
ABSTRACT
Teachers’ beliefs and experiences were explored when using videoconferencing at mainstream schools to provide distance learning to students with a chronic illness (SCIs) in a hybrid virtual classroom (HVC). Seventy-seven primary and secondary teachers participated in this study, involving a semi-structured interview and a survey. Teachers found the HVC useful to achieve continuity of learning, to support the social well-being of SCIs and to facilitate school re-entry. A multiple regression analysis showed that perceived usefulness and the actions teachers undertook to foster collaboration and communication between SCIs and their school were related to perceived engagement of SCIs. Primary school teachers enhanced significantly more activities to support interaction between SCIs and their classmates than secondary school teachers.
1. Introduction
As scientific progress and development in healthcare has drastically lowered child mortality over the last 50 years and increased the number of children with a chronic illness (CI) (Mokkink, Citation2004), a growing number of these children now attend mainstream schools where they face school-related problems (Te Meerman & Demoulin, Citation2005), and they also miss more days at school than their healthy peers (Lum et al., Citation2019). School absence adversely affects continuity of education and learning (Martinez & Erickan, Citation2009), it can lead to academic underachievement (Lum et al., Citation2019) and it can have a big impact on the social well-being of students with CI (SCI) (Hopkins et al., Citation2014). It is essential therefore to connect absent SCIs with their classes. The use of videoconferencing (VC) is seen as a promising intervention to connect SCIs with their peers and teachers at their mainstream school (Ellis et al., Citation2013; Zhu & Van Winkel, Citation2015). SCIs at home and students in class follow lessons simultaneously, and all participants have the opportunity to interact with each other. This learning environment is called a hybrid virtual classroom (HVC) (Butz & Stupnisky, Citation2016). During the Covid-19 pandemic this type of technology-enhanced education has also been used for regular students to attend lessons for part of the time in class and the other part remotely. The limited research that has been done on this has shown that students can benefit from using a HVC (Raes, Vanneste, et al., Citation2020). However, it has also revealed several pedagogical and technical challenges. New knowledge and teaching methods are required (Ramsey et al., Citation2016) and more research conducted from a teacher’s perspective is needed (Raes, Vanneste, et al., Citation2020), especially when SCIs are involved (Jackson, Citation2013; Maor & Mitchem, Citation2015; Zhu & Van Winkel, Citation2015). This study aimed to gain insight into teachers’ perceptions of teaching SCIs in a HVC.
2. Effects of chronic illness on engagement with learning
Chronic illness is defined in this study as an illness that is not or is not yet curable and persists for more than three months, based on the ICD-10 classification of the World Health Organization. This is a list of codes for illnesses and health-related problems, which is widely used internationally and is commonly used in Dutch research (Mokkink et al., Citation2008). Recent research based on Dutch national health insurance figures for all Dutch children and young people aged 0–25 years revealed that 1 in 4 had been diagnosed with a CI (Hal et al., Citation2019). Furthermore, this report shows that SCIs intend to participate in regular school, sport and work activities just like their healthy peers but have difficulty achieving full participation and continuity in education.
Participation in education can be examined with the aid of the school engagement concept of Fredricks et al. (Citation2004), in which engagement is seen as a three-component construct that is essential for learning: 1) behavioural engagement referring to student participation in learning activities and attendance in class; 2) social and emotional engagement referring to the students’ feeling of belonging to school and the school environment; and 3) cognitive engagement referring to the investments students put into learning. SCIs face difficulties on all three components of school engagement and show poorer school outcomes compared to their healthy peers (Lum et al., Citation2019). First, as a result of the illness and treatment, SCIs have lower attendance rates than their peers (Lum et al., Citation2019). Second, these students face significantly more social and emotional problems in school (Pinquart & Teubert, Citation2012) such as lower feelings of social well-being (Te Meerman & Demoulin, Citation2005), lower feelings of autonomy, competence and relatedness in school (Kirkpatrick, Citation2020), higher risk of developing depression, anxiety disorders or deficits in social competence (Pinquart & Shen, Citation2011; Pinquart & Teubert, Citation2012) and lower self-esteem (Martinez & Erickan, Citation2009). In addition, their dependence on others, their disconnection from their peers and teachers and their limited participation in school activities all negatively affect the social and emotional engagement of SCIs (Maor & Mitchem, Citation2015). Finally, their frequent and long absences from school (Kaffenberger, Citation2006) result in them missing crucial teaching, leading to low academic outcomes (Martinez & Erickan, Citation2009; Wilkie & Jones, Citation2008), which in turn can lead to lower levels of cognitive engagement and even to school dropout (De Ridder et al., Citation2013; Van Heesch et al., Citation2012). Maintaining the social and cognitive connections between SCIs at home or in hospital and their school is crucial in order to establish a feeling of relatedness with peers and teachers, to create a feeling of ‘normalcy’ (A’Bear, Citation2014; D’Agostino et al., Citation2011; Wilkie & Jones, Citation2008; Zhu & Van Winkel, Citation2015) and to enable them to learn just like their healthy peers (Hopkins et al., Citation2014). Connecting these students with their class and addressing their educational needs even when they are absent for a long period of time supports their engagement with learning (Boonen & Petry, Citation2012)
3. Hybrid virtual classrooms
Technology is seen as a promising and powerful tool to connect SCIs with the school they would normally attend (Capurso & Dennis, Citation2017; Jackson, Citation2013; Maor & Mitchem, Citation2015; Thompson et al., Citation2015). The first project to connect SCIs in hospital with their own classes via VC was called Pebbles and was launched in 2001 (Fels & Weiss, Citation2001). Several projects using this concept followed, amongst them the Dutch project ‘KlasseContact’ (Ziezon, Citation2015) and the Belgian project Bednet (Bednet, Citation2020). These last two projects created HVCs in which a SCI at home or in hospital could participate in lessons with the class at school online using a laptop connected with a computer in class with a 360° camera on top (Zhu & Van Winkel, Citation2015).
Except for teaching SCIs, HVCs were hardly ever used in mainstream education settings in the pre-Covid-19 period. In higher education, HVCs were used sporadically to allow groups of students to attend college or follow work groups at a distance at the same time as groups in class (Raes, Vanneste, et al., Citation2020). The recent systematic review of Raes, Detienne, et al. (Citation2020) showed that teaching in such an environment involves both pedagogical and technical challenges.
3.1 Technical and pedagogical challenges of HVCs
Technology itself is a crucial factor: a bad connection or even failing to connect can be frustrating for all users (Weitze, Citation2015). Teachers’ competence in using the technology influences the quality of teaching: where to position the camera, how to use the microphone and how to organise a conversation between the remote students and the class (Zydney et al., Citation2019) are questions teachers need to ask themselves before teaching a HVC.
In addition to technological challenges, teachers face several pedagogical challenges. They need to concentrate on both the students in class and the students engaged in distance learning and adjust their teaching to the specific needs of both groups (Ørngreen et al., Citation2015). They need to organise their teaching activities in such a way that students in class and remote students engage in similar and comparable learning activities (Butz & Stupnisky, Citation2016). This is a challenge as the learning experiences of students in class are not the same as those of remote students (Huang et al., Citation2017). Remote students tend to feel isolated as they are physically separated from class which can result in a more passive behaviour on their part (Weitze, Citation2015). Activating the remote students and stimulating them to interact with the teacher and the students in class is seen as a key strategy to reinforce learning engagement (Weitze, Citation2015). This requires specific knowledge and skills on the part of teachers as they are seen as facilitators of the interaction. This specific teachers’ role is also seen in the Community of Inquiry (CoI) model of Garrison et al. (Citation2000), which explains the process of creating meaningful learning using VC in an online setting. In this model teachers are seen as facilitators whose job is to ensure social and cognitive presence of distant students by stimulating interactivity and creating opportunities for communication and collaboration between students as well as between teacher and students. Rehn et al. (Citation2018) also examined the teacher’s role when using VC for remote students in mainstream school settings and identified four sub-roles: 1. pedagogical – engaging students, monitoring progress and facilitating communication; 2. managerial – planning lessons and organising learning material; 3. social – facilitating interaction, creating a class community; and 4. technical – knowing how to use the system and to deal with technical problems. They concluded that although teachers often have difficulties fulfiling these roles as they lack the knowledge and strategies to adapt their pedagogies, they still experience the benefits of VC when teaching distanced students and are more than willing to use it.
3.2 HVC for students with chronic illness
The scarce research that has evaluated the use of a HVC with SCIs in mainstream schools has shown that SCIs are positive about attending lessons via VC and that they feel engaged in the daily classroom activities (Benigno et al., Citation2014; Bresser, Citation2010; Ellis et al., Citation2013; Wilkie, Citation2010; Zhu & Van Winkel, Citation2015). Cognitive engagement as well as the opportunity for social and emotional engagement and improved social relationships with peers are reported by SCIs as positive outcomes (Maor & Mitchem, Citation2015; Zhu & Van Winkel, Citation2015). How teachers of mainstream primary and secondary schools experience the use of a HVC with SCIs is still not clear. The few studies conducted in this area show the need to identify what support, knowledge and skills teachers need to teach SCIs in a HVC and how teachers can influence the engagement of these students (Benigno et al., Citation2014; Maor & Mitchem, Citation2015; Rice & Dykman, Citation2018).
Teachers have a key role in successful use of a HVC: their competence in establishing interaction between remote students and students in class and the teacher, and their competence in using the technology are crucial to achieving cognitive, social and emotional engagement of the remote students. Furthermore, the successful implementation and integration of new technologies depends, in particular, on the teachers’ attitudes and beliefs including their confidence in the effectiveness of the technology and its contribution to educational goals (Hew & Brush, Citation2007).
4. This study
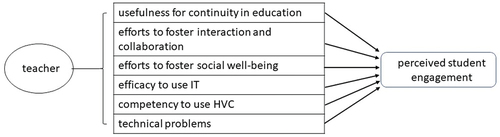
HVCs have been used to teach SCIs in the Netherlands since 2006, but no research has been conducted into the role of teachers in enhancing the engagement of SCIs. This study aimed to fill that gap and focused on the teachers’ perceptions and experiences using a HVC with a remote SCI. Based on the literature discussed above, a list of categories that influence students’ cognitive, social and behavioural engagement was drawn up (see ) to answer the following research questions:
Figure 1. Factors that influence SCIs' cognitive, social and behavioural engagement.
1. How do teachers evaluate a HVC as an intervention to ensure that a SCI experiences continuity in education?
2. What specific activities do teachers report that they use to foster interaction and collaboration and the wellbeing of the SCI in class when using a HVC with SCIs?
3. How do teachers evaluate the use of HVC technology?
4. What factors influence the behavioural engagement of SCIs?
5. Research method
5.1 Research setting
Mainstream schools in the Netherlands organising education for their SCIs at home or in hospital can apply for assistance from a network of school liaison workers who are experts in the field of education for SCIs. Their guiding principle is that SCIs should stay connected to school and return to school when possible. They are guided by this when they inform schools about the consequences of a specific illness for continuity in education, when they assist with drawing up individual learning plans and when they recommend the use of ‘KlasseContact’ to create a HVC. SCIs who are absent from school for more than six weeks owing to their chronic illness are eligible for a KlasseContact device. By 2014, when the number of installations per year was extended to 450, a new system was launched known as ‘Klasgenoot’ (‘classmate’ in English). New features of Klasgenoot were the possibility of using the 4G network to establish a better and more secure Internet connection and a remote-controlled attention light on top of the classroom computer, allowing the student at home to change colours to attract the teacher’s attention without disturbing the class. The connection between the computers is based on an embedded Microsoft LINQ solution. No other connections can be made, and it is impossible to record video or audio in order to ensure the privacy of the SCIs, teachers and students in class. In the HVC created with KlasseContact, one remote student follows the lessons simultaneously with the students in class.
5.2 Procedure
To answer the research questions, 15 teachers were interviewed, using a semi-structured interview. In addition, an online survey, based on the findings of the semi-structured interview, was completed by 62 teachers. All participants used VC devices of KlasseContact.
5.3 Sample
For the interview, all school liaison workers (N = 101) were asked to approach schools who were using or recently had used KlasseContact to participate in the study. Sixty-three teachers were contacted by the school liaison workers. Teachers of palliative students were excluded. Twenty-nine teachers responded positively, but 14 teachers did not participate owing to technical problems (N = 4) or heavy workload (N = 10), which resulted in the participation of eight primary school teachers and seven secondary school teachers. The age of the SCIs varied between 9 and 17 years old. The majority of the students had a haematological/oncological disease (N = 7), the other students were facing recovery after trauma (N = 2), had diseases of the digestive system (N = 2), the nervous system (N = 2) or the respiratory system (N = 1) or had a metabolic disease (N = 1).
For the survey, 250 teachers who had recently worked with KlasseContact or were using KlasseContact at the time of the survey were contacted by email. Thirty-one primary school teachers and 33 secondary school teachers completed the online survey. One respondent from secondary education, who was a member of the school management team and did not teach, was excluded from the analyses. The questionnaire of another secondary school teacher, whose student had recently died, was incomplete and therefore was excluded too. The age of the teachers varied between 23 and 60 years. The majority of the primary school teachers were female (93.5%), and 50% of the secondary school teachers were female. All teachers worked with VC devices of KlasseContact. The SCIs of the teachers who completed the questionnaire were 5–18 years old, and all had a disease classified as a somatic chronic illness according to the ICD-10 standard.
5.4 Interviews
In the semi-structured interviews teachers were asked questions about their goals in using HVC, how useful they found HVC, the special skills they needed and the efforts they made to teach SCIs and any technical problems they experienced. Example questions were: What is your main reason for using HVC? Did you succeed in achieving the educational goals for your SCI? Did you treat your SCI like any other student? Did using HVC change your role as a teacher? Did you use various teaching methods? Can you give some examples? Finally, they were asked some questions about technical issues.
5.5 Survey questionnaire
The online survey contained 59 items, of which 57 were scored on a 5-point Likert scale. The participating teachers could rate these statements according to their findings: 1 = not at all, 2 = not really, 3 = somewhat, 4 = quite a lot and 5 = very much. These items were clustered into seven scales of our research model: 1. Perceived usefulness of HVC for continuity in education; 2. Teacher efforts to foster interaction and collaboration; 3. Teacher efforts to foster well-being of SCI; 4. Teacher efficacy in use of IT(information technology); 5. Competency in use of HVC; 6. Technical problems; and 7. Perceived student behavioural engagement (see ). The reliability of the scales was sufficient (Cronbach’s alpha ranged from .68 to .91). For two scales (Efforts to foster well-being: 3 items; Competence teaching HVC: 2 items), we used the Spearman–Brown prediction formula to predict the reliability of these scales after changing the length of the scales to six items (see for example, Eisinga et al., Citation2013).
Table 1. Descriptive statistics of online survey for primary and secondary education.
The survey also included two open questions. In the first open question teachers were asked to describe the specific skills or actions they used to connect the student at home with the class while teaching. In the second open question teachers were asked to write down anything they wanted to share about working with HVC. In the online survey, teachers also completed some demographic data, their teaching experience and type of school (primary or secondary).
5.6 Analyses
The semi-structured interviews were audio-taped and transcribed verbatim. The answers to the open question in the survey that asked which skills and activities teachers used to connect SCIs with their class were coded in 11 themes defined using a grounded theory method (Glaser, Citation1992; see ) by two independent raters. Twelve differences between raters were found and discussed and agreed upon. The inter-rater reliability was sufficient: Cohen’s kappa .73.
Table 2. Reported teachers’ activities to connect SCIs and number of activities per teacher.
Fifty-nine teachers responded to this question.
To answer the first three research questions, descriptive statistics were used for the quantitative questionnaire data. The qualitative information from the interviews were used to illustrate and elaborate the quantitative findings. In order to answer the fourth research question, a multiple regression analysis was performed with the six scales from the questionnaire as predictors and perceived student engagement as dependent variable. In order to check differences between teachers in primary and secondary education, a multivariate analysis of variance was performed with school sector as factor and the seven questionnaire scales as dependent variables. Pearson’s correlation coefficients showed some moderate to strong associations between the questionnaire scales (see ).
Table 3. Bivariate correlations between independent variables and outcome variable.
6. Results
presents descriptive statistics of the variables of the online survey. In general, teachers found HVC useful for learning when teaching SCIs. The respondents showed moderate scores on efforts to foster interaction and collaboration and quite low scores on efforts to foster well-being. The results of the open question on the survey revealed that 65% of the responding teachers reported not using more than two different activities to connect SCIs with the class.
To explore possible differences between primary and secondary school teachers, a multivariate analysis of variance (MANOVA) was conducted. We see from the MANOVA that primary and secondary teachers differed significantly in their scores on the seven questionnaire scales (Wilks’ λ (6,55) = 3,380; p = 0.007; η2 = .269). The test of between-subjects effects indicated that both groups differed significantly on efforts to foster interaction and collaboration (F(1,61) = 5,691; p ≤ 0.001; η2 = .198). Teachers in primary education demonstrated higher scores in efforts to foster interaction than teachers in secondary education (see ).
6.1 Evaluation of HVC as an intervention to ensure continuity in education
Thirteen interviewed teachers reported that connecting SCIs with their peers was their most important goal in using HVC. One teacher reported: ‘The main reason was to keep in touch. Actually, my student had never left school, she knew what was happening in the classroom and, the other way around, she could tell us what was happening in hospital.’ Another teacher mentioned that the social aspect, connecting the SCI, and the learning aspect, teaching the SCI, were equally important. Yet another teacher reported that the opportunity to teach remotely was the main reason for using HVC. She explained that her student was a very shy girl who did not like to participate in class discussions. For this reason, social contact was not a goal as such, although it helped her to stay connected with her class and this made it easier for her to return to school. Four other teachers also reported that the use of HVC helped the SCI to return to their school. Two SCIs returned to their normal school sooner than expected, as they liked to be in school again. Two teachers of students with cancer mentioned that HVC helped them to be part of the class and feel connected to their classmates. It also helped these students to return to school emboldened, even with a feeding tube in their nose. Their appearance was not an issue as the teachers and schoolmates were used to the way they looked. One teacher described this return to school as follows:
It certainly helped my student to be part of her class. When you see this for the first time, there were mothers crying at the window when she came back to school, but we just started class as normal, for her peers it was just like normal.
Although two teachers did not succeed in teaching via HVC, all teachers reported that they thought HVC would be a useful intervention for teaching SCIs. One teacher had some difficulties in communicating with the parents and sometimes the student was too sick to attend the lessons. The other teacher mentioned that the technical problems experienced with the system resulted in arranging private tuition at home.
Twelve interviewed teachers stated they were kept well informed by parents and the school liaison workers when they started to use HVC. The other three teachers reported that they were informed, but the real diagnosis of the disease and its impact only became clear during the period they were using HVC. Nine teachers reported that working with a SCI had affected them emotionally; six of them said that talking to colleagues had helped them to cope with it.
6.2 Activities to foster interaction, collaboration and social well-being of SCIs
All but one of the interviewed teachers reported that they treated their SCIs as regular students. They also said that they changed their teaching style or initiated other activities in order to give their SCI a feeling of belonging to the class. One teacher described this as follows: ‘When we worked in groups, we put him [KlasseContact device] on a chair next to the table, at eye level, so he [SCI] was really present.’ All teachers agreed that involvement of peers was very important. Seven teachers stated that their students needed some time to adjust to the situation. One of them said: ‘In the beginning, everybody wanted to see themselves on the screen and wave, but this soon stopped.’ Another teacher explained:
Lisa is not a regular student; she has cancer for the second time. I had to explain this to her classmates: Lisa longs to be with you in class, but she cannot if you turn around and act like monkeys, it is not normal, that is not what she wants.
Another teacher used WhatsApp to motivate the SCI to join the lesson: ‘It sometimes happened she was not present, then I could say “Guys, let’s give Clare a WhatsApp-bombardment” and we all sent messages to her.’ Another example of involving classmates was the use of a buddy system: peers were instructed to collect the KlasseContact computer from storage, to turn it on and, if necessary, to transport the computer to other classrooms, but also to inform the SCI about the time schedule and classroom-related instructions.
All but one of the teachers worked with fixed schedules for HVC. In most cases, these were developed in cooperation with the SCIs and their parents. In many cases, these schedules were hard for the SCIs to follow, owing to illness and hospital visits. One teacher turned on the HVC set every morning, and her SCI could tune in whenever she liked.
The teachers used HVC in different settings. All teachers who were interviewed used HVC in front of the whole class. Five teachers also worked with small groups of students, including the SCI in one of the groups. One of the teachers, who used this small-group setting quite often, reported:
This worked very well, although it takes some planning skills. My student needed the same worksheets as her peers. Sometimes a friend went to her home during lunchbreak to take her the learning materials, so they could work together in the afternoon lessons.
Four other teachers also used HVC in a ‘one-to-one’ setting. For example, one teacher had a short conversation with the SCI prior to the lessons so that the student could ask some questions.
Seven teachers mentioned in the interviews that posing questions to the SCI was important to motivate the student to participate in the lesson. Yet four teachers reported that it was sometimes difficult to determine whether their SCI really participated in class. They missed their physical presence in the classroom. For example. one teacher reported: ‘In the class, you walk to his desk, look into his notes, chat with him in private, give a compliment or assist with a problem. With HVC this is difficult, the whole class is joining this private conversation.’ Another teacher mentioned: ‘I really found it difficult to assess whether the student at home really understood my instruction.’ Another teacher stated: ‘As a teacher you do not watch her the whole time, on the outside she is present, but if she really is? … I thought maybe because of her illness that she cannot concentrate easily.’ None of the three cited teachers had a solution to their problem. A fourth teacher did: she asked the parents at home to check whether the student was participating. Two teachers reported they had the feeling the SCI sometimes ended the lessons on purpose by switching off the computer. They did not check whether this was really the case or why this student switched off the computer before the lesson ended.
All teachers mentioned in the interviews that parents were important partners in supporting the use of HVC, and 11 teachers were in contact with the parents on a regular basis. These parents informed the teachers about medical issues and the use of HVC or discussed the time schedule. One teacher had difficulties with communication as neither parent spoke Dutch or English, and one teacher had problems communicating with parents when the parents disagreed about the school’s decision that the student was not able to keep up with his peers and needed an individual learning plan.
Seven teachers reported that they had adapted their classroom teaching to the HVC situation. One teacher explained why he changed the rules on using mobile phones:
They [peers] were allowed to use their mobile phones during HVC lessons. In regular lesson students can whisper to each other or exchange notes, that disturbs your lesson as well. But with texting messages fewer students are disturbed and Peter [the SCI] could have personal contacts during the lesson.
Six teachers allowed classmates to chat with the SCI during coffee and lunch breaks and one teacher organised chat sessions after school hours. Another teacher with a student with cancer reported: ‘Just before Christmas, we could light candles together, such activities in a HVC, yes that helps.’ Another teacher mentioned: ‘I realised that I can help my SCI with sending cards, little presents and using HVC to keep her in contact with her classmates.’
6.4 Experiences with HVC technology
In the interviews, all but two teachers reported technical problems, i.e., sound problems, camera failures and weak internet connections. Eight teachers found these technical problems frustrating. The problems were often unexpected and time-consuming, and, according to these teachers, they interfered with the lessons and had a rather big impact on both the teacher and the SCI. Four teachers reported that technical problems affected the continuation of the SCI’s education to such an extent that the student could not keep up with their peers.
All teachers indicated that they felt competent to use HVC in their lessons. Most of them asked students in class to help them with the technical aspects. Five teachers mentioned that they could ask the school IT specialist to assist. All teachers were informed about the possibility of calling a helpdesk for technical support. Only four teachers were able solve these problems by themselves; the others needed the helpdesk or IT professionals in school.
Seven teachers had received written instructions and training by school liaison workers on the day of installation of the system. The other teachers were not present on the first day and were given written instructions, or, in some cases, colleagues explained how to use HVC. Although three teachers felt slightly uneasy at the start, all the teachers reported they felt at ease when teaching with HVC. One teacher had a special agreement with the parents to be sure that what happened in the classroom was to be kept private.
6.5 Factors related to SCIs’ engagement with class
A multiple regression analysis was performed to determine whether the engagement of the students could be explained by the six scales from the questionnaire: 1. Perceived usefulness of HVC for continuity in education; 2. Teacher efforts to foster interaction and collaboration; 3. Teacher efforts to foster well-being of SCI; 4. Teacher efficacy in use of IT: 5. Competency in use of HVC; and 6. Technical problems. The results show that 54% of the variance in student engagement was explained by these six factors (R2 = .543; F = 10.903; p < .001). The ‘Perceived usefulness of HVC for learning’ and the ‘Efforts teachers make to foster interaction’ were both significantly related to the perceived engagement of the SCI (see ).
Table 4. Summary of multiple regression analysis for variables predicting student engagement (N = 62).
7. Discussion
The aim of this study was to explore teachers’ experience of the use of HVC when teaching SCIs.
7.1 HVC as a useful classroom setting
Teachers reported that they found HVC to be a useful environment for teaching SCIs in their regular classes. Continuity of education for the SCI was the most important reason they gave for using HVC. Teachers also found it useful to re-establish the social connection between the SCI and the school, with HVC contributing to the reintegration of the SCI when they returned to school. This finding corroborates results of previous research by Zhu and Van Winkel (Citation2015), who reported that SCIs felt confident and less stressed when they returned to school after using HVC.
7.2 Activities to foster interaction and collaboration
The majority of the participating teachers treated their SCIs as ‘regular’ students. This might be considered a contradiction in terms, since using HVC to teach SCIs is not a ‘regular’ classroom situation, nor is it a ‘regular’ HVC setting in which several remote students and a group of students in class are present (Butz & Stupnisky, Citation2016). The HVC setting used for connecting SCIs is different and can be described as a ‘many-to-one’ situation, as both the teacher and a large group of students are connected to one SCI. This might explain why teachers reported that some SCIs felt overwhelmed and were reluctant to participate in social activities. Our research also revealed that teachers hardly adapted their classroom teaching at all to facilitate interaction or collaboration between the class and the SCI. We know from the CoI model of Garrison et al. (Citation2000) that interaction is essential to accomplish social presence of the remote students; without interaction, teaching with VC easily descends into just giving lectures. To facilitate effective interaction with VC, it is essential to design lessons with structured interactive components (King, Citation2002) or to use scripts where specific roles and activities are allocated to individuals and group members during the learning process (Dillenbourg & Hong, Citation2008). Some teachers adopted solutions to enable the SCI to really join in during the lesson, using blended technologies and actively structuring the interaction. This demands special teaching skills and insight into how lessons can be structured to ensure interaction and which skills are required to connect all students, both remote students and those in class. Some individual teachers in our study found solutions, but there is a lack of collective knowledge and awareness of the specific skills that teaching with HVC demands (Rehn et al., Citation2018).
Another finding of this research was that communication between school and the student at home and cooperation with parents were essential in order to identify the needs of the SCI. Some teachers mentioned that their physical condition and low motivation influenced the number of hours the SCI attended school. The impact of the exhausting treatment of some diseases, such as cancer, is known to affect a student’s physical capability, but it can also influence their motivation for school (Bjork et al., Citation2009). In addition to matching the use of HVC to the physical health of the SCI, it is also clearly important to monitor whether the pedagogy meets the student’s needs. This is in line with the findings of Lum et al. (Citation2019) that communication between school, parents and school liaison workers regarding the physical health and the social and emotional needs of SCIs is essential to provide effective support to these students. Teachers in primary education have more contact hours with their students and their parents and therefore might have more opportunities to identify the needs of sick students and arrange cooperative learning activities. From that perspective it is perhaps understandable that in this research primary school teachers seemed to scaffold the interaction and collaboration more than secondary school teachers. However, the teachers in our research demonstrated very few activities designed to foster the SCI’s social well-being, although they recognised the importance of HVC for the social connection between the SCI and their peers, and they communicated with parents. This can be explained by the knowledge gap on how to foster social well-being with HVC (Maor & Mitchem, Citation2016), how to identify the needs of a SCI and how to support these students effectively (Lum et al., Citation2019).
7.3 Teachers’ experiences with HVC technology
Teachers in this study felt quite competent to teach with HVC, although they only had a moderate level of IT skills. They reported that assistance from IT specialists in school, the support of students in class and an ‘easy to reach’ helpdesk with remote assistance helped them to solve technical problems. Technical support is a critical factor for success in using HVC (Raes et al, Citation2020); this might explain why, although almost every teacher in this study experienced major technical problems, they did not lose their motivation to use HVC.
7.4 Factors related to SCIs’ engagement with class
The findings of this research show that the perceived behavioural engagement of the SCI was affected by the perceived usefulness of HVC and by the activities teachers used to foster interaction and collaboration between the SCI and the class. The importance of perceived usefulness is one of the main components in the Technology Acceptance Model (TAM; Davis, Citation1985): perceived usefulness alongside perceived ease of use predict whether the technology is actually used. According to the TAM model, perceived usefulness drives the intention to use technology, which finally leads to usage behaviour. For teachers in this research, the most important goal in using HVC was continuity of education and some activities to foster interaction and collaboration to achieve this goal were reported. However, to enhance engagement of the SCIs, it is essential that they are motivated to connect to school, to really feel related to their classmates, teachers and the classroom, to feel recognised as a real student (Yates, Citation2010) and to receive meaningful and individualised feedback (Marteney & Bernadowski, Citation2016). This implies that teachers should include activities in their lessons which contribute to the needs of SCIs and strengthen their feeling of relatedness as well as their feeling of academic competency. Teachers in this research, however, did not report many activities that fostered the social well-being of their SCIs, nor did they reinforce their feeling of belonging to the school.
7.5 Limitations and future research directions
This study provides insights into teachers’ perceptions of the use of HVC in mainstream primary and secondary schools and especially for teaching SCIs. Some limitations have to be mentioned. Firstly, owing to technical problems with HVC systems and internet access, some users could not participate in the study as they were unable to use the HVC software or unable to use it fully. Secondly, the sample of teachers was small and the teachers participated on a voluntary basis. Furthermore, for privacy reasons the researchers did not know what diseases the SCIs involved in the study had. It is not clear, therefore, whether the sample was representative of the whole target group of teachers teaching SCIs. Thirdly, this research found some examples of good teaching practices to foster collaboration and interaction between the SCIs and their classes, but it also makes clear that many teachers did not adapt their teaching to connect their SCIs with the class. Further research is needed to explore in depth the educational goals, beliefs, experiences and needs of all participants: SCIs, peers, parents and teachers. It is essential to develop tools that can specify the needs of the remote SCIs and their teachers to be able to determine which teaching methods and situation-specific pedagogy best fit those needs.
7.6 Concluding remark
HVC is a promising approach to connect distant SCIs with the mainstream schools they usually attend. This research is one of the first to contribute to insights from the teachers’ perspective. It makes clear that teachers play a crucial role when teaching in a hybrid virtual environment and that more research is needed in order to specify what pedagogical skills and knowledge are necessary to provide ‘tailor-made’ support to students with a chronic illness in a HVC. The Covid-19 pandemic has shown that HVC can also be used for teaching other remote students without a chronic illness. The findings of this study can be applied to this setting, too.
Acknowledgments
This work was supported by the Revalidatiefonds/HandicapNL.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes on contributors
Silvia Klunder
Silvia Klunder holds a Master’s degree in Educational Sciences (Leiden University) and is a PhD candidate at Leiden University Graduate School of Teaching (ICLON). She is a school liaison worker and hospital teacher at Leiden University Medical Centre (LUMC).
Nadira Saab
Nadira Saab is Professor of e-Didactics at ICLON and Strategic Advisor Research at Kennisnet. Her research is focused on collaborative learning, motivation, diversity and inclusion in education and technology-enhanced education.
Wilfried Admiraal
Wilfried Admiraal is Professor of Educational Sciences at Leiden University, the Netherlands. From 2022 he will be Professor of Technology in Education at Oslo Metropolitan University, Norway. In his research, he combines the domains of education, social psychology and technology.
References
- . (2020). http://www.bedent.be/bednet-english
- A’Bear, D. (2014). Supporting the learning of children with chronic illness. Canadian Journal of Action Research, 15(1), 22–39. https://doi.org/10.1007/978-981-13-8161-4_8
- Benigno, V., Caruso, G., Fante, C., Ravicchio, F., & Trentin, G. (2014). The TRIS Project and the socio-educational inclusion of homebound students. International Journal of Technology and Inclusive Education, 5(1), 682–689. https://doi.org/10.20533/ijtie.2047.0533.2015.0088
- Bjork, M., Wiebe, T., & Hallstrom, I. (2009). An everyday struggle – Swedish families’ lived experiences during a child’s cancer treatment. Journal of Pediatric Nursing, 24(5), 423–432. https://doi.org/10.1016/j.pedn.2008.01.082
- Boonen, H., & Petry, K. (2012). How do children with a chronic or long-term illness perceive their school re-entry after a period of homebound instruction? Child: Care, Health and Development, 38(4), 490–496. https://doi.org/10.1111/j.1365-2214.2011.01279.x
- Bresser, S. D. (2010). Ziek, maar toch op school [Master’s thesis]. University of Utrecht. http://igitur-archive.library.uu.nl/student-theses/2010-1028-200238/Masterthesis%20Bresser%2c%20SPM%20de-3198502.pdf
- Butz, N. T., & Stupnisky, R. H. (2016). A mixed methods study of graduate students’ self-determined motivation in synchronous hybrid learning environments. The Internet and Higher Education, 28, 85–95. https://doi.org/10.1016/j.iheduc.2015.10.003
- Capurso, M., & Dennis, J. (2017). Key educational factors in the education of students with a medical condition. Support for Learning, 32(2), 158–179. https://doi.org/10.1111/1467-9604.12156
- D’Agostino, N., Penney, A., & Zebrack, B. (2011). Providing developmentally appropriate psychosocial care to adolescent and young adult cancer survivors. Cancer: A Journal of the American Cancer Society, 117(S10), 2329–2334. https://doi.org/10.1002/cncr.26043
- Davis, F. (1985). Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Quarterly, 13(3), 319–340. https://doi.org/10.2307/249008
- De Ridder, K. A., Pape, K., Johnsen, R., Holmen, T. L., Westin, S., Bjørngaard, J. H., & Dowd, J. B. (2013). Adolescent health and high school dropout: A prospective cohort study of 9000 Norwegian adolescents (the Young-HUNT). Plos ONE, 8(9), 1–7. https://doi.org/10.1371/journal.pone.0074954
- Dillenbourg, P., & Hong, F. (2008). The mechanics of CSCL macro scripts. International Journal of Computer-Supported Collaborative Learning, 3(1), 5–23. https://doi.org/10.1007/s11412-007-9033-1
- Eisinga, R., Te Grotenhuis, M., & Pelzer, B. (2013). The reliability of a two-item scale: Pearson, Cronbach or Spearman-Brown? International Journal of Public Health, 58(4), 673–642. https://doi.org/10.1007/s00038-012-0416-3
- Ellis, S. J., Drew, D., Wakefield, C. E., Saikal, S. L., Punch, D., & Cohn, R. J. (2013). Results of a nurse-led intervention: Connecting pediatric cancer patients from the hospital to the school using videoconferencing technologies. Journal of Pediatric Oncology Nursing, 30(6), 333–341. https://doi.org/10.1177/1043454213514633
- Fels, D., & Weiss, P. L. (2001). Video-mediated communication in the classroom to support sick children: A case study. International Journal of Industrial Ergonomics, 28(5), 251–263. https://doi.org/10.1016/S0169-8141(01)00020-8
- Fredricks, J. A., Blumenfeld, P. C., & Paris, A. (2004). School engagement: Potential of the concept: State of the evidence. Review of Educational Research, 74(1), 59–119. https://doi.org/10.3102/00346543074001059
- Garrison, D. R., Anderson, T., & Archer, W. (2000). Critical inquiry in a text-based environment: Computer conferencing in higher education model. The Internet and Higher Education, 2(2–3), 87–105. https://doi.org/10.1016/S1096-7516(00)00016-6
- Glaser, B. (1992). Basics of grounded theory analysis. Sociology Press.
- Hal, L., Van, Tierolf, B., Rooijen, M., V., Hoff, M., & van, D. (2019). Een actueel perspectief op kinderen en jongeren met een chronische aandoening in Nederland: Omvang, samenstelling en participatie. Jonker Verwey Instituut. https://www.verwey-jonker.nl/publicatie/een-actueel-perspectief-op-kinderen-en-jongeren-met-een-chronische-aandoening-in-nederland-omvang-samenstelling-en-participatie/
- Hew, K. F., & Brush, T. (2007). Integrating technology into K-12 teaching and learning: Current knowledge gaps and recommendations for future research. Education Technology Research and Development, 55(3), 223–252. https://doi.org/10.1007/s11423-006-9022-5
- Hopkins, L., Green, J., Henry, J., Edwards, B., & Wong, S. (2014). Staying engaged: The role of teachers and schools in keeping young people with health conditions engaged in education. Australian Educational Researcher, 41(1), 25–41. https://doi.org/10.1007/s13384-013-0096-x
- Huang, Y., Shu, F., Zhao, C., & Huang, J. (2017). Investigating and analyzing teaching effect of blended synchronous classroom. Sixth International Conference of Educational Innovation through Technology (EITT) (pp. 134–135). Osaka, Japan. https://doi.org/10.1109/EITT.2017.40
- Jackson, M. (2013). The special educational needs of adolescents living with chronic illness: A literature review. International Journal of Inclusive Education, 17(6), 543–554. https://doi.org/10.1080/13603116.2012.676085
- Kaffenberger, C. J. (2006). School reentry for students with a chronic illness: A role for professional school counselors. Professional School Counseling, 9(3), 223–230. https://doi.org/10.1177/2156759X0500900312
- King, A. (2002). Structuring peer interaction to promote high-level cognitive processing. Theory into Practice, 41(1), 33–40. https://doi.org/10.1207/s15430421tip4101_6
- Kirkpatrick, K. M. (2020). Adolescents with chronic medical conditions and high school completion: The importance of perceived school belonging. Continuity in Education, 1(1), 50–63. https://doi.org/10.5334/cie.5
- Lum, A., Wakefield, C. E., Donnan, B., Burns, M. A., Fardell, J. E., Jaffe, A., Kasparian, N. A., Kennedy, S. E., Leach, S. T., Lemberg, D. A., & Marshall, G. M. (2019). School students with chronic illness have unmet academic, social, and emotional school needs. School Psychology, 34(6), 627–636. https://doi.org/10.1037/spq0000311
- Maor, D., & Mitchem, K. (2015). Can technologies make a difference for hospitalized youth: Findings from research. Journal of Computer Assisted Learning, 31(6), 690–705. https://doi.org/10.1111/jcal.12112
- Marteney, T., & Bernadowski, C. (2016). Teachers’ perceptions of the benefits of online instruction for students with special educational needs. British Journal of Special Education, 43(2), 178–194. https://doi.org/10.1111/1467-8578.12129
- Martinez, Y., & Erickan, K. (2009). Chronic illness in Canadian children: What is the effect ofillness on academic achievement, and anciety and emotional disorders? Child: Care, Health and Development, 35(3), 391–401. https://doi.org/10.1111/j.1365-2214.2008.00916.x
- Mokkink, L. B., van der Lee, J. H., Grootenhuis, M. A., Offringa, M., & Heymans, H. S. (2008). Defining chronic diseases and health conditions in childhood (0–18 years of age): National consensus in the Netherlands. European Journal of Pediatrics, 167(12), 1441–1447. https://doi.org/10.1007/s00431-008-0697-y
- Mokkink, L. (2004). Omvang en gevolgen van chronische aandoeningen bij kinderen. Emma Kinderziekenhuis AMC. https://www.academia.edu/23403617/Omvang_en_gevolgen_van_chronische_aandoeningen_bij_kinderen
- Ørngreen, R., Levinsen, K. E. T., Jelsbak, V. A., Møller, K. L., and Bendsen, T. (2015). Simultaneous Class-based and Live Video Streamed Teaching: Experiences and derived principles from the Bachelor Programme in Biomedical Laboratory Analysis. In A. Jefferies, and M. Cubric (Eds.), Proceedings of 14th European Conference on e-Learning ECEL-2015Academic Conferences and Publishing International. https://www.academia.edu/19808141/Simultaneous_Class-based_and_Live_Video_Streamed_Teaching_Experiences_and_derived_principles_from_the_Bachelor_Programme_in_Biomedical_Laboratory_Analysis
- Pinquart, M., & Shen, Y. (2011). Depressive symptoms in children and adolescents with chronic physical illness: An updated meta-analysis. Journal of Pediatric Psychology, 36(4), 375–384. https://doi.org/10.1093/jpepsy/jsq104
- Pinquart, M., & Teubert, D. (2012). Academic, physical, and social functioning of children and adolescents with chronic physical illness: A meta-analysis. Journal of Pediatric Psychology, 37(4), 376–389. https://doi.org/10.1093/jpepsy/jsr106
- Raes, A., Detienne, L., Windey, I., & Depaepe, F. (2020). A systematic literature review on synchronous hybrid learning: Gaps identified. Learning Environments Research, 23(3), 269–290. https://doi.org/10.1007/s10984-019-09303-z
- Raes, A., Vanneste, P., Pieters, M., Windey, I., Noortgate, W. V. D., & Depaepe, F. (2020). Learning and instruction in the hybrid virtual classroom: An investigation of students’ engagement and the effect of quizzes. Computers & Education, 143, 103682. https://doi.org/10.1016/j.compedu.2019.103682
- Ramsey, D., Evans, J., & Levy, M. (2016). Preserving the seminar experience. Journal of Political Science Education, 12(3), 256–267. https://doi.org/10.1080/15512169.2015.1077713
- Rehn, N., Maor, D., & McConney, A. (2018). The specific skills required of teachers who deliver K–12 distance education courses by synchronous videoconference: Implications for training and professional development. Technology, Pedagogy and Education, 27(4), 1–13. https://doi.org/10.1080/1475939X.2018.1483265
- Rice, M., & Dykman, B. (2018). The emerging research base for online learning and students with disabilities. In R. Ferdig & K. Kennedy (Eds.), Handbook of research on K-12 online and blended learning (pp. 189–206). ETC Press. https://doi.org/10.1184/R1/6686813
- Te Meerman, W., & Demoulin, L. (2005). Vraag en aanbod van ICT voor kinderen met een beperking, als gevolg van een chronische aandoening of handicap. Capgemini Nederland B.V.
- Thompson, A. L., Christiansen, H. L., Elam, M., Hoag, J., Irwin, M. K., Pao, M., Voll, M., Noll, R. B., & Kelly, K. P. (2015). Academic continuity and school reentry support as a standard of care in pediatric oncology. Pediatric Blood & Cancer, 62(S5), S805–S817. https://doi.org/10.1002/pbc.25760
- Van Heesch, M., Bosma, H., Traag, T., & Otten, F. (2012). Hospital admissions and school dropout: A retrospective cohort study of the ‘selection hypothesis’. European Journal of Public Health, 22(4), 550–555. https://doi.org/10.1093/eurpub/ckr129
- Weitze, C. L. (2015). Pedagogical innovation in teacher teams: An organisational learning design model for continuous competence development. In I. A. Jefferies, and M. Cubric (Eds.), Proceedings of 14th European Conference on e-Learning ECEL-2015. Hatfield, United Kingdom (pp. 629-638). Academic Conferences and Publishing International. Proceedings of the European Conference on e-Learning.
- Wilkie, K., & Jones, A. (2008). Link and learn: Students connecting to their schools and studies using ICT despite chronic illness. The University of Melbourne. http://www.aare.edu.au/08pap/wil08169.pdf
- Wilkie, K. (2010). Academic continuity through online collaborations: Mathematics teachers support the learning of pupils with chronic illness during school absence. Interactive Learning Environments, 19(5), 519–535. https://doi.org/10.1080/10494820903545542
- Yates, L. (2010). Keeping connected: Identity, social connection and education for young people living with chronic illness. Melbourne Graduate School of Education, the University of Melbourne. doi: 9780980823707
- Zhu, C., & Van Winkel, L. (2015). Using ICT-tool as a solution for the educational and social needs of long-term sick adolescents. Technology, Pedagogy and Education, 24(2), 231–245. https://doi.org/10.1080/1475939X.2013.856339
- Ziezon. (2015). KlasseContact. http://www.ziezon.nl/ziezon-caring-about-taking-care-of-pupils-with-chronic-or-long-term-illnesses/klassecontact-off-sick-but-still-in-the-classroom/
- Zydney, J. M., McKimm, P., Lindberg, R., & Schmidt, M. (2019). Here or there instruction: Lessons learned in implementing innovative approaches to blended synchronous learning. TechTrends, 63(2), 123–132. https://doi.org/10.1007/s11528-018-0344-z