
ABSTRACT
Objective
To estimate the cost-effectiveness of Cladribine Tablets in the treatment of relapsing multiple sclerosis (RMS) with high disease activity compared with fingolimod, from the perspective of the National Health System (NHS) in Spain.
Methods
A Markov model was developed. The annual transition probabilities, were adjusted to patients with RMS with high disease activity. The effect of the treatments compared on the Expanded Disability Status Scale (EDSS) was modeled by hazard ratios for the confirmed progression of disability. The annual relapse rate and the probability of suffering adverse reactions were obtained from a meta-analysis and the literature. The derived costs were calculated from Spanish unit costs. The utilities were obtained from the CLARITY clinical trial and the literature. Deterministic and probabilistic sensitivity analyzes were performed.
Results
Cladribine tablets was the dominant treatment: lower costs (−86,536 €) and more effective (+1.11 quality-adjusted life years – QALYs) compared to fingolimod. The probability that Cladribine Tablets was cost-effective compared to fingolimod ranged between 94.6% and 96.1% for willingness to pay from € 20,000 to € 30,000 per QALY gained.
Conclusions
Cladribine Tablets is a cost-effective treatment, compared to fingolimod, for the treatment of RMS with high disease activity.
Expert Opinion
According to the present study, compared to fingolimod, treatment with Cladribine Tablets of relapsing multiple sclerosis with high disease activity is an option that could generate savings for the Spanish National Health System, with a considerable gain in QALYs. Cladribine Tablets is considered cost-effective and dominant (less costs and more effectiveness) than fingolimod treatment option in this population.
1. Introduction
Multiple sclerosis (MS) is a disease of the central nervous system characterized by inflammation, demyelination and degenerative changes [Citation1]. It usually begins at between 20 and 40 years of age and affects women tree times more as men, being the most frequent cause of non-traumatic disability in the young adult population [Citation1,Citation2]. According to three recent studies, the prevalence of MS in Spain is estimated at between 65 and 90 cases per 100,000 inhabitants [Citation3–Citation5].
According to a cross-sectional Spanish study [Citation6], 92% and 64% of patients with MS analyzed experienced fatigue and cognitive problems, respectively, with a mean utility (quality of life as perceived by the patient) of 0.772 and costs per patient per year (from the societal perspective) ranging between 20,600 € with a score in the Expanded Disability Status Scale (EDSS) of 0 to 3 and 68,700 € with an EDSS score of 7 to 9. In Spain, the total annual cost of MS has been estimated at 1,4 billion euros (40% direct healthcare cost, 30% direct non-healthcare cost and 30% indirect cost) [Citation7].
The majority of patients with MS, between 85% and 90%, are diagnosed with relapsing MS (RMS) characterized by periods of acute exacerbation (relapses) followed by periods of remission of neurological symptoms [Citation6,Citation8,Citation9]. The European Medicines Agency (EMA) has approved fingolimod for the treatment of RMS with high disease activity for the following groups of patients: (i) Patients with highly active disease despite a full and adequate course of treatment with at least one disease modifying therapy; and (ii) Patients with rapidly evolving severe relapsing remitting multiple sclerosis defined by 2 or more disabling relapses in one year, and with 1 or more Gadolinium enhancing lesions on brain MRI or a significant increase in T2 lesion load as compared to a previous recent MRI [Citation10]. The EMA has also recently approved Cladribine Tablets in the treatment of adult patients with RMS with high disease activity defined by clinical or imaging features [Citation11].
The objective of this study was to assess the cost-effectiveness of both disease-modifying treatments (DMTs), Cladribine Tablets and fingolimod, in the treatment of RMS with high disease activity, from the perspective of the National Health System (NHS) in Spain.
2. Methods
2.1. Markov model
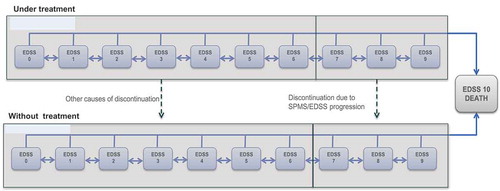
The characteristics of this model have been published previously [Citation12]. The analysis has been based on a Markov model simulating the evolution of a cohort of patients with RMS with high disease activity through different clinical situations (statuses of health), defined by the EDSS scale (10 statuses), which establishes the degree of disability and the progression of the disease. Each health status has associated costs and specific clinical consequences. The health statuses of the model are mutually exclusive; each patient in a hypothetical cohort can only be in one health status at any given time. shows the simplified scheme of the model, in which the transition between statuses and the relevant clinical and economic consequences were evaluated in cycles of 1-year [Citation12–Citation15]. For each annual cycle, the patients in each status can: (i) worsening in their illness (transition to a higher EDSS status); (ii) improve their status (transition to a lower EDSS status); (iii) maintain their status (remain in the EDSS status in which they are); or (iv) die.
Figure 1. Markov Model of 11 statuses (Hettle, 2018). Patients with RMS with high disease activity. EDSS: Expanded Disability Status Scale; RMS: relapsing multiple sclerosis; SPMS: Secondary progressive multiple sclerosis.
shows the annual probabilities of transition between the EDSS statuses, adjusted to the RMS with high disease activity [Citation12,Citation16]. offers a summary of the other premises and values adopted in the model [Citation10,Citation12,Citation15,Citation17–Citation33]. At the start of the analysis, the cohort of patients was distributed among the different health statuses (EDSS scores) according to the distribution observed in the CLARITY phase III clinical study [Citation20]. The population parameters of the cohort were adjusted to the patients of the CLARITY study, with an average age of 37.1 years[Citation20]. The average body weight was adjusted to the specific Spanish population, taking into account the average weight (68 kg) of three Spanish cohorts of patients with MS (total N = 701) [Citation3,Citation5,Citation34] ().
Table 1. Probabilities (%) per year of transition between EDSS statuses (age of MS onset ≥28 years), adjusted to the RMS with high disease activity [Citation12,Citation16]. EDSS: Expanded Disability Status Scale; RMS: relapsing multiple sclerosis.
Table 2. Premises and values adopted in the economic model.
It was assumed that patients with EDSS statuses between 0 and 6 were receiving treatment with a DMT, unless discontinued due to tolerability issues or the appearance of relapses (development of secondary progressive MS [SPMS]). Patients with EDSS statuses between 7 and 9 were assumed to not be receiving treatment with a DMT, in line with the usual clinical practice and current recommendations [Citation35].
Although it may be the case that in routine clinical practice patients may be switched to a different DMT following discontinuation (depending on the patient’s clinical history prior to the interruption), the model did not consider such sequencing in the absence of evidence to simulate the efficacy and safety of these therapies in patients who stop treatment.
The time horizon (duration) of the model was the life of the MS patient (50 years in an initial population with 37 years of age). An annual discount rate of 3% was applied both to the costs and to future effects (quality-adjusted life years [QALYs]) following the current recommendations in Spain [Citation36].
2.2. Clinical data
The probabilities of transition between statuses were based on the natural history of the disease [Citation16] and were adjusted with the data from the CLARITY study [Citation20] to represent the subgroup of patients with RMS with high disease activity (Table 1) [Citation12]. The effect of both DMTs (Cladribine Tablets and fingolimod) on the natural history of the MS was derived from the results of a network meta-analysis [Citation15] in which we estimated the hazard ratio of 3-month confirmed disability progression for Cladribine Tablets or fingolimod versus placebo, as well as the annualized relapse rate and the probability of treatment withdrawal [Citation15,Citation20] (). This meta-analysis included four clinical trials of fingolimod [Citation19,Citation21,Citation24,Citation26] and a clinical trial of Cladribine Tablets [Citation20], all of which were controlled with placebo. [Citation15] The transition probabilities were assumed to be constant over time. The occurrence of adverse events related to the treatments (progressive multifocal leukoencephalopathy, serious infections, macular oedema, cancer) were also considered in the analysis, obtaining their odds from several previously published studies [Citation12,Citation15,Citation18,Citation19,Citation21,Citation24,Citation26,Citation27].
The probability of death from any cause was assumed to be dependent on age, starting from the general mortality of the Spanish population [Citation37] and was adjusted according to the specific mortality of the MS. [Citation38]
2.3. Utilities
Utility is a measure of the preference for, or desirability of, a specific level of health status or specific health outcome. The health state utility is a cardinal number, between 0 (death) and 1 (perfect health) associated with a particular health state. Utilities for the EDSS statuses 0 to 5 were obtained from the CLARITY clinical trial [Citation20]. Utilities for the EDSS statuses 6–8 and 9 were taken from the studies of Hawton et al. [Citation29] and Orme et al. [Citation17], respectively. The loss of utilities associated with the adverse effects was also obtained from the medical literature [Citation28,Citation30,Citation33]. Finally, the loss of utilities that occurs in caregivers of patients with MS was taken from the study of Acaster et al. [Citation25] ().
2.4. Costs
Costs included in the model were the following: drug related costs (acquisition, administration and monitoring), costs based on disability and adverse events management costs.
The annual and four-year cost of the DMTs was obtained from the authorized public sale prices of each pharmaceutical company [Citation32], the recommended dosing regimens [Citation10,Citation11] and applying the deduction according to the Royal Decree-Law 8/2010 [Citation39]. The annual use of health resources (drug administration and monitoring) was estimated according to the recommendations of the Summary of Product Characteristics (SmPC) of Cladribine Tablets and fingolimod [Citation10,Citation11] and validated by an Advisory Board (Economic value of Cladribine Tablets: 4 July 2018 Bilbao; 17 July 2018 Valencia). Unit costs of associated healthcare resources were obtained from Spanish sources [Citation22,Citation23,Citation31,Citation40] ().
2.5. Sensitivity analysis
Deterministic and probabilistic analyses were carried out. Each parameter in the model varied between the limits of their 95% confidence intervals or of their credible intervals, or 50% of the means when the variances were not available [Citation12]. The probabilistic analysis was performed using a Monte Carlo simulation of the second order, with a hypothetical cohort of 1,000 patients.
There were also deterministic analyses for different scenarios: (i) time horizon of 10, 20, 30 and 40 years; (ii) annual discounts of costs and benefits of 0% and 6%; and (iii) excluding the loss of utilities of caregivers of patients with RMS with high disease activity.
3. Results
3.1. Deterministic base case
Treatment with Cladribine Tablets was cost-effective, generating lower costs (−86,536 €) and demonstrating greater effectiveness (+1.11 QALYs) than treatment with fingolimod, demonstrating that Cladribine Tablets is a dominant treatment in each patient with RMS with high disease activity (). presents the disaggregated results of the analysis. The saving was mainly due to the lower drug related cost: acquisition (in line with the SmPC, Cladribine Tablets is administered a maximum of 20 days in two courses of treatment [Citation10]), administration (Cladribine Tablets does not require the use of specific health resources for its administration [Citation10]) and monitoring (the use of resources needed to monitor Cladribine Tablets is reduced [Citation10]). The gain in QALYs was due to the delay in EDSS progression with Cladribine Tablets vs. fingolimod.
Table 3. The overall results of the deterministic cost-effectiveness analysis.
Table 4. Detailed results of the deterministic cost-effectiveness analysis.
3.2. Deterministic sensitivity analysis
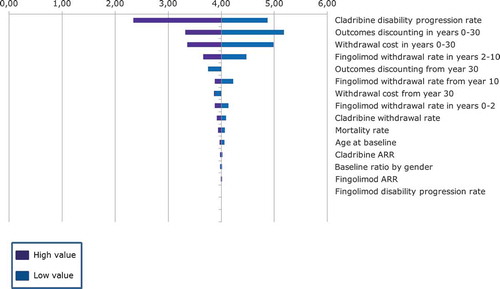
As can be seen in the tornado diagram shown in , for all the variables analyzed, there was a net positive health benefit, compared to fingolimod, with Cladribine Tablets being the dominant treatment.
Figure 2. Deterministic sensitivity analysis (tornado diagram). Net Health Benefit. ARR: annualized relapse rate. A positive net health benefit indicates that Cladribine Tablets is a cost-effective treatment compared to fingolimod.
presents the results of the deterministic sensitivity analysis for different scenarios for the time horizon, the annual discount costs and QALYs, excluding the loss of utilities in caregivers of patients with RMS with high disease activity from the analysis. In all analyses Cladribine Tablets was the dominant treatment compared to fingolimod.
Table 5. Results of the deterministic analysis of scenarios.
3.3. Probabilistic sensitivity analysis
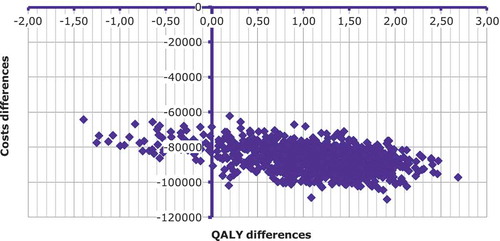
According to the probabilistic analysis (, ), compared to fingolimod, treatment with Cladribine Tablets of a patient with RMS with high disease activity would be cost-effective between 94.6% and 96.1% of the patients for willingness to pay 20,000 € to 30,000 € per QALY gained with the most effective treatment (Cladribine Tablets). In other words, the probability that fingolimod is cost-effective in comparison with Cladribine Tablets would range between 3.9% and 5.4% ().
Table 6. Detailed results of the deterministic cost-effectiveness analysis.
Figure 3. Probabilistic analysis. QALY: quality-adjusted life year. The likelihood that Cladribine Tablets is cost-effective compared to fingolimod ranged between 94.6% and 96.1% for willingness to pay between € 20,000 and € 30,000 per QALY gained.
4. Discussion
According to this analysis, compared to fingolimod, Cladribine Tablets would generate both economic savings as well as a gain of QALYs in patients with RMS and high disease activity. The volume of savings per patient in a lifelong treatment would be around 86,000 €. This saving is mainly due to drug acquisition cost (maximum of 20 days in two courses of treatment), drug administration (no use of specific health resources for its administration) and drug monitoring cost (reduced associated monitoring needed) [Citation41].
The gain of QALYs per patient in a lifelong treatment would be 1.11 QALYs according to the probabilistic analysis. It should be noted that a difference of 1.11 QALYs in favour of Cladribine Tablets versus fingolimod is very notable, given that generally it is thought that the minimally clinically important difference of utilities (i.e., that the patient is able to detect) between two interventions observed with the instruments EQ-5D, HUI2, HUI3 and SF-6D would be 0.074, 0.030, 0.030 and 0.033 QALYs, respectively [Citation41–Citation44].
The economic model simulated the evolution of a cohort of patients with RMS with high disease activity treated with Cladribine Tablets or fingolimod. For the adequate assessment of the results of the study we need to bear in mind both the possible limitations and their consistencies. With regard to the first, it must be remembered that this is a theoretical model that is, by definition, a simplified simulation of reality. A limitation of the model is the fact that the hazard ratios of confirmed progression of disability for Cladribine Tablets and fingolimod versus placebo were obtained through a network meta-analysis [Citation15], which analysed the subgroups of patients with RMS with high disease activity, because there are no clinical trials comparing both drugs in these patients. Another weakness of the study, common to many economic models, is that it was necessary to simulate the evolution of a hypothetical cohort of patients over the long term (between 10 and 50 years) on the basis of the data of clinical trials that had a maximum duration of 2 years [Citation15]. As in previously published analyses [Citation14,Citation45–Citation49] and in line with the SmPC for Cladribine Tablets, the study was modelled assuming that the results of effectiveness in 2 years would be extrapolated over the longer term. The evidence of the comparative effectiveness in the longer term of the DMTs versus placebo is limited for obvious ethical reasons [Citation12].
The greatest strength of the study lies in the stability of the economic model (the maintenance of the sense of the deterministic base case outcome in the sensitivity analyses), which was confirmed in all scenarios analysed. According to the probabilistic analysis, compared to fingolimod, treatment with Cladribine Tablets of a patient with RMS with high disease activity would be cost-effective between 94.6% and 96.1% of patients for willingness to pay 20,000 € to 30,000 € per QALY gained with Cladribine Tablets.
An analysis of the cost-effectiveness of the treatment of RMS with high disease activity in the United Kingdom (UK) has been previously published [Citation12]. According to this study, Cladribine Tablets was the dominant treatment, with a probability of cost-effectiveness of 93% for a willingness to pay 30,000 £ per QALY gained. The findings reported in this work are consistent with those reported in the UK cost-effectiveness study. No other analysis comparing the cost-effectiveness of Cladribine Tablets versus fingolimod in the RMS with high disease activity has been identified.
5. Conclusions
According to the present study, compared to fingolimod, treatment with Cladribine Tablets of RMS with high disease activity is an option that could generate savings for the Spanish NHS, with a considerable gain in QALYs in patients. Cladribine Tablets is considered a cost-effective and dominant (generating less costs and more effectiveness than fingolimod) treatment option in this patient population.
This evaluation, together with the convenient treatment regimen of Cladribine Tablets (maximum of 20 days in two courses of treatment, without specific health resources for its administration and its associated low monitoring consumption) may be useful to decision-makers in their assessment of the advantages of Cladribine Tablets as a new and valued option for RMS with high disease activity patients.
Article Highlights
The economic model simulated the evolution of a cohort of patients with relapsing multiple sclerosis (RMS) with high disease activity treated with Cladribine Tablets or fingolimod.
Treatment with Cladribine Tablets was cost-effective, generating lower costs (−86,536 €) and demonstrating greater effectiveness (+1.11 QALYs) than treatment with fingolimod, demonstrating that Cladribine Tablets is a dominant treatment in each patient with RMS with high disease activity.
The saving was mainly due to the lower drug related cost: acquisition (in line with the Summary of Product Characteristics, Cladribine Tablets is administered a maximum of 20 days in two courses of treatment), administration (Cladribine Tablets does not require the use of specific health resources for its administration) and monitoring (the use of resources needed to monitor Cladribine Tablets is reduced).
The gain in QALYs was due to the delay in Expanded Disability Status Scale (EDSS) progression with Cladribine Tablets vs. fingolimod.
The probability that Cladribine Tablets was cost-effective compared to fingolimod ranged between 94.6% and 96.1% for willingness to pay from € 20,000 to € 30,000 per QALY gained.
According to the present study, compared to fingolimod, treatment with Cladribine Tablets of RMS with high disease activity is an option that could generate savings for the Spanish National Health System (NHS), with a considerable gain in QALYs in RMS patients. Cladribine Tablets is considered a cost-effective and dominant (generating less costs and more effectiveness than fingolimod) treatment option in this patient population.
Declaration of interest
D Rubio Rodríguez is a Senior Consultant of Health Value, a company that has received fees in relation to the present study. C Rubio Terrés is Director of Health Value, a company that has received fees in relation to the present study. C Torres works in the PR & HEOR Area of Corporate Affairs Department of Merck. A Polanco leads the Department of Corporate Affairs of Merck. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Reviewer Disclosures
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Author contribution statement
JL Poveda, JL Trillo, C Rubio-Terrés, D Rubio-Rodríguez, A Polanco and C Torres made the adaptation of the economic model. C Rubio-Terrés and D Rubio-Rodríguez wrote the first draft. All authors interpreted the data and commented on the first draft. All authors revised the first draft. All authors agreed with the final version.
Disclosure statement
The abstract of this paper was presented at the ISPOR 21st Annual European Congress, 2018, Barcelona, as a poster presentation with interim findings. The poster’s abstract was published in Value in Health. 2018; 21: S339 (https://www.valueinhealthjournal.com/article/S1098-3015(18)35331-2/fulltext).
Correction Statement
This article has been republished with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
References
- Montalban X, Gold R, Thompson AJ, et al. ECTRIMS/EAN Guideline on the pharmacological treatment of people with multiple sclerosis. Mult Scler. 2018;24(2):96–120.
- MSSSI: Ministerio de Sanidad, Servicios Sociales e Igualdad. Estrategia en Enfermedades Neurodegenerativas del Sistema Nacional de Salud; 2016 [cited 2018 Jun]. Available from: http://www.msps.es/organizacion/sns/planCalidadSNS/pdf/Est_Neurodegenerativas_APROBADA_C_INTERTERRITORIAL.pdf
- Bártulos M, Marzo ME, Estrella LA, et al. Estudio epidemiológico de la esclerosis múltiple en La Rioja. Neurología. 2015;30(9):552–560.
- Izquierdo G, Venegas A, Sanabria C, et al. Long-term epidemiology of multiple sclerosis in the Northern Seville District. Acta Neurol Scand. 2015;132(2):111–117.
- Carreón-Guarnizo E, Andreu-Reinón E, Cerdán-Sánchez M, et al. Prevalencia de la esclerosis múltiple en la Región de Murcia. Rev Neurol. 2016;62(9):396–402.
- Oreja-Guevara C, Kobelt G, Berg J, et al. The European Multiple Sclerosis Platform. New insights into the burden and costs of multiple sclerosis in Europe: results for Spain. Mult Scler J. 2017;23(2S):166–178.
- Fernández O, Calleja-Hernández MA, Meca-Lallana J, et al. Estimate of the cost of multiple sclerosis in Spain by literature review. Expert Rev Pharmacoecon Outcomes Res. 2017;17(4):321–333.
- Weinshenker BG, Bass B, Rice GP, et al. The natural history of multiple sclerosis: A geographically based study. I. Clinical course and disability. Brain. 1989;112(Pt1):133–146.
- Confavreux C, Vukusic S. Natural history of multiple sclerosis: A unifying concept. Brain. 2006;129(Pt3):606–616.
- Gilenya 0,5 mg cápsulas duras. Ficha técnica o Resumen de características del producto; [cited 2018 Apr 13]. Available from: https://cima.aemps.es/cima/dochtml/ft/11677005/FT_11677005.html
- Mavenclad 10 mg comprimidos. Ficha técnica o Resumen de características del producto; [cited 2018 Apr 13]. Available from: https://cima.aemps.es/cima/pdfs/es/ft/1171212001/FT_1171212001.pdf
- Hettle R, Harty G, Wong SL. Cost-effectiveness of cladribine tablets, alemtuzumab and natalizumab in the treatment of relapsing-remitting multiple sclerosis with high disease activity in England. J Med Econ. 2018;21(7):676–686.
- Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology. 1983;33(11):1444–1452.
- Palace J, Duddy M, Bregenzer T, et al. Effectiveness and cost-effectiveness of interferon beta and glatiramer acetate in the UK multiple sclerosis risk sharing scheme at 6 years: a clinical cohort study with natural history comparator. Lancet Neurol. 2015;14(5):497–505.
- Siddiqui MK, Khurana IS, Budhia S, et al. Systematic literature review and network meta-analysis of cladribine tablets versus alternative disease-modifying treatments for relapsing-remitting multiple sclerosis. Curr Med Res Opin. 2017;34(8):1361–1371.
- Palace J, Bregenzer T, Tremlett H, et al. UK multiple sclerosis risk-sharing scheme: a new natural history dataset and an improved Markov model. BMJ Open. 2014;4(1):e004073.
- Orme M, Kerrigan J, Tyas D, et al. The effect of disease, functional status, and relapses on the utility of people with multiple sclerosis in the UK. Value Health. 2007;10(1):54–60.
- Tan K, Roda R, Ostrow L, et al. PML-IRIS in patients with HIV infection: clinical manifestations and treatment with steroids. Neurology. 2009;72(17):1458–1464.
- Cohen JA, Barkhof F, Comii G, et al. Oral fingolimod or intramuscular interferon for relapsing multiple sclerosis. N Engl J Med. 2010;362(5):402–415.
- Giovannoni G, Comi G, Cook S, et al. A placebo-controlled trial of oral cladribine for relapsing multiple sclerosis. N Engl J Med. 2010;362(5):416–426.
- Kappos L, Radue EW, Connor P, et al. A placebo-controlled trial of oral fingolimod in relapsing multiple sclerosis. New Engl J Med. 2010;362(5):387–401.
- Gubieras L, Casado V, Romero-Pinel L, et al. Cost of the relapse of multiple sclerosis in Spain. Value Health. 2011;14(5):A320.
- Karampampa K, Gustavsson A, Miltenburger C, et al. Treatment experience, burden and unmet needs (TRIBUNE) in MS study: results from Spain. Mult Scler. 2012;18(2 Suppl):35–39.
- Saida T, Kikuchi S, Itoyama Y, et al. A randomized, controlled trial of fingolimod (FTY720) in Japanese patients with multiple sclerosis. Mult Scler. 2012;18(9):1269–1277.
- Acaster S, Perard R, Chauhan D, et al. A forgotten aspect of the NICE reference case: an observational study of the health related quality of life impact on caregivers of people with multiple sclerosis. BMC Health Serv Res. 2013;13:346.
- Calabresi PA, Radue EW, Goodin D, et al. Safety and efficacy of in patients with relapsing-remittingmultiple sclerosis (FREEDOMS II): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Neurol. 2014;13(6):545–556.
- Pakpoor J, Disanto G, Altmann DR, et al. No evidence for higher risk of cancer in patients with multiple sclerosis taking cladribine. Neurol Neuroimmunol Neuroinflamm. 2015;2(6):e158.
- Shingler S, Fordham B, Evans M, et al. Utilities for treatment-related adverse events in type 2 diabetes. J Med Econ. 2015;18(1):45–55.
- Hawton A, Green C. Health utilities for multiple sclerosis. Value Health. 2016;19(4):460–468.
- Trogdon JG, Ekwueme DU, Chamiec-Case L, et al. Breast cancer in young women: health State utility impacts by race/ethnicity. Am J Prev Med. 2016;50(2):262–269.
- e-salud. Base de datos de costes sanitarios en España; 2017 [cited 2017 Nov]. Available from: http://www.oblikue.com/bddcostes
- BotPlus 2.0. Consejo General de Colegios Oficiales de Farmacéuticos (CGCOF); 2018 [cited 2018 Jan 11]. Available from: www.portalfarma.com
- NICE TA312. National Institute for Health and Clinical Excellence (NICE). Alemtuzumab for treating relapsing-remitting multiple sclerosis. NICE technology appraisal guidance 312; 2014 [cited 2016 Nov]. Available from: https://www.nice.org.uk/guidance/ta312?unlid=106213045220161014202829
- Llaneza MA Epidemiología de la esclerosis múltiple en el Área sanitaria de Ferrol. Tesis doctoral Universidad de la Coruña, 2016[cited 2017 Sep 14] . Available from: http://hdl.handle.net/2183/17565
- Scolding N, Barnes D, Cader S, et al. Association of British Neurologists: revised (2015) guidelines for prescribing disease-modifying treatments in multiple sclerosis. Pract Neurol. 2015;15(4):273–279.
- López-Bastida J, Oliva J, Antoñanzas F, et al. Propuesta de guía para la evaluación económica aplicada a las tecnologías sanitarias. Gac Sanit. 2010;24(2):154–170.
- The human mortality database; [ cited 11 de abril de 2018]. Available from: http://www.mortality.org/
- Rodríguez-Antigüedad Zarranz A, Mendibe Bilbao M, Llarena González C, et al. Mortality and cause of death in multiple sclerosis: findings from a prospective population-based cohort in Bizkaia, Basque Country, Spain. Neuroepidemiology. 2014;42(4):219–225.
- Real Decreto-ley 8/2010, de 20 de mayo, por el que se adoptan medidas extraordinarias para la reducción del déficit público. BOE Nº 126, Lunes 24 de mayo de 2010: 45070.
- Resolución de adjudicación. Suministro de productos y equipos necesarios para la realización de pruebas mediante Enzimoinmunoanálisis en el Laboratorio Central de la OSI Araba; [cited 2018 Sep 5]. Available from: http://www.contratacion.euskadi.eus/w32-1084/en/v79aWar/comunJSP/v79aObtenerFichero.do;jsessionid=fSLO1l59MGryeVEuGZ4GUYTIAj3qlo8pipVaKmOlpQOCubFtKA-E!-2033055975!-1619630890?identificador=140721&idTabla=007&R01HNoPortal=true
- Brazier J, Roberts J, Tsuchiya A, et al. A comparison of the EQ-5D and SF-6D across seven patient groups. Health Econ. 2004;13(9):873–884.
- Horsman J, Furlong W, Feeny D, et al. The Health Utilities Index (HUI): concepts, measurement properties and applications. Health Qual Life Outcomes. 2003;1:54.
- Walters SJ, Brazier JE. What is the relationship between the minimally important difference and health state utility values? The case of the SF-6D. Health Qual Life Outcomes. 2003;1:4.
- Wee H-L, Machin D, Loke W-C, et al. Assessing differences in utility scores: a comparison of four widely used preference-based instruments. Value Health. 2007;10(4):256–265.
- Tappenden P, Chilcott J, O’Hagan T, et al., [Internet]. Cost-effectiveness of beta interferons and glatiramer acetate in the management of multiple sclerosis: final report to the National Institute for Clinical Excellence; 2001 [cited 2018 Jan 31]. Available from: http://www.academia.edu/8908699/Cost_effectiveness_of_beta_interferons_and_glatiramer_acetate_in_the_management_of_multiple_sclerosis
- Tappenden P, McCabe C, Chilcott J, et al. Cost-effectiveness of disease-modifying therapies in the management of multiple sclerosis for the Medicare population. Value Health. 2009;12(5):657–665.
- Peninsula Technology Assessment Group (PenTAG) [Internet]. The effectiveness and cost-effectiveness of natalizumab for multiple sclerosis: an evidence review of the submission from Biogen; 2007 [cited 2018 Jan 31]. Available from: https://www.nice.org.uk/guidance/ta127/resources/multiple-sclerosis-natalizumabevaluation-report-evidence-review-group-report2
- Gani R, Giovannoni G, Bates D, et al. Cost-effectiveness analyses of natalizumab (Tysabri) compared with other disease-modifying therapies for people with highly active relapsing-remitting multiple sclerosis in the UK. PharmacoEconomics. 2008;26(7):617–627.
- Chilcott J, McCabe C, Tappenden P, et al. Modelling the cost-effectiveness of interferon beta and glatiramer acetate in the management of multiple sclerosis. Commentary: evaluating disease modifying treatments in multiple sclerosis. BMJ. 2003;326(7388):522.