
ABSTRACT
Over half of the world’s mortality is associated with chronic diseases. Living with chronic diseases can significantly affect patients’ quality of life. The daily management of these diseases falls mostly on patients themselves. Self-management interventions have become increasingly used as a complementary intervention to treatment and care. The Chronic Disease Self-Management Programme (CDSMP) is the most widespread self-management intervention. It aims to empower patients and provide them with the skills to manage their disease and prevent complications. A locally adapted CDSMP was piloted in the Republic of Moldova in 2018/2019 in five villages across three rural districts. In five groups led by peer facilitators, 63 participants were enrolled in the programme. Four participants were lost to follow-up. To evaluate the intervention, we used the Self-Efficacy for Managing Chronic Diseases six-item scale questionnaire with participants before and after the programme, along with a questionnaire to assess satisfaction with the programme. Additionally, we conducted a focus group discussion (FGD) with the 10 programme facilitators. We found that, not only did participants’ self-efficacy significantly increase between baseline and follow-up (from mean score of 5.3 to 8.3; t(58) = -12.2, p < 0.001), they also improved their knowledge on every individual item on how to manage a chronic disease (p < 0.001). Participants’ satisfaction was high, with 96% of respondents satisfied with content, format and delivery elements of the intervention. Hence, we believe the CDSMP is locally acceptable and effective at least in the short-term, and offers promises for scale-up in the Republic of Moldova.
Introduction
It is estimated that 17 million people die before age 70 every year due to non-communicable diseases (NCDs) and 86% of these premature deaths occur in low- and middle-income countries. Many NCD risk factors are related to lifestyle, such as inadequate diet, smoking, alcohol consumption, or a low level of physical activity (GBD Citation2015Risk Factors Collaborators 2016).
In Moldova, 34.8% of the population has high blood pressure, out of which 50% are not under treatment (WHO Citation2022b). An estimated 27.7% of the population has raised cholesterol and 31.8% of the population aged 18 to 69 years had three or more cardiovascular risk factors. Moldova has a high prevalence of tobacco consumption, particularly among men (48.9% versus 6.3% for women). Alcohol consumption, and especially heavy episodic drinking, is reported by 24.5% of men.
In recent years, Moldova has made significant progress to reform its health system. The country strengthened its policy environment for the prevention, control and management of NCDs, by introducing a tobacco taxation policy in 2018, by generating evidence with the 2018 salt intake survey, and by building the capacity of public health institutions to align practices with the WHO Package of Essential NCD (PEN) interventions (WHO Citation2018). Core individual services for NCD control, and the management of acute NCD events, are available across Moldova although there is room for improvement in coverage and quality of service (Skarphedinsdottir et al. Citation2014).
Living with chronic conditions can negatively affect patients’ quality of life and represent a serious economic burden at individual and societal levels (Essue et al. Citation2017; Heyworth et al. Citation2009). WHO recommends self-care interventions as innovative strategies to go beyond a conventional health sector response and to address challenges in accessing quality healthcare and reaching universal health coverage (UHC) (WHO Citation2022c). WHO defines self-care as ‘the ability of individuals, families and communities to promote health, prevent disease, maintain health, and to cope with illness and disability with or without the support of a health worker’ (WHO Citation2022c). WHO recognizes that self-management interventions are an essential part of self-care for long-term health condition (WHO Citation2021). Self-management can be defined as the ‘tasks and skills related to coping with the illness and growing as a person, as well as to transitioning from a focus on the illness needs to integrating the illness into the context of the individual’s life’ (Schulman-Green et al. Citation2012). Although its effectiveness varies depending on factors such as health condition, type of intervention and setting (K. Lorig Citation2014; O’Connell, Mc Carthy, and Savage Citation2018), self-management support has been shown to improve patient-level outcomes such as health status, functional status, satisfaction or quality of life among others (Donald et al. Citation2018; Reynolds et al. Citation2018; Vas et al. Citation2017).
Self-management includes a wide range of approaches (Miller et al. Citation2015; Schulman-Green et al. Citation2012; Van de Velde et al. Citation2019). Among the existing self-management programmes, Stanford’s Chronic Disease Self-Management Programme (CDSMP) is among the most widely implemented and researched worldwide (Self-Management Resource Center Citation2023). The CDSMP was developed at Stanford University School of Medicine and is organized through the Self-Management Resource Center. It aims to increase patients’ level of ‘self-efficacy’, that is, the ‘cognitive process where, through environmental influence and social influence, individuals learn new behaviors that affect their ability to improve future events’ (Bandura Citation1977). Increasing self-efficacy can improve the health outcomes and quality of life of people living with chronic diseases (Lorig Citation2014; Peters et al. Citation2019). The delivery of the CDSMP follows a structured organization and curriculum as it is argued that programme implementation fidelity enhances effectiveness (Self-Management Resource Center Citation2022a). Typically, it is delivered as a six to seven week, peer-led workshop involving interactive discussions and practical exercises. Workshop facilitators are usually patients themselves having successfully completed training with various degrees of certification (e.g. Leader trainer, Master trainer). The CDSMP was implemented globally in relation to several chronic conditions including chronic pain, diabetes, severe mental health problems, and as a post cancer programme (Self-Management Resource Center Citation2023).
CDSMP has shown acceptability and effectiveness across diverse cultural settings (Swerissen et al. Citation2006; Dongbo et al. Citation2006; Self-Management Resource Center Citation2022b). Across Europe, the CDSMP was first introduced in the UK in 2002 as the Expert Patient Programme (Tattersall Citation2002) and spread to several countries including Denmark where it has been implemented since 2006 by the Danish Committee for Health Education (pers. comm., 2018). In Switzerland, the CDSMP was implemented as the EVIVO programme (Haslbeck et al. Citation2015).
In 2016, the Swiss Agency for Development Cooperation (SDC) in collaboration with the Moldovan Ministry of Health, launched the Healthy Life Project to improve the health status of the population, especially in rural areas, through the reduction of the burden of NCDs (SDC Healthy Life project Citation2023). As part of the innovations introduced by this project, we piloted the first CDSMP in the Republic of Moldova and the results of the evaluation are presented in this article.
Materials and methods
Participants’ characteristics
A total of 63 individuals were enrolled in the CDSMP intervention, out of which 58 (92%) were female. By the end of the programme, four participants dropped out, either because they travelled abroad, or because the programme did not meet their expectations. Hence, a total of 59 participants completed the programme. The age of participants ranged from 49 to 72 years, with a majority being in the range 55 to 65 years. They were all pensioners and had at least one chronic condition, with the most frequent diseases being hypertension, diabetes, arthrosis and gastritis. Participants were recruited from five villages across three districts: Peresecina and Susleni villages in the Orhei district, Boşcana, and Ohrincea villages in the Criuleni district, and Mărăndeni village in the Falesti district. No other demographic data were collected.
Ten facilitators professionally active in the same communities were recruited to moderate the CDSMP workshops: five were nurses, two were librarians, two were school teachers, and one was a psychologist. The age range of the facilitators was 43 to 66 years. Seven of them had a chronic disease, with the most frequent conditions being type-2 diabetes, post cancer fatigue, and respiratory disease. No sampling strategy was applied as all the participants who finished the intervention and all the facilitators were recruited for the evaluation.
Procedures
The Danish Committee for Health Education (DCHE) provided international technical expertise to adapt the CDSMP to the Moldovan context in a programme named ‘Programme ABC (Autogestionarea Bolilor Cronice)’, including by assessing the feasibility of the pilot through site visits and interviews with local stakeholders. Within the local project team, an experienced Moldovan psychologist was capacitated to be a Master trainer on the Swiss EVIVO curriculum for self-management. The cultural adaptation of the EVIVO curriculum to the Moldovan context was done in two stages. Firstly, the Moldovan Master Trainer reviewed the EVIVO manual to ensure that all the concepts where culturally understandable in the Moldovan context. Secondly, a professional translator translated the manual in Romanian and Russian languages, and the Master Trainer revised the two translations for accuracy of language and content.
The DCHE expert and the Moldovan Master trainer delivered a four-day training of the CDSMP programme to 15 facilitators. Based on their performance during the training, 10 were selected to conduct the program and the remaining five were kept on stand-by in case replacements werenecessary. In parallel, awareness-raising communication on CDSMP was conducted with a range of stakeholders in the Republic of Moldova to clarify the approach and ensure buy-in by national and local partners.
The Moldovan CDSMP intervention was designed as a six-week programme, with weekly group meetings of 12 participants each, facilitated by two trained facilitators from the same rural communities. A total of five CDSMP workshops were conducted between March and April 2018. Activities were held on weekends to ensure the presence of as many participants as possible. A key feature of the weekly group discussions were individual participants’ commitments towards small lifestyle changes through personal action plans.
Several measures were implemented throughout the intervention to ensure fidelity. Firstly, the DCHE expert provided regular technical inputs to the design and implementation of the intervention, and co-animated the facilitators’ training. Secondly, the Master trainer performed at least one non-participant observation visit in each of the village workshops, followed by a debriefing conversation with the facilitators after the workshop, to ensure that the programme was delivered according to the standard. Finally, the Master trainer was in regular communication with the facilitators to answer their questions as they arose.
Materials
Using mixed methods in the frame of a convergent, parallel design, this pilot CDSMP was evaluated during May 2019 to assess the acceptability of the intervention and its impact on patients. To measure changes in programme participants’ self-efficacy, we administered the Stanford Self-Efficacy for Managing Chronic Diseases (SEMCD) (Lorig Citation2014; Ritter and Lorig Citation2014; Self-Management Resource Center Citation2023) scale. This questionnaire was developed by a group of experts from Stanford University School of Medicine. The SEMCD scale includes six items that cover several domains that are common across several chronic diseases such as symptom control, role function, emotional functioning and communicating with physicians (SMRC, undated). An investigation of the psychometric properties of the English and Spanish scale by Ritter and Lorig demonstrated the reliability and validity of the instrument. For the purpose of this intervention (Ritter and Lorig Citation2014), the English scale was translated into Romanian by a professional translator and culturally adapted in discussions between the Master trainer and the translator. The psychometric properties of the Romanian scale were not assessed.
Participants were asked to fill in the questionnaire on paper before the start of the intervention and one month after the intervention. They were instructed to select their level of confidence ranging from 1 (‘not confident at all’) to 10 (‘totally confident’) in response to questions concerning each of the six items. For the analysis, a paired-samples t-test was conducted to compare the participants’ self-efficacy score before and after the intervention. To create a general picture of data distribution, data screening was performed (Skewness and Kurtosis).
In addition, one month after the intervention, we asked patients to respond to a satisfaction questionnaire with closed-ended questions to explore their perceptions and experience with the content and delivery format of the intervention. The questionnaire was adapted from an instrument developed by the DCHE and translated into Romanian (see Appendix 1). It consisted of 10 questions which covered the most important aspects of the program such as how participants learned to set goals that can be achieved, the relevance of the program and their overall satisfaction. Data from the satisfaction questionnaire was descriptively analyzed.
Lastly, after the intervention, we conducted a 2.5 hour focus group discussion (FGD) with the 10 program facilitators using a semi-structured interview guide. The goal was to collect the facilitators’ experience and insights on the workshop dynamics with participants, including relevance and acceptability of the curriculum content; and assessments of participants’ engagement with behavior change goals through individual action plans. The facilitators’ opinions on acceptability of the intervention and engagement of participants provided an additional perspective on the intervention performance, and was used in the analysis for triangulation with the self-reported measures of actual participants. A local researcher audio-recorded the FGD and took written field notes on-site. Finally, the researcher conducted a thematic analysis of detailed written notes from the audio record, in close collaboration with the Master trainer.
Results
Self-efficacy to managing chronic disease (SEMCD) six-item scale
Concerning the self-efficacy score, we collected responses from 63 participants at baseline and 59 at follow-up; four participants were lost to follow-up. The mean score was significantly higher at follow-up (8.3, SD = 1.1) than at baseline ((5.3, SD = 1.7), t(58) = −12.2, p < 0.001). Additionally, we found that, between baseline and follow-up, there was also a significant increase in the mean score of every individual item of the self-efficacy score questionnaire (p < 0.001; ), meaning that participants improved their level of confidence in each domain of chronic disease self-management (fatigue, pain, emotions, symptoms management, functional ability, coping).
Figure 1. Pre- and post-intervention self-efficacy scores for each of the six items of the scale with standard deviations.

Satisfaction questionnaire
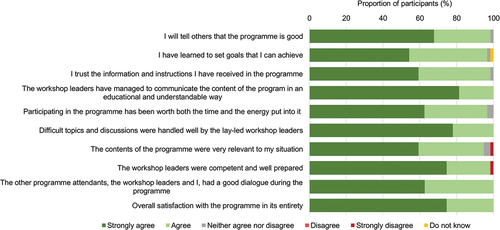
The satisfaction questionnaire was completed by 59 participants. In general, participants’ satisfaction was high, with 96% of respondents satisfied with content, format and delivery elements of the intervention (). One participant expressed dissatisfaction with the relevance of the content of the program, and the competence and preparedness of workshop facilitators.
Figure 2. Proportion of participants (%) expressing levels of agreement with the 10 statements of the satisfaction questionnaire.
Focus group discussions
Two main themes emerged from the FGD with the 10 CDSMP program facilitators: (i) acceptability and understanding by participants and facilitators of the CDSMP approach, methodology and content of the curriculum, and (ii) patients’ engagement with individual action plans for small lifestyle changes.
Concerning acceptability and understanding of the CDSMP, facilitators reported no major difficulty to understand the material and to deliver the content of the program. There was a need to define emotional states such as worry, joy, anxiety and frustration, which proved difficult to explain or understand. Programme facilitators described how they had to simplify the language and use practical examples that were outside the curriculum to convey some of the messages of the programme.
A facilitator flagged that ‘The manual that guides us has quite a theoretical character. We believe that more practical group-based activities should be introduced. Also, a collection of success stories from the pilot phase can be gathered to be distributed to facilitators for practical examples that would motivate participants and convince them that they can make change’. In some of the groups, additional facilitation techniques were introduced during the breaks to keep participants focused on the workshop activities. Facilitators emphasized that participants should be encouraged to share the actions they have undertook, since it could potentially serve as inspiration and motivation for other participants.
The balance between theoretical discussions and practical exercises was questioned as participants had greater expectations regarding the offer of physical exercises or practical advice on healthy eating: ‘Our participants requested from us to provide very specific sets of physical exercises or even recipes of different types of salads’. Some participants expected that facilitators would be medical workers who could provide them information on specific medical treatment for their conditions.
The second major theme of the FGD related to patients’ engagement with individual action plans for lifestyle changes. Programme facilitators shared that, although the development and implementation of individual action plans represented a major challenge for participants, it was also the most interesting and attractive part of the programme. Some participants changed their action plan during the course of the workshop, others chose to implement two action plans simultaneously, and many were sharing their experience with neighbors, friends and relatives. At the start of the workshop, physical exercise was the priority focus of most participants’ individual action plans, followed by a healthy diet. Emotion management and communication were the third most frequent theme of action planning. However, as participants advanced in the workshop, facilitators observed a shift in the content of individual action plans which increasingly prioritized emotion management and communication, suggesting an interest in expanding the range of coping skills and mechanisms. One facilitator noted: ‘The culture of communication and emotion management is not well developed in Moldova, especially in rural areas. Participating in the programme provided an opportunity for participants to experience the effect of activities focused on managing emotions and improving communication’. The workshop introduced stress relieving techniques, which were perceived as novel in the rural Moldovan context. Techniques such as controlled breathing exercises gained popularity among participants during the workshop.
Discussion
In this study, we assessed the satisfaction with and effect of the Stanford model of CDSMP on self-efficacy of chronic patients from rural settings in the Republic of Moldova. Our findings indicate that, after translation and cultural adaptation to the local context, the CDSMP is effective at increasing patients’ self-efficacy to manage the effect of their conditions on their lives, at least in the short-term. Specifically, the programme significantly increased the overall SEMCD six-item scale score, with an increase of almost three points between baseline and follow-up. Our study also showed a high acceptability of the programme by participants.
To the best of our knowledge, our intervention was the first attempt at piloting a peer-led model of self-management for adult chronic patients in a rural community setting in the Republic of Moldova. Our findings add to the existing body of literature that demonstrated the cross-cultural relevance, acceptability and effectiveness of the CDSMP, which has been translated in more than four languages, and implemented in diverse cultural settings, such as the Mexico border area in the USA, among multicultural populations in Hawaii, and among the Chinese population in Hong Kong (Lorig, Ritter, and Jacquez Citation2005; Siu et al. Citation2007; Tomioka et al. Citation2012). Additionally, we confirmed the applicability of the method across diverse socioeconomic settings and overall health systems frameworks.
The CDSMP is a valuable innovation to support self-management in the Republic of Moldova where modifiable risk behaviours (poor diet, lack of exercise, alcohol consumption and smoking) contribute to the heavy burden of premature mortality from NCDs (Skarphedinsdottir et al. Citation2014; WHO Citation2022a). Placing patient empowerment at the core of its approach, the CDSMP can offer solutions for disease prevention and health promotion in a resource-constrained health system, with shortage of health professionals and limited focus of health policies on prevention, or upon the occurrence of a protracted crises, for example. An essential element of the programme is the recognition of the patients, as empowered actors able to transform their wellbeing in their context. This involves change in individual settings (from lifestyle choices to exercise routines), family and home settings (including informal caregivers) as well as workplaces and communities.
The facilitators and the participants of the current intervention were mostly female. With time, some husbands and other male members of the communities joined. However, in future programmes we recommend a gender-specific recruitment strategy to recruit more males to join male- or mixed-gender groups.
Health promotion policies in the Republic of Moldova would benefit from supporting interventions that strengthen health literacy, patient empowerment and individual motivation for behavior change, while also offering equitable access to healthy lifestyle options for cardiovascular health (E. M. Raevschi and Martin Citation2020; E. Raevschi et al. Citation2022). Patient empowerment is critical to the Moldovan health system to challenge the cultural perception of the patient-professional relationship and to engage patients into finding local solutions that improve their own health (Raevschi and Martin Citation2020; Raevschi et al. Citation2022). The COVID-19 pandemic has shown that health systems cannot solve challenges alone; citizens and communities are an integral part of the health ecosystem and have to be given a more active role in an overall health planning.
However, bringing these innovations to scale and integrate them into health care systems is a constant challenge. The sustainability of community health promotion interventions, especially peer-led approaches, in resource-constrained settings is usually difficult to establish, especially if they have to exist outside of public or clinical structures (Bodkin and Hakimi Citation2020; Swerissen and Crisp Citation2004). In Denmark, the self-management programme is hosted and delivered by the DCHE, which is a national, non-profit organization, that provides health information services, in close collaboration with the Municipal authorities for funding (Danish Committee for Health Education Citation2023). In Switzerland, EVIVO has evolved towards a network of collaborators for the delivery of the programme across cantons but it remains hosted and curated by the Careum Foundation with financial support from partners including health insurances. These models demonstrate the critical importance of local partnerships for the sustainability of peer-led patient empowerment approaches in health promotion. In the Moldovan context, the Healthy Life Project has ensured that key national stakeholders from the health system were regularly informed and associated with the dissemination of the pilot results. The project has placed considerable efforts in fostering multisectoral collaborations on population health in rural districts by engaging local elected leaders and communities in joint prioritization and action planning on local health issues (Secula et al. Citation2022), or by strengthening integrated community care and enabling better collaboration between social and health sectors (Dnestrean et al. Citation2022). Scaling-up the CDSMP in Moldova in a sustainable way, will require the shared contributions of national and local actors for the funding and organisation of the programme, as well as a host institution for the overall coordination, evaluation and quality assurance of the approach.
Conclusion
The adaptation of the CDSMP programme in the Republic of Moldova has demonstrated short-term benefit on chronic patients’ self-efficacy to cope with the daily impact of their conditions. A European-level collaboration, based on the lessons learnt of CDSMP implementation in Denmark and Switzerland, was critical for the effective adaptation of this intervention in a new cultural setting. The global efforts and benefits of such collaborations support the sustainable development agenda of not leaving anyone behind. Equally important will be to strengthen the ownership of this pilot intervention by national actors in the Republic of Moldova and integrate the approach within a coherent set of health promoting policies addressing NCD risk factors in the Moldovan population.
Ethics statement
Prior to the consultations, a clear explanation was provided to all participants regarding the research objectives, emphasizing the non-collection of personal information. Only age and gender details of participants were documented, ensuring anonymity. Subsequently, verbal consent for observation was sought from each participant. In cases where a participant chose not to provide consent, no observations were carried out. Ethical approval for this study was obtained from the Ethics Committee of the Ministry of Health of Moldova (reference number 929, 26 August 2020).
Acknowledgements
The study was made possible through funding from the Swiss Agency for Development and Cooperation (SDC) in the frame of activities of the Healthy Life Project. The authors wish to thank the Moldovan Government, in particular the Ministry of Health, and district authorities for their support in conducting the Chronic Disease Self-Management Programme. We are also grateful for the technical support of experts from the Danish Committee for Health Education and the Careum Foundation who shared their insights on the adaptation of their respective self-management programmes and informed the design and implementation of this pilot intervention.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Bandura, A. 1977. “Self-Efficacy: Toward a Unifying Theory of Behavioral Change.” Psychological Review 84 (2): 191–215. https://doi.org/10.1037//0033-295x.84.2.191.
- Bodkin, A., and S. Hakimi. 2020. “Sustainable by Design: A Systematic Review of Factors for Health Promotion Program Sustainability.” BMC Public Health 20 (1): 964. https://doi.org/10.1186/s12889-020-09091-9.
- Danish Committee for Health Education. 2023. https://www.dche.eu/contact/.
- Dnestrean, T., T. Zatic, D. Popescu, A. Curteanu, and H. Prytherch. 2022. “How to Develop a Decentralized Integrated Community Care Approach - the Moldova Example.” International Journal of Integrated Care 22:120. https://doi.org/10.5334/ijic.ICIC21067.
- Donald, M., B. K. Kahlon, H. Beanlands, S. Straus, P. Ronksley, G. Herrington, A. Tong, et al. 2018. “Self-Management Interventions for Adults with Chronic Kidney Disease: A Scoping Review.” BMJ Open 8 (3): e019814. https://doi.org/10.1136/bmjopen-2017-019814.
- Dongbo, F., Y. Ding, P. McGowan, and H. Fu. 2006. “Qualitative Evaluation of Chronic Disease Self Management Program (CDSMP) in Shanghai.” Patient Education & Counseling 61 (3): 389–396. https://doi.org/10.1016/j.pec.2005.05.002.
- Essue, B. M., M. Laba, F. Knaul, A. Chu, H. V. Minh, T. K. P. Nguyen, and S. Jan. 2017. “Economic Burden of Chronic Ill Health and Injuries for Households in Low- and Middle-Income Countries.” In Disease Control Priorities: Improving Health and Reducing Poverty, edited by D. T. Jamison, H. Gelband, S. Horton, P. Jha, R. Laxminarayan, C. N. Mock, and R. Nugent. Washington (DC): The International Bank for Reconstruction and Development / The World Bank.
- GBD 2015 Risk Factors Collaborators. 2016. “Global, Regional, and National Comparative Risk Assessment of 79 Behavioural, Environmental and Occupational, and Metabolic Risks or Clusters of Risks, 1990–2015: A Systematic Analysis for the Global Burden of Disease Study 2015.” Lancet 388 (10053): 1659–1724. https://doi.org/10.1016/s0140-6736(16)31679-8.
- Haslbeck, J., S. Zanoni, U. Hartung, M. Klein, E. Gabriel, M. Eicher, and P. J. Schulz. 2015. “Introducing the Chronic Disease Self-Management Program in Switzerland and Other German-Speaking Countries: Findings of a Cross-Border Adaptation Using a Multiple-Methods Approach.” BMC Health Services Research 15:576. https://doi.org/10.1186/s12913-015-1251-z.
- Heyworth, I. T., M. L. Hazell, M. F. Linehan, and T. L. Frank. 2009. “How Do Common Chronic Conditions Affect Health-Related Quality of Life?” British Journal of General Practice 59 (568): e353–358. https://doi.org/10.3399/bjgp09X453990.
- Lorig, K. 2014. “Chronic Disease Self-Management Program: Insights from the Eye of the Storm.” Frontiers in Public Health 2:253. https://doi.org/10.3389/fpubh.2014.00253.
- Lorig, K. R., P. L. Ritter, and A. Jacquez. 2005. “Outcomes of Border Health Spanish/English Chronic Disease Self-Management Programs.” The Diabetes Educator 31 (3): 401–409. https://doi.org/10.1177/0145721705276574.
- Miller, W. R., S. Lasiter, R. Bartlett Ellis, and J. M. Buelow. 2015. “Chronic Disease Self-Management: A Hybrid Concept Analysis.” Nursing Outlook 63 (2): 154–161. https://doi.org/10.1016/j.outlook.2014.07.005.
- O’Connell, S., V. J. C. McCarthy, and E. Savage. 2018. “Frameworks for Self-Management Support for Chronic Disease: A Cross-Country Comparative Document Analysis.” BMC Health Services Research 18 (1): 583. https://doi.org/10.1186/s12913-018-3387-0.
- Peters, M., C. M. Potter, L. Kelly, and R. Fitzpatrick. 2019. “Self-Efficacy and Health-Related Quality of Life: A Cross-Sectional Study of Primary Care Patients with Multi-Morbidity.” Health and Quality of Life Outcomes 17 (1): 37. https://doi.org/10.1186/s12955-019-1103-3.
- Raevschi, E., L. Grib, O. Penina, and G. Obreja. 2022. “Relationship Between Cardiovascular Health Status and Attitudes Towards Responsibility for Health.” Folia Medica 64 (2): 327–332. https://doi.org/10.3897/folmed.64.e63538.
- Raevschi, E. M., and B. C. Martin. 2020. “Cardiovascular Health Metrics and Prevalence of Cardiovascular Disease in the Republic of Moldova.” European Journal of Public Health 30 (Supplement_5): 166–1079. https://doi.org/10.1093/eurpub/ckaa166.1079.
- Reynolds, R., S. Dennis, I. Hasan, J. Slewa, W. Chen, D. Tian, S. Bobba, et al. 2018. “A Systematic Review of Chronic Disease Management Interventions in Primary Care.” BMC Family Practice 19 (1): 11. https://doi.org/10.1186/s12875-017-0692-3.
- Ritter, P. L., and K. Lorig. 2014. “The English and Spanish Self-Efficacy to Manage Chronic Disease Scale Measures Were Validated Using Multiple Studies.” Journal of Clinical Epidemiology 67 (11): 1265–1273. https://doi.org/10.1016/j.jclinepi.2014.06.009.
- Schulman-Green, D., S. Jaser, F. Martin, A. Alonzo, M. Grey, R. McCorkle, N. S. Redeker et al. 2012. “Processes of Self-Management in Chronic Illness.” Journal of Nursing Scholarship 44 (2): 136–144. https://doi.org/10.1111/j.1547-5069.2012.01444.x.
- SDC Healthy Life project. “Reducing the Burden of Non-Communicable Disease in Moldova.” 2023. https://www.viatasan.md/en.
- Secula, F., D. Berari, A. Curteanu, S. Nicolaescu, and H. Prytherch. 2022. “A Whole-Of-Community Approach to Promote Cardiovascular Health: Healthy Communities in Moldova.” European Journal of Public Health 32 (Supplement_3): 131–324. https://doi.org/10.1093/eurpub/ckac131.324.
- Self-Management Resource Center. 2022a. “Implementation and Fidelity Manual”. In Evidence-Based Self-Management Programs Originally developed at Stanford University. Aptos, CA, USA: Self-Management Resource Center.
- Self-Management Resource Center. 2022b “Self-Efficacy for Managing Chronic Disease 6-Item Scale.” https://selfmanagementresource.com/wp-content/uploads/2022/06/English_-_self-efficacy_for_managing_chronic_disease_6-item.pdf.
- Self-Management Resource Center. 2023. “Bibliography.” https://selfmanagementresource.com/resources/bibliography/.
- Siu, A. M., C. C. Chan, P. K. Poon, D. Y. Chui, and S. C. Chan. 2007. “Evaluation of the Chronic Disease Self-Management Program in a Chinese Population.” Patient Education & Counseling 65 (1): 42–50. https://doi.org/10.1016/j.pec.2006.04.013.
- Skarphedinsdottir, M., B. Smith, A. Ferrario, O. Zues, A. Ciobanu, M. Ţîrdea, S. Domente, et al. 2014. Better Noncommunicable Disease Outcomes Challenges and Opportunities for Health Systems, n°4: Republic of Moldova Country Assessment. Regional Office for Europe: World Health Organization.
- Swerissen, H., J. Belfrage, A. Weeks, L. Jordan, C. Walker, J. Furler, B. McAvoy, et al. 2006. “A Randomised Control Trial of a Self-Management Program for People with a Chronic Illness from Vietnamese, Chinese, Italian and Greek Backgrounds.” Patient Education & Counseling 64 (1–3): 360–368. https://doi.org/10.1016/j.pec.2006.04.003.
- Swerissen, H., and B. R. Crisp. 2004. “The Sustainability of Health Promotion Interventions for Different Levels of Social Organization.” Health Promotion International 19 (1): 123–130. https://doi.org/10.1093/heapro/dah113.
- Tattersall, R. L. 2002. “The Expert Patient: A New Approach to Chronic Disease Management for the Twenty-First Century.” Clinical Medicine 2 (3): 227–229. https://doi.org/10.7861/clinmedicine.2-3-227.
- Tomioka, M., K. L. Braun, M. Compton, and L. Tanoue. 2012. “Adapting Stanford’s Chronic Disease Self-Management Program to Hawaii’s Multicultural Population.” The Gerontologist 52 (1): 121–132. https://doi.org/10.1093/geront/gnr054.
- Van de Velde, D., F. De Zutter, T. Satink, U. Costa, S. Janquart, D. Senn, and P. De Vriendt. 2019. “Delineating the Concept of Self-Management in Chronic Conditions: A Concept Analysis.” BMJ Open 9 (7): e027775. https://doi.org/10.1136/bmjopen-2018-027775.
- Vas, A., E. S. Devi, S. Vidyasagar, R. Acharya, N. R. Rau, A. George, T. Jose, and B. Nayak. 2017. “Effectiveness of Self-Management Programmes in Diabetes Management: A Systematic Review.” International Journal of Nursing Practice 23 (5). https://doi.org/10.1111/ijn.12571.
- WHO. 2018. Tackling Noncommunicable Diseases in the Republic of Moldova. Regional Office for Europe: World Health Organization.
- WHO. 2021. Classification of Self-Care Interventions for Health: A Shared Language to Describe the Uses of Self-Care Interventions. Geneva: World Health Organization.
- WHO. 2022a. “Health Systems in Action Republic of Moldova.” European Observatory on Health Systems and Policies.
- WHO. 2022b. “Web Annex 1. Prevalence of Noncommunicable Disease Risk Factors in the Republic of Moldova STEPS 2021 Fact Sheet. In: STEPS: Prevalence of Noncommunicable Disease Risk Factors in the Republic of Moldova, 2021.” Web annex 1. Prevalence of noncommunicable disease risk factors in the Republic of Moldova STEPS 2021 fact sheet. In: STEPS: prevalence of noncommunicable disease risk factors in the Republic of Moldova, 2021.
- WHO. 2022c. WHO Guideline on Self-Care Interventions for Health and Well-Being, 2022 Revision. Geneva: World Health Organization.
Appendix 1
The satisfaction questionnaire for patientsChoose among the following answers for each of the question
Strongly agree
Agree
Neither agree nor disagree
Disagree
Strongly disagree
Do not know
Q 1: I will tell others that the programme is good
Q 2: I have learned to set goals that I can achieve
Q 3: I trust the information and instructions I have received in the programme
Q 4: The lay-led workshop leaders have managed to communicate the content of the programme in an educational and understandable way
Q 5: Participating in the programme has been worth both the time and the energy put into it
Q 6: Difficult topics and discussions were handled well by the lay-led workshop leaders
Q 7: The contents of the programme were very relevant to my situation
Q 8: The lay-led workshop leaders were competent and well prepared
Q 9: The other programme attendants, the lay-led workshop leaders and I, had a good dialogue during the programme
Q 10: Overall satisfaction with the programme in its entirety.
