
ABSTRACT
Impact loading has been associated with running-related injuries, and gait retraining has been suggested as a means of reducing impact loading and lowering the risk of injury. However, gait retraining can lead to increased perceived awkwardness and effort. The influence of specifically trained and self-selected running gait modifications on acute impact loading, perceived awkwardness and effort is currently unclear. Sixteen habitual rearfoot/midfoot runners performed forefoot strike pattern, increased step rate, anterior trunk lean and self-selected running gait modifications on an instrumented treadmill based on real-time biofeedback. Impact loading, perceived awkwardness and effort scores were compared among the four gait retraining conditions. Self-selected gait modification reduced vertical average loading rate (VALR) by 25.3%, vertical instantaneous loading rate (VILR) by 27.0%, vertical impact peak (VIP) by 16.8% as compared with baseline. Forefoot strike pattern reduced VALR, VILR and peak tibial acceleration. Increased step rate reduced VALR. Anterior trunk lean did not reduce any impact loading. Self-selected gait modification was perceived as less awkward and require less effort than the specifically trained gait modification (p < 0.05). These findings suggest that self-selected gait modification could be a more natural and less effortful strategy than specifically trained gait modification to reduce acute impact loading, while the clinical significance remains unknown.
Introduction
Running is a popular sport worldwide; however, the incidence of running-related injuries is high, affecting up to 79% of runners (Van Gent et al., Citation2007). Impact loading is believed to be a key mechanical risk factor in running-related injuries (Van Der Worp et al., Citation2016), and gait retraining to reduce impact loading in novice runners has been shown to reduce injury occurrence by 62% 1 year after training (Chan et al., Citation2018). In addition, previous studies have shown increased impact loading in injured runners with plantar fasciitis (Pohl et al., Citation2009), chronic exertional compartment syndrome (Diebal et al., Citation2012) and stress fractures (Milner et al., Citation2006; Van Der Worp et al., Citation2016). Thus, running strategies that reduce impact loading could potentially manage running-related injuries.
Specifically trained gait modifications, in which runners adopt specific, prescribed modifications, have thus been proposed to reduce impact loading in runners. Adopting a forefoot strike pattern has been shown to reduce impact loading (Cheung & Davis, Citation2011) and tibiofemoral joint loading (Bowersock et al., Citation2017). Increased step rate has been shown to reduce impact loading (Hafer et al., Citation2015) and to lower mechanical energy absorbed by the hip and knee joints (Heiderscheit et al., Citation2011). Running softer can lead to decreased impact loading (Crowell et al., Citation2010) and anterior trunk lean has been suggested as a gait modification to soften footfalls (Arendse et al., Citation2004). Although the direct effect on impact loading is less clear, anterior trunk lean has been shown to reduce knee joint energetics (Arendse et al., Citation2004) and patellofemoral joint stress (Teng & Powers, Citation2014). In addition, combinations of the above mentioned specifically trained gait modifications can potentially reduce impact loading more than single modifications (Huang et al., Citation2019).
Self-selected gait modifications, in contrast with specifically trained gait modifications, allow runners the freedom to select and adopt one or more strategies to reduce impact loading. For example, Chan et al. (Citation2018) provided participants visual biofeedback of the vertical ground reaction force curve and asked them to ‘run softer’ without instructions for specific kinematic changes. This resulted in an overall reduction of about 18% in both vertical average loading rate (VALR) and vertical instantaneous loading rate (VILR) as compared to baseline. Napier et al. (Citation2019) used real-time visual feedback and a self-selected gait modification to reduce vertical braking forces and measured perceived difficulty and pain. Other gait retraining studies have shown similar results by implementing self-selected gait modifications with real-time visual and audio biofeedback (Crowell et al., Citation2010; Wood & Kipp, Citation2014).
Awkwardness quantifies how awkward participants feel about their movements and postures during gait modifications (Wheeler et al., Citation2011). And effort quantifies the difficulty experienced by participants in achieving the desired modifications (Caldwell et al., Citation2013). One general problem with both specifically trained and self-selected gait retraining programmes is that they can lead to increased perceived awkwardness and effort (Caldwell et al., Citation2013; Shull et al., Citation2013; Wheeler et al., Citation2011) which may compromise long-term sustainability of the gait modification (Eston et al., Citation1987). However, the influence of self-selected gait modification on impact loading, perceived awkwardness and perceived effort as compared with specifically trained gait modification is currently unclear. Thus, the aim and objective of this study was to investigate and compare the effects of self-selected gait modification and specifically trained gait modification on impact loading, perceived awkwardness and perceived effort in runners. As above-mentioned that specifically trained gait modification and combined gait modification both reduce impact loading as compared with baseline, we hypothesised that (1) self-selected gait modification would result in reduced impact loading as compared with baseline. Additionally, as self-selected gait modification was voluntarily chosen by participants themselves, we hypothesised that (2) self-selected gait modification would be perceived as less awkward and less effortful than specifically trained gait modifications.
Materials and methods
Participants
Participants were recruited from local running clubs to participate in this study. All participants shall be habitual shod rearfoot or midfoot strike runners (confirmed via video analysis) with a minimum running mileage of 10 km per week during the last at least 6 months. Participants were excluded if they had previously undergone lower limb or back surgery or had any cognitive impairments that would inhibit motor learning. Participants who previously participated in or were concurrently participating in gait retraining studies were excluded. Participants provided written informed consent prior to testing, and the experimental procedure was reviewed and approved by the Shanghai Jiao Tong University ethics committee (ml2018022).
Experimental protocol
Reflective markers were placed at specific body landmarks according to the modified Vicon Plug-in Gait lower body model (Vicon Motion Systems Ltd, Citation2002), and additional markers were placed at the C7 (spinous process of the seventh cervical vertebra), LSHO (acromioclavicular joint of left shoulder) and the RSHO (acromioclavicular joint of right shoulder) for capturing trunk motion. Marker trajectories were collected at 100 Hz via a 16-camera motion capture system (Vicon, Oxford, UK). Ground reaction force data were collected at 1,000 Hz via an instrumented treadmill (Bertec, Columbus, OH, USA). An inertial measurement unit (Xsens MTI300, Xsens North America Inc., CA, USA) was securely affixed to the anteromedial aspect of distal right tibia, and the x-axis was aligned with the longitudinal direction of the tibia to record peak tibial acceleration (PTA) (Crowell et al., Citation2010) at 1,000 Hz.
Participants first performed a 5-minute baseline trial while running at a self-selected pace (2.50 ± 0.24 m/s) with their own running shoes. To eliminate speed and footwear effects, the same running speed and shoes were used for all subsequent trials. Participants then performed three specifically trained gait modification trials in a randomised order: forefoot strike pattern, increased step rate (10% increased Bowersock et al., Citation2017; Hafer et al., Citation2015) and anterior trunk lean posture (10-degree increased trunk flexion Teng & Powers, Citation2014). Each trial lasted 5 min, and participants rested for 5 min or longer if requested between trials. Visual biofeedback was presented to train forefoot strike pattern (with two blocks indicating baseline and forefoot strike patterns, and a dot fall in the block during stance phase indicating the current strike pattern), and anterior trunk lean (with two blocks indicating baseline and 10-degree increased trunk lean, and a dot fall in the block indicating the current trunk lean angle), and a digital audio metronome (Seiko sq70, Seiko, Singapore) was used to help participants match the increased step rate (Heiderscheit et al., Citation2011). At the start of the trial, participants were told to follow the visual feedback to land the dot in the desired block (forefoot strike or increased trunk lean), or match the step rate to the audio feedback. Strike index was computed via a customised Matlab program (The Mathworks Inc, Natick, MA, USA) and was calculated as a measurement of the initial centre-of-pressure position relative to the foot length (Cavanagh & Lafortune, Citation1980), and forefoot strike pattern was defined as the front one-third. Trunk lean angle was measured as the intercept angle between the trunk and the pelvis segments in the sagittal plane (Teng & Powers, Citation2014), and anterior trunk lean was defined as 10 degrees more forward leaning than baseline. Step rate was calculated as the number of right foot steps recorded from the ground reaction force multiplied by two (Heiderscheit et al., Citation2011). A test facilitator monitored the modifications while standing next to the treadmill. The facilitator gave general oral instructions and encouragement to participants to adjust their gait patterns as needed, such as instructing more forefoot, increased forward lean or increased step rate.
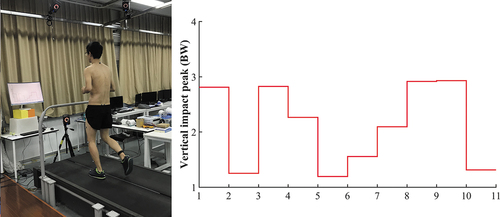
Participants then performed a 5-minute, self-selected gait modification trial with real-time vertical impact peak (VIP) feedback, in which they were free to choose any one or more simultaneous gait parameter modifications. VIP was chosen as the feedback parameter of impact loading due to its lower noise than loading rate and was computed based on established methods (Milner et al., Citation2006) via a customised Matlab program (The Mathworks Inc, Natick, MA, USA). The VIP value was updated on each step and displayed to participants as visual biofeedback on a monitor placed 1.5 m in front of the treadmill (). Participants were instructed to self-adjust their running gait pattern to decrease the real-time VIP values and given freedom to self-select gait modification(s) to accomplish this goal.
Figure 1. (Left) Typical subject running on the treadmill while receiving real-time visual biofeedback of the vertical impact peak. (Right) Vertical impact peak is displayed for the current step and the previous nine steps in the real-time stairstep plot, which is updated on each step. Participants performed self-selected running gait modifications to decrease the vertical impact peak value displayed on the monitor.
Subjective data were recorded at the end of each running trial (including baseline) to determine perceived awkwardness and perceived effort. Each participant rated the awkwardness of the running gait on a 10 cm visual analogue scale, with 0 corresponding to completely natural and 10 being maximally awkward (Barrios et al., Citation2010). Participants also rated their perception of effort required to execute the modified pattern on a 10 cm visual analogue scale, with 0 corresponding to effortless execution and 10 indicating maximal effort.
Data analysis
Marker data were filtered at 8 Hz and force and acceleration data at 50 Hz with a fourth order, recursive, Butterworth low pass filter (Crowell & Davis, Citation2011). PTA was calculated as the peak tibial acceleration during initial contact measure by the initial measurement unit. VIP was identified as the impact transient that was generated when the foot first contacted the ground (Lieberman et al., Citation2010). When no initial vertical impact peak existed, the 13% stance value was used as a surrogate (Blackmore et al., Citation2016). VALR was the slope of the line through the 20% point and the 80% point of the VIP, and VILR was the maximum slope of the vertical ground reaction force curve between successive data points in the same region (Crowell & Davis, Citation2011; Milner et al., Citation2006). For each trial, kinematic and kinetic outcomes were averaged from the last 20 steps of the third minute. Previous study found 10–12 steps were required to produce a stable estimation of running kinematics and kinetics (Riley et al., Citation2008), we chose 20 steps for conservative.
Extracted data were first examined for normality and homoscedasticity using Shapiro–Wilks and Levene’s tests, and no variable violated either assumption. One-way ANOVA and post hoc pairwise comparisons with Bonferroni adjustments were used to compare and find differences in strike index, step rate, trunk lean angle, VALR, VILR, VIP and PTA between self-selected gait modification and the three specifically trained gait modifications. Paired sample t-tests were used to compare differences in strike index, step rate, trunk lean angle for each participant and for VALR, VILR, VIP and PTA for all participants between baseline and self-selected gait modifications. Statistical analyses were conducted using SPSS (IBM, Armonk, NY, USA), and the significance level was set at 0.05 (in SPSS, p-value will be adjusted automatically when using Bonferroni adjustment).
Results
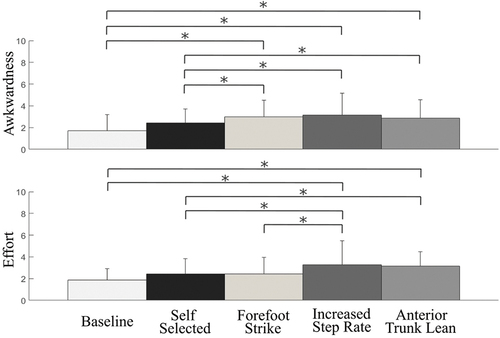
Sixteen healthy male runners (age: 22.1 ± 2.7 years; height: 1.79 ± 0.04 m; mass: 69.4 ± 6.4 kg; weekly running mileage: 16.6 ± 8.3 km; baseline perceived awkwardness: 1.7 ± 1.5; baseline perceived effort: 1.9 ± 1.1) were recruited from local running clubs to participate in this study. Overall, participants running with self-selected gait modification resulted in reduced impact loading with respect to VALR (25.3% reduction, p < 0.05), VILR (27.0% reduction, p < 0.05) and VIP (16.8% reduction, p < 0.05) as compared with baseline (). Forefoot strike pattern reduced VALR (48.4%, p < 0.05), VILR (29.2%, p < 0.05) and PTA (25.3%, p < 0.05). Increased step rate reduced VALR (24.0%, p < 0.05). Anterior trunk lean did not reduce any impact loading. Compared to baseline running, self-selected gait modification did not increase perceived awkwardness, while all three specifically trained gait modification increase perceived awkwardness (p < 0.05). For perceived effort, self-selected gait modification and forefoot strike pattern did not increase from baseline, while increased step rate and anterior trunk lean did (p < 0.05). Participants perceived more awkwardness when running with specifically trained gait modification than running with self-selected gait modification. Specifically, forefoot strike pattern was 23.4% higher (p < 0.05), increased step rate was 29.2% higher (p < 0.05) and anterior trunk lean was 17.7% higher (p < 0.05). As for perceived effort, increased step rate was 36.0% higher (p < 0.05) and anterior trunk lean was 30.0% higher (p < 0.05) compared with self-selected gait modification (). Participants successfully adopted the different specifically trained gait modifications as evidenced by the fact that: strike index was highest for the forefoot gait modification (p < 0.05); step rate was highest for the increased step rate modification (p < 0.05); and trunk angle was highest for the increased trunk angle gait modification (p < 0.05) ().
Table 1. Gait modifications, impact loading, perceived awkwardness and perceived effort for baseline, self-selected and specifically trained gait modifications across all participants.
Figure 2. Impact loading for baseline, self-selected gait modifications and specficially trained gait modifications. Bars indicate one standard deviation. Asterisks represent significant difference (p < 0.05).
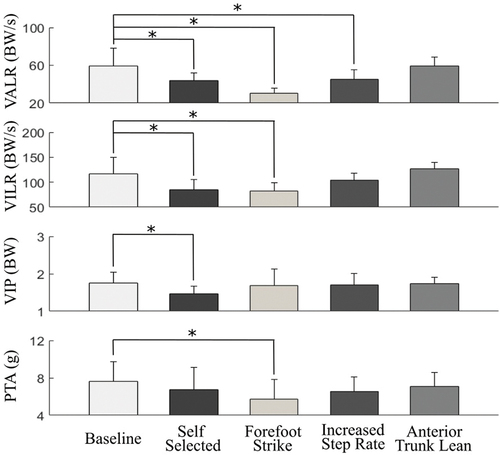
Figure 3. Perceived awkwardness and effort for baseline, self-selected gait modifications and specifically trained forefoot strike pattern, increased step rate and anterior trunk lean gait modifications. Bars indicate one standard deviation. Asterisks represent significant difference (p < 0.05).
Participants chose a variety of different self-selected gait modification strategies to reduce impact loading: strike index and step rate (four participants); anterior trunk angle (three participants); strike index (three participants); strike index, step rate and anterior trunk angle (two participants); strike index and anterior trunk angle (two participants); step rate and anterior trunk angle (one participant); step rate (one participant) ().
Table 2. Individual self-selected gait modifications by participant.
Discussion and implications
This study investigated the effect of self-selected gait modification as compared with specifically trained gait modification. In support of the first hypothesis, self-selected gait modification reduced VALR, VILR and VIP impact loading as compared with baseline, though it did not reduce PTA. In support of the second hypothesis, self-selected gait modification was perceived as less awkward and less effortful than specifically trained gait modifications with the exception of forefoot strike which was perceived as requiring equal effort as self-selected gait modification.
Results in this study demonstrating that self-selected gait modifications can reduce impact loading align with previous research in which participants were given freedom to self-select gait modifications to lower real-time PTA values, resulting in reductions in VALR, VILR and VIP (Clansey et al., Citation2014; Crowell & Davis, Citation2011; Crowell et al., Citation2010). And gait modifications to lower real-time ground reaction force values also resulted in reductions in VALR and VILR (Chan et al., Citation2018; Napier et al., Citation2019). We found no significant difference in PTA for self-selected gait modification, which aligns with other research on gait modifications targeting reductions in VALR (Chen et al., Citation2016; Yong et al., Citation2018), VILR (Chen et al., Citation2016; Cheung & Davis, Citation2011) and VIP (Cheung & Davis, Citation2011; Diebal et al., Citation2012). Other work involving increased step rate to lower impact loading (Bowersock et al., Citation2017; Heiderscheit et al., Citation2011; Willy et al., Citation2016) similarly reported no corresponding change in PTA (Yong et al., Citation2018). These indicate that gait modification to reduce other impact loading metrics might not necessarily reduce PTA. Future studies should investigate the correlation between different impact loading metrics during gait modifications. Self-selected gait modifications reduced impact loading also aligned with previous research in other loading reduction strategies, such as cushioned shoe (O’Leary et al., Citation2008) and softer running surface (Schütte et al., Citation2016). An 18% reduction in VALR and VILR after running gait modification is followed by a 62% reduction in the occurrence of injury at one-year follow-up (Chan et al., Citation2018), indicating that reduced impact loading is clinically relevant to reduce running injury. In our study, VALR and VILR were reduced by 25.3% and 27%, respectively; thus, self-selected gait modification could be a potential strategy for managing running injury, though caution should be taken that external impact loading metrics can be misleading in regards to representing loading within internal structures (Matijevich et al., Citation2019). Given that this study was an acute, one-session study, further study with longer training programme to identify compensatory loading mechanisms and potential diverse effects is required to determine whether self-selected gait modification was suitable for managing running-related injuries to confirm the clinical practice.
The reason that self-selected gait modification is perceived as less awkward and less effortful than specifically trained gait modifications may be due to the fact that each runner prefers a different modification strategy, and restricting all runners to the same specific gait modification would likely lead to increased perceived awkwardness and effort for a subset of participants. This implies that self-selected gait modification under real-time vertical ground reaction force biofeedback may be a more effective approach than specifically trained gait modification, giving runners the freedom to choose which modification they want to achieve impact loading reductions. However, it should be noted that real-time feedback of kinetic measure is the most effective strategy to reduce impact loading (Napier et al., Citation2015), which could also contribute to the success. The gait modification learned during self-selected gait may thus be more easily adopted and maintained during long-term gait training because of the lower perceived awkwardness and effort (Eston et al., Citation1987). However, before practical adoption of self-selected gait modification, more research is needed to investigate the lower-limb joint loading (internal loading) that may be necessitated to accommodate reduced impact. It should be noted that while forefoot strike gait was perceived as more awkward than self-selected gait modification, it was not perceived as requiring more effort and had a lower VALR (), which aligns with previous research that found it easier to employ a change in foot strike to minimise impact loading (Clansey et al., Citation2014). In addition, Napier et al. (Citation2015) noted that runners tended to employ a distal strategy of gait modification unless specific cues were given, which might indicate that modifying foot strike is one of the preferred methods of modifying gait. It is possible that over time, the perceived awkwardness of forefoot strike gait could subside, making it an equal or even better gait modification possibility than self-selected gait. However, whether forefoot strike gait can be sustained over longer running durations remains unknown, and thus more research over longer runs and extended training periods are needed to fully investigate the durability and effects of this gait modification strategy.
A limitation of this study was that we only tested runners during a single session. Further investigation should be performed to determine long-term learning and adaption effects with multiple training sessions and extended follow-up. It is unclear how perceived awkwardness and perceived effort may change over prolonged adoption of the self-selected and specifically trained gait modifications, and prolonged running durations as well. It is also important to investigate the motor control strategy with self-selected gait modification to reveal more insight if the modifications were passively and intuitively implemented due to comfort factor (Nigg et al., Citation2015). Another limitation is that while the three specifically trained gait modifications were randomised, the self-selected gait modification was always performed last. The original motivation for this was to first train runners to perform three gait modifications thought to influence loading rate and then give them freedom to self-select one or more modifications from those. This would potentially enable runners to more quickly and effectively reduce the loading rate biofeedback value and avoid frustration, because they would know which modifications to try as opposed to giving no directions. This clearly encouraged participants to adopt specific gait modifications; in a similar way, other self-selected gait modification studies have instructed runners to ‘run softer’ (Crowell & Davis, Citation2011; Crowell et al., Citation2010) that likely encouraged specific kinds of gait modifications. Providing less specific training or instructions in future studies could lead to a larger variety of self-selected gait modifications and provide further insights. Also, it is possible that participants reported less awkwardness for self-selected gait modifications in part because they were already somewhat familiar with the individual gait modifications performed during the specifically trained trials, which were performed first. In addition, while there were statistical differences in perceived awkwardness and effort between the self-selected gait modification and specifically trained techniques, the differences were on a very small order of magnitude, and therefore not likely to be clinically significant. Thus, more research is still needed to confirm the clinical significance. Future work could consider randomising all trials including the self-selected trial to determine whether the perceived awkwardness findings persist. Also, physiological effort could be measured with indirect metabolic cost (Shull & Xia, Citation2020), future work should measure both perceived and physiological effort to confirm the subjective measure. While we chose the specific foot strike pattern, trunk posture and cadence modification thresholds, based on recommendations from other related studies, it is possible that allowing participants to also choose their own single variable gait modification amount could also reduce impact variables, be less awkward and require less effort. In fact, in this study, six participants did choose to only modify one variable to reduce impact loading. Future research should further investigate the impact of self-selected, single-parameter gait modifications on perceived awkwardness and effort. Finally, only male participants were tested in this study, and given previously documented gender differences in gait biomechanics (Cho et al., Citation2004), further research is needed to determine whether the effects of self-selected gait modifications reported in this study for male runners can be extended to female runners.
This study implied that self-selected gait modification could be an effective training approach, by giving runners the freedom to choose which modification they want to achieve impact loading reductions. The gait modification learned during self-selected gait could be more easily adopted and maintained during long-term gait training because of the lower perceived awkwardness and effort, thus facilitate running modification. Runners could consider adopting self-selected running gait modification to reduce the risk of running-related injuries.
Conclusion
In conclusion, we investigated the effect of self-selected gait modification via real-time biofeedback and found it reduced impact loading as compared with baseline measurements. We also examined differences of self-selected gait modification compared to the specifically trained forefoot strike pattern, increased step rate and anterior trunk lean gait modifications. Result showed that self-selected gait modification is perceived as less awkward and requiring less effort, while the differences were statistically different, they were on a very small order of magnitude and therefore not likely to be clinically significant. Results of this study could broadly benefit runners, given that lower impact loading is closely related to running injuries and that self-selected gait modification is both effective in decreasing impact loading and perceived as more natural and comfortable to adopt. This could serve as a foundation to help inform gait modification approaches for runners.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Arendse, R. E., Noakes, T. D., Azevedo, L. B., Romanov, N., Schwellnus, M. P., & Fletcher, G. (2004). Reduced eccentric loading of the knee with the pose running method. Medicine and Science in Sports and Exercise, 36(2), 272–277. https://doi.org/10.1249/01.MSS.0000113684.61351.B0
- Barrios, J. A., Crossley, K. M., & Davis, I. (2010). Gait retraining to reduce the knee adduction moment through real-time visual feedback of dynamic knee alignment. Journal of Biomechanics, 43(11), 2208–2213. https://doi.org/10.1016/j.jbiomech.2010.03.040
- Blackmore, T., Willy, R. W., & Creaby, M. W. (2016). The high frequency component of the vertical ground reaction force is a valid surrogate measure of the impact peak. Journal of Biomechanics, 49(3), 479–483. https://doi.org/10.1016/j.jbiomech.2015.12.019
- Bowersock, C. D., Willy, R. W., DeVita, P., & Willson, J. D. (2017). Independent effects of step length and foot strike pattern on tibiofemoral joint forces during running. Journal of Sports Sciences, 35(20), 2005–2013. https://doi.org/10.1080/02640414.2016.1249904
- Caldwell, L. K., Laubach, L. L., & Barrios, J. A. (2013). Effect of specific gait modifications on medial knee loading, metabolic cost and perception of task difficulty. Clinical Biomechanics (Bristol, Avon), 28(6), 649–654. https://doi.org/10.1016/j.clinbiomech.2013.05.012
- Cavanagh, P. R., & Lafortune, M. A. (1980). Ground reaction forces in distance running. Journal of Biomechanics, 13, 397–406. https://doi.org/10.1016/0021-9290(80)90033-0
- Chan, Z. Y. S., Zhang, J. H., Au, I. P. H., An, W. W., Shum, G. L. K., Ng, G. Y. F., & Cheung, R. T. H. (2018). Gait retraining for the reduction of injury occurrence in novice distance runners: 1-year follow-up of a randomized controlled trial. The American Journal of Sports Medicine, 46(2), 388–395. https://doi.org/10.1177/0363546517736277
- Chen, T. L., An, W. W., Chan, Z. Y. S., Au, I. P. H., Zhang, Z. H., & Cheung, R. T. H. (2016). Immediate effects of modified landing pattern on a probabilistic tibial stress fracture model in runners. Clinical Biomechanics, 33, 49–54. https://doi.org/10.1016/j.clinbiomech.2016.02.013
- Cheung, R. T. H., & Davis, I. S. (2011). Landing pattern modification to improve patellofemoral pain in runners: A case series. Journal of Orthopaedic and Sports Physical Therapy, 41(12), 914–919. https://doi.org/10.2519/jospt.2011.3771
- Cho, S. H., Park, J. M., & Kwon, O. Y. (2004). Gender differences in three dimensional gait analysis data from 98 healthy Korean adults. Clinical Biomechanics, 19(2), 145–152. https://doi.org/10.1016/j.clinbiomech.2003.10.003
- Clansey, A. C., Hanlon, M., Wallace, E. S., Nevill, A., & Lake, M. J. (2014). Influence of tibial shock feedback training on impact loading and running economy. Medicine and Science in Sports and Exercise, 46(5), 973. https://doi.org/10.1249/MSS.0000000000000182
- Crowell, H. P., & Davis, I. S. (2011). Gait retraining to reduce lower extremity loading in runners. Clinical Biomechanics, 26(1), 78–83. https://doi.org/10.1016/j.clinbiomech.2010.09.003
- Crowell, H. P., Milnert, C. E., Hamill, J., & Davis, I. S. (2010). Reducing impact loading during running with the use of real-time visual feedback. Journal of Orthopaedic and Sports Physical Therapy, 40(4), 206–213. https://doi.org/10.2519/jospt.2010.3166
- Diebal, A. R., Gregory, R., Alitz, C., & Gerber, J. P. (2012). Forefoot running improves pain and disability associated with chronic exertional compartment syndrome. The American Journal of Sports Medicine, 40(5), 1060–1067. https://doi.org/10.1177/0363546512439182
- Eston, R. G., Davies, B. L., & Williams, J. G. (1987). Use of perceived effort ratings to control exercise intensity in young healthy adults. European Journal of Applied Physiology and Occupational Physiology, 56(February), 222–224. https://doi.org/10.1007/BF00640648
- Hafer, J. F., Brown, A. M., deMille, P., Hillstrom, H. J., & Garber, C. E. (2015). The effect of a cadence retraining protocol on running biomechanics and efficiency: A pilot study. Journal of Sports Sciences, 33(7), 724–731. https://doi.org/10.1080/02640414.2014.962573
- Heiderscheit, B. C., Chumanov, E. S., Michalski, M. P., Wille, C. M., & Ryan, M. B. (2011). Effects of step rate manipulation on joint mechanics during running. Medicine and Science in Sports and Exercise, 43(2), 296–302. https://doi.org/10.1249/MSS.0b013e3181ebedf4
- Huang, Y., Xia, H., Chen, G., Cheng, S., Cheung, R. T. H., & Shull, P. B. (2019). Foot strike pattern, step rate, and trunk posture combined gait modifications to reduce impact loading during running. Journal of Biomechanics, 86, 102–109. https://doi.org/10.1016/j.jbiomech.2019.01.058
- Lieberman, D. E., Venkadesan, M., Werbel, W. A., Daoud, A. I., D’Andrea, S., Davis, I. S., Mang’eni, R. O., & Pitsiladis, Y. (2010). Foot strike patterns and collision forces in habitually barefoot versus shod runners. Nature, 463(7280), 531–535. https://doi.org/10.1038/nature08723
- Matijevich, E. S., Branscombe, L. M., Scott, L. R., & Zelik, K. E. (2019). Ground reaction force metrics are not strongly correlated with tibial bone load when running across speeds and slopes: Implications for science, sport and wearable tech. PLoS ONE, 14(1), 1–19. https://doi.org/10.1371/journal.pone.0210000
- Milner, C. E., Ferber, R., Pollard, C. D., Hamill, J., & Davis, I. S. (2006). Biomechanical factors associated with tibial stress fracture in female runners. Medicine and Science in Sports and Exercise, 38(2), 323–328. https://doi.org/10.1249/01.mss.0000183477.75808.92
- Napier, C., Cochrane, C. K., Taunton, J. E., & Hunt, M. A. (2015). Gait modifications to change lower extremity gait biomechanics in runners: A systematic review. British Journal of Sports Medicine, 49(21), 1382–1388. https://doi.org/10.1136/bjsports-2014-094393
- Napier, C., MacLean, C. L., Maurer, J., Taunton, J. E., & Hunt, M. A. (2019). Real-time biofeedback of performance to reduce braking forces associated with running-related injury: An exploratory study. Journal of Orthopaedic & Sports Physical Therapy, 49(3), 136–144. https://doi.org/10.2519/jospt.2019.8587
- Nigg, B. M., Baltich, J., Hoerzer, S., & Enders, H. (2015). Running shoes and running injuries: Mythbusting and a proposal for two new paradigms:‘preferred movement path’and ‘comfort filter’. British Journal of Sports Medicine, 49(20), 1290–1294. https://doi.org/10.1136/bjsports-2015-095054
- O’Leary, K., Vorpahl, K. A., & Heiderscheit, B. (2008). Effect of cushioned insoles on impact forces during running. Journal of the American Podiatric Medical Association, 98(1), 36–41. https://doi.org/10.7547/0980036
- Pohl, M. B., Hamill, J., & Davis, I. S. (2009). Biomechanical and anatomic factors associated with a history of plantar fasciitis in female runners. Clinical Journal of Sport Medicine, 19(5), 372–376. https://doi.org/10.1097/JSM.0b013e3181b8c270
- Riley, P. O., Dicharry, J., Franz, J., Croce, U. D., Wilder, R. P., & Kerrigan, D. C. (2008). A kinematics and kinetic comparison of overground and treadmill running. Medicine and Science in Sports and Exercise, 40(6), 1093–1100. https://doi.org/10.1249/MSS.0b013e3181677530
- Schütte, K. H., Aeles, J., De Beéck, T. O., van der Zwaard, B. C., Venter, R., & Vanwanseele, B. (2016). Surface effects on dynamic stability and loading during outdoor running using wireless trunk accelerometry. Gait and Posture, 48, 220–225. https://doi.org/10.1016/j.gaitpost.2016.05.017
- Shull, P. B., Silder, A., Shultz, R., Dragoo, J. L., Besier, T. F., Delp, S. L., & Cutkosky, M. R. (2013). Six-week gait retraining program reduces knee adduction moment, reduces pain, and improves function for individuals with medial compartment knee osteoarthritis. Journal of Orthopaedic Research : Official Publication of the Orthopaedic Research Society, 31(7), 1020–1025. https://doi.org/10.1002/jor.22340
- Shull, P. B., & Xia, H. (2020). Modeling and prediction of wearable energy energy rate outside of the lab. Sensors, 20(23), 6915. https://doi.org/10.3390/s20236915
- Teng, H. L., & Powers, C. M. (2014). Sagittal plane trunk posture influences patellofemoral joint stress during running. Journal of Orthopaedic & Sports Physical Therapy, 44(10), 785–792. https://doi.org/10.2519/jospt.2014.5249
- Van Der Worp, H., Vrielink, J. W., & Bredeweg, S. W. (2016). Do runners who suffer injuries have higher vertical ground reaction forces than those who remain injury-free? A systematic review and meta-analysis. British Journal of Sports Medicine, 50(8), 450–457. https://doi.org/10.1136/bjsports-2015-094924
- Van Gent, R. N., Siem, D., van Middelkoop, M., van Os, A. G., & Koes, B. W. (2007). Incidence and determinants of lower extremity running injuries in long distance runners: A systematic review. British Journal of Sports Medicine, 41(8), 469–480. https://doi.org/10.1136/bjsm.2006.033548
- Vicon Motion Systems Ltd. (2002). Plug-in-Gait model. Vicon® Manual.
- Wheeler, J. W., Shull, P. B., & Besier, T. F. (2011). Real-time knee adduction moment feedback for gait retraining through visual and tactile displays. Journal of Biomechanical Engineering, 133(4), 041007. https://doi.org/10.1115/1.4003621
- Willy, R. W., Buchenic, L., Rogacki, K., Ackerman, J., Schmidt, A., & Willson, J. D. (2016). In-field gait retraining and mobile monitoring to address running biomechanics associated with tibial stress fracture. Scandinavian Journal of Medicine and Science in Sports, 26(2), 197–205. https://doi.org/10.1111/sms.12413
- Wood, C. M., & Kipp, K. (2014). Use of audio biofeedback to reduce tibial impact accelerations during running. Journal of Biomechanics, 47(7), 1739–1741. https://doi.org/10.1016/j.jbiomech.2014.03.008
- Yong, J. R., Silder, A., Montgomery, K. L., Fredericson, M., & Delp, S. L. (2018). Acute changes in foot strike pattern and cadence affect running parameters associated with tibial stress fractures. Journal of Biomechanics, 76, 1–7. https://doi.org/10.1016/j.jbiomech.2018.05.017