
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Objectives
To investigate the perception of interaural level differences (ILDs) in children with bilateral cochlear implants (BiCIs) and compare them to normal hearing peers. As intracranial shifts in perception of ILDs might have an effect on localization, this was further investigated.
Methods
ILD responses on four different frequency bands (broadband, low-pass, mid-pass and high-pass) were measured in 9 children with BiCIs and 15 children with normal hearing. In the children with BiCIs, 7 of them were implanted sequentially and 2 of them simultaneously. The outcomes were compared with the outcomes from a previous study on advanced localization using the same stimuli as in the current study. The effect of chronological age, inter-implant delay and preoperative residual hearing were also taken into account.
Results
No significant differences in ILD responses between children with BiCIs and children with normal hearing were found. For broadband stimuli, children with sequential BiCIs showed a significant shift in their response towards the first implant. A significant correlation was found between inter-implant delay and shift in ILD response for the broadband and high-pass stimuli. The shift in ILD response had no effect on localization.
Conclusion
Children with BiCIs are able to perceive ILD responses similar to those of normal hearing children. The inter-implant delay has a negative effect on the lateralization of the response towards the first implant side, indicative of deprivation of high-frequency sounds prior to receiving a second implant. This shift, however, is not associated with a shift in localization response.
Introduction
In many countries, bilateral cochlear implants (BiCIs) in children with severe to profound hearing loss are nowadays reimbursed. Due to this change in policy, older children suddenly were eligible candidates for a second cochlear implant (CI2). As the period of unilateral deprivation has a negative influence on the outcomes with BiCIs (Killan et al., Citation2019; Polonenko et al., Citation2018), within this group of children, children with significant residual hearing were especially thought to benefit from a CI2, because of the sufficient contralateral stimulation over the years.
The advantage of BiCIs over a unilateral cochlear implant (UCI) is the ability to perceive sounds from the right and left ear. In normal hearing subjects, binaural input enables sound source localization and improves the detectability of sound at lower levels in noisy environments (Akeroyd, Citation2006; Blauert, Citation1997; Wightman and Kistler, Citation1992). These advantages are the result of a very fine process of the bilateral input at the level of the brainstem. For sound source localization in the horizontal plane, the two most important cues are interaural differences in level and arrival time. Interaural level differences (ILDs) are most effective at high-frequency sounds (>3000 Hz), whereas interaural time differences (ITDs) are most effective at low frequencies (<1500 Hz) (Moore, Citation2003). Children with normal hearing show adult-like localization abilities by the age of 5 years (Grieco-Calub and Litovsky, Citation2010; Van Deun et al., Citation2009). In children with BiCIs, several studies showed bilateral advantages over hearing with a UCI in localization, although these outcomes were not comparable with their peers with normal hearing (Litovsky et al., Citation2006; Sparreboom et al., Citation2014). Due to the limited access to temporal fine structure information, it is likely that BiCI recipients only have access to weak ITDs from the envelope of the signal (Laback et al., Citation2004). In agreement, from various studies in children and adults with BiCIs, it seems that most participants primarily rely on ILD cues (Ehlers et al., Citation2016, Citation2017; Eklof and Tideholm, Citation2018; Gordon et al., Citation2014; Grantham et al., Citation2008; Litovsky et al., Citation2012; Salloum et al., Citation2010; Sparreboom et al., Citation2014). The difficulties in the perception of both ILD and ITD cues in BiCI users could be explained by the fact that both sound processors work independently. In many studies on ITD and ILD cues, however, this factor is excluded by direct stimulation of the electrodes, in which both the front-end processing and the coding strategy are not taken into account. Also, the insertion depth into the cochlea might differ between cochlear implants (CIs), which causes a mismatch in interaural frequencies. Kan et al. (Citation2013) showed that in case of a large mismatch in interaural frequency, the ITD cue was more often affected than the ILD cue in adults with BiCIs. Moreover, the period of binaural experience, the different neural survival between ears and/or maturational factors like asymmetry in arrival times between implant sides caused by sequential bilateral cochlear implantation, might also distort these cues needed for localization (Sparreboom et al., Citation2010). Another factor that might have an influence on optimal binaural hearing, is the fitting of the sound processors. At present, there is no consensus on how fitting should be performed in subjects with BiCIs. However, from research it seems that bilaterally loudness-balanced electrode pairs do not necessarily lead to a centred auditory image in adults with BiCIs (Fitzgerald et al., Citation2015; Goupell et al., Citation2013). When stimuli are presented diotically to both ears in normal hearing subjects, the sound is perceived intra-cranially as a centred auditory percept, whereas an ILD, leads to the perception of an intracranial shift towards the left or right side. Children with normal hearing, also experience a centred auditory percept (Ehlers et al., Citation2016; Salloum et al., Citation2010), although more variability is seen than in adults (Ehlers et al., Citation2016).
In the studies addressing ILDs in children with BiCIs, most studies make use of direct electrical stimulation of single electrodes to perform this task (Ehlers et al., Citation2017; Eklof and Tideholm, Citation2018; Gordon et al., Citation2014; Salloum et al., Citation2010), which is not representative of the perception of ILDs in daily life. From the studies using direct stimulation, all children experience an intracranial percept as a result of the ILDs, although some differences with normal hearing children were observed (Ehlers et al., Citation2017; Salloum et al., Citation2010). It also seems that children with BiCIs are less sensitive to smaller changes in ILDs than their peers with normal hearing (Ehlers et al., Citation2017). Eklof and Tideholm (Citation2018), showed a significant relationship between the just noticeable difference (JND) in ILD and broadband sound localization. The children in their study had small or no inter-implant delays. Because of possible differences in auditory pathway maturation between the two implant sides caused by a delay between implantations, this period might have an influence on ILD lateralization and consequently on localization. An advantage of using a lateralization task instead of a JND task in assessing the perception of ILDs is that information with regard to the interaural level balance is available. By using a lateralization task, an insight into the bilateral balance can be gathered by looking at the position of the psychometric curve of the ILD towards the centre. If the psychometric ILD curve is centred around 0 dB, one might hypothesize that the loudness between ears is balanced. This measure might be used in fitting procedures and/or can be compared to localization outcomes.
In the current study, lateralization of ILDs on four different frequency bands was measured in seven children with BiCIs implanted sequentially and compared to the outcomes in 15 children with normal hearing and two children with BiCIs implanted simultaneously. The children with sequential BiCIs had moderate-severe hearing loss prior to implantation of the CI2. Testing was performed with their own sound processor settings, to have a more realistic impression of their perception of ILD cues in daily life. Results were also compared to a previous study on localization using the same stimuli (Sparreboom et al., Citation2021). Both preoperative hearing loss and inter-implant delay were taken into account. The first question of the study was whether children with BiCIs show a clear psychophysical curve indicative of the perception of ILD cues and how does it relate to peers with normal hearing. The second question was if children show an intracranial shift of ILDs towards the left or the right side, was this also seen in a shift in localization using the same stimulus? Could a possible shift be explained by inter-implant delay? We hypothesized that children with BiCIs could perceive ILD cues, although to a lesser extent than children with normal hearing. We also hypothesized that a shift in ILD towards the first implanted side might be partly explained by the inter-implant delay, especially for high-frequency sounds. This ILD shift might yield a localization bias towards the first CI (CI1) side.
Material and methods
Subjects
Seven children with BiCIs implanted sequentially, two children with BiCIs implanted simultaneously and 15 children with normal hearing participated in the study. Children were at least 8 years of age. The children with BiCIs had a phoneme score in quiet at 65 dB SPL of at least 85% on the Dutch NVA test with their best performing CI, had a complete insertion of the electrode array and had at least one year of BiCI use. The children with BiCIs implanted sequentially had a phoneme score in quiet of at least 50% with the hearing aid (HA) prior to implantation of the CI2. The two children with BiCIs implanted simultaneously were implanted before the age of 18 months. All CI children were implanted with a Nucleus® multichannel device (Cochlear Corp, Australia) and used the ACE strategy. In the children with normal hearing, audiometric thresholds were obtained prior to testing. If thresholds between 250 and 8000 Hz exceeded 25 dB HL, children were excluded from the study. None of the children had reported learning and/or cognitive deficits.
The children with hearing loss were recruited via the Radboud University Medical Centre Nijmegen and the children with normal hearing via the first author. Testing was performed at the Radboud University Medical Centre Nijmegen. For this study, ethical approval was given by the Central Committee on research involving Human subjects of the Radboud University Medical Centre Nijmegen. In the subject characteristics are provided.
Table 1 Subject characteristics.
Fitting: the Nijmegen approach
The BiCI children all received fitting of their sound processors on a routine basis of once a year after the standard rehabilitation period of one year after implantation. During the fitting procedure, first the individual T- and C-levels are set. Afterwards, filtered speech-like sounds that are traceable to specific electrodes are used in the free field to balance loudness within and between CIs. During this procedure, the loudness of complex speech-like sounds was assessed by presenting the vowels [ʊ:], [ɑː], [iː] and consonants [tʃ] and [s] through a loudspeaker. Responses were given by the listener by pointing at a 5-item loudness scale from ‘little soft’ to ‘too loud’. Together, these sounds covered the speech spectrum. Each sound was presented 9 times without pause and therefore allowed loudness summation across electrodes and summation over a time span similar to that of a short sentence. Each sound was spectrally filtered to minimize spectral overlap between sounds, so that aberrant responses were traceable to specific electrodes and could be adjusted as the clinician seemed fit. Presentation at 75 dB SPL was used to assess the occurrence of discomfort; sounds presented at 65 dB SPL were expected to be of moderate loudness. Stimulus loudness was first assessed with both CIs separately. If sounds presented at 65 dB SPL were too soft or too loud, individual C-levels that correspond to the presented sound were adjusted in steps of 3 current levels. After the CIs were separately balanced, the loudness for both CIs was binaurally assessed. If loudness differed between sides, global C-level assessments were made in steps of 3 current levels.
Perception of ILD cues
Stimuli and task
The perception of ILD cues was measured with a child-friendly application on an I-pad, developed by the manufacturer in which two stimuli were repeatedly presented with ILD differences of between −20 and +20 dB SPL compared to the right side, with steps of 5 dB in between them. A two-alternative forced choice method was used in which the child had to indicate on the I-pad on which side the stimulus was heard. Children were encouraged to guess if they were not able to indicate if a stimulus was either heard from the left or the right. Before actual testing, a short unilateral training session was performed, to test the concept of hearing a stimulus on either the left or the right side.
The perception of ILDs was tested with four different types of stimuli with a duration of 150 ms and a presentation level of 60 dB (roving +/−3 dB). The four different stimuli were: a broadband stimulus (100–7938 Hz), a low pass filtered stimulus (100–1563 Hz), a mid-pass filtered stimulus (1563–3563 Hz) and a high-pass filtered stimulus (3563–7838 Hz). The three band-pass filtered stimuli were chosen to cover the whole range of frequencies provided by the CI. The number of repetitions per ILD difference was 8, which created a total number of 72 stimuli per condition. For the normal hearing children, stimuli were presented with a headphone placed over the ears (Beyerdynamic DT 770 PRO). The children with BiCIs were tested with the direct audio-input (DAI), in which no environmental sounds were presented. The test duration was approximately 15 min.
Data analyses
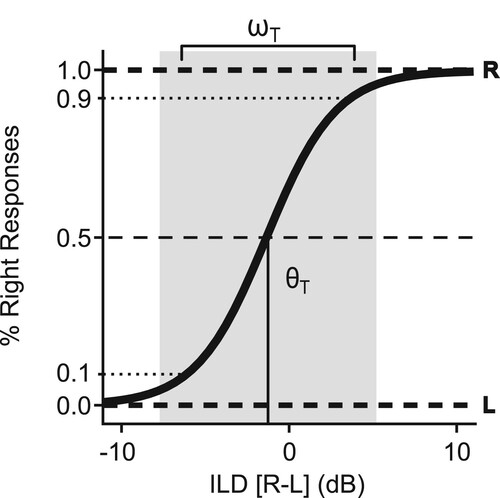
The psychophysical ILD data were described by performing a sigmoid fit over the binary left and right responses with the logistic function (1):
(1)
(1)
with the acoustic cue of the target in decibels and
the perceptual bias or shift in decibels. A negative bias indicates a shift towards the right or CI1 side, whereas a positive bias indicates a shift towards the left or CI2 side. The width or
in decibels is considered a measure that is indicative of how sensitive children are in perceiving ILD cues and it denotes the 10–90% width of the sigmoid. This is also illustrated by the example of the ILD fitting in .
Figure 1 An example of an ILD psychometric curve as described by Equation (1). The is the perceptual bias or shift in decibels, with a negative value indicating a shift towards the right or CI1 side and a positive value indicating a shift towards the left or CI2 side. In this example, a shift of −1.25 dB is shown, indicating no clear bias. The grey shaded zone indicates the width or
in decibels, which denotes the 10–90% width of the sigmoid. In this example the width is around 10 dB.
Influencing factors
To measure any influencing factors, correlation coefficients were used. The effect of chronological age on the acuity in ILD perception was tested in all children. The acuity in ILD perception was indicated by the width.
In the children with BiCIs, the effect of both residual hearing and inter-implant delay was assessed. Residual hearing was defined by the pure tone average (PTA) hearing thresholds over the frequencies 250 and 500 Hz (PTA250/500Hz).
ILDs and localization
Sparreboom et al. (Citation2021) recently published a paper on localization, spatial release of masking and fundamental frequency perception in children with CIs. In this study, the same children with normal hearing and with BiCIs were included as in the current study. The results on localization of the children with BiCIs and children with normal hearing from that paper were compared to the results on ILD perception from the current study. In particular, the parameter target bias (bT in degrees) was used to compare with the shift towards the CI1 (right) or CI2 (left) side. Localization was described by modelling the target-response relationship into a sigmoid function. The corresponds to the angle of deviation from the midline. A negative value indicates a bias towards the right side (or CI1 side) and a positive value toward the left side (or CI2 side). Correlation coefficients were calculated to investigate if the shift in ILD perception has an influence on the target bias in localization.
Statistical analyses
Data analyses were carried out in IMB SPSS Statistics 25. The level of statistical significance was set at an alpha of 5%. As we only included two children with BiCIs implanted simultaneously, their results were not included in the between-group analyses but described descriptively. The Shapiro–Wilk test was used for analysing the distribution of the data. As all data were not normally distributed, groups were compared using the Mann–Whitney test. Spearman’s rho was used to calculate bivariate correlation coefficients, in which the data of the simultaneously implanted children were also included.
Results
Perception of ILDs
In the children with normal hearing, in two out of the 15 children no data on the LP stimulus was gathered due to a technical issue. With regard to the children with BiCIs, there were no missing values.
All children perceived the ILD stimuli as one intracranial sound, although some children, both normal hearing and implanted, indicated that some stimulus types were easier to lateralize than others, with no clear pattern. In , the individual plots are shown for both the children with normal hearing and the children with BiCIs. For the children with normal hearing, three children were poorly able to perceive ILD cues, indicated by the outliers in width and the more shallow sigmoids in , whereas for the BiCI children only one child was considered an outlier.
Figure 2 ILDs for the different groups and stimulus types (BB, LP, MP and HP). The normal hearing children (NH) are shown at the top (A–D), whereas the sequential (SEQ) and simultaneous (SIM) BiCI children are respectively shown in the middle (E–H) and bottom (I–L) of the figure. The grey lines within the plots describe the individual results, whereas the bold lines indicate the mean for that particular group. For the NH and SEQ groups, the mean shift (θ) and width (ω) are depicted. For the SIM children, the individual values are listed. A negative value indicates an ILD towards the right or CI1 side and a positive value indicates an ILD towards the left or CI2 side. For the children with simultaneous BiCIs, no bold line was drawn. With the exception of three children, a steep ILD curve is observed in most children with normal hearing, indicative of good ILD perception.
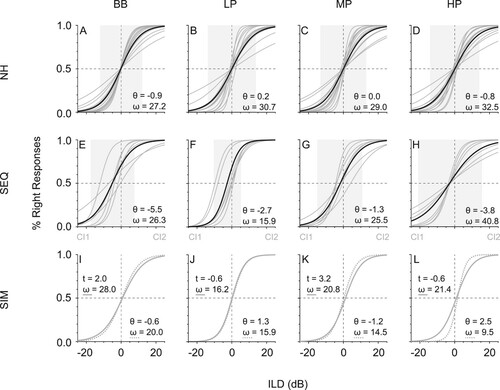
The results on ILD width and shift are depicted in . The median width of the sigmoid for the children with normal hearing was 17.2, 22.5, 22.3 and 23.5 dB for respectively the BB, the LP, the MP and HP stimulus, whereas the median width for the sequential BiCI children was slightly smaller with median values of 13.5, 14.9, 22.0 and 22.7 dB. The width between the two groups did not differ significantly (BB: U = 46.0, p = .680; LP: U = 33.0, p = .351; MP: U = 52.5, p = .1.0; HP: U = 46.0, p = .680). The median width of the two children with BiCIs implanted simultaneously were 24.0, 16.1, 17.7 and 15.5 dB for respectively the BB, the LP, the MP and the HP stimulus.
Figure 3 Scatterplot of ILD width (ωILD) against shift (θILD) for the different groups and stimulus types. A negative shift corresponds with a shift towards the right or CI1 side and a positive shift is a shift towards the left or CI2 side. No significant difference in ILD width between groups was found (p > .05). Compared to the children with normal hearing, children with sequential BiCIs showed a significant larger shift towards the CI1 side for the BB stimulus (A), but not for the other stimulus (p < .05).
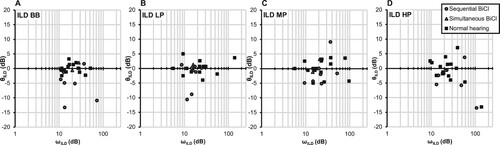
The results on the ILD shift only showed a significant difference between children with sequential BiCIs and children with normal hearing for the BB stimulus (U = 20.5, p < .05), but not for the other stimuli (LP: U = 33.5, p = .351; MP: U = 31.0, p = .142; HP: U = 32.0, p = .162). The children with BiCIs had a significant shift towards their CI1 for the BB stimulus with a median of 5 dB compared to the children with normal hearing, who showed median ILD shifts of 0 dB for all stimulus frequencies. ILD shifts for the children with BiCIs implanted simultaneously were also around 0 dB. Based on the outcomes in children with normal hearing, a shift between −5 and 5 dB is considered a centred response.
Influencing factors
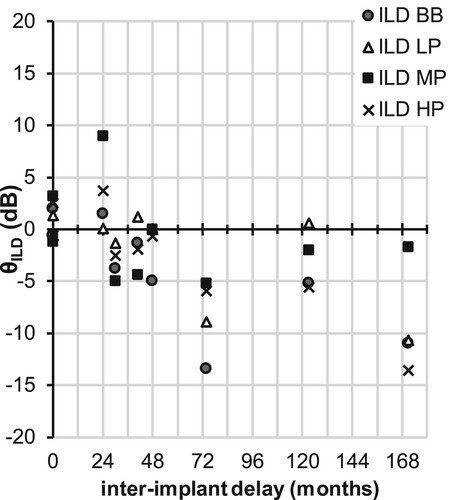
There was no significant effect of chronological age on the acuity of perceiving ILD cues as was indicated by no significant correlation between ILD width and chronological age (p > .05). Furthermore, in the children with BiCIs implanted sequentially, no effect of preoperative PTA250/500Hz was seen on either the ILD width or the ILD shift (p > .05). The effect of inter-implant delay was significant with regard to the ILD shift of the BB and HP stimulus (BB: ρ = −0.9, p < .01; HP: ρ = −0.9, p < .01). This indicates that the larger the inter-implant delay, the larger the shift towards the CI1 side for both the BB and HP stimulus ().
Figure 4 Scatter plot with inter-implant delay depicted against ILD shift (θILD) for the children with BiCIs. There is a significant negative correlation between inter-implant delay and the ILD shift for both the BB and the HP stimulus.
ILDs and localization
In , the relationship between the shift of the ILD plots and the sound localization target bias is shown. Although the responses of the BiCI children were a little bit off centre towards the CI1 side, no significant difference in target bias was found between the children with sequential BiCIs and the children with normal hearing for all stimulus frequencies (BB: U = 42.0, p = .490, LP: U = 30.0, p = .123; MP: U = 48.5, p = .783; HP: U = 45.0, p = .630). There was also no significant correlation between the shift of the ILD plots and the sound localization target bias (p > .05).
Figure 5 Scatterplot of ILD shift (θILD) against the target bias (bT) in localization for the different groups and stimulus types. In this Figure can be seen that when a shift in ILD is higher than 5 dB to the CI1 or CI2 side for the children with BiCIs, this shift is also seen in localization for S26 and S11, but not for S28.
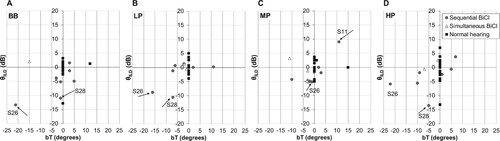
When taking a closer look at , only two children with sequential BiCIs had a shift higher than 5 dB towards the CI1 side, whereas one child had only in one condition (MP stimulus) a shift towards the CI2 side. One of the children that showed a shift towards the CI1 side also had large ILD widths (S28). The other child (S26) indicated that the CI1 sounded louder than the CI2. Although there was no correlation between ILD shift and target bias on localization, for these particular cases with ILD shifts off centre (>±5 dB), a target bias in localization was also seen. Therefore, although a significant correlation between inter-implant delay and ILD shift (BB and HP stimulus) was found, in some cases the shift in ILD might be the result of disbalance in loudness between CIs that might be solved by fitting.
Discussion
From this study, it became clear that children with BiCIs were able to perceive ILD cues presented to the subjects own sound processors via DAI. Compared to children with normal hearing, there was no significant difference in the perception of ILD cues in children with BiCIs as indicated by a similar width of the ILD curves. Both chronological age and the amount of residual hearing prior to implantation of the CI2 had no significant effect on the ILD width. As opposed to the children with normal hearing, who showed psychometric ILD curves centred around 0 dB, the children with sequential BiCIs showed a significant median shift of 5 dB towards the side of the CI1 for the BB stimulus. The shift in the ILD curve was also significantly correlated with inter-implant delay for the BB and HP stimuli, indicating that as inter-implant delay increased, the perception of the BB and HP stimuli were more towards the CI1 side. Although there was a significant shift for these stimuli in the children with sequential BiCIs, this did not lead to a significant shift in localization as was shown by the non-significant correlation between shift in ILD and localization target bias.
The shift in ILD might be explained by the difference in timing between the two implant sides. In a previous study from Sparreboom et al. (Citation2010) on electrically auditory brainstem responses (EABRs) in prelingually deaf children with sequential BiCIs, some interaural latency differences were seen, with the CI1 side showing faster responses than the CI2 side. The reason that the shifts towards the CI1 side were only significantly affected by inter-implant delay for the BB and HP stimuli, might be explained by the fact that these sequential BiCI children had significant residual hearing prior to implantation of the CI2, with better low-frequency hearing levels than high-frequency hearing levels. This resulted in longer deprivation of the high-frequency sounds, which might have caused a shift towards the CI1 side due to differences in pathway maturation. As all children perceived the ILD stimuli as one intracranial sound, sounds from both sides, however, seem to integrate. Another explanation for the shift in ILD, might be the fitting. This was presumably the case in the subject that indicated that the CI1 sounded louder than the CI2 in daily life. The other children, however, indicated no difference in loudness between CI sides in daily life. This is also seen in adults with BiCIs, in which bilaterally balanced electrode pairs does not necessarily lead to a centred auditory image (Fitzgerald et al., Citation2015; Goupell et al., Citation2013).
In contrast with other studies in both adults and children, ILD perception skills in our study were not significantly different between children with normal hearing and children with BiCIs (Ausili et al., Citation2020; Ehlers et al., Citation2016, Citation2017; Grantham et al., Citation2008). In the current study, no significant effect of chronological age was found on the ILD width. However, compared to ILD perception in adults with normal hearing and BiCIs in a similar test set-up, the children with normal hearing in our study showed larger widths with more variability (Ausili et al., Citation2020).
As the children with normal hearing showed adult-like localization skills in a previous study by Sparreboom et al. (Citation2021), it can be concluded that binaural hearing was mature, but that the ILD task, which involves higher cognitive functions, was difficult to perform, leading to less acuity and more variability in ILD perception. This is in agreement with other studies on ILD or ITD tasks (Ehlers et al., Citation2016; Peng et al., Citation2020), in which children showing more variability or immature decision-making strategies compared to adults.
A limitation of the present study was the low number of BiCI subjects included in the study. Nevertheless, although the study shows that the ILD task was not an easy task to perform in this particular age group, all children were able to perceive ILD cues. The measure might give some insight into the loudness balance between ears, but doing this the conventional way by a loudness scale seems more reliable and valid. With regard to gaining more insight into ILD perception of particular groups of children, both normal hearing and hearing impaired, it seems feasible. For future testing, the inclusion of an ITD task would also be very interesting to gain more insight into both basal cues necessary for localization in the horizontal plane.
In this study, children with BiCIs were able to perceive intracranial ILDs for BB, LP, MP and HP stimuli via presentation of the stimuli by DAI. The ILD psychometric curves were similar in width to those of children with normal hearing, indicating similar acuity in the perception of ILD cues. No effect of chronological age was found. As ILD perception within the current study was less accurate than seen in the literature for adults, the outcomes should be interpreted with care. For the BB stimulus, the ILD curve was significantly more shifted towards the CI1 side. The inter-implant delay had a significant negative effect on the shift towards the CI1 for both the BB and HP stimulus, indicating some form of deprivation for high-frequency sounds for longer inter-implant delays. The shift in ILD was not associated with a shift in localization target bias.
Disclaimer statements
Contributors All authors contributed to the study, with: MS, SA and EM designing the experiment and conceptualization; MS mainly collecting the data; MS and SA analysing the data; MS, SA and EM writing, reviewing & editing the manuscript.
Funding This project received partial financial support from Cochlear Benelux.
Conflicts of interest The authors report no conflict of interest.
Acknowledgements
This project received partial financial support from Cochlear Benelux. We thank all the children and their parents for their participation in this study. We also thank Seki Geelen for collecting the data and Robbert-Jan Miserus as a clinical investigator in this research project.
Additional information
Notes on contributors
M. Sparreboom
M. Sparreboom is currently employeed at the Radboud University Medical Centre Nijmegen in The Netherlands.
S. A. Ausili
S. A. Ausili is employeed at the University of Miami in the USA
E. A. M. Mylanus
E. A. M. Mylanus is currently employeed at the Radboud University Medical Centre Nijmegen in The Netherlands.
References
- Akeroyd, M.A. 2006. The psychoacoustics of binaural hearing. International Journal of Audiology, 45(Suppl 1): S25–S33. doi:https://doi.org/10.1080/14992020600782626.
- Ausili, S.A., Agterberg, M.J.H., Engel, A., Voelter, C., Thomas, J.P., Brill, S., et al. 2020. Spatial hearing by bilateral cochlear implant users with temporal fine-structure processing. Frontiers in Neurology, 11: 915. doi:https://doi.org/10.3389/fneur.2020.00915.
- Blauert, J. 1997. The psychophysics of human sound localization. 2nd ed. Cambridge, MA: The MIT Press.
- Ehlers, E., Goupell, M.J., Zheng, Y., Godar, S.P., Litovsky, R.Y. 2017. Binaural sensitivity in children who use bilateral cochlear implants. Journal of the Acoustical Society of America, 141(6): 4264. doi:https://doi.org/10.1121/1.4983824.
- Ehlers, E., Kan, A., Winn, M.B., Stoelb, C., Litovsky, R.Y. 2016. Binaural hearing in children using Gaussian enveloped and transposed tones. Journal of the Acoustical Society of America, 139(4): 1724. doi:https://doi.org/10.1121/1.4945588.
- Eklof, M., Tideholm, B. 2018. The choice of stimulation strategy affects the ability to detect pure tone inter-aural time differences in children with early bilateral cochlear implantation. Acta Oto-laryngologica, 138(6): 554–561. doi:https://doi.org/10.1080/00016489.2018.1424999.
- Fitzgerald, M.B., Kan, A., Goupell, M.J. 2015. Bilateral loudness balancing and distorted spatial perception in recipients of bilateral cochlear implants. Ear and Hearing, 36(5): e225–e236. doi:https://doi.org/10.1097/AUD.0000000000000174.
- Gordon, K.A., Deighton, M.R., Abbasalipour, P., Papsin, B.C. 2014. Perception of binaural cues develops in children who are deaf through bilateral cochlear implantation. PLoS One, 9(12): e114841. doi:https://doi.org/10.1371/journal.pone.0114841.
- Goupell, M.J., Kan, A., Litovsky, R.Y. 2013. Mapping procedures can produce non-centered auditory images in bilateral cochlear implantees. Journal of the Acoustical Society of America, 133(2): EL101–EL107. doi:https://doi.org/10.1121/1.4776772.
- Grantham, D.W., Ashmead, D.H., Ricketts, T.A., Haynes, D.S., Labadie, R.F. 2008. Interaural time and level difference thresholds for acoustically presented signals in post-lingually deafened adults fitted with bilateral cochlear implants using CIS+ processing. Ear and Hearing, 29(1): 33–44. doi:https://doi.org/10.1097/AUD.0b013e31815d636f.
- Grieco-Calub, T.M., Litovsky, R.Y. 2010. Sound localization skills in children who use bilateral cochlear implants and in children with normal acoustic hearing. Ear and Hearing, 31(5): 645–656. doi:https://doi.org/10.1097/AUD.0b013e3181e50a1d.
- Kan, A., Stoelb, C., Litovsky, R.Y., Goupell, M.J. 2013. Effect of mismatched place-of-stimulation on binaural fusion and lateralization in bilateral cochlear-implant users. Journal of the Acoustical Society of America, 134(4): 2923–2936. doi:https://doi.org/10.1121/1.4820889.
- Killan, C., Scally, A., Killan, E., Totten, C., Raine, C. 2019. Factors affecting sound-source localization in children with simultaneous or sequential bilateral cochlear implants. Ear and Hearing, 40(4): 870–877. doi:https://doi.org/10.1097/AUD.0000000000000666.
- Laback, B., Pok, S.M., Baumgartner, W.D., Deutsch, W.A., Schmid, K. 2004. Sensitivity to interaural level and envelope time differences of two bilateral cochlear implant listeners using clinical sound processors. Ear and Hearing, 25(5): 488–500. doi:https://doi.org/10.1097/01.aud.0000145124.85517.e8.
- Litovsky, R.Y., Goupell, M.J., Godar, S., Grieco-Calub, T., Jones, G.L., Garadat, S.N., et al. 2012. Studies on bilateral cochlear implants at the University of Wisconsin's binaural hearing and speech laboratory. Journal of the American Academy of Audiology, 23(6): 476–494. doi:https://doi.org/10.3766/jaaa.23.6.9.
- Litovsky, R.Y., Johnstone, P.M., Godar, S.P. 2006. Benefits of bilateral cochlear implants and/or hearing aids in children. International Journal of Audiology, 45(Suppl 1): S78–S91. doi:https://doi.org/10.1080/14992020600782956.
- Moore, B.C.J. 2003. An introduction to the psychology of hearing. 5th ed. New York: Academic Press.
- Peng, Z.E., Kan, A., Litovsky, R.Y. 2020. Development of binaural sensitivity: Eye gaze as a measure of real-time processing. Frontiers in Systems Neuroscience, 14: 39. doi:https://doi.org/10.3389/fnsys.2020.00039.
- Polonenko, M.J., Papsin, B.C., Gordon, K.A. 2018. Limiting asymmetric hearing improves benefits of bilateral hearing in children using cochlear implants. Scientific Reports, 8(1): 13201. doi:https://doi.org/10.1038/s41598-018-31546-8.
- Salloum, C.A., Valero, J., Wong, D.D., Papsin, B.C., van Hoesel, R., Gordon, K.A. 2010. Lateralization of interimplant timing and level differences in children who use bilateral cochlear implants. Ear and Hearing, 31(4): 441–456. doi:https://doi.org/10.1097/AUD.0b013e3181d4f228.
- Sparreboom, M., Ausili, S., Agterberg, M.J.H., Mylanus, E.A.M. 2021. Bimodal fitting and bilateral cochlear implants in children With significant residual hearing: The impact of asymmetry in Spatial release of masking on localization. Journal of Speech Language and Hearing Research, 64(10): 4030–4043. doi:https://doi.org/10.1044/2021_JSLHR-20-00720.
- Sparreboom, M., Beynon, A.J., Snik, A.F., Mylanus, E.A. 2010. Electrically evoked auditory brainstem responses in children with sequential bilateral cochlear implants. Otology & Neurotology, 31(7): 1055–1061. doi:https://doi.org/10.1097/MAO.0b013e3181dbb33d.
- Sparreboom, M., Langereis, M.C., Snik, A.F., Mylanus, E.A. 2014. Long-term outcomes on spatial hearing, speech recognition and receptive vocabulary after sequential bilateral cochlear implantation in children. Research in Developmental Disabilities, 36C: 328–337. doi:https://doi.org/10.1016/j.ridd.2014.10.030.
- Van Deun, L., van Wieringen, A., Van den Bogaert, T., Scherf, F., Offeciers, F.E., Van de Heyning, P.H., et al. 2009. Sound localization, sound lateralization, and binaural masking level differences in young children with normal hearing. Ear and Hearing, 30(2): 178–190. doi:https://doi.org/10.1097/AUD.0b013e318194256b.
- Wightman, F.L., Kistler, D.J. 1992. The dominant role of low-frequency interaural time differences in sound localization. Journal of the Acoustical Society of America, 91(3): 1648–1661. doi:https://doi.org/10.1121/1.402445.