

ABSTRACT
Introduction: In the past few years, administrating monoclonal humanized antibodies, namely checkpoint inhibitors, against programmed cell death protein 1 (PD-1), and its ligand (PD-L1), has yielded reassuring tumor regression rates. Anti-PD-1/PD-L1 checkpoint inhibitors disrupt the engagement of PD-1 on T-cells and their ligands on tumor or other target cells and reactivate the tumor-specific T infiltrating lymphocytes (TILs), which are mostly in a state of anergy before the PD-1/PD-L1 blockade. However, a limited number of patients initially respond, and the others show a primary (innate) resistance. Moreover, the rate of relapse and tumor progression after a partial, or even complete response (secondary or acquired resistance) is relatively considerable.
Areas covered: This paper presents a comprehensive discussion on the mechanisms of primary and secondary resistance to PD-1/PD-L1 blockade. Loss of T-cell infiltration or T-cell exclusion, lack of PD-L1 or PD-1 expression, and also lack of tumor immunogenicity are among the most important mechanisms, and also biomarkers of resistance in patients undergoing PD-1/PD-L1 blockade. Several somatic mutations in tumors are known to be related to at least one of the resistance mechanisms.
Expert opinion: Identification of the novel resistance mechanisms suggests further combinatorial therapies to tackle primary and secondary resistance to PD-1/PD-L1 blockade.
GRAPHICAL ABSTRACT
Article highlights
Response to anti-PD-1/PD-L1 therapy needs an adequate number of tumor-specific PD-1+ CD8+ TILs, an inflammatory tumor microenvironment, and proper cytokine secretion and sensitivity.
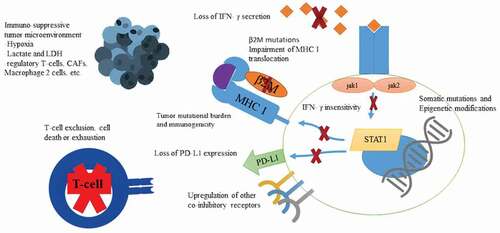
Lack of antigen presentation, PD-L1 expression, and insensitivity to interferon-gamma (IFN-γ) render tumor cells resistant to PD-1/PD-L1 blockade.
Tumors bearing an immunosuppressive tumor microenvironment, indicated by abundant regulatory T-cells and a low ratio of CD8+ effector/regulatory T-cells, are more probably resistant to PD-1/PD-L1 blockade.
Somatic mutations leading to the impairment of the major histocompatibility complex (MHC) class I complex recruitment, resistance to IFN-γ, upregulation of other co-inhibitory receptors than PD-L1 and decrease in the amount of tumor neoantigen can result in the acquired resistance to PD-1/PD-L1 blockade.
This box summarizes key points contained in the article.
Declaration of interest
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Reviewer Disclosures
Peer reviewers on this manuscript have no relevant financial relationships or otherwise to disclose.