
ABSTRACT
Objective
In 2018, 371,750 people were diagnosed with kidney cancer globally, constituting 2.2% of all cancer diagnoses. Since 2010, the number of kidney cancer deaths in Europe have decreased in people under 65. However, this is not the case in Greece and Portugal. This study estimated the mortality and lost productivity due to premature mortality from kidney cancer in Greece and Portugal.
Methods
Years of life lost (YLL) and present value of future lost productivity (PVFLP) due to kidney cancer mortality (ICD-10 code: C64 – Malignant neoplasm of kidney, except renal pelvis) were calculated using the human capital approach. Age-specific mortality, mean earnings, and labor force participation rates were used in these calculations.
Results
In 2019, there were 564 and 454 kidney cancer deaths in Greece and Portugal, respectively, resulting in 5,871 (3,636 in males and 2,234 in females) and 5,397 (3,100 in males and 2,297 in females) YLL, respectively. YPLL and annual PVFLP were estimated to be 1,326 and €14.8 M in Greece and 1,278 and €11.8 M in Portugal, respectively.
Conclusion
YLL and PVFLP due to kidney cancer mortality are substantial in Greece and Portugal. These results provide new evidence to assist decision-makers in allocating resources to reduce cancer burden.
1. Introduction
Kidney cancer is a type of malignancy that forms in the kidneys, developing from the renal parenchyma [Citation1]. Renal cell carcinoma (RCC) accounts for about 90% of kidney cancer cases in adults, and Wilms tumor (largely found in children) and transitional cell carcinoma are the other two main forms of kidney cancer. These types of cancer form in the tissues of the kidney that make urine. On the other hand, transitional cell cancer forms in the renal pelvis and ureter in adults [Citation2].
The Global Burden of Disease study from 2019 reports that the incident cases of kidney cancer were 371,750 which represents a 154.78% increase from 1990 [Citation3]. The study also reports that worldwide, kidney cancer has resulted in 72,100 deaths [Citation3]. The regions with the most incident cases of kidney cancer were high-income countries in North America, Western Europe, and East Asia. The European Cancer Observatory (ECO) estimates that in 2012, kidney cancer deaths accounted for 3.2% of all cancer deaths in Europe [Citation4]. There is large variability in the incidence and mortality of kidney cancer across Europe, with the highest rates observed in Eastern Europe. These variations in cancer rates may be due to variations in healthcare access, socioeconomic factors, population demographics, and cancer targeting policies [Citation1]. In addition to the variability reported, temporal trends in Europe have been reported by the ECO, with slight increases over time in some countries and stabilized incidence rates in already high-incidence countries in Eastern Europe [Citation4]. For this reason, targeted health policies are required to ease the humanistic and economic burden of this disease on the wider society.
Variations in mortality trends over time can be seen throughout Europe, with cancer mortality decreasing in high-income Western European countries and mortality increasing in Eastern European countries. This favorable trend of reduced mortality in high-income Western European countries has been reported since the 1990s and is in line with the adoption of improved cancer screening strategies which improve survival outcomes [Citation5]. However, this positive trend of decreased mortality was not observed across all European countries, including Greece and Portugal. It is not clear why Greece and Portugal do not follow the same trend as the rest of Europe, however it could be due to reasons including population demographics, health expenditure or access to care.
To tackle the various facets encompassing the burden of kidney cancer, evidence-based health policies with cancer screening at its core are required [Citation6]. Portugal’s National Cancer Plan (launched in 2016) promotes prevention, early diagnosis, and treatment of cancer [Citation7]. These aims are aligned with ‘Europe’s Beating Cancer Plan,’ launched in 2021 by the European Union, which has four focus areas: prevention, early detection, treatment, and improving the quality of life of cancer patients [Citation8]. Similarly, in Greece, following years of significant reductions in health expenditure due to austerity measures following economic instability, a plan that aims to adopt comprehensive approaches to modernizing public health services has been put into place [Citation9].
The treatment landscape for kidney cancer is evolving rapidly, with the development of new treatment paradigms, most recently with the introduction of targeted immune-oncology therapies. There is a growing body of evidence that recognizes the importance of quantifying the economic burden of kidney cancer, given that it plays an important role in decision-making and the efficient allocation of resources in the health sector [Citation10]. Estimating the costs associated with cancer goes beyond estimating direct health-care costs as cancer is a debilitating disease where patients accrue indirect costs, such as productivity losses. However, at the time of writing, no published literature on productivity loss due to kidney cancer in Greece and Portugal has been identified.
This analysis was conducted to estimate the monetary value of the productivity losses due to premature mortality from kidney cancer in Greece and Portugal in 2019. Greece and Portugal were selected for this analysis as these countries do not follow the same trend of decreased mortality in the population younger than 65 that is observed in other European countries (Supplement 1). While the overall kidney cancer deaths have been decreasing consistently each year from 2011 to 2019, in Greece and Portugal the number of deaths rates have fluctuated each year, with a slight rise in the rates across this same time period. However, as there are few deaths each year (less than 200 in each country), it is difficult to determine whether this is an upwards trend, or an artifact of the small sample.
This model quantified a key aspect of the societal costs resulting from premature kidney cancer-related mortality by calculating years of life lost (YLL), years of productive life lost (YPLL), and present value of future lost productivity (PVFLP). In addition to illustrating the impact of kidney cancer deaths on productivity losses, the results from this analysis provide valuable insights on the economic burden of kidney cancer further emphasizing the critical importance of shaping cancer control policies in these two countries.
2. Methods
2.1. Model structure
The human capital approach (HCA) was used to estimate labor productivity loss costs due to premature death from kidney cancer (ICD-10 code: C64 Malignant neoplasm of kidney, except renal pelvis) in Greece and Portugal. The methodology used is consistent with the study by Bencina et al., 2022 [Citation11] on the lost productivity due to head and neck cancer mortality in Hungary, Poland, and Romania.
The model has three primary outcomes of interest: YLL, YPLL, and PVFLP. To calculate these outcomes, the model considers kidney cancer-related deaths in 2019, with the potential costs being considered up to the life expectancy. As the model is focused on indirect costs of illness, direct costs, such as treatment costs, were not considered as patients only entered the model at death. The model population included kidney cancer patients who died in 2019 in Greece and Portugal, stratified by age groups to reflect varying kidney cancer-related mortality and labor productivity at different ages. When calculating YLL, deaths across all age categories were included; however, the years of life lost after the retirement age were not included in the YPLL and PVFLP calculations as productivity loss in this model were defined as loss of wages, and therefore this is not relevant after retirement. The default model retirement ages are country- and gender-specific. Although PVFLP calculations only considered kidney cancer patients before the retirement age, the total mortality was obtained by summing the number of deaths across all the age groups in the Eurostat database. For each kidney cancer-related death, the model used national life expectancy estimates to calculate the YLL.
For details regarding model calculations, refer to the publication by Bencina et al., 2022 [Citation11].
2.2. Inputs and assumptions
The model included epidemiological data to estimate YLL and YPLL and economic data to estimate PVFLP () [Citation12–18].
Table 1. Key inputs and data sources used in model.
2.2.1. Epidemiological inputs
Country-specific epidemiological inputs included age-specific mortality data and sex-specific life expectancy. Mortality data were derived from Eurostat () which stratifies mortality by country, age group, and cancer indication. Mortality was assumed to be uniformly distributed within each age group due to a lack of more granular data. Life expectancy data were used to determine the remaining years of life at the age patients die of kidney cancer. Country and sex-specific life expectancy estimates were sourced from the World Bank ().
2.2.2. Economic inputs
The model used country-specific economic inputs including mean annual earnings and labor force participation rates to estimate the PVFLP. The most recent available data before 2020 were used to account for the impact that COVID-19 has had on the labor market and annual earnings. Mean annual earnings were reported in Euros () and labor force participation rates were reported as percentages (). Direct costs that could have been incurred (e.g. future medical costs) were not considered as these are not associated with labor productivity losses.
The Eurostat database was used as the source for annual earnings, GDP, and labor force participation rates [Citation15, Citation16, Citation18, Citation18]. Mean annual earnings by age and sex were used in the base case and were estimated as an average of 29 statistical classifications of economic activities in the European Union (EU). Where the age categories in the Eurostat data did not correspond to the age categories used in the model, a weighted average was used to populate those in the model. For instance, for the 15–39 years age category, a weighted average of the ‘less than 30’ and the ‘30–49 years’ age categories from Eurostat were calculated.
Annual earnings were used in the base case as by definition GDP per capita is the GDP of a country divided by its total population and therefore, if GDP was used as a measure of income for the working population, it will be an underestimation of their true productivity, as it also includes those who are not working. So, while the use of annual earnings to measure productivity loss is not the most conservative assumption in terms of PVFLP, it is a more realistic assumption. In the model, individuals in the 0–14 age category were assumed to have a wage of zero. This assumption was based on the age category splits in the Eurostat mortality data where the model assumes the youngest age category (0–14) are unemployed but does not try to assume further splits in employment status in the next age category (15–39).
Unemployment rates represent the percentage of people within the labor force who are currently unemployed whereas the labor force participation rate considers everyone in the labor force including those who are currently unemployed but actively seeking employment. Country-level labor force participation rates were included in the PVFLP calculations in the base case as to provide a more conservative estimate of productivity losses when compared to using unemployment rates. Labor force participation was assumed to remain constant until the retirement age (66.5 years in Portugal and 67 years in Greece), as the data source used to populate the model assumes a constant labor force participation rate across the population. As such, these rates were only applied to the working-age population, assumed to be over 15 in this model.
Discounting was applied across the future costs to ensure that the present value was reflected in the total cost estimations. A 3% discount rate was applied annually to the potential future productivity value across the expected potential life for each age group modeled.
2.3. Sensitivity analysis and scenario analysis
A deterministic sensitivity analysis (DSA) was used to investigate the robustness of results to input parameters, by varying epidemiological and economic inputs, namely mortality, life expectancy, retirement age, measures of income and measures of unemployment. The univariate DSA varied parameters by a default range of ±10%. As both epidemiological and economic inputs were made up of population-specific data (e.g. mortality rates were stratified by age group and sex), all related inputs were varied simultaneously to model the impact in overall changes to every type of input. This was sufficient to observe a difference in outcomes and record the impact on the PVFLP/death in a single year’s mortality from kidney cancer.
Scenario analyses included the use of alternative input sources for key data values. GDP per capita by country (refer to supplementary materials, Supplement 3) was used in place of annual earnings, and unemployment rate (refer to supplementary materials, Supplement 4), in place of labor force participation. It was assumed that GDP per capita was equal across age groups whereas unemployment rates were age-specific.
3. Results
There was a total of 1,018 deaths, 11,268 YLL, and 2,604 YPLL in 2019 resuting from premature kidney cancer-related deaths in Greece and Portugal (). Total PVFLP in 2019 was €26,559,384 M across both countries. The results stratified by gender () show a total of 176 women and 388 men died in 2019 of kidney cancer in Greece. The number of deaths reported in Portugal were lower compared to Greece; however, a similar trend was observed in that considerably more deaths were recorded in males.
Table 2. Total number of deaths, YLL, YPLL, and PVFLP by country in 2019.
Table 3. Total number of deaths, YLL, YPLL, and PVFLP by country in 2019 stratified by sex.
Across the productivity-loss outcomes investigated, Greece showed more unfavorable labor productivity loss outcomes with a PVFLP/death of €26,172 compared to €25,987 in Portugal, and a YLL/death of 10 and 12, respectively. In Greece, there was a total of 5,871 YLL, 1,326 YPLL, and approximately €14.8 M PVFLP compared to Portugal which reported a total of 5,397 YLL, 1,278 YPLL, and approximately €11.8 M PVFLP. When comparing the two countries, the number of kidney-related deaths are slightly higher in Greece compared to Portugal (). However, when taking into account the population sizes of each respective country (10.7 M in Greece and 10.2 M in Portugal) [Citation24, Citation25], the mortality rates are similar.
The difference in total productivity losses associated with all kidney cancer-related deaths when stratified by sex revealed that the gap in productivity loss amongst men and women was larger in Greece ( and ). In 2019, the difference in YLL amongst kidney cancer-related deaths for men and women in Greece was 1,402 years, whereas the difference was 804 years in Portugal. Of the total YLL across both countries, 60% of this was in males. The difference in total YPLL attributable to kidney cancer in the same year was 498 years in Greece and 389 in Portugal. The difference in total PVFLP associated with all kidney cancer-related deaths amounted to approximately €6.7 M in Greece and €4.5 M in Portugal. Of the total PVFLP across both countries, 71% of productivity loss occurred in males.
Figure 1. Percentage of YLL and PVFLP by sex in 2019.
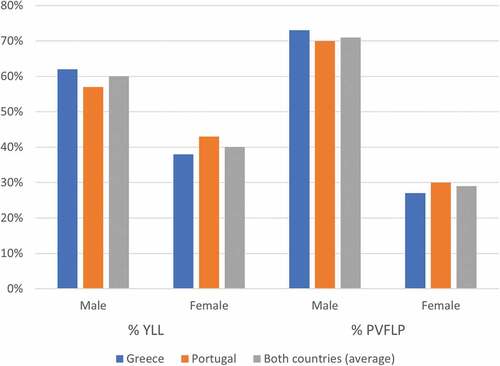
Table 4. Percentage of YLL and PVFLP by sex in 2019.
The DSA () showed that the PVFLP for kidney cancer-related deaths (total for Portugal and Greece) was most sensitive to changes in the retirement age, followed by the measure of productivity used (annual earnings in the base case). Consistent with the study by Bencina et al., 2022, no change in results was observed when mortality or life expectancy were varied in the DSA for two reasons. Firstly, when mortality is increased by a range of ± 10%, costs and mortality are also increased proportionally; therefore, no impact is seen on the results. Secondly, even when life expectancy is increased by a range of ± 10%, it never drops below the retirement age, therefore it does not change the impact on the YPLL and therefore the PVFLP. PVFLP estimates at the lower and upper values of the input parameters varied for the three timepoints are shown in .
Figure 2. DSA results for annual PVFLP per death varied using lower and higher input parameter values.
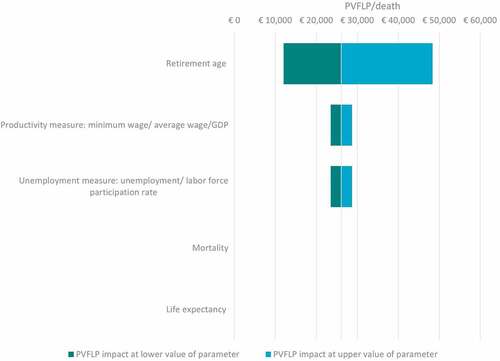
Table 5. PVFLP (€)/kidney cancer-death at the lower and upper values of the input parameters.
PVFLP: Present value of future lost productivity.
A scenario analysis using GDP and unemployment rate resulted in a higher PVFLP compared to the base case model settings which used annual earnings and labor for participation to calculate PVFLP. In 2019, PVFLP across the two countries exceeded €34.6 M when using the alternative inputs, as opposed to €26.6 M in the base case. Results by country in the base case compared to scenario analysis are presented in the Supplement 10.
4. Discussion
Europe currently has a decreasing trend in mortality due to kidney cancer, however this is not the case in Greece and Portugal. Based on this analysis, a total of 1,018 deaths from kidney cancer occurred in Greece and Portugal in 2019. Of the two countries, Greece reported the higher absolute number of deaths; however, when accounting for population size, the crude mortality rates were similar. When looking at the mortality results stratified by sex in Greece, the number of deaths in females was less than half the number of deaths reported in males (178 vs 388). A similar trend was observed in Portugal where 158 female deaths were reported compared to 296 male deaths. Analyzing mortality rate trends will allow decision-makers to understand the evolution of kidney cancer-related mortality in these two countries which will lead to more impactful policies in the future.
Based on these mortality data, a total of 11,268 years of life were lost in 2019 due to kidney cancer-related premature mortality. The model also estimated a YPLL of 2,604 years. In the base case setting, the YLL due to kidney cancer was estimated to cause a loss in productivity of approximately €14.8 M in Greece and €11.8 M in Portugal. Despite the conservative approach that was used in this model to estimate the PVFLP, significant losses of productivity have been estimated across both countries. Costs accrued due to premature kidney cancer-related mortality were estimated to exceed €26.5 M in 2019 in the two countries, reinforcing the need for efficient policies prioritizing kidney cancer prevention and treatments.
There are no previous studies investigating productivity losses specifically due to kidney cancer-related premature mortality in Greece and Portugal, however, studies have reported that productivity losses due to cancer mortality are upwards of hundreds of billions of dollars worldwide [Citation26]. The estimation of productivity losses varies depending on the methods and types of productivity losses included in the study, but in the EU alone they are estimated to be between €42.6 and €75.5 billion [Citation26]. Another study estimated that these productivity losses consisted of €50 billion due to premature mortality and €20 billion due to morbidity [Citation27]. This study is the first comprehensive study to estimate productivity losses due to kidney cancer-related premature mortality in these two countries specifically, providing crucial evidence that can be used to inform health policies in Greece and Portugal and the wider EU member states.
Although cancer prevention and treatment strategies have improved over the years, cancer diagnoses appear to be rising [Citation28]. The reasons behind this increase are not limited to environmental and lifestyle factors but can also be attributed to improved cancer screening methods which are expected to increase the number of cancer cases detected over time. Additionally, this could be attributed to the shift in population demographics (increased life expectancy) due to improvements in the treatment landscape and so, a greater proportion of the population is likely diagnosed with cancer in the long term. Kidney cancer is an important contributor to the morbidity and mortality from non-communicable diseases (NDCs) due to its high incidence with more than 400,000 new cases of kidney cancer diagnosed every year; an estimate projected to increase in the upcoming years [Citation29]. The pressing burden caused by this disease on the wider society is an area that should be actively addressed to meet the United Nation’s Sustainable Development Goal target to reduce premature mortality from NDCs by a third by 2030 [Citation30].
It is recognized that men are more frequently diagnosed with kidney cancer compared to women. A study reported that males are twice as likely to develop kidney cancer than females, with evidence pointing toward individual generic or pathological differences that affect the patient [Citation31]. This aligns with the findings of this model which illustrated higher male deaths, with 212 and 138 additional male deaths reported in Greece and Portugal in 2019, respectively. These results suggest a higher gap in mortality between the two sexes in Greece compared to Portugal. This variation can be attributed to various factors which include the exposure of the population to risk factors, which is more prominent in the Eastern spectrum of Europe as evidenced by the increased cancer incidence experienced in that region. Several risk factors for kidney cancer have been established including obesity, diabetes, hypertension, and smoking, however guidelines have failed to address the various sex-related differences with regard to the distribution of kidney cancer-related risk factors [Citation1]. The gap between the sexes was also observed when comparing the productivity losses where PVFLP was higher in males in both countries (additional 6.7 M in Greece and 4.6 M in Portugal). Analyzing these trends with the aim of providing sex-specific treatment will allow European countries to offer precision medicine to patients affected by kidney cancer, a growing area of medicine requiring further research and development [Citation32].
Consistent with the YPLL findings from this study, other studies have also shown that premature kidney cancer-related mortality can lead to substantial economic burden from absenteeism and loss of productive life years [Citation33]. It is recognized that the disease stage has a direct impact on the extent of the productivity losses as progressed disease is associated with shorter survival outcomes. Moreover, these findings support the rationale to implement strategies targeting sex-specific improvements in productivity [Citation33].
Given the substantial losses estimated in this model, kidney cancer consolidates itself as a significant contributor to the overall productivity costs due to cancer mortality in Europe, particularly in Greece and Portugal where kidney cancer mortality rates appear to be on the lower end of the spectrum showing an expectation of a high burden in other nations where mortality rates are higher. A multidisciplinary plan of action that considers all factors that are contributing to the premature mortality of working-age patients affected by kidney cancer is therefore needed to alleviate this burden. In addition to preventative and screening measures, improvements in the current kidney cancer treatment landscape which resulted in improved patient outcomes play a significant role in reducing productivity losses.
Consistent with the study by Bencina et al., 2022 [Citation11], this model presents a robust modeling approach to quantify productivity losses due to kidney cancer using reliable data sources. The model was based on publicly available datasets from reputable organizations including the WHO, the Eurostat database, and World Bank. Another strength of this model was the use of country-specific input values which are reflective of the local setting (e.g. local retirement ages, etc.). Moreover, the study uses gender-specific annual earnings, retirement ages, and life expectancies. This is particularly important when estimating productivity losses in kidney cancer as the lifetime risk of developing this type of cancer is higher in men than women [Citation34]. If sex differences were not accounted for, the model would overestimate the productivity losses as, on average, men are in employment for longer and earn higher wages [Citation35].
Nonetheless, this study also presents some limitations which include the simplification of input parameters due to the complexity of real-world data, and the availability of data. The impact of gender and age on mortality and wages was incorporated in detail, however these were still grouped into age categories rather than modeling each age. Furthermore, a single labor force participation rate is applied to the population in each country. In addition, the model assumed that children under the age of 14, and adults over the retirement age, did not participate in paid work. This assumption will mean that the calculated productivity losses are conservative, as patients in those age categories might participate in paid work.
As the model focused on the impact of premature on productivity loss from a societal perspective, this study does not account for direct costs of kidney cancer to the healthcare system, such as drug or surgery costs, and it does not therefore capture the overall economic burden of this cancer indication. The direct costs of kidney cancer in these countries would be an interesting future study that would add to the evidence base regarding the burden of this disease in Greece and Portugal.
Another limitation of the model is the narrow definition of ‘productivity losses’ which is limited to loss of earnings caused by premature mortality due to kidney cancer. More broadly, productivity loss would also include health-related productivity losses resulting from sickness absence, morbidity, and early retirement. As these were not captured in the current analysis, the results are considered conservative estimates of the actual productivity losses resulting from kidney cancer. Moreover, there is a wider impact on the caregivers of patients with cancer which is often overlooked [Citation36]. As there are no consensus guidelines for the categories and costs that should be included when estimating productivity loss, and as the proportion of productivity losses due to premature mortality will vary depending on disease characteristics (e.g. age of death; chronic versus acute disease; severity of comorbidities), it is difficult to determine the proportion of total productivity costs that are attributable to premature mortality, however an estimation of total productivity losses due to kidney cancer would be an interesting area for further study.
Despite this conservative approach to calculating productivity losses, the model estimated productivity losses exceeding €26.6 M in a single year in just two EU countries. To further highlight the conservative approach used in the base case setting of this model, a scenario analysis using unemployment rate and GDP as inputs was conducted. In the scenario analysis, lost productivity losses amounted to approximately €34.6 M compared to €26.6 M in the base case. The findings from this study may be extrapolated to other EU countries where the population demographics and exposure to risk factors follow a similar trend to the countries included in this analysis.
5. Conclusion
Based on the results from this analysis, lost productivity costs due to premature kidney cancer-related mortality in Greece and Portugal were estimated to exceed €26.5 M in 2019 alone. These results provide new information that may assist decision-makers in the allocation of resources to reduce the burden that kidney cancer imposes on the working-age population. Whilst major efforts are still required to reduce the economic burden of kidney cancer in these countries, insights into productivity losses resulting from kidney cancer can be used as a stepping stone to inform future policy work in this area.
Declaration of interest
G. Bencina, C. Baxter and S. Salomonsson are employees of MSD subsidiaries of Merck & Co., Inc., Rahway, NJ, USA and may own stocks and/or stock options in Merck & Co., Inc., Rahway, NJ, USA.
N. Chami, R. Hughes and G. Weston are employees of Adelphi Values (PROVE), paid consultants to MSD.
Reviewer disclosures
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Author contributions
G. Bencina designed the study. N. Chami; R. Hughes; G. Weston and G. Bencina developed the model. N. Chami; RH; G. Weston; G. Bencina and C. Baxter conducted the analysis. N. Chami; R. Hughes; G. Weston and G. Bencina; C. Baxter and S. Salomonsson were involved in the interpretation of results.
Data availability
All data used in this study are available in the public domain and is fully referenced throughout.
Supplemental Material
Download MS Word (251.7 KB)Supplementary material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/14737167.2023.2180356
Additional information
Funding
References
- Scelo G, Larose TL. Epidemiology and risk factors for kidney cancer. J Clin Oncol. 2018;36(36):Jco2018791905.
- Hsieh JJ, Purdue MP, Signoretti S, et al. Renal cell carcinoma. Nat Rev Dis Primers. 2017;3:17009.
- Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1204–1222.
- Li P, Znaor A, Holcatova I, et al. Regional geographic variations in kidney cancer incidence rates in European countries. Eur Urol. 2015;67(6):1134–1141.
- Hofmarcher T, Brådvik G, Svedman C, et al. Comparator report on cancer in Europe 2019–disease burden, costs and access to medicines. IHE Rep. 2019;7:204–209.
- Deppen SA, Aldrich MC, Hartge P, et al. Cancer screening: the journey from epidemiology to policy. Ann Epidemiol. 2012;22(6):439–445.
- OECD, Systems EOoH, Policies. Portugal: country health profile 2021. European Observatory on health systems and policies. 2021.
- European Commission. Europe’s beating cancer plan. Brussels: European Parliament and European Council; 2021 February.
- OECD/European observatory on health systems and policies. Portugal: Country Health Profile 2021, State of Health in the EU, OECD Publishing, Paris; 2021. DOI:10.1787/8f3b0171-en
- Shih Y-CT, Chien C-R, Xu Y, et al. Economic burden of renal cell carcinoma: part I--an updated review. Pharmacoeconomics. 2011;29(4):315–329.
- Bencina G, Chami N, Hughes R, et al. Lost productivity due to head and neck cancer mortality in Hungary, Poland, and Romania. J Cancer Policy. 2022 Oct 13;100366.10.1016/j.jcpo.2022.100366. Epub ahead of print. PMID: 36244644.
- Eurostat. Causes of death - deaths by country of residence and occurrence mortality data (2019). https://ec.europa.eu/eurostat/web/health/data/database. Cited Nov 2021.
- World Bank. Life expectancy at birth, male (years). https://data.worldbank.org/indicator/SP.DYN.LE00.MA.IN. Cited Nov 2021.
- World Bank. Life expectancy at birth, female (years). https://data.worldbank.org/indicator/SP.DYN.LE00.FE.IN. Cited Nov 2021.
- Eurostat. Mean annual earnings by sex, age and economic activity. 2018. https://ec.europa.eu/eurostat/databrowser/view/EARN_SES18_27__custom_1501377/default/table?lang=en. Cited Oct 2021.
- Eurostat. Gross domestic product at market prices. https://ec.europa.eu/eurostat/web/products-datasets/-/tec00001. Cited Oct 2021
- World Bank. Labor force participation rate, total (% of total population ages 15+) (national estimate) - European Union, Hungary, Poland, Romania Published 2021. https://data.worldbank.org/indicator/SL.TLF.CACT.NE.ZS. Cited Nov 2021.
- Eurostat. Unemployment rate. Published 2021. https://ec.europa.eu/eurostat/databrowser/view/tepsr_wc170/default/table?lang=en. Cited Oct 2021.
- Eurostat. Causes of death - deaths by country of residence and occurrence mortality estimates (2010, 2015 and 2019). https://ec.europa.eu/eurostat/web/health/data/database. Cited Oct 2021.
- The World Bank. Life expectancy at birth, female (years). https://data.worldbank.org/indicator/SP.DYN.LE00.FE.IN. Cited Oct 2021.
- The World Bank. Life expectancy at birth, male (years). https://data.worldbank.org/indicator/SP.DYN.LE00.MA.IN. Cited Oct 2021.
- Mean annual earnings by sex, age and economic activity. Eurostat. 2018. https://ec.europa.eu/eurostat/databrowser/view/EARN_SES18_27__custom_1501377/default/table?lang=en. Cited Nov 2021.
- The World Bank. Labor force participation rate, national estimate. 2019. https://data.worldbank.org/indicator/SL.TLF.CACT.NE.ZS. Cited Nov 2021.
- World Bank. Population, total - Greece. 2019. https://data.worldbank.org/indicator/SP.POP.TOTL?locations=GR. Cited Jul, 2022.
- World Bank. Population, total - Portugal. 2019. https://data.worldbank.org/indicator/SP.POP.TOTL?locations=PT. Cited Jul, 2022.
- Hanly P, Soerjomataram I, Sharp L. Measuring the societal burden of cancer: the cost of lost productivity due to premature cancer‐related mortality in E urope. Int J Cancer. 2015;136(4). E136-E145
- Hofmarcher T, Lindgren P, Wilking N, et al. The cost of cancer in Europe 2018. Eur J Cancer. 2020;129:41–49.
- Office of national statistics: cancer: are there more people diagnosed with cancer? https://blog.ons.gov.uk/2019/04/26/are-there-more-people-diagnosed-with-cancer/. Cited Oct, 2022.
- Huang J, Leung DK-W, Chan EO-T, et al. A global trend analysis of kidney cancer incidence and mortality and their associations with smoking, alcohol consumption, and metabolic syndrome. Eur Urol Focus. 2022;8(1):200–209.
- Sustainable Development UU. Goals as a framework for postgraduate future research following COVID-19 pandemic: a new norm for developing countries. Higher Edu Future. 2021;8(1):123–132.
- Peired AJ, Campi R, Angelotti ML, et al. Sex and gender differences in kidney cancer: clinical and experimental evidence. Cancers (Basel). 2021;13:18.
- Laskar RS, Muller DC, Li P, et al. Sex specific associations in genome wide association analysis of renal cell carcinoma. Eur J Hum Genet. 2019;27(10):1589–1598.
- Li C, Ekwueme DU, Rim SH, et al. Years of potential life lost and productivity losses from male urogenital cancer deaths–United States, 2004. Urology. 2010;76(3):528–535.
- Cancer.org. Key statistics about kidney cancer. https://www.cancer.org/cancer/kidney-cancer/about/key-statistics.html. Cited Aug 2022.
- Anderson WF, Jatoi I, Tse J, et al. Male breast cancer: a population-based comparison with female breast cancer. J Clin Oncol. 2010 Jan 10;28(2):232–239. Epub 2009 Dec 7. PMID: 19996029; PMCID: PMC2815713.
- Bradley CJ. Economic burden associated with cancer caregiving. Semin Oncol Nurs. 2019;35(4):333–336.