
I would like to thank the authors for the letter to my paper ‘Another Evidence For Pressure Transfer Mechanism In Incomplete Partition Two Anomaly Via Enlarged Vestibular Aqueduct’. They indicated that the theory of pressure transfer via enlarged vestibular aqueduct (EVA) was mentioned in the past, and according to the present-day literature, genetics is accepted as the cause of hearing loss, rather than mechanical pressure transfer in EVA and incomplete partition type II (IP-II) cases. They concluded that it is proven that EVA is not a cause for cochlear anomalies.
I have a huge respect to the findings of other investigators but, my observations strongly indicate that there is a pressure transfer into the cochlea in EVA patients which, I think, plays a major role in the mechanism causing other pathologies in the cochlea and hearing loss in IP-II cases. There are four observations which make me regard pressure transfer as the cause of cochlear damage and hearing loss in this specific group of patients with IP-II:
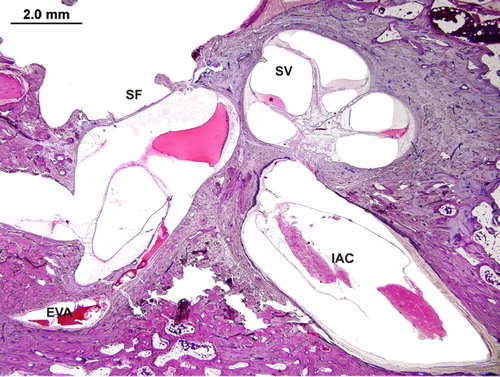
1. Histopathological evidence: In patients with EVA, there is dilatation in the scala vestibuli pushing interscalar septum upwards. This was already published before (Sennaroglu, Citation2016), but the figure is reproduced here once again (). It shows us that during embryological period there is a higher pressure in scala vestibuli, causing the interscalar septum to move upwards; if this had happened after ossification of the interscalar septum, one would have expected it to fracture. As it is intact and moved upwards, it likely means pressure changes took place in the cartilaginous phase during embryological development. It is difficult to find another logical explanation for the hydropic changes observed in the scala tympani, other than pressure transfer via EVA, that will move the interscalar septum upwards as in . This must be the earliest sign of IP-II; if there is more destruction in the modiolus and interscalar septa in IP-II, it is, most probably, due to more patent or larger EVA, causing earlier and more pressure transfer into developing cochlea.
Figure 1. An IP-II cochlea with scala vestibuli (SV) dilatation, in case of EVA (SF = Stapes footplate, IAC = internal auditory canal) (with permission of Department of Otolaryngology of Massachusetts Eye and Ear Infirmary and Cochlear Implants International).
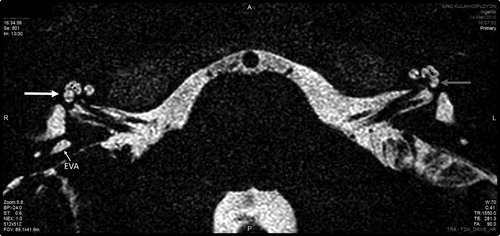
2. Radiological evidence: In the published paper (Sennaroglu, Citation2018), there is a dilatation in the scala vestibuli pushing interscalar septum upwards on the side with EVA (). This provides radiological evidence to the first point. On the contralateral side with normal vestibular aqueduct (VA), there is normal scala vestibuli showing that there is a role of EVA for the upward placement of interscalar septum.
Figure 2. Magnetic resonance imaging of the temporal bone. Right side: EVA, interscalar septum (two small black arrows) pushed upwards resulting in enlarged scala vestibuli (white arrow). Left side: No enlargement of vestibular aqueduct with normal scala vestibuli (grey arrow) and normal located interscalar septum (one black small arrow) (with permission of Cochlear Implants International).
3. Surgical evidence: In patients with IP-II, during surgery, once the round window is opened, it is very common to observe pulsation; usually there is no fluid leakage, but if a few millilitres of steroid are placed in the opening, there is a strong pulsation coming from inside of cochlea (https://youtu.be/snwqecEKQu0, ‘Pulsation IP-II’). This shows us that there is a strong pulsation inside the cochlea. This is not observed in normal cochlea or other cases of inner ear malformations and the most possible explanation is the pressure transfer via EVA.
My three observations show that there is a pulsating pressure inside the cochlea, in cases with EVA which is higher than normal, possibly causing modiolar defects in the cochlea.
4. Clinical observations: Progressive nature of hearing loss: this suggests that there is a continuation of the process causing hearing loss. We have many patients with normal hearing at birth, passing hearing screening tests but then developing progressive hearing loss in cases of IP-II. I am sure that such an observation is common to other clinicians in IP-II. It looks more possible to explain the progressive hearing loss observed in IP-II with this pulsating pressure, observed when the scala tympani is opened, which pushes the interscalar septum in scala vestibuli superiorly. It is more difficult to explain progressivity with genetic abnormality; it is more likely to observe stable hearing loss if only genetics were involved in the pathophysiology of cochlear destruction. This is the only group of inner ear malformation with progressive hearing loss most probably due to the pressure transfer via EVA.
Taking into account these four observations and previous genetic studies, I strongly believe that genetic abnormalities are the cause of enlarged vestibular sac and duct. Resultant anatomical defect in the otic capsule (EVA), which is larger than normal, allows pressure transfer into the cochlea. This causes various modiolar defects (which were classified before) (Sennaroglu, Citation2016) allowing pressure transfer only, sometimes oozing and rarely gusher to be seen during cochlear implant (CI) surgery. The timing of pressure transfer and efficiency of the pressure transfer is different between individuals (depending on the patency of EVA) and this is the reason why we see different pathologies: sometimes isolated EVA, sometimes EVA with modiolar destruction (IP-II) in different individuals.
My belief in the pressure transfer theory comes from my observations particularly, in the first three situations. Therefore, I would like to disagree with the authors’ comment that ‘I believe it has been proven beyond doubt now that vestibular aqueduct enlargement is not a cause for cochlear anomalies, rather they are just associations due to genetic/developmental reasons’. The present evidence strongly indicates that there is a pressure transfer into the cochlea via EVA.
References
- Sennaroglu, L. 2016. Histopathology of inner ear malformations: Do we have enough evidence to explain pathophysiology? Cochlear Implants International, 17(1): 3–20. doi: 10.1179/1754762815Y.0000000016
- Sennaroglu, L. 2018. Another evidence for pressure transfer mechanism in incomplete partition two anomaly via enlarged vestibular aqueduct. Cochlear Implants International, 19(6): 355–357. doi: 10.1080/14670100.2018.1489938