conditioning on other factors that shape risk perceptions in this Pandemic.
As shown in Table 1 (Technical Appendix), the 18-day-lead death measure is only marginally associated with risk. I assume this correlation is not higher because of timing. For example, in Italy and China, the period leading to the apex of the curve occurs before March (beige and blue lines, far left of ). This means that risk perceptions are far lower in these societies because the public senses the worst is over and adjusted more to life in a pandemic, an effect identified recently in an ongoing survey of the German population (Naumann et al Citation2020). Other societies that just began to experience a severe outbreak in April, such as Brazil and Mexico, are still in the ‘sudden and fierce’ stage, and risk perceptions are heightened. Therefore, I theorize that the time passed since the infection curve inflected from an increasing to decreasing rate week-over-week, should be a critical causal factor. I label this variable Days Since Curve Inflection and it gets a value of zero for societies that have not experienced an inflection. In the absence of longitudinal data, introducing timing in an independent variable helps me to investigate longitudinal factors in a cross-sectional data set.
The United States experience helps identify another key causal factor. Although the curve inflected in early April, the infection rate stayed very high. Therefore, whether the new cases are increasing or decreasing in the past week should also be a cause of risk perceptions. Countries such as Italy and Germany have lower risk perceptions as a result of steadily decreasing week-over-week cases since the Inflection, whereas in the United States and Great Britain the curve inflected but the rate stayed relatively high leaving risk perceptions presumably higher. Therefore, I measure New Cases on a scale from −1 to 1, where positive are increasing and negative are decreasing week-over-week rates. Again, these data only reveal results of positive tests, which leaves uncertainty related to testing differences; however, the benefit of this measures is that results of tests are what the media reports and therefore should impact individuals as much or more than the outbreak severity itself. The data for deaths and cases are from the Johns Hopkins Coronavirus Resource Center (Dong et al. Citation2020) and are aggregated along with individual respondents, so the measure is the average across all respondents in the sample matched to the day of their interview.
Other factors are that societies with more material wealth and productivity have greater resources to alleviate risks. They have stronger infrastructure and rule of law to maintain stability and services despite a pandemic. I use GDP at 2017 US dollar parity from the Maddison Project (Bolt et al. Citation2018) to measure this. In addition, governments that took intervention measures earlier during the spread of the virus should have reduced the perceived risks of their members as time passes. I measure Government Intervention as the average number of days prior to the first Covid–19 death that the government closed schools and issued stay home orders using data from Roser et al. (Citation2020). In the short-term the economic and movement restrictions of interventions may increase risk perceptions (Lieberoth et al. Citation2020b) - this is confirmed by a tiny positive correlation in Table 1 of 0.09. This is further confounded by timing, as countries that just experienced their first death in April and intervened quickly are still in the early panic phase of the pandemic. The intervention effect will reduce risk perceptions more as time passes and these measures demonstrate better results than other societies that did not take early measures. Thus, this effect is crucial to interpret as indirect and highly contingent on other factors. I consider an interaction of this variable with New Cases and Strength of Welfare State as ways to get at these complex pathways and recover what should be an indirect effect of Intervention over time.
Findings
The multivariate models are OLS regressions predicting personal () and societal (Table 3, Technical Appendix) concerns. Unfortunately, GDP and welfare state strength correlate at 0.61, therefore with 70 country-cases it is not possible to fully adjudicate unique effects. I offer M1 through M4 as baseline models for comparison. I do not believe these are accurate data-generating models, but it is important to identify that the test variables of interest increase the r-squared substantially and to compare the fitting of GDP versus Welfare State Strength, to see if models favor one or the other.
Table 2. Regressions Predicting Personal Risk-Perceptions of the Novel Coronavirus
The top two rows of measuring the timing and severity of the outbreak explain about 25% (one-quarter) of country level variation in risk perceptions (M1 adjusted r2 = 0.245). Addition of GDP or Welfare State variables independently increases this value only slightly to 26% (M2) and 27% respectively. However, the impact of GDP is not significant at p < 0.10 whereas Welfare State is significant and represents a standardized effect size of −0.21. Although this finding favors the Welfare State over GDP as a predictor variable, the difference is tiny. However, when I consider the strength of Government Intervention, a clearer image of the role of the welfare state emerges. This is indicated by an interaction of Welfare State and Government Intervention in M5.Footnote1
As interaction effects should never be interpreted in coefficient form, especially not those of continuous variables, I present the predicted margins of M5 from in .
Figure 4. Outbreak Severity of COVID-19 across 70 Countries
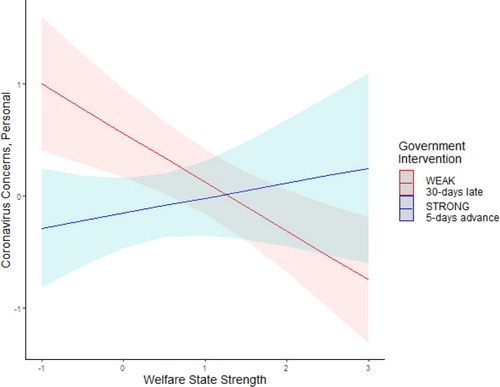
demonstrates that in societies where it took a long time for government intervention, here 30 days after the first death, Welfare State strength is associated with 1.5 standard deviations in personal risk perceptions between the weakest and strongest welfare states. On the other hand, governments that got out in front of the pandemic show no impact of the welfare state.
To contextualize, consider that the Swedish government did not enforce intervention measures, and instead urged individuals to follow best practices on their own. The resulting high infection rates should have produced high risk perceptions; however, as seen in , they were among the lowest in the world revealing the Swedish Paradox. I attribute this to the super-strong Swedish welfare state. A comparison case is the United States where the national government took only weak intervention measures. The US has a ‘strong’ welfare state in comparison to the globe, but relatively weak in comparison to Sweden. I believe that this explains some of the higher risk perceptions in the US. Brazil and France intervened somewhat late and had high infection rates, but concerns in Brazil were much higher in April than in France; and of course, the welfare state differences here are dramatic. It is difficult to compare countries within South America in April because the virus was increasing so rapidly. This is why it is important to take these claims as ‘all else equal’ using the counterfactual power of multivariate regression as opposed to interpreting single countries and single variables.
Conclusion
Results suggest that the welfare state influenced risk perceptions among the publics of 70 countries in April, 2020. Essentially all publics were affected by the pandemic by this time, either directly or as communicated through channels of media, social networks and governments. Interestingly, results suggest that the welfare state may not be a universal pandemic risk alleviator. It only appears to come into play when governments fail to take appropriate intervention measures. A strong and early intervention by the government is enough to alleviate potentially heightened risk perceptions due to the pandemic, net of the timing and severity of the virus in a given country. However, when the government fails to intervene, the longer term risk perception consequences are higher and then the welfare state becomes the next line of defense, a logical explanation for the Swedish Paradox. All else equal, comparing countries with the strongest and the weakest welfare states whose governments failed to take strong intervention measures, suggests that publics range from barely concerned (just above the mid-point on the 6-point concern scale) to very concerned (above 5 on the scale).
There are limitations to the interpretation of this large welfare state effect, some that were identified in the peer review process concerning the data-generating model. One potential threat is that risk perceptions are not only an outcome, but a cause of policy interventions. Almost all governments represented in the sample had taken some measures to intervene already in April, making it impossible to use time to sort out causality. I can only offer logic in defense. Interventions are correlated with welfare states at −0.37, meaning that weaker interventions occurred in stronger welfare states. If interventions were a response to public risk perceptions they should remove this correlation between risk perceptions and welfare states in a multivariate model, because they would be consistent with the severity of public risk perceptions. This was not the case for roughly half the sample of countries, those represented by the red line in , suggesting that the welfare state, or something highly correlated with it, likely caused risk perception outcomes. As I do not have the timing of events cross-nationally to operationalize, I cannot claim true causal inference and results should be taken cautiously. Another concern is the media and potential media-bias that most certainly causes public risk perceptions. Although it was beyond the scope of the current study, I must consider if media threatens the validity of my model. I argue it does not because it would have to be systematically correlated with welfare states, as I assume it is with risk perceptions, to act as a confounder. The only correlation I imagine is that authoritarian and state-centered media could reduce risk perceptions by downplaying the virus and hiding the facts; however, many authoritarian societies had relatively high risk perceptions as with Hungary, Vietnam and Pakistan suggesting this was not systematically true.
A third concern is the CiS internet sample. In a pandemic, household, in-person surveys are not possible so there is a potential non-representativeness of the sample with respect to households. This is a problem only if there is heterogeneity of risk perceptions in the un-sampled populations by country. My expectation is that an internet survey under-represents older persons, so the question becomes: are older persons more or less risk assuming than the rest of the populations in a way that is different depending on the country? I do not have the answer to this, but offer a speculation. My expectation, and that of one reviewer, is that older persons have higher risk perceptions, especially given that the case-to-death ratio of Covid-19 is much higher in older persons. If true, this should bias my findings toward under-estimation because weaker welfare states (mostly poorer countries) would be sampled with lower risk perceptions than the true population parameter. This makes it even more striking that the models revealed a significant effect, despite this under-estimation bias.
Although I only found partial support of my hypothesis, it is possible that the welfare state still matters in societies where the government took strong actions in response to the Pandemic. Many of the countries in this sample had just experienced their outbreak in late April and the government had only just responded. Therefore, the publics did not have time to react or determine the effectiveness of the response. This could be a source of bias in the model. Moreover, it is likely that risk perceptions among the public are part of the cause of government’s responses. Where risk perceptions are lower, government response may be more nonchalant, as policymakers have strong incentives to follow public opinion. However, in the case of a pandemic, this reaction is costly to human lives. Earlier government intervention inevitably leads to short-term risk perception heightening. Unemployment surged and small businesses risked bankruptcy, parents were mostly forced into homeschooling or caring for their children, and people experienced a high degree of social isolation as a result of lock down measures. But, if my model here is reasonably accurate, it means that governments should intervene in pandemics no matter what. Even if the public do not want it, the long term reductions to risk will outweigh the short term negative public response.
As discussed at the outset, risk perceptions are a negative psychological load in individual’s lives and might lead to irrational or fear-based actions. Of course some sense of risk is necessary to motivate healthy individual and public choices, but when it is too great or extends for too long the impact on well-being is detrimental. Some research suggests that disasters have scarring effects on individual risk perceptions, so that they are more likely to perceive risk in the future, again increasing their likelihood for negative affect and potential for reduced societal well-being (see discussion in Brown et al. Citation2018). This suggests early interventions are particularly important for longer term well-being in both strong and weak welfare states, it boils down to whether prevention of the disturbance of government imposed restrictions outweighs the scarring effect of mass unattended human burials in the long run – I am doubtful. This suggests careful consideration of not only short term, but also long term feedback effects of risk perceptions along with public opinion and policymaking (as discussed in Breznau Citation2017).
This study complements others finding non-material welfare benefits to stronger welfare states. For example, social scientists found that fear of crime is lower among individuals living where social security replacement rates are higher (Hummelsheim et al. Citation2011). One researcher demonstrated that subjective well-being is predicted by unemployment benefit generosity, suggesting that insurance provides peace of mind as much as income replacement (Sjöberg Citation2010). Based on psychological research I infer that individuals with higher risk perceptions measured as concern for themselves, families and friends experience negative well-being. As such, this study suggests that the welfare state could have large impacts on individual well-being in case of societal-level shocks or states of emergency. Building a strong welfare state has spillover effects by making societies better prepared for both the economic and psychological impacts of future pandemics.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes on contributors
Nate Breznau
Nate Breznau holds a PhD in Sociology from the Bremen International Graduate School of Social Sciences, has done extensive research on public opinion and individual attitudes as they relate to politics, social welfare and inequality and works on issues of social policy in both sociology and political science. He previously held postdoctoral positions at the University of Bremen and University of Mannheim, and was the recipient of a Wikimedia Freies Wissen Fellowship to promote open science and a German Science Foundation grant to study the ‘Reciprocal Relationship of Public Opinion and Social Policy'.
Notes
1 A note to readers: the interaction of Intervention and New Cases proved to be problematic most likely because the virus only just arrived in many countries in April and Interventions taken in these countries are strong, but still positively correlate with New Cases; whereas countries with strong interventions that took place longer ago have the opposite correlation, thus the indirect effect of Interventions was not identified and dropped from the models.
References
- Arts, W. and Gelissen, J. (2001) ‘Welfare states, solidarity and justice principles: does the type really matter?’, Acta Sociologica 44(4): 283–299. doi: 10.1177/000169930104400401
- Bolt, J., Inklaar, R., de Jong, H. and van Zanden, J. L. (2018) Maddison Project Database, Version 20. Rebasing ‘Maddison’: New Income Comparisons and the Shape of Long-Run Economic Development. University of Groningen. https://www.rug.nl/ggdc/historicaldevelopment/maddison/releases/maddison-project-database-2018.
- Breznau, N. (2017) ‘Positive returns and equilibrium: simultaneous feedback between public opinion and social policy’, Policy Studies Journal 45(4): 583–612. doi: 10.1111/psj.12171
- Briggs, Asa. 1961. ‘The welfare state in historical perspective’, in C. Pierson and F. G. Castles (eds.), The Welfare State Reader, Cambridge: Polity Press, pp. 17–29.
- Brown, P., Daigneault, A. J., Tjernström, E. and Zou, W. (2018) ‘Natural disasters, social protection, and risk perceptions’, World Development 104: 310–25. doi: 10.1016/j.worlddev.2017.12.002
- Dong, E., Du, H. and Gardner, L. (2020) ‘An interactive web-based dashboard to track COVID-19 in real time’, The Lancet Infectious Diseases 20(5): 533–34. https://coronavirus.jhu.edu/map.html. doi: 10.1016/S1473-3099(20)30120-1
- Esping-Andersen, G. (1989) ‘The three political economies of the welfare state’, Canadian Review of Sociology 26(1): 10–36. doi: 10.1111/j.1755-618X.1989.tb00411.x
- Ferrer, R. A. and Klein, W. M. (2015) ‘Risk perceptions and health behavior’, Current Opinion in Psychology 5: 85–89. doi: 10.1016/j.copsyc.2015.03.012
- Flora, Peter, and Jens Alber. 2009. ‘Modernization, democratization, and the development of welfare states in Western Europe’, in The Development of Welfare States in Europe and America [Originally Published 1976], ed. Peter Flora and Arnold J. Heidenheimer, New Brunswick: Transaction Publishers, pp. 37–80.
- Green-Pedersen, C. (2004) ‘The dependent variable problem within the study of welfare state retrenchment: defining the problem and looking for solutions’, Journal of Comparative Policy Analysis: Research and Practice 6(1): 3–14.
- Gurría, A. (2020) Release of the June 2020 Economic Outlook: Revamping the International Policy Architecture to Emerge from the Pandemic Stronger Together – OECD. OECD Secretary-General Press Release. https://www.oecd.org/economy/release-of-the-june-2020-economic-outlook.htm [Accessed 21 Jun 2020].
- Hummelsheim, D., Hirtenlehner, H., Jackson, J. and Oberwittler, D. (2011) ‘Social insecurities and fear of crime: a cross-national study on the impact of welfare state policies on crime-related anxieties’, European Sociological Review 27(3): 327–45. doi: 10.1093/esr/jcq010
- ILO (2014) ‘Global Programme Employment Injury Insurance and Protection | GEIP Data’. https://www.ilo.org/wcmsp5/groups/public/—ed_emp/—emp_ent/documents/publication/wcms_573083.pdf.
- ILO (2019) Social Expenditure as a Percentage of GDP (Table 16). International Labor Organization. https://www.social-protection.org/gimi/gess/ShowWiki.action?id=594#tabs-3.
- Lerner, Jennifer S. and Dacher Keltner. 2001. ‘Fear, anger, and risk', Journal of Personality and Social Psychology 81: 146–59. doi: 10.1037/0022-3514.81.1.146
- Lieberoth, A., Ćepulić, D.-B., Rasmussen, J., Tran, T., Han, H., Lin, S.-Y., Tuominen, J. and Travaglino, G.-A. (2020a) ‘COVIDiSTRESS Global Survey,’ Open Science Framework (osf.io/z39us).
- Lieberoth, A., Lin, S.-L., Kowal, M. and Chrona, S. (2020b) Stress and Worry in the 2020 Coronavirus Pandemic: Relationships to Trust and Compliance with Preventive Measures across 45 Countries. Registered Report accepted at the Royal Society for Open Science, final paper currently under-review.
- Naumann, E., Mata, J., Reifenscheid, M., Möhring, K., Wenz, A., Rettig, T., Lehrer, R., Krieger, U., Juhl, S., Friedel, S., Fikel, M., Cornesse, C. and Blom, A. G. (2020) Die Mannheimer Corona-Studie: Schwerpunktbericht Zum Angstempfinden in Der Bevölkerung. Survey Results. University of Mannheim. https://www.uni-mannheim.de/media/Einrichtungen/gip/Corona_Studie/Schwerpunktbericht_Angstempfinden_Mannheimer_Corona_Studie.pdf.
- Nosić, A. and Weber, M. (2010) ‘How riskily do i invest? The role of risk attitudes, risk perceptions, and overconfidence’, Decision Analysis 7(3): 282–301. doi: 10.1287/deca.1100.0178
- Roser, M., Hasell, J., Ortiz-Ospina, E. and Ritchie, H. (2020) ‘Coronavirus Pandemic (COVID-19): Policy Responses to the Coronavirus Pandemic’, Our World in Data. https://ourworldindata.org/coronavirus.
- Scruggs, L. and Allan, J. (2006) ‘Welfare-state decommodification in 18 OECD countries: a replication and revision’, Journal of European Social Policy 16(1): 55–72. doi: 10.1177/0958928706059833
- Sjöberg, O. (2010) ‘Social insurance as a collective resource: unemployment benefits, job insecurity and subjective well-being in a comparative perspective’, Social Forces 88(3): 1281–1304. doi: 10.1353/sof.0.0293
- Sönmez, S. F. and Graefe, A. R. (1998) ‘Determining future travel behavior from past travel experience and perceptions of risk and safety’, Journal of Travel Research 37(2): 171–77. doi: 10.1177/004728759803700209
- Taylor-Gooby, P. and Zinn, J. O. (2006) ‘Current directions in risk research: new developments in psychology and sociology’, Risk Analysis 26(2): 397–411. doi: 10.1111/j.1539-6924.2006.00746.x
- Tompkins, Mary Kate, Pär Bjälkebring, and Ellen Peters. 2018. ‘Emotional aspects of risk perceptions’, in Martina Raue, Eva Lermer, and Bernhard Streicher (eds.) Psychological Perspectives on Risk and Risk Analysis: Theory, Models, and Applications. Cham: Springer International Publishing, pp. 109–30.
- Verity, R. (2020) ‘Estimates of the severity of coronavirus disease 2019: a model-based analysis’, The Lancet Infectious Diseases 20(6): 669–77. doi: 10.1016/S1473-3099(20)30243-7