
Abstract
In an Israeli qualitative study with adolescent cancer survivors and parents who had considered fertility preservation, practically all participants could not recall any discussions with healthcare providers about plans for cryopreserved biological materials in the case of death. This finding is surprising given recent court struggles in Israel over the posthumous use of cryopreserved sperm. In interviews with these adolescent survivors and their parents, intended future use of cryopreserved biological materials is directed for affected individuals’ reproductive purposes later in life, with hardly any consideration of others' use of these materials for posthumous reproduction. To avoid future ethical and legal quagmires, healthcare professionals should have frank discussions with adolescents and their parents about what to do with such materials in the case of death. This paper discusses the socio-cultural and legal Israeli context and considers the ethical implications of using minors’ biological materials for posthumous assisted reproduction in Israel.
Introduction
Since cancer and/or its treatment may be gonadotoxic (Lee et al. Citation2006), strides have been made to preserve cancer patients’Footnote1 fertility, i.e their future possibility to have genetically-related children. Despite the rarity of childhood cancer (Ward et al. Citation2014) and recent increased overall survival rates for children and adolescents (Siegel, Miller, and Jemal Citation2017), cancer remains a leading cause of childhood death in developed countries (American Cancer Society Inc. Citation2011). Furthermore, accidents are the main cause of death for children, adolescents, and young adults (Heron Citation2018). Thus, it is plausible that a patient who undergoes fertility preservation (FP) may die prior to using their cryopreserved biological materials for reproductive purposes. In such a case, what should be done with the cryopreserved biological materials, especially those of minors?Footnote2 Three distinct options are possible: destruction, donation for medical research, and donation for reproductive purposes. The following deliberations focus on the last possibility.
Although the European Society of Human Reproduction and Embryology (ESHRE), as well as the American Society for Reproductive Medicine (ASRM), concur that it is highly inappropriate for parents to use the cryopreserved gametes or reproductive tissue of a deceased child for posthumous assisted reproduction (PAR), some Israeli studies challenge this notion. Interestingly, in surveys of Israeli soldiers and secular parents of combat soldiers in active duty, both parties were more inclined to consider PAR if the other party (e.g. deceased child or bereaved parent) had previously expressed an explicit desire for it (Bokek-Cohen and Ravitsky Citation2019; Ravitsky and Bokek-Cohen Citation2018). Thus, despite the fact that it is unconventional to think of reproduction as a joint intergenerational decision of children and parents (Young Citation2014), it seems that in Israel the death of a child can conceivably create such a scenario.
A smattering of recent headlines indicate multiple cases of Israeli parents requesting to pursue PAR with their deceased son’s preserved spermFootnote3 (CitationAbramov; CitationBarkan; CitationCohen Friedman; CitationOkbi; Zarchin Citation2011). These stories detail the emotional plight of bereaved parents, often including pictures of the deceased and/or their parents, and framed to appeal to Israeli readers’ pronatalism. On the other hand, a preliminary study of Israelis’ opinions on PAR indicates greater disapproval of posthumous grandparenthood than posthumous reproduction (Hashiloni-Dolev Citation2015), which calls for greater nuance in the understanding of the Israeli context.
This paper reports on and analyzes a subset of findings from a study on adolescent oncofertility decision making in Israel. The proceeding findings specifically report on thoughts and discussions Israeli adolescent oncology patients and their parents recall having with respect to plans for cryopreserved biological materials in case of the adolescent’s death. The results are followed by a discussion that contextualizes these findings within Israeli culture and policy, offers recommendations for clinical practice worldwide, and expands on the ethical issues related to PAR with minors’ biological material that are likely to arise first in Israel due to its particular culture and legal/regulatory landscape.
How international guidelines address disposition of minors’ cryopreserved biological materials
In their paper on the “Ethical consideration for the cryopreservation of gametes and reproductive tissues for self use,” ESHRE urges healthcare professionals to discuss the possibility of death (of those affected by serious diseases) during counseling sessions, advises that preserved reproductive tissue and gametes of children or adolescents should be discarded upon death of the provider, and insists that parents do not have the right to decide about the reproductive use of a child’s biological material after her/his death (ESHRE Task Force on Ethics and Law Citation2004).
Furthermore, in their paper on “Posthumous assisted reproduction,” ESHRE asserts that at the time of storage or before the start of IVF, it is necessary to have obtained written consent of the deceased for PAR (ESHRE Task Force on Ethics and Law et al. Citation2006). Additionally, ESHRE declares that while preserved gametes or embryos can be put at the disposition of a surviving partner, parents of the deceased have no say regarding PAR (ESHRE Task Force on Ethics and Law et al. Citation2006). The paper also notes that while there is no consensus about posthumous donation to third parties, a donor’s deceased status ought to be known to third party recipients (ESHRE Task Force on Ethics and Law et al. Citation2006).
The American Society for Reproductive Medicine (ASRM) also addresses the matter in two committee opinions. In their opinion on “Fertility preservation and reproduction in patients facing gonadotoxic therapies,” ASRM suggests that all persons who undergo FP or their legal guardians give written directions for the future disposition of biological materials, such as disposal, use in research, or PAR (Ethics Committee of the American Society for Reproductive Medicine Citation2013a). They further specify that such directions should be made when biological materials are removed or preserved, but can be given or amended at any time thereafter (Ethics Committee of the American Society for Reproductive Medicine Citation2013a).
In their opinion on “Posthumous collection and use of reproductive tissue,” ASRM proclaims that although medical institutions are not obliged to participate in PAR, they should develop written policies regarding the specific circumstances in which they will or will not (Ethics Committee of the American Society for Reproductive Medicine Citation2013b). Additionally, in the absence of written directions from the deceased, medical institutions should only consider PAR when requests are initiated by a surviving partner (Ethics Committee of the American Society for Reproductive Medicine Citation2013b). ASRM states that parents and children are never considered to have a joint reproductive project (Ethics Committee of the American Society for Reproductive Medicine Citation2013b).
The Israeli context: pronatalism
Israeli society is extremely pronatalist. Voluntary childlessness is almost unheard of and individuals often experience tremendous social pressure to procreate. This social context is the result of religious, historical, and political factors. First, halachic (Jewish religious law) and traditional influences are present in family life, societal norms, policy making and every other aspect of Israel’s social fabric. The country’s pronatalist attitudes and high fertility rates can be partly attributed to the biblical commandment to “be fruitful and multiply” (in Hebrew: p’ru u’rvu). Reproduction is seen both as an individual and as a national imperative (Kahn Citation2000). The interrelation of biological and social reproduction is an integral part of Jewish history. Second, the trauma of the Holocaust and the ideology of Zionism contribute to an emphasis on regeneration through reproduction to ensure the continuity of the Jewish people and to secure the political survival of Israel in the long term (Birenbaum-Carmeli and Carmeli Citation2010; Prainsack and Firestine Citation2006). Third, in modern-day Israel, which defines itself as a Jewish-democratic state, the preservation of a Jewish majority presents a constant demographical challenge (Gross and Ravitsky Citation2003).
Parenthood and family are highly valued in Israel, not only within religious contexts but also secular ones. These values should be considered in ethical and legal discussions of fertility and infertility in Israel, and particularly in cases where decisions concerning potential lives and deaths are intertwined (such as with PAR). The serious ethical reservations over new applications of reproductive technologies that generally dominate Western political discourse and legal decision-making are not as pronounced in the Israeli context. Acceptance of reproductive technologies (e.g. IVF and PGD) is grounded within socio-cultural norms and expectations, as well as traditional values (Ben-Or and Ravitsky Citation2010). While Israel’s common law is secular and based on democratic procedures,Footnote4 strong influences of Jewish religious law, or Halacha, are present in Israeli legislation and jurisprudence. This is especially true in the realm of family law that is heavily infused with halachic concepts and approaches.
The Israeli context: third party assisted reproduction
Unless a surviving female ex-partner initiates PAR with her deceased partner’s sperm, PAR will require the assistance of third parties. Therefore, to understand PAR in the Israeli context, it is necessary to understand the legal and religious policies with respect to third party assisted reproduction – namely gamete donation and surrogacy.
All sperm donation in Israel is anonymous (Ministry of Health Citation2019b).Footnote5 Egg donation is also anonymous, however directed donation, outside of the family, is possible (Ministry of Health Citation2019a). Though egg and sperm donors must be unmarried, donation from a married woman is possible only when an egg recipient and her husband provide consent for such a donation (Ministry of Health Citation2019a, Citation2019b).Footnote6
Aspects of Israel’s policies regarding gamete donation can seem puzzling at first, but are clearly compatible with halachic aspects of personal and marital status. Some rabbis rule that a child born following artificial insemination of a married woman with the sperm of a Jewish donor is considered a mamzer/mamzeret (f.) (i.e. totally illegitimate in a religious sense) or at least potentially illegitimate (safek mamzer) (Steinberg Citation2003). Mamzerim are considered offspring of adulterous or incestuous relationships and are forbidden to marry other Jews (only converts or other mamzerim) (Zemer Citation1999). Even though most halachic authorities do not consider the child a mamzer due to their opinion that the status of mamzerut only applies if prohibited coitus takes place – and with artificial insemination there is no sexual intercourse – the concern remains that a “brother may unwittingly marry a sister” or vice versa from the same father who is the sperm donor (Steinberg Citation2003).
The matter of surrogacy is also halachically complex. According to the majority of halachic authorities, the egg provider is not considered the mother, but rather the woman who gives birth (Bleich Citation1991; Steinberg Citation2003; Wahrman Citation2005). In contrast, according to the Israeli surrogacy law, the genetic mother, who provides the egg, is considered to be the legal mother of the resulting child. Israel's surrogacy law - the Embryo Carrying Agreement Law of 1996 - allows only stable heterosexual couples to apply for permission to use a surrogate. It permits only gestational surrogacy utilizing the sperm of the intended father (i.e. where the surrogate carries a fetus that is genetically related to its intended parents) (Birenbaum-Carmeli Citation2016).Footnote7 Surrogacy with donor sperm is not permitted. Parties involved in a surrogacy agreement must be above the age of legal capacity, the carrying mother should not be married and cannot be a relative of either intended parent. She should be of the same religion as the intended mother, to avoid confusion regarding the religious identity of the child (which in the case of Judaism is determined by the religious identity of the mother). The law further requires the registration of all children born under surrogacy agreements in a special registry (Shalev Citation1998).
Several rules of the surrogacy law bear the influence of Halacha. The prohibition that the carrying mother may neither be a married woman nor a family relative of either one of the commissioning parents, as well as the mandatory registration of the children born under surrogacy agreements, are due to the laws of mamzerut and the religio-legal intention to prevent potential forbidden (incestuous) relationships that could lead to mamzerut in the future (Shalev Citation1998). Although, as mentioned above, most authorities do not consider a child conceived by an unmarried woman by means of assisted reproductive technologies (ART) to be a mamzer, Israeli law rules along the stringent halachic position in these matters.
The Israeli context: PAR
With respect to PAR, Israeli Posthumous Reproduction Guidelines limit requests for PAR to female partners of the deceased and allow courts to approve them even in the absence of explicit written consent, based on testimony that the deceased expressed a desire for parenthood, even if not explicitly for PAR (Ravitsky Citation2004). Despite these guidelines, more than ten cases of bereaved parents of a deceased child have sought permission from the courts to use their deceased son’s sperm to create genetic grandchildren (Rimon-Greenspan and Ravitsky Citation2013).
From a halachic perspective, PAR has been discussed only in relation to cases of married deceased donors, with respect to male gametes. If the deceased man did not father a child, the widow is allowed to be inseminated with his sperm, since the event of death does not nullify per se the initial project of procreation. Allowing the widow to give birth and raise the child of her deceased husband is understood to be an act of gemilut chassadim (loving-kindness) (Steinberg Citation2017). On the other hand, not all halachic authorities endorse the use of sperm that was cryopreserved before the death of the husband, due to prohibitions of masturbation.
Some halachic authorities do allow post-mortem sperm retrieval for purposes of inseminating the surviving wife if the deceased agreed to such a procedure or if there is strong evidence of his probable consent. It is interesting to note that post-mortem sperm retrieval of non-married men is permissible when surviving parents file a request. Furthermore, one halachic arbiter opines that parents’ wishes trump those of the widow with respect to post-mortem sperm retrieval (Steinberg Citation2017).
Materials and methods
The first author made three visits to Israel between January and June 2016 to conduct semi-structured interviews in person with adolescent cancer survivors and their respective parents. Adolescents and parents were interviewed separately. Inclusion criteria included adolescents currently between the ages of 12 and 19 years who were treated at a major medical center in Israel, had been given the opportunity to preserve their fertility via sperm, ova, and/or ovary cryopreservation, and were in remission for at least 2 months, as well as their parents. Patients and parents that met the inclusion criteria and were scheduled for follow up appointments during the time of the first author’s visits were invited for interviews to discuss their previous FP decision making. Semi-structured interviews were conducted in Hebrew at the time and location of the participant’s choice: an empty office at the hospital, his/her home, or a café. Prior to the start of the study, ethics approval was obtained from the cantonal Swiss ethics committee in Switzerland and the Israeli hospital’s ethics committee.
Audio recordings of the interviews were translated and transcribed directly into English – the language understood by all project team members. An independent individual, fluent in both Hebrew and English, reviewed and validated transcript translations. With the assistance of MAXQDA 12 software, the first author thematically analyzed all transcripts using an essentialist/realist approach, whereby prevalent patterned responses, or themes, were identified in the interviews’ semantic content and organized according to the theoretical structure of the interview guide (Braun and Clarke Citation2006). A second team member examined all thematic codes based on her full reading of a quarter of all transcripts. In cases of initial discrepancy, both team members discussed thematic codes in order to reach mutual agreement. All participants were given pseudonyms.
Results
Sixteen out of 28 invited adolescents (10/14 females and 6/14 males) and 19/30 invited parentsFootnote8 (14 individuals and 5 pairs) agreed to be interviewed. Altogether, these interviews represent 20 cases of adolescent FP decision making. In 15 of these cases, both the adolescent and parent(s) were interviewed, separately. In the remaining 5 cases, only the adolescent or parent was interviewed. (See .)
Figure 1. Profile of Interviews.
Note: cells marked with F represent cases of female FP; cells marked with M represent cases of male FP; crossed cells refer to cases when FP was not pursued; and darker cells represent cases where both the adolescent and parent(s) were interviewed (separately).
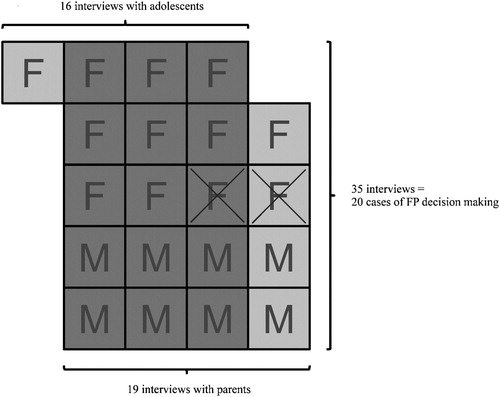
Of the 20 cases of adolescent fertility decision making, 12 pertained to females and 8 to males. In 2 of the 12 female cases, FP was declined. In all other cases, FP was pursued. (See .) Therefore, there was an underrepresentation of declining females and no representation of declining males. Furthermore, there was an underrepresentation of the Arab population and no representation of Orthodox Jews. For further details on interviewee demographics and specific FP techniques pursued, please refer to (Barlevy et al. Citation2019).
In discussing their FP decision making, participants who pursued FP were asked what they planned to do with the preserved biological materials in the case of adolescent death. As a lead up to this sensitive question, participants were asked if they had thought about what they would do with the preserved gametes and/or organs in the future. All adolescents and parents responded that they would use them if necessary, referring to the case that the adolescent or their partner could not get pregnant via coitus.
Reminding participants that the majority of adolescent cancer is receptive to treatment, they were then asked what they had discussed with a physician regarding what would happen to preserved biological materials in the case of death. Except for one adolescent male, Idan (age 14, diagnosed at 12), who was unsure whether such a discussion took place, all participants responded that they did not discuss this matter with a physician. Ofer (age 15, diagnosed at 14) added that he was aware that it was a “hot topic” in Israel,
[b]ecause when there are soldiers that die and they take the sperm. Then the parents decide what to do with it. Sometimes they have a child with a surrogate woman or anything else – if he had a wife or a girlfriend.
In addition to registering the lack of such discussion, Lily (age 17, diagnosed at 16) said, “Also the type of cancer I had, the percentages of death are … really, really, really, really small. Most, eh, recover from it completely and for most it doesn't at all return.”
One mother, Sharon (mother of Rachel – age 16, diagnosed at 14) admitted, “I didn’t know you could do something with it [after death].” She also specifically requested the interviewer not to ask this question of her daughter. Additionally, two mothers shared their reticence and difficulty over even imagining such a scenario. Simona (mother of Dalia – age 16, diagnosed at 15) said, “This topic wasn't raised. And I … don't [mentally] get into it, even.” Similarly, Dana (mother of Avi – age 15, diagnosed at 13) replied, “No and I also don't want to think about it.”
Despite lack of discussion recall, participants were asked what they thought might happen with their cryopreserved biological materials in the case of death. Though most participants admitted to having not thought about such a scenario, a couple of adolescent females conjectured that they would donate their ova or ovaries. Na’amah (age 19, diagnosed at 15) explained, “I understand that there is like the possibility to donate. Right?” Inbar (age 18, diagnosed at 16) said, “I like thought, myself, that if I, if I won't use it, I would be happy to donate it to someone who will need.”
A few mothers said they had briefly thought about what they would do in case the preserved materials were unused including: destruction, donation, or use within the family. For example, Sara (mother of Tamara – age 17, diagnosed at 15) mused, “Sometimes, there were some thoughts, what … let’s say that everything will be alright and she’ll have children [via coitus]. What do we do with it from there? If we destroy it or donate it?” Daphna (mother of Lily – age 17, diagnosed at 16) shared,
I don’t think that I would do something family-wise with them. That's to say I don't think that I would preserve them in the case that one of my girls maybe won't be fertile, so I would give them. No. I wouldn’t do this. Between me and myself, is what I'm telling you.
In contrast, Orna (mother of Inbar – age 18, diagnosed at 16) admitted, “I-, just a personal opinion, I believe that-, I don't know. I would think of something … . Maybe offer them to her sister or … . Maybe for me – it's a little hallucinatory, but eh, I don't know.”Footnote9
Additionally worth noting is a comment by Daphna (mother of Lily – age 17, diagnosed at 16), who did not think that doctors should talk about what will happen in the case of death. When asked why, she replied, “Because it’s not an option for my daughter to die.”
Discussion
The vast lack of recall regarding discussion of posthumous use of cryopreserved materials is surprising not only in light of international guidelines which specify that patients’ posthumous directives for preserved biological materials should be discussed and recorded (ESHRE Task Force on Ethics and Law Citation2004; Ethics Committee of the American Society for Reproductive Medicine Citation2013a), but also because of the highly contentious matter of PAR in Israel today. This finding indicates a reticence among healthcare professionals to discuss this matter or the challenge of discussing this matter in ways that register with adolescent patients and their families. Further research is necessary to explore current clinical norms of practice in Israel, as well as physicians’ recall and patients’ medical files (Barlevy et al. Citation2019). This third perspective is critical for a more complete picture of these discussions.
FP can be considered what Sarah Franklin calls “hope technology” (Franklin Citation2002). It may not only serve as somewhat of an “insurance” against infertility (that participants hope they never have to use) and give a sense of securing the future possibility of having a genetically-related child. FP may also subconsciously provide patients with hope for survival after cancer treatment.Footnote10 In light of this, discussing posthumous plans of cryopreserved materials is particularly challenging for all involved.
Undoubtedly, discussing death with any patient facing a serious diagnosis, such as cancer, is difficult, especially for healthcare professionals who are far more accustomed to serving in a medical advisory role than a psychosocial advisory one (Lakhani Citation2003). However, such discussions may prove to be even more challenging for healthcare professionals when the patient is an adolescent. While it is recommended for healthcare professionals to discuss death in a direct, honest, and realistic manner with adolescent patients, allowing them time for introspection, it is crucial to work with parents to specifically identify the individual needs of the adolescent and be sensitive to the wishes of the family (Nielson Citation2012). As the quotes above from several mothers denote, it also may be necessary to address parents’ fears and insecurities over the possibility of their child’s death.
To best tackle this sensitive issue physicians should explain to adolescent patients and their parents that posthumous planning of cryopreserved materials is not solely done for cancer patients, but for anyone who undergoes FP (Crawshaw et al. Citation2004). Additionally, physicians should emphasize that premature death could occur for reasons other than cancer or its recurrence. In fact, accidents are the leading cause of premature death in adolescents and young adults (Heron Citation2018). Such discussions should occur, and posthumous directives ought to be obtained after procurement. Discussing the topic prior to procurement can add stress to the provider and can therefore complicate sample collection, particularly in the case of sperm (Bahadur Citation1996).
Thus, healthcare professionals should undergo training in how to best communicate this sensitive matter. Such training will help them feel more comfortable discussing psychosocial matters with patients. Furthermore, not only reliance on, but collaboration with psychosocial healthcare providers is crucial, especially when adolescent patients and/or parents may need assistance in processing fears and insecurities regarding death.
Additionally, it is important to emphasize that in this study all adolescent participants’ intended to self-use cryopreserved materials in the future only in case of necessity (i.e. if she or his partner could not get pregnant via coitus). Parent participants provided complementary responses to those of adolescents’ intended self-use. Thus, the purpose of FP for these individuals is significantly different than the presumed possible use of soldiers’ cryopreserved sperm samples, especially in the context of previously cited studies investigating Israeli attitudes regarding PAR. Sperm of combat soldiers is specifically cryopreserved not only for self-use in case of injury, but also in case of death, so that it may be used by the deceased’s partner. In contrast, adolescent cancer patients and their parents do not give much thought to the use of cryopreserved gametes and reproductive organs/tissue in case of death. The purpose of FP for these individuals is to use cryopreserved materials for themselves only if they will experience reproductive challenges. Use by third parties is an afterthought, if at all.
Interestingly, despite lack of recall about discussion of posthumous plans for cryopreserved materials, some female participants shared their personal thoughts on what they thought might be done with cryopreserved materials in the case of adolescent death or lack of self-utilization. Both adolescents speculated that their cryopreserved materials could be donated for someone else to use. Theoretically, this would be possible in the case of their death, considering that these adolescents are not married, since donations from married women in Israel is forbidden. However, the ethical considerations in the use of a deceased minor’s gametes or reproductive organs/tissue for reproduction are complex, as discussed below.
Additionally, three mothers shared their ideas for plans of cryopreserved materials in the case that their daughters do not use them. Sara was unsure whether to donate or destroy them. It is not clear whether donation should be directed for reproductive use or medical research. While Orna considered possibly saving them for use within the family (e.g. in case of the provider’s sister having fertility problems), Daphna was staunchly opposed to such an idea.
It is evident from these few participants’ remarks that adolescents and their parents are not aware of the legal options available to them in Israel regarding cryopreserved materials in the case of provider death or lack of use. Seeing as Orna expressed plans that are explicitly forbidden in Israel, it is crucial to educate healthcare professionals – in Israel and elsewhere – about the legalities of posthumous donation or destruction of cryopreserved materials and for them in turn to inform their adolescent patients and their parents.
An initial cursory review of Clalit’sFootnote11 written FP consent forms indicate that only its sperm cryopreservation form mentions what happens in the case of death: destruction. Clalit’s consent forms for ova or ovarian cryopreservation do not include any stipulation with regards to patient death. It is unclear why this discrepancy exists between cryopreserved sperm and ova/ovarian cryopreservation. (While further review of FP consent forms offered by other healthcare funds goes beyond the scope of this paper, such review is needed to inform Israeli guidelines and policy.) Relegating the professional obligation to inform patients about their options to a singular clause in a consent form is not enough. While worldwide it is necessary for FP consent forms to include stipulations for cryopreserved materials in the case of provider death, healthcare professionals should still discuss the issue with families to avoid future quagmires in the profoundly unfortunate and upsetting situation of adolescent death.
Ethical issues associated with PAR using minors’ biological materials
While participants of this study did not directly raise the topic of PAR in their interviews, considering the pronatalist Israeli context, it is worthwhile to consider the ethical issues associated with PAR, especially when involving minors’ gametes or reproductive organs/tissue. First, the principle of respecting individuals’ autonomy gives credence to an individual’s capacity to make well-informed decisions in line with her/his values. Many ethical analyses of PAR often discuss the autonomy of the deceased as well as that of the surviving partner or parent(s). A deceased’s interest in PAR can be framed as an “indisputable” interest in genetic continuity (Affdal and Ravitsky Citation2019; Benshushan and Schenker Citation1998). Although an interest in genetic continuity also may be claimed by the surviving partner or parent(s), some authors question these survivors’ motivations, specifically drawing attention to their immediate state of grief (Landau Citation1999; Lawson, Zweifel, and Klock Citation2016; Schellinski Citation2014).
To address this issue, some recommend establishing a waiting period of between 6 and 12 monthsFootnote12 before survivors can use a deceased’s cryopreserved gametes for PAR (Bahadur Citation1996; ESHRE Task Force on Ethics and Law et al. Citation2006; Ethics Committee of the American Society for Reproductive Medicine Citation2013b; Lawson, Zweifel, and Klock Citation2016; Raziel et al. Citation2010). It is worthwhile noting that when comparing three types of bereavement of adults – i.e. over the death of a spouse, a child, or a parent – the case of parents surviving their child’s death generates significantly higher intensities of grief (Sanders Citation1980). Also noteworthy is the fact that prolonged counseling and delays often lead widows to not utilize their late husbands’ sperm (Bahadur Citation1996).
In the case of PAR, the motivation of potential recipients of cryopreserved gametes also needs to be considered. Some recipients might be solely motivated by their personal reproductive interests, possibly finding preferred traits within a donor’s profile that often times indicates a well-rounded and positive character (Pennings Citation2000). Others might be motivated by the idea of helping bereaved parents in their endeavors to become genetic grandparents, possibly seeking such a donation in order to intentionally foster a relationship between the future child and her/his genetic grandparents (Affdal and Ravitsky Citation2019). However, in the case of deceased minors’ cryopreserved biological materials, the notion of choosing based on the donor’s profile is challenging, considering that minors’ personalities are still very much in flux as compared with more mature individuals. Since minors do not have the legal competence to consent but only assent (Miller, Drotar, and Kodish Citation2004), use of their cryopreserved gametes for donation in the context of PAR raises ethical and legal challenges.
In the context of the Israeli norm of anonymous sperm donation, it is of interest to consider the advantages of using sperm from identifiable deceased donors, in contrast to anonymous sperm. Donated sperm in the context of PAR would be identifiable, and single women who use it may even wish to maintain a relationship with the parents of the deceased and allow them to take on the role of – genetic and social – grandparents (Affdal and Ravitsky Citation2019). This has already been the case in some PAR cases in Israel. It is thus conceivable that if courts decide to allow requests for PAR by parents of deceased minors, such cases may also end up with donated sperm to women who wish to use domestic identifiable, rather than anonymous, sperm.
Within the context of PAR, discussions of beneficence invariably include reflection upon furthering the well-being of a surviving partner or parent(s). Some argue that the wishes of living relatives is of utmost importance (Hashiloni-Dolev Citation2015). Others are wary of the benefits that PAR may bring to bereaved survivors, concerned that it could instead lead to the lengthening or complication of one’s mourning process (ESHRE Task Force on Ethics and Law et al. Citation2006; Landau Citation1999; Landau Citation2004). Discussions of “replacement children” (Schellinski Citation2014) or “memorial candles” (Landau Citation1999) raise concerns over the well-being of potential children born of PAR, who could carry unrealistic or burdensome expectations to fulfill an emotional gap or behave in some predetermined way (ESHRE Task Force on Ethics and Law et al. Citation2006; Lawson, Zweifel, and Klock Citation2016). Currently, it is neither possible to substantiate nor refute these concerns due to a lack of empirical evidence on the psychosocial well-being of children resulting from PAR (ESHRE Task Force on Ethics and Law et al. Citation2006; Lawson, Zweifel, and Klock Citation2016).
It is also worthwhile to consider how PAR may benefit the deceased. For someone who has an interest in genetic continuity and did not actualize that goal prior to death, designating her/his cryopreserved materials for PAR may offer some comfort while alive, thinking s/he could become a genetic parent after death (Aziza-Shuster Citation1994). Such considerations can lead to more philosophical discussions about the meaning of parenthood (Aziza-Shuster Citation1994; Robertson Citation1993).
Finally, with respect to the principle of justice, PAR challenges traditional arrangements of inheritance. With the various stakeholders involved in PAR, what inheritance rights can the future child legally claim? And what rights are transferred when these materials are donated to third parties? European guidelines recommend that a child born after the death of a parent be recognized as the child of that person and her/his inheritance rights be secured (ESHRE Task Force on Ethics and Law et al. Citation2006). This is already challenging when PAR is achieved by a surviving partner (due to the impact on existing children and their rights in relation to the deceased’s estate, in light of the birth of an additional child). When PAR is achieved by a surviving parent, and the deceased is a minor, inheritance issues can be further complicated. As for donation to third parties, guidelines suggest that the general rules of donation ought to apply, meaning that no inheritance or other rights are to be transferred to either recipient or offspring (ESHRE Task Force on Ethics and Law et al. Citation2006).
Conclusion
While destruction and use in research are the most conservative options for minors’ posthumous disposition of cryopreserved gametes and/or reproductive organs/tissue (with the former recommended by European and American guidelines), the question remains as to whether minors or their parents should be allowed to direct those materials to be used for PAR. To date, it has only been bereaved Israeli parents of children that reached the age of majority who requested to pursue PAR. However, in the pronatalist Israeli context, it seems that it is only a matter of time before bereaved parents of minors also make such requests. As evidenced by the study’s findings, some parents may wish to use cryopreserved biological material of their deceased adolescent children for future use within their family, e.g. by a sibling, which currently runs afoul of Israeli law. Scholars and policymakers everywhere should address relevant ethical and country-specific legal issues before such quagmires arise. Protection of the minor and her/his developing capacity to make such consequential decisions are matters which warrant further consideration.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes
1 Those of and prior to reproductive age.
2 Depending on jurisdiction, age of medical majority may be equivalent to or younger than age of legal majority. In Israel, the age of medical majority is the same as that of legal majority: 18. However, Israel’s Patient’s Rights Law stipulates that minors from the age of 14 may consent, without parental consent, to routine and simple medical treatment (CitationKol-Zchut). Though FP is technically an elective procedure, it cannot be categorized as “routine and simple medical treatment.”
3 Although these cases involve a mix of fallen soldiers, accident victims, and patients that died due to cancer, all involve individuals who died above the age of majority.
4 Israeli law, as in most English-speaking countries, is based primarily on the “common law” legal system. Common law is based on judicial precedent or case law. Jewish religio-legal, or halachic, decision-making is based on casuistry. In contrast, continental-European systems of civil law are based on codified law.
5 While IVF is state-funded, sperm and egg donation are not (Birenbaum-Carmeli Citation2016; Ministry of Health Citation2019a, Citation2019b).
6 Such requirements lead to a lack of domestic egg supply, which in turn leads many to acquire eggs from abroad.
7 Cross-border surrogacy is an option for single and gay Israelis, as well as heterosexual couples who wish to distance the surrogate from their lives. All related costs with cross-border surrogacy are covered by the commissioning persons (Birenbaum-Carmeli Citation2016).
8 The parents of all 28 invited adolescents were invited to be interviewed as well as 2 parents whose female adolescents were not invited because they were unaware that FP had been discussed. Protocol at the Israeli hospital where the study occurred is to inform minor patients’ parents about FP and to encourage inclusion of minor patients in these discussions.
9 Under current Israeli law, donation within the family is forbidden.
10 Though study participants did not bring this up in interviews, it is possible that such hope subconsciously exists. Future studies should specifically explore what FP means or represents to cancer patients.
11 Clalit is one of the four main public healthcare funds in Israel. Each healthcare fund has its own set of consent forms.
12 Although a relatively small minority of bereaved individuals demonstrate chronic symptoms, most return to normal levels of functioning by the end of the first year (Bonanno and Kaltman Citation2001).
References
- Abramov, Etty. “Our Heart is Beating Again (in Hebrew).” Accessed January 2, 2016. http://yedioth.ynet.co.il/articles/0,7340,L-4746072,00.html.
- Affdal, Aliya O, and Vardit Ravitsky. 2019. “Parents’ Posthumous use of Daughter’s Ovarian Tissue: Ethical Dimensions.” Bioethics 33 (1): 82–90.
- American Cancer Society Inc. 2011. Global Cancer Facts & Figures. 2nd ed. Atlanta: American Cancer Society.
- Aziza-Shuster, Evelyne. 1994. “Ethics and Society: a Child at all Costs: Posthumous Reproduction and the Meaning of Parenthood.” Human Reproduction 9 (11): 2182–2185.
- Bahadur, G. 1996. “Posthumous Assisted Reproduction: Posthumous Assisted Reproduction (PAR): Cancer Patients, Potential Cases, Counselling and Consent.” Human Reproduction 11 (12): 2573–2575.
- Barkan, Noam. “The Emotional Battle of Bereaved Parents: Let us Fertilize Our Son’s Sperm (in Hebrew).” Accessed April 4, 2017. http://www.ynet.co.il/articles/0,7340,L-4850474,00.html.
- Barlevy, D., T. Wangmo, S. Ash, B. S. Elger, and V. Ravitsky. 2019. “Oncofertility Decision Making: Findings From Israeli Adolescents and Parents.” Journal of Adolescent and Young Adult Oncology 8 (1): 74–83. doi:10.1089/jayao.2018.0016.
- Ben-Or, Gali, and Vardit Ravitsky. 2010. “Cultural Values in Action: The Israeli Approach to Human Cloning.” In Kin, Gene, Community: Reproductive Technology Among Jewish Israelis, edited by Daphna Birenbaum-Carmeli, and Yoram S. Carmeli, 226–251. New York: Berghahn Books.
- Benshushan, Abraham, and Joseph G Schenker. 1998. “The Right to an Heir in the Era of Assisted Reproduction.” Human Reproduction 13 (5): 1407–1410.
- Birenbaum-Carmeli, Daphna. 2016. “Thirty-five Years of Assisted Reproductive Technologies in Israel.” Reproductive Biomedicine & Society Online 2: 16–23.
- Birenbaum-Carmeli, Daphna, and Yoram S. Carmeli. 2010. Kin, Gene, Community: Reproductive Technologies among Jewish Israelis. New York: Berghahn Books.
- Bleich, J David. 1991. “SURVEY OF RECENT HALAKHIC PERIODICAL LITERATURE: In Vitro Fertilization: Questions of Maternal Identity and Conversion.” Tradition: A Journal of Orthodox Jewish Thought 25 (4): 82–102.
- Bokek-Cohen, Ya’arit, and Vardit Ravitsky. 2019. “Soldiers’ Preferences Regarding Sperm Preservation, Posthumous Reproduction, and Attributes of a Potential “Posthumous Mother”.” OMEGA-Journal of Death and Dying 79 (2): 132–156. doi:10.1177/0030222817725179.
- Bonanno, George A, and Stacey Kaltman. 2001. “The Varieties of Grief Experience.” Clinical Psychology Review 21 (5): 705–734.
- Braun, Virginia, and Victoria Clarke. 2006. “Using Thematic Analysis in Psychology.” Qualitative Research in Psychology 3 (2): 77–101. doi:10.1191/1478088706qp063oa.
- Cohen Friedman, Naama. “Tomer Died, and a Woman he Did not Know Will be the Mother of his Child (in Hebrew).” Accessed December 16, 2014. http://www.ynet.co.il/articles/0,7340,L-4603097,00.html.
- Crawshaw, M., A. Glaser, J. Hale, and P. Sloper. 2004. “Professionals’ Views on the Issues and Challenges Arising From Providing a Fertility Preservation Service Through Sperm Banking to Teenage Males with Cancer.” Human Fertility 7 (1): 23–30. doi:10.1080/1464727042000198087.
- ESHRE Task Force on Ethics and Law. 2004. “Taskforce 7: Ethical Considerations for the Cryopreservation of Gametes and Reproductive Tissues for Self use.” Human Reproduction 19 (2): 460–462.
- ESHRE Task Force on Ethics and Law, G. Pennings, G. de Wert, F. Shenfield, J. Cohen, P. Devroey, and B. Tarlatzis. 2006. “ESHRE Task Force on Ethics and Law 11: Posthumous Assisted Reproduction.” Human Reproduction 21 (12): 3050–3053. doi:10.1093/humrep/del287.
- Ethics Committee of the American Society for Reproductive Medicine. 2013a. “Fertility Preservation and Reproduction in Patients Facing Gonadotoxic Therapies: a Committee Opinion.” Fertility and Sterility 100 (5): 1224–1231.
- Ethics Committee of the American Society for Reproductive Medicine. 2013b. “Posthumous Collection and use of Reproductive Tissue: a Committee Opinion.” Fertility and Sterility 99 (7): 1842–1845.
- Franklin, Sarah. 2002. Embodied Progress: A Cultural Account of Assisted Conception. London: Routledge.
- Gross, Michael L, and Vardit Ravitsky. 2003. “Israel: Bioethics in a Jewish-Democratic State.” Cambridge Quarterly of Healthcare Ethics 12 (3): 247–255.
- Hashiloni-Dolev, Yael. 2015. “Posthumous Reproduction (PHR) in Israel: Policy Rationales Versus Lay People’s Concerns, a Preliminary Study.” Culture, Medicine, and Psychiatry 39 (4): 634–650.
- Heron, Melonie. 2018. “Deaths: Leading Causes for 2016.” In National Vital Statistics Reports 67 (6): 1–77.
- Kahn, Susan Martha. 2000. Reproducing Jews: A Cultural Account of Assisted Conception in Israel. Durham, NC: Duke University Press.
- Kol-Zchut. “Medical Care Minors May Receive Without Parental Consent.” Accessed November 27, 2019. https://www.kolzchut.org.il/en/Medical_Care_Minors_May_Receive_without_Parental_Consent.
- Lakhani, Shaheen Uddin. 2003. “Finding the Comfort Zone: Physicians’ Perspectives on Addressing Infertility with Adolescent Bone Marrow Transplant Patients and Their Parents.” Dissertation Abstracts International: Section B: The Sciences and Engineering 64 (4-B): 1906.
- Landau, R. 2004. “Posthumous Sperm Retrieval for the Purpose of Later Insemination or IVF in Israel: An Ethical and Psychosocial Critique.” Human Reproduction 19 (9): 1952–1956.
- Landau, Ruth. 1999. “Planned Orphanhood.” Social Science & Medicine 49 (2): 185–196.
- Lawson, Angela K, Julianne E. Zweifel, and Susan C. Klock. 2016. “Blurring the Line Between Life and Death: a Review of the Psychological and Ethical Concerns Related to Posthumous-Assisted Reproduction.” The European Journal of Contraception & Reproductive Health Care 21 (5): 339–346.
- Lee, Stephanie J., Leslie R. Schover, Ann H. Partridge, Pasquale Patrizio, W. Hamish Wallace, Karen Hagerty, Lindsay N. Beck, Lawrence V. Brennan, and Kutluk Oktay. 2006. “American Society of Clinical Oncology Recommendations on Fertility Preservation in Cancer Patients.” Journal of Clinical Oncology 24 (18): 2917–2931.
- Miller, Victoria A, Dennis Drotar, and Eric Kodish. 2004. “Children’s Competence for Assent and Consent: a Review of Empirical Findings.” Ethics & Behavior 14 (3): 255–295.
- Ministry of Health, State of Israel. 2019a. “Egg Donation.” Accessed February 6, 2019. https://www.health.gov.il/English/Topics/fertility/Pages/ovum_donation.aspx.
- Ministry of Health, State of Israel. 2019b. “Sperm Donation - Sperm Bank.” Accessed February 6, 2019. https://www.health.gov.il/English/Topics/fertility/Pages/sperm-bank.aspx.
- Nielson, Danelle. 2012. “Discussing Death with Pediatric Patients: Implications for Nurses.” Journal of Pediatric Nursing 27 (5): e59–e64.
- Okbi, Yasser. “The Court Confirmed: The Parents of a Deceased Soldier will be Able to Bring a Grandson from his Sperm (in Hebrew).” Accessed August 28, 2017. http://www.maariv.co.il/news/law/Article-597140.
- Pennings, Guido. 2000. “The Right to Choose Your Donor: A Step Towards Commercialization or a Step Towards Empowering the Patient?” Human Reproduction 15 (3): 508–514. doi:10.1093/humrep/15.3.508.
- Prainsack, Barbara, and Ofer Firestine. 2006. “‘Science for Survival’: Biotechnology Regulation in Israel.” Science and Public Policy 33 (1): 33–46.
- Ravitsky, Vardit. 2004. “Posthumous Reproduction Guidelines in Israel.” The Hastings Center Report 34 (2): 6.
- Ravitsky, Vardit, and Ya’arit Bokek-Cohen. 2018. “‘Life After Death’: The Israeli Approach to Posthumous Reproduction.” In Bioethics and Biopolitics in Israel, edited by Hagai Boas, Yael Hashiloni-Dolev, Shai J Lavi, Nadav Davidovitch, and Dani Filc, 202–220. Cambridge: Cambridge University Press.
- Raziel, Arieh, Shevach Friedler, Deborah Strassburger, Sarit Kaufman, Ana Umansky, and Raphael Ron-El. 2010. “Using Sperm Posthumously: National Guidelines Versus Practice.” Fertility and Sterility 94 (3): 1154–1156.
- Rimon-Greenspan, Hila, and Vardit Ravitsky. 2013. “New Frontiers in Posthumous Reproduction.” Accessed September 1, 2017. http://www.bionews.org.uk/page_313450.asp.
- Robertson, John A. 1993. “Posthumous Reproduction.” Indiana Law Journal 69: 1027.
- Sanders, Catherine M. 1980. “A Comparison of Adult Bereavement in the Death of a Spouse, Child, and Parent.” OMEGA-Journal of Death and Dying 10 (4): 303–322.
- Schellinski, Kristina. 2014. “Dreams and Existential Questions of Replacement Children.” Journal of Analytical Psychology 59 (2): 189–210.
- Shalev, Carmel. 1998. “Halakha and Patriarchal Motherhood—An Anatomy of the New Israeli Surrogacy Law.” Israel Law Review 32 (1): 51–80.
- Siegel, R. L., K. D. Miller, and A. Jemal. 2017. “Cancer Statistics, 2017.” CA: A Cancer Journal for Clinicians 67 (1): 7–30. doi:10.3322/caac.21387.
- Steinberg, Avraham. 2003. Encyclopedia of Jewish Medical Ethics. 3 vols. Jerusalem: Feldheim Publishers.
- Steinberg, Avraham. 2017. Jewish Medical Law & Ethics: Halakhic Rulings Pertaining to Patients, Physicians and Health-Care Policy Makers From Before Conception to After Death: With Clarifications, Comments and Sources [Hebrew]. Jerusalem: Avraham Steinberg.
- Wahrman, Miryam Z. 2005. “Fruit of the Womb: Aritificial Reproductive Technologies & Jewish Law.” Journal of Gender, Race and Justice 9: 109.
- Ward, E., C. DeSantis, A. Robbins, B. Kohler, and A. Jemal. 2014. “Childhood and Adolescent Cancer Statistics, 2014.” CA: A Cancer Journal for Clinicians 64 (2): 83–103. doi:10.3322/caac.21219.
- Young, Hilary. 2014. “Presuming Consent to Posthumous Reproduction.” Journal of Law and Health 27: 68.
- Zarchin, Tomer. 2011. “Parents Ask Court to Allow Use of Dead Son’s Sperm.” Accessed August 30, 2017. https://www.haaretz.com/1.5118630.
- Zemer, Moshe. 1999. Evolving Halakhah: A Progressive Approach to Traditional Jewish Law. Woodstock: Jewish Lights Publishing.
