
ABSTRACT
Family caregivers’ social determinants of health are little assessed in previous intervention studies. We assess the extent to which diet-related disparities and inequalities in quality of life occur among family caregivers of different financial groups and if individually tailored nutritional guidance can narrow these inequalities. Data were collected between June 2019 and June 2020 at family caregivers’ households. The sample included 113 family caregivers from Finland. They were divided into intervention (n = 63) and control (n = 50) groups. The intervention group was further divided by those experiencing subjective poverty (n = 36) or financial security (n = 77) and subgroups of rural or urban participants. Family caregivers were interviewed on quality of life, nutritional variables, and sociodemographic factors. The intervention group received individually tailored nutritional guidance. Family caregivers experiencing subjective poverty had a lower overall quality of life, and physical, psychological, and environmental state of quality of life, and slightly poorer nutritional status at baseline than those who were financially secure. However, nutritional guidance improved the quality of life among family caregivers experiencing subjective poverty and somewhat narrowed inequalities in nutritional status among financial groups. Therefore, individually tailored nutritional guidance may improve the quality of life and, to some extent, the nutritional status of family caregivers experiencing subjective poverty, reducing inequalities. However, the issue requires increasing attention in caregiving research and healthcare to narrow family caregivers’ social and health inequalities.
Introduction
Family caregiving is usually unpaid care provided at home by close ones for individuals with cognitive, physical, or mental health challenges. Around 20% of the population provides family care in Canada, the United States, and the United Kingdom (International Alliance of Carer Organizations (IACO Citation2021), and from 6% to 13% in Finland (Eurocarers Citation2020). The estimate of family caregivers in Finland varies due to limited data on individuals providing care at home. However, those providing care in Finland can apply for a care allowance, an optional social service the municipality provides (please note: from 2023, the service was transferred to well-being services counties). Therefore, these family caregivers with a care allowance are in the municipalities’ registers, allowing data collection on the population. For example, evidence shows that most family caregivers in Finland with care allowance are older adults (Sotkanet Citation2022).
The number of older family caregivers has increased in Finland since the early 1990s (Sotkanet Citation2022). Nevertheless, the number of family caregivers is expected to grow globally due to the increasing care needs of the aging population (ILO Citation2018). Therefore, it is necessary to provide evidence on how to support family caregivers in this rapidly aging world. Yet, family caregivers are often seen as heroes who bear their responsibilities. Although this narrative is harmful in many ways, the same phenomenon has been seen during the pandemic when discussing health professionals (McAllister, Lee Brien, and Dean Citation2020).
Consequently, family caregivers need sustainable actions through healthcare and policy. Not only because care recipients deserve the best possible care, but family caregivers also need support in maintaining their health and decent quality of life. Thus, they have the right to health, healthy food, rest, routine health check-ups, and qualified health care (Antonella et al. Citation2017).
Background
Caregiving may put some family caregivers at risk of financial harm (NASEM Citation2016; Raiber, Visser, and Verbakel Citation2022). Family caregivers might experience opportunity costs owing to lost careers, earnings, pension entitlements (UNECE Citation2019), and wage penalties (Raiber, Visser, and Verbakel Citation2022). Some family caregivers may be more likely to live in poverty than non-caregivers (Kaplan Citation2018), and some experience subjective poverty linked to health disparities (Savela et al. Citation2022).
Moreover, family caregivers may experience cumulative inequality in life (Wakabayashi and Donato Citation2006). Cumulative inequality indicates that life-course events negatively affect each other, accumulating over time and resulting in economic consequences in older age (Wakabayashi and Donato Citation2006). These socioeconomic disparities may lead to avoidable health inequalities (Solar and Irwin Citation2010). This might become a vicious cycle: caregiving may increase the risk of poverty, whereas poverty increases the risk of adverse health outcomes, creating health inequalities.
However, the current evidence notably lacks the assessment of family caregivers’ social determinants of health (Hepburn and Siegel Citation2020; Savela et al. Citation2022; Young et al. Citation2020), including the inequalities in quality of life (QoL) and nutrition. For instance, some intervention studies have failed to assess family caregivers’ rurality and social disparities (Young et al. Citation2020). Therefore, this study aims to meet future healthcare needs by assessing practical solutions to narrow inequalities in nutrition and QoL among family caregivers of older adults experiencing subjective poverty. If these inequalities are not assessed, they will be ignored instead of improved across the globe.
The objective is twofold. First, we aim to assess family caregivers’ QoL and diet-related disparities among those experiencing subjective poverty and financial security at the baseline. Second, we assess whether individually tailored nutritional guidance can narrow the inequalities among these financial groups, also divided into subgroups of rural and urban family caregivers, after six months of intervention.
Terminology
This study follows the previous definitions of assessed concepts. “Subjective poverty” is an individual’s subjective experience of their financial resources. It does not refer to a direct measure of poverty or identification of the poor (Papuchon & Duvoux, Citation2019), and straightforward conclusions cannot be drawn based on an individual’s or household’s income. “Inequality” refers to unjust differences among the population (Braveman Citation2006). “Diet-related disparities” are the differences in dietary intake among different population segments, resulting in poor dietary quality and unequal disease burden (Satia Citation2009). Finally, “equity” means the absence of unfair and avoidable differences among groups of family caregivers and recognizing the circumstances that affect their resources and opportunities, whereas ”equality” would refer to the same resources given to all people without, for example, recognizing the allocation of resources. We will also reflect on the Conceptual Framework for Action on the Social Determinants of Health (Solar and Irwin Citation2010) when addressing the social determinants of health.
Social determinants of health are “the conditions in which people are born, grow, live, work, and age” (Solar and Irwin Citation2010). These determinants are responsible for avoidable inequalities in health and well-being (Solar and Irwin Citation2010). Although well-being is not equal to the QoL, a prior definition has described QoL as “the coverage of a broad range of content, including physical, functional, emotional, and social well-being” (Cella Citation1994). Currently, QoL is more commonly defined as “an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns’’ (The WHOQOL Group Citation1995). However, QoL is also a range of subjective (incl. finances, housing conditions, and environment) and objective indicators of how satisfied individuals are with their lives (Wallace and Abbott Citation2007).
Methods
Design
This LifEstyle, NutriTion, and Oral health in caregivers (LENTO) research is a randomized population-based multidisciplinary intervention study. The trial was registered at ClinicalTrials.gov, and its methodological details are presented in the study protocol (Nykänen et al. Citation2021)
Sampling and recruitment
The recruitment process was active in 2019. The eligible criteria for participants were: (i) family caregivers with a valid care allowance by the municipality in 2019, (ii) family caregivers taking care of a person aged 65 and older, and (iii) family caregivers living in an urban municipality or rural municipality in Eastern Finland. The definitions of rural and urban municipalities are based on the definitions by Statistics Finland (Statistics Finland Citation2022).
Care allowance means a discretionary caring agreement between the municipality and family caregiver, including services, e.g. taxable cash benefit for the family caregiver. Family caregiving in Finland has been described previously (Savela et al. Citation2022). The exclusion criteria were: (i) family caregivers taking care of an institutionalized care recipient and (ii) care recipients in end-of-life care.
The eligible family caregivers were contacted by social and health services persons from the municipalities using a convenience sampling approach. As a result, they identified 449 family caregivers. The research team sent the information letters via mail to these family caregivers. In addition, study participants also contacted the research team via phone or e-mail.
The first home visits were arranged with those family caregivers interested in participating. Family caregivers received comprehensive oral and written information about the study during the first home visit and wrote consent forms (June to December 2019). Thus, informed written consent was requested before the study nurse started interviews and clinical examinations.
Finally, 113 participated in this randomized control trial (. CONSORT Flow Diagram). There were 126 family caregivers at the study nurse’s visit at the baseline, but one participant declined to continue in the study, and the final number of participants at baseline was 125. However, twelve of them later excluded themselves for various reasons. The dropout rate was 10%.
Figure 1. CONSORT Flow Diagram.
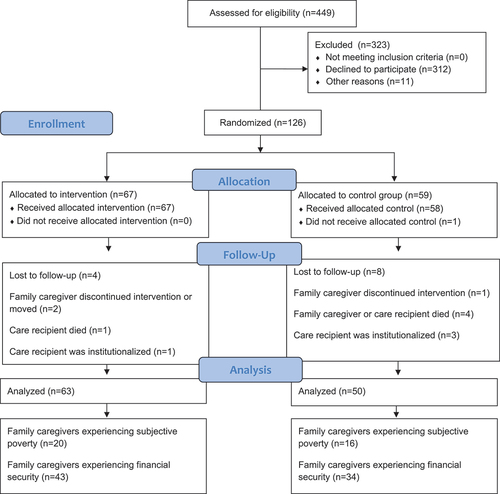
Randomization and sample
The IBM SPSS statistical software was used to generate the random allocation sequence. One of the researchers made the allocation, and the allocation ratio was 1:1. The study participants were randomized into intervention and control groups at the baseline (n = 125) and sequentially numbered by the same researcher. No specific criteria for receiving the intervention were followed. The study nurse and clinical nutritionist were not blinded due to the nature of the study. Moreover, neither the participants were blinded.
Data collection
Data were collected prospectively at the family caregivers’ households by a trained study nurse and clinical nutritionist. The baseline data collection period was from June to December 2019. The data at the end of the six-month intervention were collected between December 2019 and June 2020, mainly through similar procedures. However, some interviews were done via phone (between March 2020 and June 2020) because of the COVID-19 pandemic. Otherwise, personal protective equipment was used during the home visits in the summer of 2020, and social distancing was maintained. We also conducted some interviews outdoors during the pandemic.
Outcome measures at baseline and after the six-month intervention
Nutrition
The clinical nutritionist assessed family caregivers’ nutritional status using the Mini-Nutritional Assessment (MNA) tool, including daily fruit and vegetable consumption. The tool includes four sections: global, subjective, anthropometric, and dietetic view. The total score was 30 points: <17 indicates malnutrition, <17–23.5 is a risk of malnutrition, and > 23.5 a good nutrition. The tool is suitable for assessing older adults’ nutrition (Koponen et al. Citation2022; Nykänen et al. Citation2021).
Quality of life
Family caregivers were interviewed using the WHOQOL-BREF questionnaire, a shortened version of the WHOQOL-100 (The WHOQOL Group Citation1998). This tool is valuable, showing Cronbach’s alpha of 0.64 to 0.90 among older adults (Goes et al. Citation2021). The WHOQOL-BREF includes 26 questions and covers all four domains of QoL, which are (1) physical health, (2) psychological health, (3) social relationships, and (4) environment.
The first domain, “physical health”, includes questions on how pain prevents the performance of necessary tasks, the need for medical treatment to function in daily life, and the satisfaction with work capacity. The second domain, “psychological health’’, focuses on, for instance, how individuals feel their life is meaningful. Third, the “social relationships’’ domain focuses on satisfaction with personal relationships and social support systems. Finally, the fourth domain, “environment’’, includes safety and physical environment questions. The tool included items on a scale from 1 to 5, and the raw domain scores were transformed to a scale of 4 to 20 (The WHOQOL Group Citation1998).
Sociodemographic factors
The study nurse interviewed family caregivers based on age, gender, marital status, municipality (rural/urban), educational attainment, monthly household net income, and financial satisfaction at the baseline. Financial satisfaction was assessed using the ‘Have you enough money to meet your needs?’ question from the World Health Organization Quality-of-Life (WHOQOL). The responses ranged from 1 (no money at all) to 5 (completely enough). Then, the intervention group was divided for data analysis purposes based on financial satisfaction. Family caregivers who reported moderately, a little, or no money at all (scores 1 to 3) were classified as “experiencing subjective poverty’’, and those who reported having mostly or completely enough money (scores 4 to 5) as “financially secure”.
Intervention
Family caregivers in the intervention group (n = 63) received individually tailored nutritional guidance at baseline (Koponen et al. Citation2022; Nykänen et al. Citation2021). The clinical nutritionist guided family caregivers individually on, for instance, having five meals per day and five servings of fruit and vegetables per day. In contrast, family caregivers in the control group did not receive any guidance. Moreover, the clinical nutritionist did a follow-up meeting two months after the beginning of the intervention. The aim was to continue giving nutritional advice, evaluate the implementation of previous plans, and provide further instructions if needed. Finally, the study nurse and clinical nutritionist did the final measurements at the end of the six-month intervention, the same as the baseline.
Data analysis
Frequently used statistical methods were applied. Before the data analysis, normality and missing data variables were examined. In addition, we assessed sociodemographic factors between the intervention and control groups to avoid possible confounding factors. These included age, gender, marital status, municipality, educational attainment, monthly household income, and financial satisfaction. We assessed these baseline data factors between the intervention and control groups with t-tests (for continuous variables) and chi-square tests (for categorical variables). There were no significant differences between the intervention (n = 63) and control groups (n = 50) on sociodemographic factors (data not shown).
Next, similar data analyses were used to assess baseline characteristics of family caregivers experiencing subjective poverty (n = 36) and those who experienced financial security (n = 77). Thus, this assessment measured family caregivers’ disparities in QoL and nutrition at baseline. Then, the Paired Samples t-test or Wilcoxon signed-rank test for continuous variables and McNemar’s test for nominal data were used to assess the effectiveness of the intervention among these family caregivers. Similarly, the differences in QoL and nutrition after the intervention between rural and urban family caregivers were assessed using t-tests (for continuous variables) and chi-square tests (for categorical variables) or alternatives. Then, the results were summarised using numbers, percentages, means, standard deviations (SD), and a 95% confidence interval (CI). Significance was determined with a two-tailed p-value less than .050. All analyses were conducted using the IBM SPSS statistical software (v. 27.0).
Sample size and power
The study protocol has previously addressed the required sample size per group (Nykänen et al. Citation2021). As a result, the needed sample size was identified as 60 per group to achieve a statistical power of 0.80 with an α of 0.05 (Nykänen et al. Citation2021).
Ethical approval
The LENTO study follows the principles of the Declaration of Helsinki. The ethics committee of the Northern Savo Hospital District reviewed the ethical issues involved in this research and gave a favorable opinion.
Results
shows the baseline characteristics of family caregivers collected between June 2019 and December 2019.
Table 1. Baseline characteristics between family caregivers experiencing subjective poverty and financial security (n = 113).
Effects of nutritional guidance on those experiencing subjective poverty
Family caregivers who experienced subjective poverty had an improvement in their overall QoL compared to baseline (p = 0.010, 95% CI −15.9, −2.3). Similarly, after the six-month intervention, there was an improvement in their psychological (Z = −2.0, p = .047) and environmental state of QoL (Z = −2.4, p = 0.017). In contrast, financially secure family caregivers’ overall QoL and physical health decreased.
The risk of malnutrition of family caregivers who experienced subjective poverty decreased, and servings of fruit and vegetables per day increased. However, their nutritional status did not improve based on the MNA score. Results are presented in .
Table 2. Changes in quality of life and nutrition among intervention groups (n = 63).
Effects of nutritional guidance on rural and urban family caregivers
Rural family caregivers who experienced subjective poverty had a higher overall QoL (M = 94, SD = 6.2) at baseline compared to their urban peers (M = 87.4, SD = 9.9). At baseline, rural family caregivers also had better social relationships (M = 16.3, SD = 0.6 vs. M = 13.9, SD = 3.0), and the environmental state of QoL (M = 16.0, SD = 1.0 vs. M = 14.6, SD = 1.8). Nevertheless, both groups had an increase in their overall QoL and QoL domains after the intervention, and there were no significant differences before or after the intervention (data not shown).
Rural family caregivers who experienced subjective poverty improved their nutritional status based on MNA scores (M = 25.3, SD = 1.6 to M = 27.3, SD = 1.3). In contrast, their urban peers had a reduction in nutrition (M = 25.8, SD = 2.0 to M = 24.9, SD = 2.3). In addition, rural family caregivers who experienced financial security improved their nutritional status (M = 24.9, SD = 1.7 to M = 27.5, SD = 1.7). On the other hand, their urban peers had a slight reduction (M = 25.6, SD = 2.0 to M = 25.5, SD = 1.9). Therefore, financially secure rural family caregivers had a significantly better nutritional status (U = 128.5, p = 0.031) than their urban peers after the six-month intervention. No other statistically significant results were identified.
Discussion
The evidence showed that individually tailored nutritional guidance could improve QoL and, to some extent, the nutritional status of family caregivers experiencing subjective poverty, reducing inequalities. Nevertheless, the mechanisms of how the nutritional guidance improved QoL among family caregivers who experienced subjective poverty are unclear. Hence, it is uncertain if nutritional guidance improved nutritional knowledge, which led to better food choices. These healthier and improved choices could have then led to better QoL. However, some qualitative evidence might have been required to confirm this conclusion. For instance, it would have been insightful to assess how these family caregivers experienced the nutritional guidance and whether there were any financial difficulties in following it. This method would have also provided more information and tools to social and healthcare on how to face, guide, and promote the health of family caregivers experiencing subjective poverty.
We must also address the structural determinants of nutritional status. Family caregivers’ diet-related disparities are found to be related to their social and health inequalities (Savela et al. Citation2023), which may also indicate food insecurity risk. Food insecurity is broadly linked to social and health inequalities (FAO, Citation2020; Pooler et al., Citation2019) and human rights (UN Human Rights Citation2021). However, these inequalities result from structural factors shaping societies. Inequalities in health and well-being then flow from patterns of social stratification (Solar and Irwin Citation2010). outlines the possible pathways of family caregivers’ inequalities based on the Conceptual Framework for Action on the Social Determinants of Health (Solar and Irwin Citation2010).
Figure 2. Applied and modified from conceptual framework for action on the Social Determinants of Health by Solar and Irwin (Citation2010).
Previous European research shows that good governance significantly reduces the probability of experiencing subjective poverty among poor (monetary income) households (Baldini, Peragine, and Silvestri Citation2018). This previous study by Baldini et al. included Finland, but the issue should be investigated more precisely, particularly among family caregivers experiencing subjective poverty and how they experience governance. In future research, it would be relevant to assess well-being from a societal perspective using the Social Quality Model (Abbott and Wallace Citation2012).
Moreover, rural and urban family caregivers’ inequalities in QoL might be related to regional inequalities. Regional inequalities refer to ‘“differences in the quality of life, wealth and living standards of people living and/or working in different places”’ (Dunford Citation2009, 1). Unfortunately, little is known about regional inequalities among family caregivers across Finland and other countries. On the other hand, a study conducted in Norway, which used WHOQOL-BREF to assess older adults’ QoL, found that rural residents had a significantly higher QoL than urban and semi-rural residents (Santora, Byrne, and Klöckner Citation2021).
Nevertheless, our study had a relatively small sample size of rural residents. Then again, these results might be truly relevant and explained by environmental satisfaction, community trust, and better social connections among rural residents. For example, evidence from the United Kingdom estimated that aspects associated with higher environmental QoL among older adults included positive perceptions of their physical environment (Munford et al. Citation2020). Moreover, they estimated that greater social QoL was derived from social support and better personal relationships (Munford et al. Citation2020). This phenomenon might be equivalent to our study’s results on the QoL of rural family caregivers. However, more longitudinal evidence with a larger sample size is required to investigate the issue. In addition, it would be interesting to assess the factors buffering against rural family caregivers’ decline in QoL despite their experience of subjective poverty. In light of this evidence, we may only assume that the effect is associated with their living environment and social network, which protects their QoL.
Nonetheless, there are some study limitations. For example, these results may not be generalizable to all family caregivers of older adults. In addition, the intervention may have included only those family caregivers with enough well-being and resources to continue the study. Besides these aspects, there is limited previous evidence to compare these results and make conclusions.
The strengths of this study are linked to its population-based design and the randomized method used. This randomized controlled trial also used validated measurement tools, which provides the reliability of the results. In addition, these tools were used by a clinical nutritionist and study nurse, which also improves the reliability. We also followed the CONSORT Checklist for reporting. In addition, we acknowledged the previous evidence on improving the interpretation of the results of clinical trials (Gates and Ealing Citation2019). Hence, although we could not reach a conventional threshold for ‘’statistical significance’’ in some parts of the study, we cannot conclude that there were no improvements in the intervention group. For instance, only three rural family caregivers were experiencing subjective poverty. Therefore, assessing the issue with a larger sample size would be essential.
Future steps to narrow family caregivers’ health disparities require more research and intervention studies on their social health inequalities, mainly focusing on rural and urban family caregivers and their subjective poverty. In addition, more education on social determinants of health among health professionals, screening of individuals’ social needs in healthcare, and equal healthcare and health policy are needed. More importantly, healthcare requires multi-professional cooperation to enhance health equity. Nevertheless, health professionals must understand the social determinants of health and social health disparities. Education and training are the most effective ways to fill the knowledge gap (Rosa et al. Citation2021).
Conclusion
Family caregivers may experience social, regional, and diet-related disparities and inequalities in QoL. Individually tailored nutritional guidance might improve QoL and, to some extent, the nutritional status of family caregivers experiencing subjective poverty, reducing inequalities. However, the issue requires increasing attention in healthcare and policy to narrow family caregivers’ inequalities.
Reporting Method
CONSORT Checklist (Consolidated Standards of Reporting Trials).
Trial and Protocol Registration
ClinicalTrials.gov NCT04003493. Registered on 28 June 2019. Retrospectively registered.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Abbott, P., and C. Wallace. 2012. “Social Quality: A Way to Measure the Quality of Society.” Social Indicators Research 108 (1): 153–167. https://doi.org/10.1007/s11205-011-9871-0.
- Antonella, S., V. Flavia, T. Daniela, T. Giuseppe, and S. Daniele. 2017. “The ‘Charter of Rights for Family Caregivers’. The Role and Importance of the Caregiver: An Italian Proposal.” ESMO Open 2 (5): e000256. https://doi.org/10.1136/esmoopen-2017-000256.
- Baldini, M., V. Peragine, and L. Silvestri. 2018. “Quality of Government and Subjective Poverty in Europe.” CESifo Economic Studies 64 (3): 371–395. https://doi.org/10.1093/cesifo/ifx023.
- Braveman, P. 2006. “Health Disparities and Health Equity: Concepts and Measurement.” Annual Review of Public Health 27 (1): 167–194. https://doi.org/10.1146/annurev.publhealth.27.021405.102103.
- Cella, D. F. 1994. “Quality of Life: Concepts and Definition.” Journal of Pain and Symptom Management 9 (3): 186–192. https://doi.org/10.1016/0885-3924(94)90129-5.
- Dunford, M. 2009. “Regional Inequalities.” International Encyclopedia of Human Geography 236–245. https://doi.org/10.1016/B978-008044910-4.00874-9.
- Eurocarers. 2020. Finland. https://eurocarers.org/country-profiles/finland/.
- FAO (2020). Role of Income Inequality in Shaping Outcomes on Individual Food Insecurity. In Background paper for The State of Food Security and Nutrition in the World 2019. FAO. https://doi.org/10.4060/cb2036en.
- Gates, S., and E. Ealing. 2019. “Reporting and Interpretation of Results from Clinical Trials That Did Not Claim a Treatment Difference: Survey of Four General Medical Journals.” BMJ Open 9 (9): e024785. https://doi.org/10.1136/bmjopen-2018-024785.
- Goes, M., M. Lopes, J. Marôco, H. Oliveira, and C. Fonseca. 2021. “Psychometric Properties of the WHOQOL-BREF(pt) in a Sample of Elderly Citizens.” Health and Quality of Life Outcomes 19 (1): 146. https://doi.org/10.1186/s12955-021-01783-z.
- Hepburn, K., and E. O. Siegel. 2020. “New Directions to Advance Family Caregiving Research.” The Gerontologist 60 (Supplement_1): S1–S4. https://doi.org/10.1093/geront/gnz182.
- IACO (International Alliance of Carer Organizations). 2021. Global Carer Facts. IACO. https://internationalcarers.org/carer-facts/global-carer-stats/.
- ILO (International Labour Organization). 2018. Executive Summary: Care Work and Care Job for the Future of Decent Work. International Labour Office (ILO).
- Kaplan, R. L. 2018. “Family Caregiving and the Intergenerational Transmission of Poverty.” Journal of Law, Medicine & Ethics 46 (3): 629–635. https://doi.org/10.1177/1073110518804216.
- Koponen, S., I. Nykänen, R.-M. Savela, T. Välimäki, A. L. Suominen, and U. Schwab. 2022. “Individually Tailored Nutritional Guidance Improved Dietary Intake of Older Family Caregivers: A Randomized Controlled Trial.” European Journal of Nutrition 61 (7): 3585–3596. https://doi.org/10.1007/s00394-022-02908-w.
- McAllister, M., D. Lee Brien, and S. Dean. 2020. “The Problem with the Superhero Narrative During COVID-19.” Contemporary Nurse 56 (3): 199–203. https://doi.org/10.1080/10376178.2020.1827964.
- Munford, L. A., M. Panagioti, P. Bower, and S. M. Skevington. 2020. “Community Asset Participation and Social Medicine Increases Qualities of Life.” Social Science & Medicine 259 (March): 113149. https://doi.org/10.1016/j.socscimed.2020.113149.
- NASEM (National Academies of Sciences, Engineering, and Medicine). 2016. Families Caring for an Aging America. R. Schulz & J. Eden edited by. National Academies Press. https://doi.org/10.17226/23606
- Nykänen, I., T. Välimäki, L. Suominen, and U. Schwab. 2021. “Optimizing Nutrition and Oral Health for Caregivers–Intervention Protocol.” Trials 22 (1): 625. https://doi.org/10.1186/s13063-021-05589-8.
- Papuchon, A. and N. Duvoux 2019. “‘’Subjective Poverty as Perceived Lasting Social Insecurity: Lessons from a French Survey on Poverty, Inequality and the Welfare State (2015–2018).’‘.” SSRN Electronic Journal. 10.2139/ssrn.3465214.
- Pooler, J. A., H. Hartline‐Grafton, M. DeBor, R. L. Sudore, and H. K. Seligman. 2019. “Food Insecurity: A Key Social Determinant of Health for Older Adults.” Journal of the American Geriatrics Society 67 (3): 421–424. https://doi.org/10.1111/jgs.15736.
- Raiber, K., M. Visser, and E. Verbakel. 2022. “The Wage Penalty for Informal Caregivers from a Life Course Perspective.” Advances in Life Course Research 53 (June): 100490. https://doi.org/10.1016/j.alcr.2022.100490.
- Rosa, W. E., C. J. Hannaway, C. McArdle, M. F. McManus, S. T. Alharahsheh, and M. Marmot. 2021. Nurses for Health Equity: Guidelines for Tackling the Social Determinants of Health. WISH.
- Santora, L., D. Byrne, and C. Klöckner. 2021. “Exploring Quality of Life Reported by Norwegian Older Adults Using Classification Tree Approach on Group Profiles.” Ageing International 123456789 (4): 816–846. https://doi.org/10.1007/s12126-021-09454-6.
- Satia, J. A. 2009. “Diet-Related Disparities: Understanding the Problem and Accelerating Solutions.” Journal of the American Dietetic Association 109 (4): 610–615. https://doi.org/10.1016/j.jada.2008.12.019.
- Savela, R.-M., I. Nykänen, S. Koponen, A. L. Suominen, U. Schwab, and T. Välimäki. 2023. “Older Family caregivers’ Diet‐Related Disparities: Cross‐Sectional Evidence from Finland.” International Journal of Older People Nursing e12570 (6). https://doi.org/10.1111/opn.12570.
- Savela, R.-M., I. Nykänen, U. Schwab, and T. Välimäki. 2022. “Social and Environmental Determinants of Health Among Family Caregivers of Older Adults.” Nursing Research 71 (1): 3–11. https://doi.org/10.1097/NNR.0000000000000559.
- Savela, R.-M., U. Schwab, and T. Välimäki. 2022. “An Integrative Review of the Social Determinants of Mental Health Among Older Caregivers.” Nursing Open 9 (1): 94–107. https://doi.org/10.1002/nop2.1094.
- Solar, O., and A. Irwin 2010. “A Conceptual Framework for Action on the Social Determinants of Health.” In Social Determinants of Health Discussion Paper 2, Policy and Practice.
- Sotkanet. 2022. Support for Informal Care, Carers Who Have Made an Official Care Agreement in Services Funded by the Municipality. https://sotkanet.fi/.
- Statistics Finland. 2022. Statistical Grouping of Municipalities. https://www.stat.fi/meta/kas/til_kuntaryhmit_en.html.
- UNECE. 2019. “The Challenging Roles of Informal Carers.” UNECE Policy Brief on Ageing 22: 1–20. http://www.unece.org/population.
- UN Human Rights. 2021. Key Aspects of the Right to Food. UN Human Rights and the Right to Food. https://www.ohchr.org/en/food.
- Wakabayashi, C., and K. M. Donato. 2006. “Does Caregiving Increase Poverty Among Women in Later Life? Evidence from the Health and Retirement Survey.” Journal of Health and Social Behavior 47 (3): 258–274. https://doi.org/10.1177/002214650604700305.
- Wallace, C., and P. Abbott. 2007. “From Quality of Life to Social Quality: Relevance for Work and Care in Europe the Origins of Social Quality.” Quality 1: 109–123.
- The WHOQOL Group. 1995. “The World Health Organization Quality of Life Assessment (WHOQOL): Position Paper from the World Health Organization.” Social Science & Medicine 41 (10): 1403–1409. https://doi.org/10.1016/0277-9536(95)00112-K.
- The WHOQOL Group. 1998. “Development of the World Health Organization WHOQOL-BREF Quality of Life Assessment.” Psychological Medicine 28 (3): 551–558. https://doi.org/10.1017/S0033291798006667.
- Young, H. M., J. F. Bell, R. L. Whitney, R. A. Ridberg, S. C. Reed, P. P. Vitaliano, and K. Hepburn. 2020. “Social Determinants of Health: Underreported Heterogeneity in Systematic Reviews of Caregiver Interventions.” Gerontologist 60 (Supplement_1): S14–S28. https://doi.org/10.1093/geront/gnz148.
