
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Objectives
To determine preferences for COVID-19 vaccinations in the young adult population in the United Kingdom (UK).
Method
A discrete choice experiment survey was conducted in UK young adults. Participants were asked to choose between two hypothetical vaccines the one they preferred the most. Vaccines were defined by five attributes (effectiveness, risk of side effects, duration of protection, number of doses, confidence in available evidence), identified following a systematic literature review and qualitative interviews with 13 young adults. A random parameters logit model, a latent class model, and subgroup analyses were used to identify preferences.
Results
One hundred and forty-nine respondents were included (70% women, mean age 23 years). All five attributes significantly influenced respondents’ vaccination decisions. Respondents valued higher effectiveness, lower risk of side effects, longer protection duration, and a smaller number of doses. Based on the range of levels of each attribute, vaccine effectiveness was the most important attribute (relative importance 34%), followed by risk of side effects (32%), and duration of vaccine protection (22%).
Conclusions
The five investigated vaccine attributes appear to play an important role in young adults’ decision-making process. Results of this study may help health authorities designing appropriate strategies in future vaccines campaigns in the younger UK population.
1. Introduction
COVID-19 resumes being a major global threat affecting the lives of people worldwide [Citation1]. Within the European region and also worldwide, the United Kingdom (UK) was one of the most affected countries at the beginning of 2021 [Citation2–4]. To stabilize the situation, the UK approved vaccines very early and implemented a vaccination program that prioritized the elderly and at-risk populations [Citation5], resulting in a steady decline in incidence and mortality [Citation6]. As of 28 July 2021, 71.1% of the adult population in the UK was fully vaccinated, demonstrating a high vaccine uptake. However, the decline in case numbers reached a plateau in mid-June and the trend reversed. In early July, an increase of more than 50% in case numbers and about 20% in hospitalization rates was recorded [Citation7]. Infection rates are highest among younger adults, who are often not fully vaccinated and therefore more susceptible to COVID-19 [Citation6].
The future success of the UK vaccination program will depend on uptake rates in the young population, as the majority of older people in the UK have been vaccinated [Citation8]. Vaccine hesitancy could significantly undermine efforts to control the COVID-19 crisis. It is therefore essential to develop and promote effective policies and promotional activities to ensure that vaccine uptake is sufficient to provide herd immunity [Citation9].
Vaccine hesitancy in the UK has been estimated at around 82% [Citation10] and has been shown to correlate with the relative newness of the disease and the associated knowledge gaps [Citation11,Citation12] as well as with younger age [Citation10]. The Office for National Statistics [Citation8] confirmed the highest vaccine hesitancy in the population aged 16–29 years, with 10% of this group, while overall public attitudes toward COVID-19 vaccines improved between May 30 and 4 July 2021 [Citation8]. Although an expected vaccine uptake rate of about 90% in this age group may seem high, it has been shown that intention and health behavior uptake can vary, suggesting that actual vaccine uptake may be lower [Citation13].
Preference research could be a valuable addition to the already existing body of research by identifying factors that may influence public acceptance of COVID-19 vaccines [Citation14]. Studies have shown that an individual’s attitude toward vaccine characteristics is very important for understanding vaccination behavior [Citation15,Citation16]. In addition to classifying the underlying motivations, estimating the relative importance of these aspects is essential for designing effective vaccination policies and tailoring interventions to the needs of specific groups [Citation17].
Preference research is now widely used to understand people’s decision-making processes. Discrete choice experiment (DCE), a widely used preference research method, provides participants with a set of attributes and allows them to assess the relative importance or the trade-offs between these different attributes [Citation18]. This is particularly relevant for vaccine research, as DCEs can also be used to predict the uptake of potential vaccines-based observed preferences [Citation19].
Previous DCEs examining COVID-19 vaccine preferences have found that vaccine efficacy, number of side effects, and duration of protection are among the most important attributes [Citation20–25]. However, no study has focused solely on the preferences of young adults, despite data showing that this age group has the highest reported vaccine hesitancy. Ensuring that herd immunity is achieved requires not only sufficient health system capacity [Citation9] but also policies that promote vaccine acceptability and uptake. Looking ahead to future vaccine strategies, the revealed preferences observed in this study may also be useful in formulating effective policies. Therefore, it seems crucial to understand vaccination preferences and decision-making in the young population as well. This study aims to elicit preferences for features of COVID-19 vaccines in the young UK population using a DCE method.
2. Methods
The research followed the ISPOR guidelines for conducting a DCE. First, attributes and levels were identified. Based on this, the questionnaire was developed. This was followed by a pilot phase, data collection, and statistical analysis [Citation26,Citation27].
2.1. Identification of attributes and levels
A sequential process was followed to identify and select COVID-19 vaccine-related attributes and levels of relevance to the UK public. The first step was to conduct a literature search using PubMed and Web of Science. The search was conducted in April 2021. To identify important factors influencing public attitudes and acceptance in the decision-making process regarding vaccination uptake, the search terms used were preference research, DCE, vaccine characteristics, and vaccination behavior. Using a combination of these key search terms, 20 publications published since 2010 were identified as potentially relevant to our research. In addition, available information on COVID-19 vaccines was considered, such as the weekly updated WHO publication on the candidate vaccines developed worldwide [Citation3].
Of the 20 potential references identified during our literature search, 8 appeared to be relevant to our research: 2 DCEs on pandemic vaccination [Citation17,Citation28] and 6 on COVID-19 vaccine preference [Citation20–25]. From these eight studies, a preliminary list of nine attributes was identified. The characteristics selected were those that were most frequently mentioned and were considered to be applicable to the UK setting, given that vaccines are already available (Appendix Table A1.1). This list was then reviewed in a second step during interviews with young adults living in the UK (n = 13) to prioritize and potentially identify other relevant attributes. The interviewees were recruited through the same channel as the final study population (see section ‘Sample and data collection’). They were also asked to select the attributes they considered important and to give reasons for their decision. Further, they were asked to rank the selected attributes in order to assess their importance, which in turn should facilitate the narrowing down of the list [Citation26,Citation29].
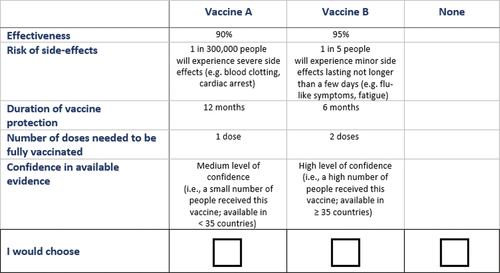
In the third step, the results of the previous steps were discussed with the research team (n = 5), consisting of researchers with experience in preference research. The list of attributes was reviewed, and the five attributes that seemed most relevant were decided and approved. There are no specific rules regarding the number of attributes that can be included in a DCE. However, in practice, most DCEs include a maximum of 10 attributes, with a mean of 5.74 reported in a recent systematic review [Citation30], to ensure that responders are able to consider all proposed attributes when making a selection. The final selection of attributes was made in a research meeting, and five important attributes emerged from this meeting. The choice of five attributes seemed sufficient to capture preferences while keeping decisions simple. The appropriate levels were identified from the literature and cross-checked with the research team. Accordingly, the following five attributes were included in the DCE: effectiveness, side effects, protection duration, number of doses, and confidence in the available evidence (see ). The attribute ‘side effects’ was divided into four different levels. Because both mild and severe side effects could be of interest, and to distinguish between severe and mild side effects, two levels were associated with the risk of mild side effects and two levels were associated with the risk of severe side effects. In each choice set, one of the four levels was selected for each hypothetical option. More details on the procedure can be found in Appendix S1 Supplemental Material.
Table 1. Attributes and levels included in the DCE.
2.2. Experimental design
Choice sets containing different combinations of the selected attributes and levels were constructed. To define the best combinations, a Bayesian efficient design was applied using the Ngene software that maximized the D-efficiency. A multinomial logit model was designed including main effect only. Thereby, sets were created that were the smallest size possible but still could determine all essential parameters and minimize the parameter-estimate variance [Citation31]. In total, a set of 36 choice sets were designed, which were grouped into three blocks. Each block consisted of 12 choice tasks randomly assigned to the participants. For each choice task, the participant had to decide between Vaccine A, Vaccine B, or No Vaccine, introducing an opt-out option to maximize the external validity [Citation32]. Moreover, a test–retest was included as a 13th choice task in which the participant was presented with the same choice task twice [Citation32]. shows an example of a choice task.
Figure 1. Example of choice task.
2.3. Questionnaire
The questionnaire consisted of three sections. The first section contained an introductory text about the research and a detailed explanation of the tasks, attributes, and levels, and an example of a completed choice task. In the second section, the choice sets were presented to the respondents. After completing the item sets, participants were asked about the perceived difficulty of the task using a five-point Likert scale ranging from ‘very difficult’ to “very easy. The final part of the questionnaire collected information on participants’ sociodemographic characteristics (i.e. age, gender, and education) and experience with COVID-19, such as vaccination status and a seven-point Likert scale question asking participants whether they were concerned about contracting COVID-19. The questionnaire was developed online using the software Qualtrics.
Prior to the actual study, a pilot study was conducted to check for interpretation problems, face validity, and the length of the questionnaire. A convenience sample of five young adults living in the UK was asked to complete the survey in Qualtrics. Only minor textual changes were made.
2.4. Sample and data collection
Data were collected through an online questionnaire using Qualtrics and completed by 150 UK residents between 25 and 27June 2021. The questionnaire was distributed through the Prolific online participant recruitment tool. Participants are recruited via the Prolific participant pool, which is representative of the UK population. To utilize Prolific, the researchers had to pay participants. Prolific shared the link to the questionnaire with a random group of participants. After completing the study, participants were redirected to the Prolific website and were paid a small incentive (£7.52 per hour, for 15 min participants got £1.88. The £7.52 was the minimum recommended by Percipio).
Previously proposed research standards [Citation33,Citation34] have suggested that a sample of more than 100 participants allows for modeling preference data. Therefore, a sample of 150 survey participants was deemed sufficient. In addition, as there is currently no standard for determining the minimum sample size for a DCE, Johnson and Orme (2010) have established a way to approximate the best fit: nta/c ≥ 500, where n = number of respondents, t = number of tasks, a = number of alternatives per task, and c = the largest number of levels for any one attribute. Based on this estimate, the minimum sample size for this DCE was established to be 55. The inclusion criteria applied were age (18–29 years) and UK residency. The age range was selected as this group reported the highest vaccine hesitancy in the UK [Citation35] and are the last group to be vaccinated [Citation8].
Ethical approval was obtained from the Brunel Research Ethics Committee (30721-MHR-Jun/2021- 32776-2) and the Maastricht University Research Ethics Committee (FHML/HPIM/2021.020). Informed consent was obtained from all participants by including an informed consent part within the questionnaire. Only if respondents agreed with the data collection, they were allowed to continue and participate in the study.
2.5. Statistical analysis
Data analysis was performed using Nlogit software 6.0. Respondent characteristics were analyzed by utilizing descriptive statistics.
The following utility model was estimated:
where Uijs|c represents the utility of respondent i belonging to class c (c = 1, 2, 3) for scenario j (j = 1,2,3) in choice sets (s = 1, … ,12), β is a parameter vector measuring the effect of the vaccine attributes described in . A dummy sentence was used for the opt out.
Table 2. Patient characteristics of the total sample (n = 149).
First, a random parameter logit model was run to estimate preferences and heterogeneity across the data set. A total of 1,000 Halton draws were used to evaluate the model. By yielding not only the mean coefficient but also the standard deviation across the sample, the model allowed to measure the distribution of preferences weights across the sample. Thereby variation within the responses is revealed, i.e. heterogeneity, meaning that a standard deviation, which significantly varies from zero, implies a significant preference heterogeneity for the attribute in the sample. All variables were expected to be normally distributed and incorporated as effects-coded categorical variables. Hence, mean attributes were standardized to zero, and added preference weights were proportional to the different levels of the attribute’s mean effect. The sign of a coefficient indicates whether a certain attribute level increases (positive) or decreases (negative) the willingness to get vaccinated. The importance that respondents attached to each attribute level was represented by the value of each coefficient. The variation in preference weights was deemed statistically significant if the 95% confidence interval around two levels did not overlap.
The conditional relative importance of attributes was calculated based on the preference estimates from the model using the range method. The relative importance of attributes calculated using this method always depends on the range of levels chosen per attribute and on the other attributes included in the experiment [Citation27]. The main analysis was performed on the full sample of the participants including those who failed the test–retest as it was seen as a learning process. However, a sensitivity analysis excluding the participants who failed the test–retest was also proposed to test the impact of this decision on the results.
Second, a latent class model was fitted to identify potential classes of respondents. In a latent class model, individuals are grouped into mutually exclusive groups based on differences in preferences or shared values within the sample [Citation36]. The model with the best fit was chosen utilizing Akaike’s information criterion. This model determined the number of classes needed to explain the preference heterogeneity. Subsequently, ‘preference to be vaccinated’ was assessed in the three classes and, thus, the probability of being in one of the classes was linked to this covariate. Participants were assigned to latent classes based on their posterior probability of membership and each respondent was assigned to a class when its probability to belonging was ≥ 80%. To analyze whether participants’ characteristics significantly differed between the latent classes, multiple pairwise tests were performed using software IBM SPSS 24TM. The Bonferroni approach was utilized as a multiple testing to adjust p-values. For the results, a significance level of < 0.05 was deemed as statistically significant as suggested by Hauber et al. [Citation27].
Finally, subgroup analyses were conducted to understand the preference heterogeneity found within the sample. Subgroups on age (≤23 years old vs. >23 years old), gender (female vs. male), worrying about contracting COVID-19 (yes vs. no), and contracting COVID-19 (yes vs. no) were considered based on the characteristics of the final sample. A joint model was estimated using interaction terms to assess whether preferences were significantly different between subgroups. Preferences were considered to vary across subgroups if the parameters estimated for the interaction terms were statistically (at a 5% level) different from zero. A normally distributed random component was added to each subgroup dummy.
A joint model was estimated using interaction terms to assess the significance of the differences between subgroups. A normally distributed random component was added for the dummy variable describing the age group.
3. Results
3.1. Respondent characteristics
The final sample consisted of 149 participants. A total of 150 questionnaires were completed; however, one participant did not meet the eligibility criteria (age) and was excluded from the final analysis. The majority of the participants were female, aged 18–23 years old, and lived in the south of the UK. Approximately 80% of the participants had either completed secondary school or an undergraduate degree. Sixty-two percent of the respondents were either fully or partially vaccinated, and 27% planned to be vaccinated. The rest (9%) did not want to be vaccinated, which is consistent with national statistics (i.e. 10% vaccine hesitancy) (Statistics, 2021b). Most respondents did not contract COVID-19 undiagnosed (69%) or were not tested positive (86%), and only 1 participant was hospitalized for COVID-19. Yet, more than half of the participants (65%) reported that at least one of their family members and/or friends contracted COVID-19. Of this group, 13% had died because of COVID-19. Finally, the perceived COVID-19 risk was moderate: only 27% disagreed or strongly disagreed with the statement that they were not worried about getting COVID-19, while 24% agreed or strongly agreed with the statement. Most of the votes (27%) were given for ‘somewhat disagree.’ The summary of the sample characteristics is shown in .
On average, the difficulty of the task was rated as moderately easy with a mean score of 2.72, based on the results of a five-point Likert scale where one was extremely easy and five extremely difficult. Twenty-three respondents failed the test–retest (i.e. 15.3%).
3.2. Respondents’ preferences
The random parameter logit model results are shown in and . All attributes were statistically significant at a p-value <0.01, indicating that all attributes were important for the respondents. Overall, the constant was positive and statistically significant (p < 0.01), indicating that respondents preferred to be vaccinated. No major difference was found between the full sample (n = 149) and the sample restricted to participants who did not fail the test–retest (n = 126) (Appendix S2 Table A2.1).
Figure 2. Patients’ preferences estimate.
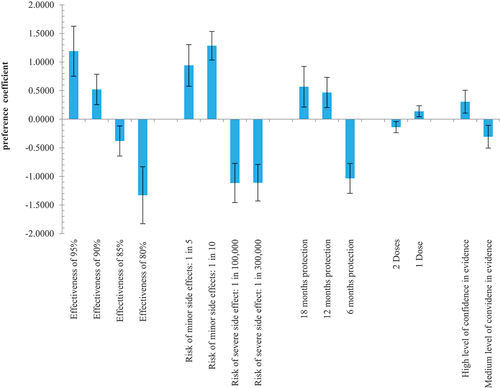
Table 3. Results from the random parameters logit model.
Based on the range of levels of each attribute, vaccine effectiveness was the most important attribute (relative importance 34%), followed by risk of side effects (relative importance 32%), and duration of vaccine protection (relative importance 22%). The least important attributes were confidence in available evidence (relative importance 8%) and number of doses (relative importance 4%). Respondents had a greater aversion to severe and rare side effects than to minor and more common side effects, but the difference between rare side effects did not appear to be of great importance, as indicated by the similar and non-significantly different coefficients.
All the relationships observed were in the expected direction: the coefficient increased as the level of each attribute improved. In general, respondents preferred a vaccine with higher effectiveness, a longer duration of protection, fewer number of doses, and for which they had a high level of confidence in the available evidence. A lower risk of minor side effects compared to the severe and rare side effects was preferred.
Significant standard deviations were observed for all coefficients, i.e. significant heterogeneity for all attributes, revealing variation in preferences among respondents for all attributes.
3.3. Latent class model
The results of the latent class model are presented in . All participants had a ≥ 80% probability of belonging to a class and were therefore included in the latent class analysis. Three preference latent classes were identified and included 81 (Class 1), 51 (Class 2), and 17 (Class 3) participants, respectively. Within each class, heterogeneity in the preferences was identified which may be due to differences in vaccination preferences explained by the constants (positive = in favor of vaccination; negative = against vaccination). A positive constant was reported for classes 1 and 2 while a negative constant was reported for Class 3.
Table 4. Results from the latent class model.
In all classes, the coefficients and their significance of attribute levels differed from those estimated by the random parameter model for the full sample, meaning that preferences also varied. This also led to changes in the ranking of importance of attribute levels. Only the risk of side effects and almost all associated attribute levels remained statistically significant at a p-value of < 0.01 across all classes.
Respondents in classes 1 and 3 preferred the highest vaccine effectiveness (95%), whereas respondents in class 2 appeared to be indifferent if the vaccine had a higher effectiveness than 80%. Particularly, the respondents of class 3 seemed to consider high vaccine effectiveness to be extremely important. The risk of side effects was considered important in all three classes. In case of risk of severe but rare side effects, the coefficient was negative for respondents in all three classes suggesting a preference for lower risk of severe side effects. However, only in classes 2 and 3 the response was statistically significant in both attribute levels (1 in 100,000 and 1 in 300,000). For minor side effects, the response was statistically significant in the case of ‘1 in 10 people’ indicating that all respondent (classes 1, 2, 3) preferred a vaccine with lower risk of minor side effects. In terms of duration of vaccine protection and number of doses seemed to be of no relevance for classes 2 and 3. Only in Class 1 statistically significant responses were measured. Respondents in class 1 preferred a longer duration of vaccine protection and a lower number of doses. Finally, a higher level of confidence in available evidence was preferred in all groups but the strongest preference for a high level of confidence was measured in class 1 (p-value <0.01).
No difference in terms of characteristics of participants in the different latent classes was observed at one exception (Table A2.2 Appendix S2 Supplementary Materials). In fact, a significantly higher proportion of young adults do not plan to be vaccinated (58.8%) in latent class 3 compared to young adults belonging in the other classes (p < 0.001).
3.4. Subgroup analyses
The subgroup analysis ‘worry about contracting COVID-19’ showed a significant difference between the two groups. Difference in the relative importance of attributes were also observed. Respondents who were not concerned about contracting COVID-19 were less willing to be vaccinated, rated vaccine effectiveness as more important, and were less concerned about the severity of side effects than respondents who were concerned about contracting COVID-19. Moreover, number of doses and the confidence in available evidence were not significant and thus not predictor when deciding to get vaccinated. The respondents appeared to be indifferent about the difference. Participants worried about contracting COVID-19 were most concerned about side effects followed by vaccine effectiveness. In addition, these participants preferred a lower number of doses and higher level of confidence.
A significant difference in the constant was also found in the subgroup analysis ‘age’. The constant for the younger age group (18–23) was observed to be higher than the one for the older age group (24–29) indicating that the respondents aged between 18 and 23 years were more in favor of getting vaccinated. The only significant difference at a 5% level was observed for risk of side effects. Besides that, age did not appear to have a significant impact on respondents’ preference. The subgroup analysis on gender found that the female participants were more likely to get vaccinated (constant coefficient of 1.442) compared to the male participants (0.812). The analysis showed that male participants valued lower side effects more than female participants. Furthermore, a lower number of doses was preferred by male participants compared to female participants. No other significant differences were observed for other attributes/levels. Finally, the subgroup analysis comparing participants who contracted COVID-19 versus those who did not revealed no significant difference. More detailed results of the analyses are shown in Table A2.3, A2.4, A2.5, and A2.6 Appendix S2 Supplementary Materials.
4. Discussion
This DCE identified the importance of COVID-19 vaccines attributes for young adults. Vaccine effectiveness, the severeness and incidence of side effects, the duration of the vaccine protection, the number of doses needed, and the level of confidence in the available evidence appeared to influence people’s decisions. Given the range of levels included, the most important outcomes to respondents were a high level of effectiveness and low risk of side effects, whilst high confidence in evidence and a small number of doses were the least important. Although these results are in the expected direction, this is the first time preferences for characteristics of COVID-19 vaccines are provided for young adults using a DCE robust methodology. Nevertheless, because relative importance is based on the range between the highest and lowest coefficient for attribute levels, the results should be interpreted with caution.
The results of this study are largely consistent with previous DCEs of COVID-19 vaccines. Most of the previous studies also reported that the vaccine effectiveness was one of the most important influencing factors, although some studies considered additional characteristics [Citation20–25]. Yet, although often still perceived as a decisive factor the importance of the risk of side effects differed between the studies [Citation20–22,Citation25]. For example, Dong et al. [Citation25] observed that the protective duration of the vaccine was more important for the Chinese population than the risk of few adverse events. Additionally, the results of other studies showed that the location of administration, the number of acquaintances vaccinated, and potential proof of vaccination could also impact the peoples’ choice of vaccine [Citation20,Citation21,Citation23].
Furthermore, the latent class model revealed some differences in the importance of attributes among the participants. Contrarily to respondents of classes 1 and 2, the constant of class 3 was negative, revealing that the probability of accepting the vaccination is lower for respondents of this class. As expected, a lower proportion of respondents belonging in class 3 reported to be fully vaccinated or partially vaccinated at the time of the survey. For classes 1 and 2, the attitude toward vaccination appeared to be similarly positive; however, differences in preferences were observable. Respondents in class 1 perceived all attributes to be important, whereas in class 2 respondents seemed to be indifferent to all attributes besides the risk of side effects. The findings are in contrast to the studies of Borriello et al. [Citation20] and Leng et al. [Citation22] which revealed that side effects were observed to be less important and vaccine effectiveness appeared to have a greater influence in the latent classes.
Finally, the subgroup analyses found that the preference of vaccines, while positive in all cases, did significantly differ between the groups in the subgroup analysis ‘age’ (18–23 vs. 24–29) as well as in the subgroup analysis ‘worry’ (not worried vs. worried). In addition, respondents who were concerned about contracting COVID-19 were also more concerned about severe but rare side effects.
The identified preferences of young adults in the UK for COVID-19 vaccines may be considered when developing strategies and interventions to increase vaccine coverage. As the young adult population appears to be less fearful of contracting COVID-19 which in turn also affects potential uptake rates [Citation10], targeted information campaigns on the benefits of the vaccines and the need to be vaccinated need to be developed. Proactively communicating the effectiveness, the risk of side effects, and the length of protective duration of vaccines could be critical factors to boost vaccine uptake. Moreover, ensuring that the information and evidence available is perceived of high quality appears to positively influence the willingness of people to get vaccinated. Particularly, the mistrust and concerns about future adverse effects of vaccines should be taken seriously and accounted for in these communications. Another point to consider in the planning process is the complexity of vaccine hesitancy. Not only the found heterogeneity of preferences in the study sample suggests that personal attitudes toward vaccines differ but also the results of the latent class model and subgroup analyses. For example, according to the latent class model, the preference of people not willing to be vaccinated is mostly influenced by effectiveness and side effects whereas for the two groups willing to get vaccinated either side effects or all attributes appeared to have the greatest impact on the choice of the vaccine. Notwithstanding the potential implications of the findings, one has to consider that because of the rapidly changing COVID-19 pandemic the results might not be as useful in informing communication strategies. Yet, at the time of data collection (June 2021), the vaccine hesitancy in the younger population was evident and was proposed to have a potential impact on the success of the vaccination strategies. This might also be the case in future vaccine strategies related to COVID-19 vaccine and others. Therefore, findings of the attitudes toward vaccine in this population was thought to be of interest. Further research could investigate young adults’ attitudes toward and preferences in vaccines not only for COVID-19 but in general since vaccine hesitancy appears to be especially high in these groups.
5. Study limitations
Several limitations of the study must be addressed. First, although the selection and definition of attributes and levels followed a comprehensive methodological process, it is still possible that some relevant attributes in people’s preferences were omitted. Also, the attribute ‘confidence in available evidence’ was a broad attribute that could potentially include a very large number of levels. To make a clear difference between efficacy and side effects, this attribute was rather focused on the number of participants who already received the vaccine and the number of countries in which the vaccine is available. Nevertheless, it is obvious that this attribute would have been able to provide additional information if it would also have covered other aspects of confidence. Second, the range method was used to assess the conditional relative importance of attributes, with the inherent limitation that the number and range between levels of an attribute has an impact on the measured importance of it. Although this method is a common way to present DCE data as suggested by ISPOR guidelines [Citation27], the interpretation of the relative importance should be done with caution. Third, the generalizability of the results cannot be disregarded. Indeed, although the sample was representing all ages in the selected age group, gender, and regions in the UK, an overrepresentation of females and the younger age group (19–23) is observed and needs to be considered when assessing the generalizability of the study. Also, the sample was small and only people having knowledge about and being registered at Prolific were considered. Fourth, indifference between rare and common severe side effects, and between probabilities of minor side effects could be due to the fact that all side effects levels combing severity and frequency were included into one attribute. Finally, we did not estimate interaction effects but focused on main effects, both when planning the experiment and when analyzing the data. Nevertheless, it would be interesting in the future to assess potential interaction effects by example between side effects and vaccine effectiveness.
6. Conclusion
Overall, the study revealed that young adults have strong preferences for vaccine attributes. All five attributes appear to play an important role in the decision-making process of young adults. Based on the results of the study, it can be concluded that a high level of effectiveness and duration of protection as well as a reduced risk of severe and mild side effects have a positive impact on individual vaccine preference. It appears to be of critical importance to promote vaccine uptake by clearly communicating these factors. Policies should be tailored to address the concerns and preferences of younger people in order to achieve better uptake rates in the future, which is essential to ensure the stabilization of COVID-19 infection rates. The observed heterogeneity of preferences among the younger population should encourage health authorities to develop policies that take into account the different expectations regarding COVID-19 vaccines. Hence, in the case of people who are not worried about COVID-19 and not in favor of getting vaccinated, policies should target strategies promoting the effectiveness and reduced risk of side effects of vaccines. Finally, for future vaccine strategies the findings may help to develop effective strategies for the younger population.
Article highlights
The discrete choice model identified the preferences in vaccine characteristics as well as trade-offs made by young adults in the UK regarding COVID-19 vaccines.
On average, young adults are in favor of getting vaccinated and value a higher effectiveness, lower risk of side effects, longer protection duration, and a smaller number of doses in vaccines.
Preference heterogeneity among the younger population was determined.
Young adults who are against being vaccinated still have a preference for vaccines with higher effectiveness and a lower risk of side effects.
Health authorities should develop policies considering the variation in expectations regarding COVID-19 vaccines.
Declaration of interest
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Reviewer disclosures
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Availability of materials
Available under request to the corresponding author.
Supplemental Material
Download MS Word (78.4 KB)Supplementary material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/14737167.2023.2223983
Additional information
Funding
References
- WHO. (2021). Weekly epidemiological update 13 Jul 2021. Retrieved 13.Jul.2021 from https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19—13-july-202
- BBC. (2021). Covid-19 in the UK: how many coronavirus cases are there in your area? Retrieved 7.Jan.2021 from https://www.bbc.com/news/uk-51768274
- WHO. (2021). Draft landscape of COVID-19 candidate vaccines. Retrieved 7.Jan.2021 from https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines
- WHO. (2021). Weekly epidemiological update 12 Jan 2021. Retrieved 23.Jan.2021 from https://www.who.int/publications/m/item/weekly-epidemiological-update—12-january-202
- Baraniuk C. Covid-19: how the UK vaccine rollout delivered success, so far. BMJ. Retrieved 18.2021.
- Statistics OFN (2021). Coronavirus (COVID-19) latest insights: infections Retrieved 21.Jul.2021 from https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/articles/coronaviruscovid19latestinsights/infections#infections-by-age
- Gov.UK. (2021). Coronavirus (COVID-19) cases in the UK. Retrieved 28.Jul.2021 from https://coronavirus.data.gov.uk/
- Statistics OFN (2021). Coronavirus (COVID-19) latest insights: vaccines. Retrieved 28.Jul.2021 from https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/articles/coronaviruscovid19latestinsights/vaccines
- Lazarus JV, Ratzan SC, Palayew A, et al. A global survey of potential acceptance of a COVID-19 vaccine. Nat Med. 2020;27(2):225–228. DOI:10.1038/s41591-020-1124-9
- Robertson E, Reeve KS, Niedzwiedz CL, et al. Predictors of COVID-19 vaccine hesitancy in the UK household longitudinal study. Brain Behav Immun. 2021;94:41–50. DOI:10.1016/j.bbi.2021.03.008
- Palamenghi L, Barello S, Boccia S, et al. Mistrust in biomedical research and vaccine hesitancy: the forefront challenge in the battle against COVID-19 in Italy. Eur J Epidemiol. 2020;35(8):785–788. DOI:10.1007/s10654-020-00675-8
- Chou WYS, Budenz A. Considering emotion in COVID-19 vaccine communication: addressing vaccine hesitancy and fostering vaccine confidence. Health Commun. 2020;35(14):1718–1722. DOI:10.1080/10410236.2020.1838096.
- Sniehotta FF, Scholz U, Schwarzer R. Bridging the intention–behaviour gap: planning, self-efficacy, and action control in the adoption and maintenance of physical exercise. Psychology & Health. 2005;20(2):143–160. DOI:10.1080/08870440512331317670.
- van Overbeeke E, Whichello C, Janssens R, et al. Factors and situations influencing the value of patient preference studies along the medical product lifecycle: a literature review. Drug Discov Today. 2019;24(1):57–68. DOI:10.1016/j.drudis.2018.09.015
- González-Lorenzo M, Piatti A, Coppola L, et al. Conceptual frameworks and key dimensions to support coverage decisions for vaccines. Vaccine. 2015;33(9):1206–1217. DOI:10.1016/j.vaccine.2014.12.020
- Guo N, Wang J, Nicholas S, et al. Behavioral differences in the preference for hepatitis B virus vaccination: a discrete choice experiment. Vaccines (Basel). 2020;8(3):527. DOI:10.3390/vaccines8030527
- Determann D, Korfage IJ, Lambooij MS, et al. Acceptance of vaccinations in pandemic outbreaks: a discrete choice experiment. PLoS ONE. 2014;9(7):e102505. DOI:10.1371/journal.pone.0102505
- Clark MD, Determann D, Petrou S, et al. Discrete choice experiments in health economics: a review of the literature. Pharmacoeconomics. 2014;32(9):883–902. DOI:10.1007/s40273-014-0170-x
- de Bekker-Grob EW, Donkers B, Bliemer MCJ, et al. Can healthcare choice be predicted using stated preference data? Soc Sci Med. 2020;246:112736. DOI:10.1016/j.socscimed.2019.112736
- Borriello A, Master D, Pellegrini A, et al. Preferences for a COVID-19 vaccine in Australia. Vaccine. 2021;39(3):473–479. DOI:10.1016/j.vaccine.2020.12.032
- Craig BM. United States COVID-19 vaccination preferences (CVP): 2020 hindsight. Patient-Patient-Centered Outcomes Res. 2021;14(3):309–318. DOI:10.1007/s40271-021-00508-0.
- Leng A, Maitland E, Wang S, et al. Individual preferences for COVID-19 vaccination in China. Vaccine. 2021;39(2):247–254. DOI:10.1016/j.vaccine.2020.12.009
- McPhedran R, Toombs B. Efficacy or delivery? An online discrete choice experiment to explore preferences for COVID-19 vaccines in the UK. Econ Lett. 2021;200:109747.
- Schwarzinger M, Watson V, Arwidson P, et al. COVID-19 vaccine hesitancy in a representative working-age population in France: a survey experiment based on vaccine characteristics. Lancet Public Health. 2021;6(4):e210–21. DOI:10.1016/S2468-2667(21)00012-8
- Dong D, Xu RH, Yi WE, et al. Public preference for COVID-19 vaccines in China: a discrete choice experiment. Health Expectations. 2020;23(6):1543–1578. DOI:10.1111/hex.13140
- Bridges JFP, Hauber AB, Marshall D, et al. Conjoint analysis applications in health—a checklist: a report of the ISPOR good research practices for conjoint analysis task force. Value Health. 2021;14(4):403–413. DOI:10.1016/j.jval.2010.11.013.
- Hauber AB, González JM, Groothuis-Oudshoorn CGM, et al. Statistical methods for the analysis of discrete choice experiments: a report of the ISPOR conjoint analysis good research practices task force. Value Health. 2016;19(4):300–315. DOI:10.1016/j.jval.2016.04.004.
- Determann D, Korfage IJ, Fagerlin A, et al. Public preferences for vaccination programmes during pandemics caused by pathogens transmitted through respiratory droplets–a discrete choice experiment in four European countries, 2013. Eurosurveillance. 2016;21(22):30247. DOI:10.2807/1560-7917.ES.2016.21.22.30247
- Coast J, Al‐Janabi H, Sutton EJ, et al. Using qualitative methods for attribute development for discrete choice experiments: issues and recommendations. Health Econ. 2012;21(6):730–741. DOI:10.1002/hec.1739
- Trapero-Bertran M, Rodríguez-Martín B, López-Bastida J, et al. What attributes should be included in a discrete choice experiment related to health technologies? A systematic literature review. PLoS ONE. 2019;14(7):e0219905. DOI:10.1371/journal.pone.0219905
- Johnson FR, Lancsar E, Marshall D, et al. Constructing experimental designs for discrete-choice experiments: report of the ISPOR conjoint analysis experimental design good research practices task force. Value Health. 2013;16(1):3–13. DOI:10.1016/j.jval.2012.08.2223
- Ryan M, Skåtun D. Modelling non‐demanders in choice experiments. Health Econ. 2004;13(4):397–402. DOI:10.1002/hec.821.
- Orme B. Getting started with conjoint analysis: strategies for product design and pricing research. Madison, WI: Research Publishers LLC; 2010.
- Pearmain D, Kroes EP. Stated preference techniques: a guide to practice. 1990.
- Statistics OFN (2021). Coronavirus and vaccine hesitancy, Great Britain: 26 May to 20 June 2021. Retrieved 21.Jul.2021 from https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthandwellbeing/bulletins/coronavirusandvaccinehesitancygreatbritain/26mayto20june2021.
- Zhou M, Thayer WM, Bridges JF. Using latent class analysis to model preference heterogeneity in health: a systematic review. Pharmacoeconomics. 2018;36(2):175–187. DOI:10.1007/s40273-017-0575-4.