
ABSTRACT
There is a large body of evidence which demonstrates that breastfeeding a child to the age of two years and beyond provides the optimal health benefits for both women and child. However, the wider perception of the ideal breastfeeding duration is often debated and there are stark differences in prevalence of breastfeeding beyond infancy globally. Therefore, this narrative synthesis was employed as a way of rapidly and efficiently gathering relevant information to provide context to understanding a woman’s ability to continue breastfeeding. Extracted emerging themes were categorised against the Bronfenbrenner’s Ecological Systems framework, a widely accepted theoretical model which offers explanation on how individual’s behaviour interplays with five layers of social environment ‘systems’. The themes include 1) Microsystems: Postnatal challenges, Parental style and preference, Age, First-time mothers and Adversity and trauma. 2) Mesosytems: Fathers/domestic relationships, Grandparents, Peer to peer. 3) Exosystems: Public perception and representations, Returning to work. 4) Macrosystems: ethnic group distinctions, religion, national systems. 5) Chronosytems: inequality groups, immigration, and historical context. The review has demonstrated that breastfeeding, and any interventions targeted to support the initiation or continuation of it, must be viewed with an intersectional lens.
Introduction
For the optimal health benefits for both mother and child the World Health Organisation (WHO Citation2019) recommends breastfeeding exclusively for the first six months and then to continue along with the introduction of solid food until the infant is at least two years and beyond. The terms used to describe breastfeeding beyond the age of infancy (12 months) varies including prolonged, continued, sustained, extended, long-term or natural-term breastfeeding (Faircloth Citation2017). A previous breastfeeding duration review, by Mortensen and Tawia (Citation2013), highlighted that there are those who consider prolonged feeding to be at three months, others six or nine months. However, the age when a child naturally weans ranges from two to seven years old (Dettwyler Citation2017) and whilst the benefits of initiating breastfeeding are widely accepted, its duration is often debated. This could partly be explained because the guidance for the introduction of solid foods (weaning) is inconsistent both between and within countries and, in the past, recommendations have changed (Koplin and Allen Citation2013). Additionally, commercial weaning food is targeted for children at four months (García et al. Citation2013) giving mixed messages to parents. Faircloth (Citation2010) highlighted that breastfeeding duration is contentious because there is a view breastfeeding beyond infancy is strange and possibly perverted. This indicates that there is a need for greater understanding of the complexities around a women’s ability to continue breastfeeding.
Benefits of breastfeeding beyond infancy
There is a strong body of evidence for the benefits of continuing breastfeeding beyond infancy for both mother and child. For the child, benefits range from improved mental performance and language development (Knio et al. Citation2018; Oddy et al. Citation2011; Whitehouse et al. Citation2011), a healthier diet and reduced risk of obseity (Spaniol et al. Citation2020; Scott, Tsz Ying, and Oddy Citation2012) and strengthened child attachment security (Weaver, Schofield, and Papp Citation2018). For the mother breastfeeding beyond infancy reduces the risk of breast cancer (Baulies et al. Citation2015), diabetes (Grainger, Joseph, and Sherring Citation2015) and cardiovascular disease (Wiklund et al. Citation2012). This evidence illustrates the importance of supporting women to initiate breastfeeding and to continue beyond infancy.
Understanding disparities in breastfeeding beyond infancy
There are stark differences in prevalence of breastfeeding beyond infancy globally. Victora et al. (Citation2016) highlighted that high-income countries had the lowest percentage of mothers breastfeeding at 12 months and there were notable differences between the UK (<1%), USA (27%) Norway (35%) and Sweden (16%) recorded. This data came over a decade after the launch of the Global Strategy for Infant and Young Child Feeding (WHO Citation2003) which set out to tackle major disparities in duration. Developing integrated knowledge of the multifaceted complexities which impact prevalence differences between countries could aid in addressing this. Therefore, this narrative review has been conducted to synthesise evidence to understand a women’s ability to continue breastfeeding. These insights can then support the refinement of breastfeeding interventions and subsequent inquiries.
Ecological Systems Theory
The Bronfenbrenner’s ecological systems theory has been applied as a theoretical framework for examining the contextual layers of enablers and barriers to continued breastfeeding (Härkönen, Citation2001). Although this theoretical model has evolved and been adapted over time (Tudge et al. Citation2009), this study adopts the earlier perspective, which offers explanation on how individual’s behaviour interplays with five layers of social environment ‘systems’ (Bronfenbrenner Citation1975, Citation1979). The microsystem layer incorporates elements which are directly related to the breastfeeding women whereas the mesosytem layer considers wider formal and informal social structures. However, these social structures also interact directly with the breastfeeding individual. In the exosystem layer, larger social systems, such as the individual’s community are considered. The macrosystem comprises of cultural patterns and values. The last layer, chronosystem incorporates the wider societal changes and the historical context. As such, this model situates the review findings within the different contexts which shape women’s feeding choices (see ).
Method
Narrative reviews are common in medical literature and was employed as a way of rapidly and efficiently gathering relevant information that provides context (Baethge, Goldbeck-Wood, and Mertens Citation2019). The literature search was conducted using the following electronic databases; Medline, Embase, Cumulative Index to Nursing and Allied Health Literature (CINAHL), The Cochrane Library, PsycInfo and grey literature (The Healthcare Management Information Consortium, HMIC) between January and April 2021. The search was limited by ten years and languages of dissemination was limited to English due to the large number of identified papers. Free text ‘keywords’ search terms were identified from the synthesis of the introductory literature. These terms were used in a variety of combinations and were exhaustively explored: breastfeed* experience*, behaviours* continued, patterns, duration, enabler, barrier, challenge. Boolean Operators were used to expand and combine searches.
The purpose of the review was to gather a broad range of literature for the phenomena of interest (Peters et al. Citation2015) and so both qualitative and quantitative research were included. The inclusion and exclusion criteria reflected the aim of understanding a women’s ability to continue breastfeeding. Papers were included if they examined interventions aimed to reduce breastfeeding cessation and excluded if they were only concerned with the breastfeeding initiation and/or the outcomes of breastfeeding. Anecdotal articles, economic analysis, or clinical practice guidelines were also excluded.
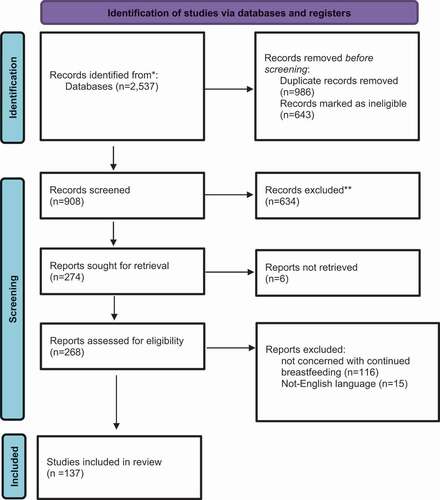
There were n = 908 papers screened and a total of n = 137 selected for synthesis (see ). A textual narrative summary approach was applied to identify the context (Lucas et al. Citation2007). Title and abstracts were screened and organised into subjects using a referencing manager software. A charting table was used to identify study author/year, objectives/methodology, context (study location) and the concept related to a women’s ability to continue breastfeed. This included highlighted enablers and barriers to breastfeeding. Identified themes were then categorised against the Bronfenbrenner’s Ecological Systems framework (Härkönen, Citation2001) (see ).
Figure 1. PRISMA flow diagram (Page et al. Citation2021).
Findings
Figure 2. Schematic illustration of findings against Bronfenbrenner’s ecological systems.
Microsystem (individual)
Postnatal challenges
A body of literature attempts to understand why parents stop breastfeeding, earlier then planned, in the postnatal period. Reasons identified include, perceived difficulties producing breastmilk (Newby and Davies Citation2016), illness or difficulties associated with pumping (Odom et al. Citation2013). Cohen et al. (Citation2018) identified mode of delivery at birth, parity, dyad separation, maternal breastfeeding education as barriers. Additionally, women who experienced difficulties with attachment, engorged breasts, sore nipples, milk stasis and mastitis were more likely to stop (Levinienė et al. Citation2013). Women with an unplanned pregnancy (Rudzik Citation2012) or who are measured as overweight or obese (Bjørset et al. Citation2018) have reduced odds of continuing. In terms of the enabling continuation, a vaginal birth delivery is identified as a positive factor (Bell et al. Citation2015).
Parental styles and preference
Parental choices impact breastfeeding duration. For example, infants fed expressed breastmilk are at a higher risk of discontinuing than those feeding directly at the breast (Pang et al. Citation2017). Parents who supplement their breastmilk with substitutes have been seen to have a shorter duration (Kim et al. Citation2013). Despite the recommendations against co-sleeping with the infant, this practice has been associated with a longer duration (Huang et al. Citation2013). Parents who do not give their child additional fluids or pacifiers (Levinienė et al. Citation2013), who do not introduce complementary food early (Scott et al. Citation2019), and who actively abstain from drinking alcohol (Logan et al. Citation2016) have all been associated with lower rates of early cessation. Psychological factors such as breastfeeding plan, intention, attitudes, subjective norms, beliefs, confidence, or self-efficacy, are identified as good predictors for a longer duration (Susiloretni et al. Citation2015).
Age
Adolescent mothers have been identified as having lower rates of breastfeeding (Kanhadilok and McGrath Citation2015). One barrier identified, in a study conducted with teenage mothers in South Africa, is lack of autonomy due to maternal grandmother taking on parenting decision-making (Jama et al. Citation2018). In a study conducted among Thai teenage mothers in Bangkok, it was thought that the complexity of balancing their own adolescent development and breastfeeding acts as a challenge to continue (Nuampa et al. Citation2019, Citation2018; Supannee et al. Citation2016).
First-time mothers
First-time mothers have been shown to have significantly different breastfeeding experiences then those who have breastfed a child previously. Women with multiple children have been shown to be more likely to breastfeed for longer (Hackman et al. Citation2015). However, Bai, Fong, and Tarrant (Citation2015) indicated that women who breastfed for less than three months were more likely to wean early with subsequent children. A higher number of children in the family and later birth order of the child have shown correlations with longer duration (Hunegnaw, Gelaye, and Ali Citation2018).
Adversity and trauma
There is indication that maternal stress, sensitivity, and mental health has an impact on a women’s ability to continue to breastfeed (Bell et al. Citation2012). Dozier, Nelson, and Brownell (Citation2012) identified associated stress categories such as financial, traumatic, or emotional. Additionally, infant sleep and maternal fatigue can be a factor as it increases stress (Prendergast and James Citation2016). Intimate partner violence (domestic abuse) has also been shown to impact duration (Caleyachetty et al. Citation2019). Diwakar et al. (Citation2019) explored associations between armed conflict-related causalities in Iraq and a significant decline in breastfeeding.
Mesosystems (interpersonal)
Fathers and/or domestic relationships
Women have been shown to appreciate supportive partners and fathers’ preference has a positive influence (Felix Akpojene et al. Citation2020). Fathers who are sensitive to the mother’s needs consistently enable continued breastfeeding (Rempel et al. Citation2020). However, for the heterosexual couple, gender differences caused by the cultural constructs of masculinity have been seen as a barrier (Martínez-Plascencia, Rangel-Flores, and Rodríguez-Martinez Citation2017) and fathers can be unsure of their place in the feeding process (Merritt et al. Citation2019). Hounsome and Dowling (Citation2018) identified that whilst some fathers saw advantages for breastfeeding others felt continuing breastfeeding beyond infancy was abnormal. Juntereal and Spatz (Citation2020) also highlighted that for same sex mothers, the non-gestational parent is an essential support.
Grandparents
Successful breastfeeding is an acquired skill learnt via observing the practice of elder generations (Scelza and Hinde Citation2019). Karmacharya et al. (Citation2017) showed that when Grandmothers had the required knowledge, they had a positive impact on feeding practices. The generational influence can have both a positive and negative impact, depending on their own experience (Alianmoghaddam, Phibbs, and Benn Citation2018). Additionally, support from wider family circles have a strong role to play (Prendergast and James Citation2016).
Peers
Women benefit from social networks which affirm their breastfeeding practices (Quinn, Gallagher, and de Vries Citation2019). They seek this peer-to-peer support in a variety of ways; for example, by attending local breastfeeding groups (Kabakian-Khasholian et al. Citation2019) or targeted peer-to-peer support programs (Clark et al. Citation2018). These encourage positive social interactions, emotional support and health educational information which have a positive impact continuation (Afonso Bertoldo, Siqueira Boccolini, and Faerstein Citation2019). Women also seek peer support from online communities which reaffirms the norms of duration (Jackson and Hallam Citation2021).
Exosystems (community)
Public perception and representation
The role of the public and social stigma in the UK is highlighted (Boyer Citation2018). Sheehan, Gribble, and Schmied (Citation2019) found public breastfeeding is rarely observed and there is a view that women should adhere to certain social rules for it to be accepted. Rosen-Carole et al. (Citation2018) reports safety and privacy concerns when breastfeeding in public. Bresnahan et al. (Citation2019) found that stigma was communicated via negative attributions to illegal body exposure. However, Foss and Blake (Citation2019) found that positive media messages could help improve public attitude.
Returning to work
The return to work has been identified with early cessation (Dagher et al. Citation2016; Scott et al. Citation2019). There is a systematic review which reports a low-level evidence associated (Mangrio, Persson, and Bramhagen Citation2018). However, other studies report that women feel uncomfortable expressing at work (or school) (Clark and Price Citation2018), are not provided with space or time (Snyder et al. Citation2018) and found disapproval from colleagues needing to take breaks to express (Bresnahan et al. Citation2018). Additionally, women who do breastfeed for longer experience prolonged earning losses (Dinour and Szaro Citation2017). Employers and childcare providers have an important role in supporting continued breastfeeding (Ana María, Miguel, and Francisco José Citation2020; Lundquist et al. Citation2019).
Macrosystems (societal)
Ethnic group distinctions
Breastfeeding is rooted in an historical and cultural context. Ethnic differences have been identified in the initiation and duration of breastfeeding (Santorelli et al. Citation2013). In U.S research of African American women highlights an experience of racism, bias and discrimination when it comes to breastfeeding care, support and outcomes (Griswold et al. Citation2018; Robinson, Fial, and Hanson Citation2019). Whereas, Hispanic women been identified as having stronger ability to continue to breastfeed (Fryer et al. Citation2018). In stark contrast, however, UK research has identified higher breastfeeding rates among Black and Asian communities (Griffiths and Tate Citation2007). Therefore, there are variations unique to individual countries.
Religion
Burdette and Pilkauskas (Citation2012) sought to understand religious variations in breastfeeding behaviours and identified that mothers who frequently attend religious services are more likey to initiate breastfeeding. Laroia and Deeksha (Citation2006) highlight that for the Hindu community breastfeeding continues for most children beyond infancy. In a study completed in the USA, protestants were identifed as the religious group who were least likely to breastfeed then any other religious group (Stroope et al. Citation2018). Additionally, Bensaid (Citation2019) highlighted that the religious beliefs deeply shape Muslims’ breastfeeding culture and that breastfeeding is a fundamental Islamic human right.
National systems
Breastfeeding is a health-related behaviour less frequent within high-income countries (Victora et al. Citation2016). A longer duration of breastfeeding has been shown in the Middle East, Africa, and Southeast Asia (Scott et al. Citation2019). Factors such as variations in parental leave, childcare policies and government support have been highlighted as reasons (Galtry Citation2003; Lubold Citation2016, Citation2019). However, even breastfeeding rates within countries vary considerably. For example, China has previously reported a median age of six months for breastfeeding urban settings and eight months for those living in rural communities (Huang et al. Citation2012).
Chronosystems (change over time)
Inequality groups
There is a clear social divide in the duration of breastfeeding. For example, inadequate educational attainment and poor economic position are correlated with a shorter duration of breastfeeding (Ajami et al. Citation2018). Breastfeeding duration is additionally challenging for protected characteristic groups more at risk to the wider determinants of health (Bambra et al. Citation2010). For example, a study conducted Barros da Silva, Barbieri-Figueiredo, and Van Riper (Citation2019) identified additional challenges for mothers breastfeeding children with a learning disability. A case study identified further challenges for children on a child services safeguarding plan (Gribble and Gallagher Citation2014) and women in prison (Paynter & Snelgrove-Clarke, Citation2019). The sex of a child also has an influence on duration, however, both sexes were seen to have a disadvantage when different ethnic groups were investigated (Jayachandran and Kuziemko Citation2011; Shafer and Hawkins Citation2017).
Immigration
There are several studies which indicate that parents who have immigrated, to various countries, have a longer duration of breastfeeding (Dennis et al. Citation2019; Kersuzan, Tichit, and Thierry Citation2018; Rosenthal et al. Citation2019). There are also several studies which indicate that the acculturation of western norms for women immigrating to these countries negatively impacts breastfeeding duration (Bigman et al. Citation2018; Qianling, Katherine, and John Citation2018). McFadden, Atkin, and Renfrew (Citation2014) also identified that the intergenerational transmission of knowledge had been disrupted for Bangladeshi women who migrated to the UK. In a New York study, immigrated Chinese mothers, needed to negotiate with elders for breastfeeding, as sending infants back to China to be taken care of by grandparents was common (Lee and Brann Citation2015).
Historical context
The ancient hunter-gatherers, Egyptians, Greeks, and Romans are all thought to have had a communal approach to breastfeeding practices (Kramer and Veile Citation2018; Baumgartel, Sneeringer, and Cohen Citation2016). In the era of slavery, African mothers were forced to breastfeed the infants of the slave-owners, which disadvantaged their own children (West and Knight Citation2017). This reveals a historical experience of breastfeeding routed in exploitation. The legacy of this terrible atrocity is thought to be continuing to manifest among feelings associated with breastfeeding for black communities today (Louis-Jacques et al. Citation2020). Additionally, in industrialised countries, the advances in sanitation and the development of formula has resulted in a societal perception of low risk for formula use (Stuart-Macadam Citation2017). The retail value of the formula milk market is now estimated at 62.5 billion dollars (Statista Citation2020). This industry uses their resources for sophisticated marketing campaigns which seek to elicit emotional parental responses (Hastings et al. Citation2020).
This is despite the World Health Organisation (WHO Citation1981) implementing the International Code of Marketing of Breast-milk Substitutes over 40 years ago in response to the aggressive advertising being association with an increase in mortality, malnutrition and diarrhoea in infants, particularly within low-socioeconomic countries. However, the global adoption of the code into national law has never been fully realised and violations of the code are thought to be frequent and have virtually no legal consequences (Shenker Citation2018). Additionally, health-care professionals continue to be targeted by the industry (Hickman et al. Citation2021) and it is only very recently that the Royal College of Paediatrics and Child Health announced they would stop accepting funding from formula milk companies (Mayor Citation2019).
Discussion
The breastfeeding body of evidence has been applied to the Bronfenbrenner’s ecological system layers to demonstrate that a women’s ability to continue breastfeeding is shaped by a complex range of contexts. This synthesis highlights a spectrum of barriers and enablers from individual to global. Additionally, these layers interact and manipulate one another. For example, adversity and trauma is situated within the microsystems layer because of the direct impact on mental health. However, war exists at a society macrosystem layer. Additionally, a mother’s parental style might be shaped by several factors from wider systems layers such as family, peers, public perception and representation, religion and be embedded within a historical context of cultural parenting norms. This highlights the importance of understanding and being sensitive to the wider contexts which play a part in shaping women’s feeding practice. Therefore, whilst interventions which aim to increase a women’s education and health literacy may be useful for supporting a woman’s confidence in their abilities to breastfeed (Morrison, Glick, and Yin Citation2019) they do not consider how families absorb wider ideologies and translate them to each other. Additionally, the findings highlight the importance that peer-to-peer support plays for the continuation of breastfeeding. In an age of information, many women are turning to their peers on social media to inform their choices (Jackson and Hallam Citation2021). This could be of benefit when women do not receive the appropriate information needed from their health-care providers but it may also be counterproductive to breastfeeding behaviours. For example, breastfeeding during the pandemic was identified as essential (Williams et al. Citation2020). However, there has also been a proliferation of misinformation, confusion, and uncertainty in relation to COVID-19 and breastfeeding online (Israel-Ballard Citation2021). This reinforces the argument for social media platforms need to take a responsibility for removing misinformation which has detrimental effect on the health and wellbeing of its community (Naeem, Bhatti, and Khan Citation2021). And healthcare interventions (or online via an app) should be designed and utilise to provide reliable information and support for the virtual environment.
These findings presented in this review also highlight the way breastfeeding is situated varies immensely globally. These vast experiences mean any generalisations to individual groups must be considered with caution. However, global cultural differences such as in Western Europe and North America, have been described as ‘individualism’, whereas most other countries are described as ‘collectivism’ and this might explain a disparity (Triandis Citation2018). These findings show that breastfeeding requires a collective approach and responsibility for its success and the western’s focus on individual choice and freedom, places responsibility solely on the mother to feed her child. The expectations of good mothering, the society view of breast as sexual organ and that breastfeeding should hidden from view in public spaces are all key issues, which need to be addressed (Lee Citation2012, Citation2018; Whiley, Stutterheim, and Grandy Citation2020; Young Citation2020).
A women’s ability to continue breastfeeding also mean they need to do so in public spaces and whilst in employment. This means governments need to pass appropriate legislation, which protects all women, regardless of religious, cultural and national status. Perspectives from black feminist academics cannot be ignored when designing and delivering interventions because inequalities, discrimination, racism, intergenerational and historical trauma are crucial considerations (Jamil Citation2018; Johnson et al. Citation2021). These findings complement Snyder et al. (Citation2021) qualitative exploration, which similarly adapt a socio-ecological perspective and recommends hospital-community partnerships, family-centred education, and improved breastfeeding legislation as a way to support breastfeeding continuation. A limitation of this synthesis is that only English publications were included and therefore further global perspectives are needed. It should also be recognised that breastfeeding is predominantly viewed as an embodied experience of women. There is an increasing recognition that gender is separate to the biological sex assigned at birth (Mauvais-Jarvis et al. Citation2020). Therefore, sensitivity to the wider cultural and social needs, which interplay is necessary for inclusivity.
Conclusion
This narrative review is an important synthesis of evidence, situated within the ecological systems theory, to understand a mother’s ability to continue breastfeed. The review has demonstrated that breastfeeding, and any interventions targeted to support the initiation or continuation of it, must be viewed with an intersectional lens. Breastfeeding is an acquired skill which historically has been communally shared and learnt via observing practices from elders. However, the cultural normalisation of formula feeding means that the breastfeeding skills are no longer being acquired or passed through generations. Society needs to unlearn and collectively raise more awareness of this detrimental historical shift and begin to represent breastfeeding as the biological norm again if we are to enable its optimal benefits.
Declarations
There were no conflicts or competing interests for conducting this study.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Afonso Bertoldo, L. A., C. Siqueira Boccolini, and E. Faerstein. 2019. “Dimensions of Social Support and Breastfeeding Outcomes: The Pró-saúde Study [Article].” Dimensões do apoio social e prática de aleitamento materno: estudo pró-saúde 14 (Suppl. 1): 1–20.
- Ajami, M., M. Abdollahi, F. Salehi, W. Oldewage-Theron, and Y. Jamshidi-Naeini. 2018. “The Association between Household Socioeconomic Status, Breastfeeding, and Infants’ Anthropometric Indices.” International Journal of Preventive Medicine 9 (1, September): 89. doi:https://doi.org/10.4103/ijpvm.IJPVM_52_17.
- Alianmoghaddam, N., S. Phibbs, and C. Benn. 2018. “The Impact of Family Culture on Six Months Exclusive Breastfeeding: A Qualitative Study in New Zealand.” Breastfeeding Review 26 (1): 23–36.
- Ana María, L., B. Miguel, and P. Francisco José. 2020. “Lactation and Work: Managers’ Support for Breastfeeding Enhance Vertical Trust and Organizational Identification [Article].” Frontiers in Psychology 11: 18.
- Baethge, C., S. Goldbeck-Wood, and S. Mertens. 2019. “SANRA—a Scale for the Quality Assessment of Narrative Review Articles.” Research Integrity and Peer Review 4 (1): 1–7. doi:https://doi.org/10.1186/s41073-019-0064-8.
- Bai, D. L., D. Y. T. Fong, and M. Tarrant. 2015. “Previous Breastfeeding Experience and Duration of Any and Exclusive Breastfeeding among Multiparous Mothers [Report].” Birth 42 (1): 70. doi:https://doi.org/10.1111/birt.12152.
- Bambra, C., M. Gibson, A. Sowden, K. Wright, M. Whitehead, and M. Petticrew. 2010. “Tackling the Wider Social Determinants of Health and Health Inequalities: Evidence from Systematic Reviews.” Journal of Epidemiology & Community Health 64 (4): 284–291. doi:https://doi.org/10.1136/jech.2008.082743.
- Barros da Silva, R., M. D. C. Barbieri-Figueiredo, and M. Van Riper. 2019. “Breastfeeding Experiences of Mothers of Children with down Syndrome [Article].” Comprehensive Child & Adolescent Nursing 42 (4) (December): 250–264. doi:https://doi.org/10.1080/24694193.2018.1496493.
- Baulies, S., M. Cusido, F. Tresserra, F. Fargas, I. Rodriguez, B. Ubeda, C. Ara, and R. Fabregas. 2015. “Biological and Pathological Features in pregnancy-associated Breast Cancer: A Matched case-control Study.” European Journal of Gynaecological Oncology 36 (4): 420–423.
- Baumgartel, K. L., L. Sneeringer, and S. M. Cohen. 2016. “From Royal Wet Nurses to Facebook: The Evolution of Breastmilk Sharing.” Breastfeeding Review: Professional Publication of the Nursing Mothers‘ Association of Australia 24 (3): 25.
- Bell, L., M. Lacombe, F. Gallagher, M. Ferland, and M.-E. Couture. 2012. “The Factors Involved in the Decision to Stop Breastfeeding Early.” Soins. Pediatrie, puericulture 269: 39–45.
- Bell, L., A. Benoit, J. Simoneau-Roy, S. Blouin, and F. Gallagher. 2015. “Factors Associated with Breastfeeding Continuation in Young Canadian Mothers.” Sante publique (Vandoeuvre-les-Nancy, France) 27 (1): 7–15.
- Bensaid, B. 2019. “The Evolution of Spirituality, Religion and Health Publications: Yesterday, Today and Tomorrow.” Journal of Religion and Health 58 (1): 1. doi:https://doi.org/10.1007/s10943-018-00739-w.
- Bigman, G., A. V. Wilkinson, A. Pérez, and N. Homedes. 2018. “Acculturation and Breastfeeding among Hispanic American Women: A Systematic Review.” Maternal and Child Health Journal 22 (9): 1260–1277. doi:https://doi.org/10.1007/s10995-018-2584-0.
- Bjørset, V. K., C. Helle, E. R. Hillesund, and N. C. Øverby. 2018. “Socio-economic Status and Maternal BMI are Associated with Duration of breast-feeding of Norwegian Infants.” Public Health Nutrition 21 (8): 1465–1473. doi:https://doi.org/10.1017/S1368980017003925.
- Boyer, K. 2018. “The Emotional Resonances of Breastfeeding in Public: The Role of Strangers in Breastfeeding Practice.” Emotion, Space and Society 26: 33–40. doi:https://doi.org/10.1016/j.emospa.2016.09.002.
- Bresnahan, M., J. Zhuang, J. Anderson, Y. Zhu, J. Nelson, and X. Yan. 2018. “The ‘Pumpgate’ Incident: Stigma against Lactating Mothers in the US Workplace.” Women & Health 58 (4): 451–465. doi:https://doi.org/10.1080/03630242.2017.1306608.
- Bresnahan, M., Y. Zhu, J. Zhuang, and X. Yan. 2019. “‘He Wants A Refund because I’m Breastfeeding My Baby’: A Thematic Analysis of Maternal Stigma for Breastfeeding in Public.” Stigma and Health. doi:https://doi.org/10.1037/sah0000208.
- Bronfenbrenner, U. 1975. “The Ecology of Human Development in Retrospect and Prospect.”
- Bronfenbrenner, U. 1979. The Ecology of Human Development: Experiments by Nature and Design. U.S.A: Harvard university press.
- Burdette, A. M., and N. V. Pilkauskas. 2012 01 October 2012. “Maternal Religious Involvement and Breastfeeding Initiation and Duration.” American Journal of Public Health 102 (10): 1865–1868. doi:https://doi.org/10.2105/AJPH.2012.300737.
- Caleyachetty, R., O. A. Uthman, H. N. Bekele, R. Martín-Cañavate, D. Marais, J. Coles, B. Steele, R. Uauy, and P. Koniz-Booher. 2019. “Maternal Exposure to Intimate Partner Violence and Breastfeeding Practices in 51 low-income and middle-income Countries: A population-based cross-sectional Study.” PLoS Medicine 16 (10): 1–15. doi:https://doi.org/10.1371/journal.pmed.1002921.
- Clark, A., S. S. Baker, K. McGirr, and M. Harris. 2018. “Breastfeeding Peer Support Program Increases Breastfeeding Duration Rates among Middle- to High-Income Women.” Breastfeeding Medicine 13 (2): 112–115. doi:https://doi.org/10.1089/bfm.2017.0021.
- Clark, C., and K. Price. 2018. “Exploring the Role of Social Support in Understanding Barriers to Breastfeeding Practices for Adolescent Mothers in Western North Carolina: A Preliminary Study.” International Public Health Journal 10 (4): 333–342.
- Cohen, S. S., D. D. Alexander, N. F. Krebs, B. E. Young, M. D. Cabana, P. Erdmann, N. P. Hays, et al. 2018 12/01 December 2018. “Factors Associated with Breastfeeding Initiation and Continuation: A Meta-Analysis [Article].” The Journal of Pediatrics 203: 190–196. doi: https://doi.org/10.1016/j.jpeds.2018.08.008.
- Dagher, R. K., P. M. McGovern, J. D. Schold, and X. J. Randall. 2016. “Determinants of Breastfeeding Initiation and Cessation among Employed Mothers: A Prospective Cohort Study.” BMC Pregnancy and Childbirth 16 (1): 194. doi:https://doi.org/10.1186/s12884-016-0965-1.
- Dennis, C. L., R. Shiri, H. K. Brown, H. P. Santos, V. Schmied, and K. Falah‐Hassani. 2019. “Breastfeeding Rates in Immigrant and Non‐immigrant Women: A Systematic Review and Meta‐analysis.” Maternal & Child Nutrition 15 (3): N.PAG–N.PAG. doi:https://doi.org/10.1111/mcn.12809.
- Dettwyler, K. A. 2017. “A Time to Wean: The Hominid Blueprint for the Natural Age of Weaning in Modern Human Populations.” In Breastfeeding, 39–74. New York: Routledge.
- Dinour, L. M., and J. M. Szaro. 2017. “Employer-Based Programs to Support Breastfeeding among Working Mothers: A Systematic Review.” Breastfeeding Medicine: the Official Journal of the Academy of Breastfeeding Medicine 12 (3): 131–141. doi:https://doi.org/10.1089/bfm.2016.0182.
- Diwakar, V., M. Malcolm, and G. Naufal. 2019. “Violent Conflict and Breastfeeding: The Case of Iraq.” Conflict and Health 13 (1): 1–20.
- Dozier, A. M., A. Nelson, and E. Brownell. 2012. “The Relationship between Life Stress and Breastfeeding Outcomes among Low-Income Mothers [Article].” Advances in Preventive Medicine 2012: 1–10. doi:https://doi.org/10.1155/2012/902487.
- Faircloth, C. 2010. “‘If They Want to Risk the Health and well-being of Their Child, That’s up to Them’: Long-term Breastfeeding, Risk and Maternal Identity [Article].” Health, Risk & Society 12 (4): 357–367. doi:https://doi.org/10.1080/13698571003789674.
- Faircloth, C. 2017. “‘Natural’ Breastfeeding in Comparative Perspective: Feminism, Morality, and Adaptive Accountability.” Ethnos: Journal of Anthropology 82 (1, February): 19. doi:https://doi.org/10.1080/00141844.2015.1028562.
- Felix Akpojene, O., J. A. Blessing, Y. A. Kedir, G. R. Abdon, O. O. Akorede, E. U. Noel, K. E. Osita, and E. A. Kingsley, M. on Behalf of the Global, and C. Child Health Research. 2020. “Breastfeeding in the Community—How Can Partners/Fathers Help? A Systematic Review [Article].” International Journal of Environmental Research and Public Health 17 (2): 413.
- Foss, K. A., and K. Blake. 2019. ““It’s Natural and Healthy, but I Don’t Want to See It”: Using Entertainment-Education to Improve Attitudes toward Breastfeeding in Public.” Health Communication 34 (9): 919. doi:https://doi.org/10.1080/10410236.2018.1440506.
- Fryer, K., H. P. Santos Jr., C. Pedersen, and A. M. Stuebe. 2018. “The Hispanic Paradox: Socioeconomic Factors and Race/Ethnicity in Breastfeeding Outcomes.” Breastfeeding Medicine: the Official Journal of the Academy of Breastfeeding Medicine 13 (3): 174–180. doi:https://doi.org/10.1089/bfm.2017.0157.
- Galtry, J. 2003. “The Impact on Breastfeeding of Labour Market Policy and Practice in Ireland, Sweden, and the USA.” Social Science & Medicine 57 (1): 167–177. doi:https://doi.org/10.1016/S0277-9536(02)00372-6.
- García, A. L., S. Raza, A. Parrett, and C. M. Wright. 2013. “Nutritional Content of Infant Commercial Weaning Foods in the UK.” Archives of Disease in Childhood 98 (10): 793–797. doi:https://doi.org/10.1136/archdischild-2012-303386.
- Grainger, A., J. Joseph, and N. Sherring. 2015. “Parity, Breastfeeding, and the Subsequent Risk of Maternal Type 2 Diabetes.” British Journal of Healthcare Assistants 9 (8): 386–393. doi:https://doi.org/10.12968/bjha.2015.9.8.386.
- Gribble, K. D., and M. Gallagher. 2014. “Rights of Children in Relation to Breastfeeding in Child Protection Cases.” British Journal of Social Work 44 (2): 434–450. doi:https://doi.org/10.1093/bjsw/bcu004.
- Griffiths, L. J., and A. R. Tate. 2007. “Do Early Infant Feeding Practices Vary by Maternal Ethnic Group?” Public Health Nutrition 10 (9): 957–964. doi:https://doi.org/10.1017/S1368980007665513.
- Griswold, M. K., S. L. Crawford, D. J. Perry, S. D. Person, L. Rosenberg, Y. C. Cozier, and J. R. Palmer. 2018. “Experiences of Racism and Breastfeeding Initiation and Duration among First-Time Mothers of the Black Women’s Health Study [Original Paper].” Journal of Racial and Ethnic Health Disparities 5 (6): 1180. doi:https://doi.org/10.1007/s40615-018-0465-2.
- Hackman, N. M., E. W. Schaefer, J. S. Beiler, C. M. Rose, and I. M. Paul. 2015. “Breastfeeding Outcome Comparison by Parity.” Breastfeeding Medicine 10 (3): 156–162. doi:https://doi.org/10.1089/bfm.2014.0119.
- Härkönen, U. 2001. The Bronfenbrenner Ecological Systems Theory of Human Development
- Hastings, G., K. Angus, D. Eadie, and K. Hunt. 2020. “Selling Second Best: How Infant Formula Marketing Works.” Globalization and Health 16 (1). 1. doi:https://doi.org/10.1186/s12992-020-00597-w.
- Hickman, N., S. Morgan, H. Crawley, and M. Kerac. 2021. “Advertising of Human Milk Substitutes in United Kingdom Healthcare Professional Publications: An Observational Study.” Journal of Human Lactation 37 (4): 674–682. doi:https://doi.org/10.1177/08903344211018161.
- Hounsome, L., and S. Dowling. 2018. “‘The Mum Has to Live with the Decision Much More than the Dad’; a Qualitative Study of Men’s Perceptions of Their Influence on Breastfeeding decision-making [Article].” International Breastfeeding Journal 1: 1. doi:https://doi.org/10.1186/s13006-018-0145-1.
- Huang, L., G. Zeng, M. Li, L. Ran, K. Chen, X. Pang, and L. Yu. 2012. “Duration of Breastfeeding and Its Relevant Influencing Factors in Urban and Rural Areas of Chengdu.” Wei Sheng Yan Jiu= Journal of Hygiene Research 41 (5): 760.
- Huang, Y., F. R. Hauck, C. Signore, A. Yu, T. N. K. Raju, T. T. K. Huang, and S. B. Fein. 2013. “Influence of Bedsharing Activity on Breastfeeding Duration among US Mothers.” JAMA Pediatrics 167 (11): 1038–1044. doi:https://doi.org/10.1001/jamapediatrics.2013.2632.
- Hunegnaw, M. T., K. A. Gelaye, and B. M. Ali. 2018. “Factors Associated with the Time to Cessation of Breastfeeding among Mothers Who Have Index Children Aged Two to Three Years in Debre Markos, Northwest Ethiopia: A Retrospective Follow up Study.” BMC Pediatrics 18 (1): 77. doi:https://doi.org/10.1186/s12887-018-1012-3.
- Israel-Ballard, K. 2021. “Aligning Best Practices and Addressing Misinformation for Optimal Infant Feeding during the COVID-19 Pandemic.”
- Jackson, J. E., and J. Hallam. 2021. “Against All odds—why UK Mothers’ Breastfeeding beyond Infancy are Turning to Their International Peers for Emotional and Informative Support.” Health Care for Women International 42 (4–6): 739–755.
- Jama, N. A., A. Wilford, L. Haskins, A. Coutsoudis, L. Spies, and C. Horwood. 2018. “Autonomy and Infant Feeding decision-making among Teenage Mothers in a Rural and Urban Setting in KwaZulu-Natal, South Africa.” BMC Pregnancy and Childbirth 18 (1): 52. doi:https://doi.org/10.1186/s12884-018-1675-7.
- Jamil, N. A. 2018. “The Influence of Religious Belief and Sociocultural on Breastfeeding Practice: A Literature Review.” The Malaysian Journal of Nursing (MJN) 9 (4): 79–85.
- Jayachandran, S., and I. Kuziemko. 2011. “Why Do Mothers Breastfeed Girls Less than Boys? Evidence and Implications for Child Health in India* [Article].” Quarterly Journal of Economics 126 (3): 1485–1538. doi:https://doi.org/10.1093/qje/qjr029.
- Johnson, A. M., R. Menke, J. E. Handelzalts, K. Green, and M. Muzik. 2021. “Reimagining Racial Trauma as a Barrier to Breastfeeding versus Childhood Trauma and Depression among African American Mothers.” Breastfeeding Medicine 16 (6): 493–500. doi:https://doi.org/10.1089/bfm.2020.0304.
- Juntereal, N. A., and D. L. Spatz. 2020. “Breastfeeding Experiences of Same‐sex Mothers.” Birth: Issues in Perinatal Care 47 (1): 21–28. doi:https://doi.org/10.1111/birt.12470.
- Kabakian-Khasholian, T., H. Nimer, S. Ayash, F. Nasser, and M. Nabulsi. 2019. “Experiences with Peer Support for Breastfeeding in Beirut, Lebanon: A Qualitative Study.” PLoS ONE 14 (10): e0223687. doi:https://doi.org/10.1371/journal.pone.0223687.
- Kanhadilok, S., and J. M. McGrath. 2015. “An Integrative Review of Factors Influencing Breastfeeding in Adolescent Mothers.” Journal of Perinatal Education. Spring2015 24 2: 119. doi:https://doi.org/10.1891/1946-6560.24.2.119.
- Karmacharya, C., K. Cunningham, J. Choufani, and S. Kadiyala. 2017. “Grandmothers’ Knowledge Positively Influences Maternal Knowledge and Infant and Young Child Feeding Practices.” Public Health Nutrition 20 (11): 2114–2123. doi:https://doi.org/10.1017/S1368980017000969.
- Kersuzan, C., C. Tichit, and X. Thierry. 2018. “Breastfeeding Practices among Immigrants and Natives in France, from the ELFE Cohort [Article].” Population 73 (3): 545–566. 00324663 doi:https://doi.org/10.3917/pope.1803.0545.
- Kim, E., S. E. Hoetmer, Y. Li, and J. E. Vandenberg. 2013. “Relationship between Intention to Supplement with Infant Formula and Breastfeeding Duration [Original Paper].” Canadian Journal of Public Health: A Publication of the Canadian Public Health Association 104 (5): e388. doi:https://doi.org/10.17269/cjph.104.3898.
- Knio, A., A. Abdulrahman, B. Al-Isa, M. Shammout, N. Al-Nasser, and T. Mustafa. 2018. “Influences of Different Feeding Patterns on Cognitive Development of Infants Aged 12 and 24 Months in Primary Health Care Clinics, Nurseries and Public Parks.” Arab Journal of Nutrition & Exercise 3 (1, January): 1.
- Koplin, J., and K. Allen. 2013. “Optimal Timing for Solids introduction–why are the Guidelines Always Changing?” Clinical & Experimental Allergy 43 (8): 826–834. doi:https://doi.org/10.1111/cea.12090.
- Kramer, K. L., and A. Veile. 2018 01 September 2018. “Infant Allocare in Traditional Societies.” Physiology & Behavior 193: 117–126. doi:https://doi.org/10.1016/j.physbeh.2018.02.054.
- Laroia, N., and S. Deeksha. 2006. “The Religious and Cultural Bases for Breastfeeding Practices among the Hindus.” Breastfeeding Medicine 1 (2): 94–98. doi:https://doi.org/10.1089/bfm.2006.1.94.
- Lee, R. 2012. “Breastfeeding and Constraints on Mothers’ Agency.” Journal of the Motherhood Initiative for Research & Community Involvement 3 (2): 93.
- Lee, A., and L. Brann. 2015. “Influence of Cultural Beliefs on Infant Feeding, Postpartum and Childcare Practices among Chinese-American Mothers in New York City [Original Paper].” Journal of Community Health: The Publication for Health Promotion and Disease Prevention 40 (3): 476. doi:https://doi.org/10.1007/s10900-014-9959-y.
- Lee, R. 2018. “Breastfeeding Bodies: Intimacies at Work.” Gender, Work & Organization 25 (1): 77–90. doi:https://doi.org/10.1111/gwao.12170.
- Levinienė, G., E. Tamulevičienė, J. Kudzytė, A. Petrauskienė, A. Zaborskis, I. Aželienė, and L. Labanauskas. 2013. “Factors Associated with Breastfeeding Duration.” Medicina (Kaunas, Lithuania) 49 (9): 415–421.
- Logan, C., T. Zittel, S. Striebel, F. Reister, H. Brenner, D. Rothenbacher, and J. Genuneit. 2016. “Changing Societal and Lifestyle Factors and Breastfeeding Patterns over Time [Article].” Pediatrics 137 (5, May): 1–10. doi:https://doi.org/10.1542/peds.2015-4473.
- Louis-Jacques, A. F., S. L. Marhefka, J. Brumley, E. J. Schafer, T. I. Taylor, A. J. Brown, T. A. Livingston, D. L. Spatz, and E. M. Miller. 2020. “Historical Antecedents of Breastfeeding for African American Women: From the Pre-Colonial Period to the Mid-Twentieth Century.” Journal of Racial and Ethnic Health Disparities 7 (5): 1003–1012.
- Lubold, A. M. 2016. “Breastfeeding and Employment: A Propensity Score Matching Approach [Article].” Sociological Spectrum 36 (6): 391–405. doi:https://doi.org/10.1080/02732173.2016.1227286.
- Lubold, A. M. 2019. “Historical-qualitative Analysis of Breastfeeding Trends in Three OECD Countries.” International Breastfeeding Journal 14 (1): 1–12.
- Lucas, P. J., J. Baird, L. Arai, C. Law, and H. M. Roberts. 2007. “Worked Examples of Alternative Methods for the Synthesis of Qualitative and Quantitative Research in Systematic Reviews.” BMC Medical Research Methodology 7 (1): 4. doi:https://doi.org/10.1186/1471-2288-7-4.
- Lundquist, A., B. A. McBride, S. M. Donovan, and A. Kieffer. 2019. “An Exploratory Look at the Role of Childcare Providers as a Support and Resource for Breastfeeding Mothers.” Breastfeeding Medicine 14 (5): 313–319. doi:https://doi.org/10.1089/bfm.2018.0091.
- Mangrio, E., K. Persson, and A. C. Bramhagen. 2018. “Sociodemographic, Physical, Mental and Social Factors in the Cessation of Breastfeeding before 6 Months: A Systematic Review.” Scandinavian Journal of Caring Sciences 32 (2): 451–465. doi:https://doi.org/10.1111/scs.12489.
- Martínez-Plascencia, U., Y. Y. Rangel-Flores, and M. E. Rodríguez-Martinez. 2017. “Maternal Breastfeeding, Alone or as A Couple? A Study on the Experiences of Reconfiguration of Bodies, Roles, and Daily Routines in Mexican Mothers and Fathers.” Cadernos de Saúde Pública 33 (9): e00109616.
- Mauvais-Jarvis, F., N. B. Merz, P. J. Barnes, R. D. Brinton, -J.-J. Carrero, D. L. DeMeo, G. J. De Vries, C. N. Epperson, R. Govindan, and S. L. Klein. 2020. “Sex and Gender: Modifiers of Health, Disease, and Medicine.” The Lancet 396 (10250): 565–582.
- Mayor, S. 2019. “Royal College Stops Taking Funding from Formula Milk Firms.” British Medical Journal Publishing Group 364 (1743). doi:https://doi.org/10.1136/bmj.l743.
- McFadden, A., K. Atkin, and M. J. Renfrew. 2014. “The Impact of Transnational Migration on Intergenerational Transmission of Knowledge and Practice Related to Breast Feeding.” Midwifery 30 (4): 439–446. doi:https://doi.org/10.1016/j.midw.2013.04.012.
- Merritt, R., M. Vogel, P. Ladbury, and S. Johnson. 2019 January23. “A Qualitative Study to Explore Fathers’ Attitudes Towards Breastfeeding in South West England.” Primary Health Care Research & Development. 20th ed. Vol. E24. N.PAG. UK: Cambridge University Press. doi:https://doi.org/10.1017/S1463423618000877.
- Morrison, A. K., A. Glick, and H. S. Yin. 2019. “Health Literacy: Implications for Child Health.” Pediatrics in Review 40 (6): 263–277. doi:https://doi.org/10.1542/pir.2018-0027.
- Mortensen, K., and S. Tawia. 2013. “Sustained Breastfeeding.” Breastfeeding Review 21 (1): 22–34.
- Naeem, S. B., R. Bhatti, and A. Khan. 2021. “An Exploration of How Fake News Is Taking over Social Media and Putting Public Health at Risk.” Health Information & Libraries Journal 38 (2): 143–149. doi:https://doi.org/10.1111/hir.12320.
- Newby, R. M., and P. S. W. Davies. 2016. “Why Do Women Stop breast-feeding? Results from a Contemporary Prospective Study in a Cohort of Australian Women.” European Journal of Clinical Nutrition 70 (12): 1428–1432. doi:https://doi.org/10.1038/ejcn.2016.157.
- Nuampa, S., F. Tilokskulchai, N. Sinsuksai, C. L. Patil, and W. Phahuwatanakorn. 2018 10 October-December 2018. “Breastfeeding Experiences among Thai Adolescent Mothers: A Descriptive Qualitative Study.” Pacific Rim International Journal of Nursing Research 22 (4):288.
- Nuampa, S., F. Tilokskulchai, C. L. Patil, N. Sinsuksai, and W. Phahuwatanakorn. 2019. “Factors Related to Exclusive Breastfeeding in Thai Adolescent Mothers: Concept Mapping Approach.” Maternal and Child Nutrition(2) 15 (2): e12714. doi:https://doi.org/10.1111/mcn.12714.
- Oddy, W. H., M. Robinson, G. E. Kendall, J. Li, S. R. Zubrick, and F. J. Stanley. 2011. “Breastfeeding and Early Child Development: A Prospective Cohort Study.” Acta Paediatrica 100 (7): 992–999. doi:https://doi.org/10.1111/j.1651-2227.2011.02199.x.
- Odom, E. C., R. Li, K. S. Scanlon, C. G. Perrine, and L. Grummer-Strawn. 2013. “Reasons for Earlier than Desired Cessation of Breastfeeding.” Pediatrics 131 (3): e726–e732. doi:https://doi.org/10.1542/peds.2012-1295.
- Page, M. J., J. E. McKenzie, P. M. Bossuyt, I. Boutron, T. C. Hoffmann, C. D. Mulrow, L. Shamseer, J. M. Tetzlaff, E. A. Akl, and S. E. Brennan. 2021. “The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews.” Bmj 372 (1): 1–11.
- Pang, W. W., J. Y. Bernard, G. Thavamani, Y. H. Chan, D. Fok, S.-E. Soh, M. C. Chua, et al. 2017. “Direct Vs. Expressed Breast Milk Feeding: Relation to Duration of Breastfeeding.” Nutrients 9 (6): 547. doi:https://doi.org/10.3390/nu9060547.
- Paynter, M. J., and E. Snelgrove-Clarke. 2019. “'Breastfeeding in Public' for Incarcerated Women: The Baby-Friendly Steps.” International Breastfeeding Journal 14 (1): 1–8.
- Peters, M. D., C. M. Godfrey, H. Khalil, P. McInerney, D. Parker, and C. B. Soares. 2015. “Guidance for Conducting Systematic Scoping Reviews.” JBI Evidence Implementation 13 (3): 141–146.
- Prendergast, E., and J. James. 2016. “Engaging Mothers: Breastfeeding Experiences Recounted (EMBER). A Pilot Study.” Breastfeeding Review 24 (2): 11–19.
- Qianling, Z., M. Y. Katherine, and M. K. John. 2018. “Infant Feeding Practices in China and Ireland: Ireland Chinese Mother Survey [Article].” Frontiers in Public Health. doi:https://doi.org/10.3389/fpubh.2018.00351.
- Quinn, E. M., L. Gallagher, and J. de Vries. 2019 01 November 2019. “A Qualitative Exploration of Breastfeeding Support Groups in Ireland from the Women’s Perspectives [Article].” Midwifery 78: 71–77. doi:https://doi.org/10.1016/j.midw.2019.08.001.
- Rempel, J. K., L. A. Rempel, D. T. P. Hoa, L. T. Vui, and T. K. Long. 2020 03 March-April 2020. “Parenting Teamwork: The Impact of a Fathering Intervention on Mothers and Infants in Vietnam [Article].” Child Development 91 (2): e345–e364. doi:https://doi.org/10.1111/cdev.13244.
- Robinson, K., A. Fial, and L. Hanson. 2019. “Racism, Bias, and Discrimination as Modifiable Barriers to Breastfeeding for African American Women: A Scoping Review of the Literature [Report].” Journal of Midwifery & Women’s Health 64 (6): 734. doi:https://doi.org/10.1111/jmwh.13058.
- Rosen-Carole, C., K. Allen, M. Fagnano, A. Dozier, and J. Halterman. 2018. “Mothers’ Concerns for Personal Safety and Privacy while Breastfeeding: An Unexplored Phenomenon.” Breastfeeding Medicine 13 (3): 181–188. doi:https://doi.org/10.1089/bfm.2017.0187.
- Rosenthal, A., S. B. Oliveira, U. Madubuko, H. Tanuos, J. Schwab, and I. M. Monteiro. 2019 01 April 2019. “Effects of Immigration on Infant Feeding Practices in an Inner City, Low Socioeconomic Community [Article].” Journal of the National Medical Association 111 (2): 153–157. doi:https://doi.org/10.1016/j.jnma.2018.07.006.
- Rudzik, A. E. F. 2012. “The Experience and Determinants of First-Time Breast-Feeding Duration among Low-Income Women from São Paulo, Brazil.” Current Anthropology 53 (1, February): 108. doi:https://doi.org/10.1086/663693.
- Santorelli, G., E. Petherick, D. Waiblinger, B. Cabieses, and L. Fairley. 2013. “Ethnic Differences in the Initiation and Duration of Breast Feeding–Results from the B Orn in B Radford Birth Cohort Study.” Paediatric and Perinatal Epidemiology 27 (4): 388–392. https://onlinelibrary.wiley.com/doi/abs/https://doi.org/10.1111/ppe.12052
- Scelza, B. A., and K. Hinde. 2019. “Crucial Contributions: A Biocultural Study of Grandmothering during the Perinatal Period [Original Paper].” Human Nature: An Interdisciplinary Biosocial Perspective 30 (4): 371. doi:https://doi.org/10.1007/s12110-019-09356-2.
- Scott, J. A., C. Tsz Ying, and W. H. Oddy. 2012. “Food Variety at 2 Years of Age Is Related to Duration of Breastfeeding.” Nutrients 4 (10): 1464–1474. doi:https://doi.org/10.3390/nu4101464.
- Scott, J., E. Ahwong, G. Devenish, D. Ha, and L. Do. 2019. “Determinants of Continued Breastfeeding at 12 and 24 Months: Results of an Australian Cohort Study.” International Journal of Environmental Research and Public Health 16 (20): 3980. doi:https://doi.org/10.3390/ijerph16203980.
- Shafer, E., and S. Hawkins. 2017. “The Impact of Sex of Child on Breastfeeding in the United States.” Maternal & Child Health Journal 21 (11): 2114–2121. doi:https://doi.org/10.1007/s10995-017-2326-8.
- Sheehan, A., K. Gribble, and V. Schmied. 2019. “It’s Okay to Breastfeed in Public but.” International Breastfeeding Journal 14 (1, November 06): N.PAG. doi:https://doi.org/10.1186/s13006-019-0216-y.
- Shenker, N. S. 2018. “The Resurgent Influence of Big Formula.” British Medical Journal Publishing Group k3577. doi:https://doi.org/10.1136/bmj.k3577.
- Snyder, K., K. Hansen, S. Brown, A. Portratz, K. White, and D. Dinkel. 2018. “Workplace Breastfeeding Support Varies by Employment Type: The Service Workplace Disadvantage.” Breastfeeding Medicine 13 (1): 23–27. doi:https://doi.org/10.1089/bfm.2017.0074.
- Snyder, K., E. Hulse, H. Dingman, A. Cantrell, C. Hanson, and D. Dinkel. 2021. “Examining Supports and Barriers to Breastfeeding through a socio-ecological Lens: A Qualitative Study.” International Breastfeeding Journal 16 (1): 52. doi:https://doi.org/10.1186/s13006-021-00401-4.
- Spaniol, A. M., T. H. M. da Costa, G. A. Bortolini, and M. B. Gubert. 2020. “Breastfeeding Reduces ultra-processed Foods and Sweetened Beverages Consumption among Children under Two Years Old.” BMC Public Health 20 (1, March 14): 1. doi:https://doi.org/10.1186/s12889-020-8405-6.
- Statista. 2020. “Retail Value of the Baby Milk Formula Market Worldwide in 2010 and 2020.” https://www.statista.com/statistics/719436/global-market-size-baby-formula/
- Stroope, S., H. M. Rackin, J. L. Stroope, and J. E. Uecker. 2018. “Breastfeeding and the Role of Maternal Religion: Results from a National Prospective Cohort Study.” Annals of Behavioral Medicine 52 (4): 319–330. doi:https://doi.org/10.1093/abm/kax013.
- Stuart-Macadam, P. 2017. Breastfeeding: Biocultural Perspectives. New York: Routledge.
- Supannee, K., N. L. McCain, J. M. McGrath, N. Jallo, S. K. Price, and C. Chiaranai. 2016. “Factors Associated with Exclusive Breastfeeding through Four Weeks Postpartum in Thai Adolescent Mothers.” The Journal of Perinatal Education 25 (3): 150. doi:https://doi.org/10.1891/1058-1243.25.3.150.
- Susiloretni, K. A., H. Hadi, Y. S. Prabandari, Y. S. Soenarto, and S. A. Wilopo. 2015. “What Works to Improve Duration of Exclusive Breastfeeding: Lessons from the Exclusive Breastfeeding Promotion Program in Rural Indonesia.” Maternal and Child Health Journal 19 (7): 1515–1525. doi:https://doi.org/10.1007/s10995-014-1656-z.
- Triandis, H. C. 2018. Individualism and Collectivism. New York: Routledge.
- Tudge, J. R. H., I. Mokrova, B. E. Hatfield, and R. B. Karnik. 2009. “Uses and Misuses of Bronfenbrenner’s Bioecological Theory of Human Development.” Journal of Family Theory & Review 1 (4): 198–210. doi:https://doi.org/10.1111/j.1756-2589.2009.00026.x.
- Victora, C. G., R. Bahl, A. J. Barros, G. V. França, S. Horton, J. Krasevec, S. Murch, M. J. Sankar, N. Walker, and N. C. Rollins. 2016. “Breastfeeding in the 21st Century: Epidemiology, Mechanisms, and Lifelong Effect.” The Lancet 387 (10017): 475–490. doi:https://doi.org/10.1016/S0140-6736(15)01024-7.
- Weaver, J. M., T. J. Schofield, and L. M. Papp. 2018. “Breastfeeding Duration Predicts Greater Maternal Sensitivity over the Next Decade.” Developmental Psychology 54 (2): 220–227. doi:https://doi.org/10.1037/dev0000425.
- West, E., and R. J. Knight. 2017. “Mothers’ Milk: Slavery, Wet-Nursing, and Black and White Women in the Antebellum South.” Journal of Southern History 83 (1): 37–68. doi:https://doi.org/10.1353/soh.2017.0001.
- Whiley, L. A., S. Stutterheim, and G. Grandy. 2020. “Breastfeeding,‘tainted’love, and Femmephobia: Containing the ‘Dirty’performances of Embodied Femininity.” Psychology & Sexuality 13 (1): 101–114.
- Whitehouse, A. J. O., M. Robinson, J. Li, and W. H. Oddy. 2011. “Duration of Breast Feeding and Language Ability in Middle Childhood [Article].” Paediatric & Perinatal Epidemiology 25 (1): 44–52. doi:https://doi.org/10.1111/j.1365-3016.2010.01161.x.
- WHO. 1981. International Code of Marketing of breast-milk Substitutes. The Netherlands: World Health Organization.
- WHO. 2003. “Implementing the Global Strategy for Infant and Young Child Feeding: Geneva, 3-5 February 2003: Meeting Report.” World Health Organization.
- WHO. 2019. “Breastfeeding.” World Health Organization. https://www.who.int/topics/breastfeeding/en/
- Wiklund, P., L. Xu, A. Lyytikäinen, J. Saltevo, Q. Wang, E. Völgyi, E. Munukka, S. Cheng, M. Alen, and S. Keinänen-Kiukaanniemi. 2012. “Prolonged breast-feeding Protects Mothers from later-life Obesity and Related cardio-metabolic Disorders.” Public Health Nutrition 15 (1): 67–74. doi:https://doi.org/10.1017/S1368980011002102.
- Williams, J., L. Namazova-Baranova, M. Weber, M. Vural, J. Mestrovic, A. Carrasco-Sanz, J. Breda, N. Berdzuli, and M. Pettoello-Mantovani. 2020. “The Importance of Continuing Breastfeeding during Coronavirus Disease-2019: In Support of the World Health Organization Statement on Breastfeeding during the Pandemic.” The Journal of Pediatrics 223: 234. doi:https://doi.org/10.1016/j.jpeds.2020.05.009.
- Young, C. 2020. “Theorizing ‘Deviant’embodiment and the Act of Breastfeeding.” Journal of Gender Studies 29 (6): 685–693. doi:https://doi.org/10.1080/09589236.2020.1771291.
